
Abstract
Performing aesthetic breast operations requires the surgeon’s ability, creativity, knowledge, mental concentration, and adequate ambiance in the operating room. Because of the very heavy and complex activities during the operation the surgeon should not be in charge of administering medication for sedation of the patient during surgery. It is not safe for a surgeon to take care of the patient’s condition: fluctuations of blood pressure, pulse, irregularity of respiratory depth and rate. It is essential for an anesthesiologist to be in charge of the anesthesia during the operation. The choice of the anesthesia is a matter of a good understanding between the surgeon and the anesthesiologist, which may be: general anesthesia; local anesthesia combined with intravenous sedation, or epidural anesthesia combined with intravenous sedation. Problems that are considered to be of little consequence in other surgical specialties are of major importance to the patient undergoing aesthetic breast surgery, because she is much more concerned about the surgical results and about pain during the operation and postoperatively.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
1 Introduction
Anesthesia is an important specialty in medicine with great developments since the first decade of the twentieth century, which provides fantastic support to the progress in all surgical fields, particularly plastic surgery. The first anesthesia is credited to Crawford Williamson Long in 1846 (Reis Junior 2006) using sulfuric ether for surgical procedures, which opened up a wide field. Later, Long was serving in the Army during the North American Civil War (1861–1865) when he had opportunity to do a great deal of work using his knowledge. Afterward, chloroform was also employed for surgical amputations. During the World War I in Europe, as there were many people requiring surgical repairs, Long’s knowledge was useful (Reis Junior 2006). Several other types of anesthesia emerged for performing operations without pain during World War II in several fields of medicine, especially disfigurement of the human body, as described by Gillies and Millard (1957). Unfortunately, during those periods of great bloodshed, some specialties showed remarkable improvements and evolution because of the emergency procedures for repairs of physical deformities.
Ever since I made the decision to publish a book concerning aesthetic surgery of the breast, it was clear in my mind that it was necessary to include a chapter dedicated to anesthesia, that could be written by a well-qualified anesthesiologist. However, the purpose of this chapter is not to teach how to perform anesthesia, or even to inform the reader about particular details concerning drugs and some technical topics. This knowledge may be very well described in books and in the Journal of Anesthesia along with all the technical information. As I have always been interested in this subject, I edited a book called Local and Regional Anesthesia in Aesthetic Plastic Surgery (Avelar 1993a, b) focusing on information for plastic surgeons. The main purpose of that book was not to encourage other plastic surgeons to perform operations by themselves alone without the active presence of an anesthesiologist. There are 45 outstanding Brazilian authors who wrote other chapters about their methodology for performing aesthetic plastic surgery under local or regional anesthesia. All authors described updated topics along the lines of not encouraging our colleagues to perform aesthetic procedures without the participation of anesthesiologists. In mean time, aesthetic breast surgeons were fascinated to perform surgery under local anesthesia combined with intravenous sedation under the care of an anesthesiologist (Avelar 1980, 1993b; Avelar and Catunda 1985).
Performing an aesthetic breast operation requires a surgeon’s ability, creativity, knowledge, mental concentration, and adequate ambiance in the operating room. Thus, on top of all those surgical steps, it is not appropriate for he or she to take care of the patient’s condition as well, i.e., fluctuations in blood pressure, pulse, irregularity of respiratory depth and rate, bucking and coughing, increased bleeding in the wound, straining and moving during application of the surgical dressing, all signs and symptoms that require special attention and immediate treatment. For all these reasons, the presence of an anesthesiologist during surgery in the operating room may deal with any problems, providing adequate support for the surgeon in performing the operation (Avelar 1993b). As I had the privilege to be Prof. Pitanguy’s resident, I learned from him, as he always used to perform his operations with an anesthesiologist, and this is mentioned in some of his publications (Pitanguy 1961; Pitanguy et al. 1971, 1977; Pitanguy and Garcia 1972). Problems that are considered to be of little consequence in other specialties are of major importance to the patients undergoing breast aesthetic surgery, during the operation as well as postoperatively regarding pain, which should be minimal (Avelar 1993a).
2 Method
2.1 Preoperative Evaluation
Before a patient goes to the hospital to undergo a breast operation, his or her surgeon has already examined her during previous consultations for surgical indications and planning in addition to surgical pre-marking, according to the routine of each surgeon.
My preference is to demarcate some reference points 1 day before surgery and once more to examine the breasts and take other photos. It is useful to do pre-marking at my clinic to provide essential orientation, as the patient is awake and follows my work, which is done in front of two parallel vertical mirrors strategically placed on the walls of examination room (Fig. 5.1). Under this system, each patient sees my pre-marking and she can confirm all the information about location and size of the scars as well. She can even observe again her asymmetric breasts and the posterior aspect of the torso and chest deformities secondary to the hypertrophic breasts. After pre-marking, my patients sign informed consent.

Photo of a patient in the examination room at my clinic. She is in a standing position in front of one vertical mirror (VM), she sees her body from the frontal view and from the back view simultaneously through the oblique mirrors (OM), as indicated by the arrows
Routine blood test, heart examination and other specific examinations according to the surgical planning are always carried out, which are carefully observed.
2.1.1 At the Hospital
When a patient goes to the hospital it is essential that the anesthesiologist visits and examine her before aesthetic breast surgery to gain the confidence of the patient and to relieve any fears and anxieties. In fact, this is the first time they meet each other. That brief moment is adequate opportunity for a good understanding between them. Also, a patient with a history of heart, lung, chronic kidney disease, unstable blood pressure, and other circumstances that raise concerns regarding anesthesia for the operation, is given careful consideration. Because of the increased risk involved, elective surgery should not be attempted following any previous disease. A patient who is accustomed to a daily alcohol intake, or who routinely takes sedatives for insomnia should be well evaluated before premedication, and, most likely, given higher concentrations of anesthetic agents to produce a satisfactory state of unconsciousness. A detailed oral examination is mandatory because of the many delicate dental restorations commonly observed today. Most potential errors in the management of anesthesia can be avoided by careful preoperative evaluation and planning. Finally, the patient should have confidence in the anesthesiologist before undergoing breast surgery (Avelar 1993b).
Gentleness is an art when inducing and sustaining a pain-free unconscious state. Administering an anesthetic means applying a measured physiological insult to a patient under precise pharmacological control. The choice of premedication and anesthetic agents is made at this time, according to anesthesiologist’s decision.
2.2 Premedication
The patient who has undergone proper administration of premedication usually arrives in the operating room in a drowsy, amnesic, and cooperative estate, with no circulatory or respiratory depression. This optimal condition may be achieved by a combination of drugs, which is given by anesthesiologist. Because of its pharmacological activity, each drug plays an important role in the final result. Drugs used for premedication include barbiturates, belladonna alkaloids, tranquilizers, and narcotics. All these decisions and drug administration are under the anesthesiologist’s control. Even if he or she takes the decision not to administer any drugs as premedication, it means that it is an appropriate condition for the patient undergoing the operation. Such a circumstance sometimes occurred with my patients, that I did not take part in the decisions, as long as the operation is carried out under good conditions.
2.2.1 Breast Surgery
The choice of the anesthesia technique is a matter of a good understanding between the plastic surgeon and the anesthesiologist. I do not feel comfortable decide which method must be followed. In fact, each surgeon may take his or her decision in accordance with the anesthesiologist so that they are both comfortable bearing in mind that the patient’s life is in their hands. Sometimes, a patient says that her preference for one or other type of anesthesia, which should have been previously well-evaluated during consultation at the office and during premedication. As long as the patient’s suggestion is well understood and accepted by the surgeon and the anesthesiologist it is a matter of good sense and reasonable to do that.
2.3 The Choice of Anesthesia
There are five types of anesthesia used for performing breast surgery:
-
(1)
General anesthesia (Fig. 5.2)
Fig. 5.2 
Drawings to demonstrate surgical marking during the operation under general anesthesia with endotracheal intubation. (a)—A long line is stitched on the sternal notch and another on the xyphoid process. (b) Using forceps, the two lines are held for comparison of the two breasts after surgical marking and during surgery
-
(2)
Local anesthesia combined with intravenous sedation (Fig. 5.3)
Fig. 5.3 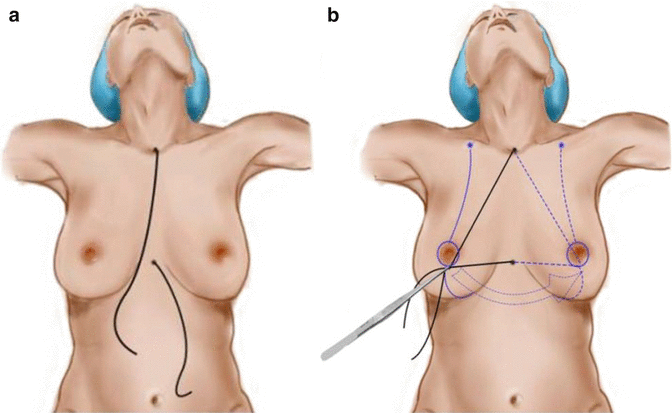
Two drawings show surgical marking during the operation under local anesthesia combined with intravenous sedation. (a) A long line is stitched on the sternal notch and another on the xyphoid process. (b) Using forceps, the two lines are held for comparison of the two breasts after surgical marking
-
(3)
Epidural anesthesia combined with intravenous sedation (Fig. 5.4)
Fig. 5.4 
Epidural anesthesia for aesthetic breast surgery. Photo shows the epidural being performed by the anesthesiologist with the patient sitting on the operating table
-
(4)
Intercostal block infiltration combined with intravenous sedation
-
(5)
Local anesthesia without participation of an anesthesiologist



2.3.1 General Anesthesia
Performing breast surgery under general anesthesia is the most frequent procedure, as the patient’s condition is under the control of the anesthesiologist and the surgeon may work comfortably. Even when associated surgical procedures are scheduled, general anesthesia provides adequate and safe conditions. Nevertheless, local infiltration can be performed to avoid too much bleeding during the operation. The patient’s breathing (through the endotracheal tube), heart control, drug administration, and all other aspects during surgery are under the rigid control of the anesthesiologist, who should provide the surgeon with peaceful conditions under which to work (Fig. 5.2).
My preference is to perform breast surgery with the patient in a semi-sitting position with the arms at a 45° angle from the body laterally on each side of the torso (Fig. 5.3) (Pitanguy 1961; Gillies and McIndoe 1939). When I perform a combined procedure of mastoplasty with rhytidoplasty, or rhinoplasty, or with abdominoplasty, or any procedure on the lower extremities, I always start the operation by first performing the mastoplasty because of the semi-sitting position of the patient on the operating table. I consider this safer than vice versa (Pitanguy 1981). It is important to emphasize that I perform only one procedure associated with the breast operation on a patient if she is in good health and the anesthesiologist is in agreement to performing the two procedures.
After endotracheal intubation and all the activities concerning the anesthesiologist’s medications providing good conditions for anesthesia, the patient is then prepared for the operation according to the routine of each surgeon. I prefer to raise the table to about 45° to elevate the head and torso of the patient so that the breasts show the natural degree of ptosis. I had the privilege of being trained by Prof. Pitanguy, who used to perform combined procedures and mastoplasty with the patient in the semi-sitting position (Pitanguy 1975; Pitanguy and Garcia 1972; Pitanguy et al. 1977).
In addition to the patient being under general anesthesia, local infiltration may be done with the use of vasoconstrictor agents to reduce bleeding during surgery. These agents, by causing local vasoconstriction (a chemical tourniquet effect), reduce the rate of absorption of the local anesthetic agent, if it is added to the solution in accordance with the anesthesiologist and thus reduces the incidence of adverse reactions. They also prolong the duration of the anesthetic. The dangers of these agents, particularly epinephrine (which is the best), lie in the use of unnecessarily high concentrations. The solution I am used to employing is 1:200,000 (1 mL of epinephrine (1:1000) and 200 mL of serum) produces a proper degree of vasoconstriction (Pitanguy et al. 1971). Stronger solutions increase the vasoconstrictor effect and may induce complications of epinephrine intoxication, which are nervousness, cold sweats, hypertension, and tachycardia, in addition to severe arrhythmias. Errors in the preparation of local analgesic agents containing epinephrine should be avoided.
Usually, a volume of 200 mL of solution is enough to perform local infiltration for both breasts, even in large hypertrophic breasts, as it is not necessary to infiltrate the mammary gland (Avelar 1993a, b).
Infiltration of the solution with epinephrine is done on three levels (Fig. 5.5a):

Local infiltration is performed by the surgeon at two levels: on the subcutaneous plane and between the mammary gland and the fascia of the pectoralis major muscle. (a) The drawing demonstrates the two levels of infiltration. (b) Photo during infiltration shows the surgeon holding the left breast with one hand and using a long needle that is being introduced below the mammary gland. (c) Photo shows the surgeon holding the right breast and using a long needle to infiltrate below the mammary gland and above the fascia of the pectoralis major muscle. (d) Photo showing the infiltration in a different direction below the mammary gland
-
(a)
Below the mammary gland. Using a long needle, infiltration is carried out all over the area below the mammary gland. With left hand, the surgeon holds the breast and pulls it forward to create a natural space between the mammary gland and the aponeurosis of the pectoralis major (Fig. 5.5b–d). Caution is necessary to avoid infiltration inside the muscle, which leads to massive absorption of the solution with undesirable consequences. With the left hand holding the breast, the surgeon can be sure that the needle is passing just below the tip of his fingers and above the muscular level. Under this maneuver, the needle passes on “dead” space between the mammary gland and the pectoralis major. This infiltration provides good conditions for surgery, as there is minimal absorption of the solution.
-
(b)
On a subcutaneous level on the pre-axillary line at the external border of the breast. Through this infiltration good anesthesia is achieved during and after the operation, as branches of the intercostobrachial nerve and the ends of the intercostal nerves are adequately infiltrated (Fig. 5.6a).
Fig. 5.6 
Local infiltration is being performed by the surgeon on a subcutaneous level. (a) Photo shows the surgeon holding the left breast to infiltrate the external border on the pre-axillary line to block the innervation of the ending of the intercostobrachial nerve in the subcutaneous plane. (b) Photo during infiltration shows the surgeon holding the left breast with one hand and using a regular needle to infiltrate the demarcated lines of the mastoplasty
-
(c)
On a subcutaneous level, all around the areola and the demarcated lines on the anterior surface of the breasts (Fig. 5.6b). Once again, it is important to emphasize that it should not infiltrate the mammary gland.

Afterward, reduction mastoplasty or mastopexy is performed following surgical demarcations.
2.3.2 Local Anesthesia Combined with Intravenous Sedation
This is my favorite choice, as long as the anesthesiologist can induce good sedation to provide comfortable conditions. Once again, pre-marking and premedication follow the same methods described above. Pre-marking is done at my clinic on the day before the operation.
In the operating room, the anesthesiologist administers proper intravenous sedation according to his criteria and decision. Afterward, the patient is prepared for surgery, as described for general anesthesia (Figs. 5.5 and 5.6).
Local infiltration is carried out according to the previous description. In this type of local anesthesia combined with intravenous sedation, it is mandatory to add anesthesia (my preference is lidocaine) to the solution, which I call 201 (Avelar 1993a, b), as it is easily prepared by this method: 160 mL of serum + 40 mL of lidocaine (2%) + 1 mL of epinephrine (1/1000).
The technique of infiltration is similar to that previously described, that is it: below the mammary gland, on the lateral and external borders of the breast, underneath of the areola and subcutaneously on the demarcated area for mastoplasty (Figs. 5.3, 5.5 and 5.6). Once again, it is important to emphasize that it is not necessary to infiltrate the mammary gland.
2.3.3 Epidural Anesthesia Combined with Intravenous Sedation
This type of anesthesia is not at all my preferred option, but it may be the anesthesiologist's preference. If the surgeon has enough confidence in the anesthesiologist, it is possible to perform breast surgery (Fig. 5.4). I used to perform operations at a hospital where the anesthesiologists are very well trained and they perform outstanding epidural anesthesia, which provides excellent conditions for performing breast operations. In addition to the epidural anesthesia, I do carry out local infiltration in all patients without anesthetic drugs, but only with epinephrine to avoid bleeding during the operation (Figs. 5.3 and 5.4). It is important to emphasize that the patient chooses her surgeon to perform breast surgery; therefore, he takes all responsibility for the operation.
When this type of anesthesia is administered, all conditions for the operation may be organized according to the surgeon’s necessities: the position of the patient on the operating table, the position of the table, local infiltration to avoid too much bleeding, etc. (Fig. 5.7).

Epidural anesthesia for aesthetic breast surgery. Photo during surgery shows a patient under local anesthesia combined with intravenous sedation under the care of an anesthesiologist behind the patient with all equipment in the operating room
There is no relationship between the type of anesthesia and the surgical results, as long as the patient feels very comfortable after surgery (Figs. 5.8 and 5.9). Such a procedure may also be employed for breast augmentation with silicone prosthesis (Fig. 5.10), even when mastoplasty is performed for removal of the breast implant combined with mastopexy (Fig. 5.11).


A 49-year-old patient with hypertrophic, asymmetrical, and ptotic breasts underwent reduction mastoplasty. (a, c, e, g) Photos before surgery. (b, d, f, h) Photos after reduction mastoplasty under local anesthesia combined with intravenous sedation

A 38-year-old patient with hypertrophic breasts underwent reduction mastoplasty. (a, c) Photos before surgery. (b, d) Photos after reduction mastoplasty under local anesthesia combined with intravenous sedation

Local infiltration for augmentation mastoplasty with a silicone prosthesis implant. (a) Photo shows the surgeon infiltrating the external border of the right breast on the pre-axillary line to block the innervation of the ending of the intercostobrachial nerve in the subcutaneous plane using a regular needle. (b) The infiltration is done all way to the external border of the breast

Local infiltration for removing of a mammary implant followed by mastopexy. (a) Photo shows the surgeon infiltrating the external border of the right breast on the pre-axillary line to block the innervation of the ending of the intercostobrachial nerve in the subcutaneous plan using a regular needle. (b) Photo during infiltration shows the surgeon holding the right breast with one hand and using a long needle to infiltrate below the mammary implant and above the pectoralis major muscle. (c) Photo shows the surgeon holding the right breast and using a long needle to infiltrate below the mammary implant and above the fascia of the pectoralis major muscle. (d) Photo showing the infiltration of the demarcated lines of the mastoplasty using a regular needle
2.3.4 Intercostal Block Infiltration Combined with Intravenous Sedation
2.3.5 Local Anesthesia Without Participation of an Anesthesiologist
I consider both types of anesthesia the worst for breast operations, no matter whether intercostal block infiltration is carried out by the anesthesiologist or by the surgeon, as reported by Huang et al. (1979). There has already been some sort of complications during such anesthesia with severe problems for patients and surgeons alike. It is mentioned here only to demonstrate the possibility, but I do not at all recommend it. I have heard about perforation of the chest wall with tearing of the pleura with the needle due to intercostal block infiltration. Infiltration may not be regular throughout the intercostal spaces if some of the injections do not reach the nerves. Therefore, the effect of the anesthesia will not be satisfactory. If other injections have to be administered during surgery, this may spoil the ambience of the operation.
3 Discussion
Local anesthesia for breast surgery associated with general anesthesia or with intravenous sedation under the care of an anesthesiologist is a useful procedure. Safe administration depends on certain conditions, such as.
-
1.
Proper dose of premedication.
It is my personal preference that it is not wise for a surgeon to perform breast operations by himself or herself with only his or her staff, without the participation of an anesthesiologist. The desire to avoid patient discomfort during local anesthesia leads the surgeon to attempt to produce the state of general anesthesia by ordering heavy premedication. The presence of an anesthesiologist who has enough knowledge provides adequate support for the surgeon to perform aesthetic surgery on the breast in addition to other types of surgery. Premedication is designed merely to produce a state of calm relaxation, while unusual or uncomfortable situations may occur before the operation. The patient should sustain all vital functions, including responsiveness. It is much safer for the surgeon to perform his or her operations under adequate medication than to run the risk of any iatrogenic complications.
-
2.
The application or injection of the adequate concentration of the selected agent.
The surgeon must remember that it is almost impossible to predetermine the exact amount of premedication that will be effective for each patient. Continuous injection of small doses intravenously may not produce an adequate degree of control.
-
3.
Avoidance of intravenous injections of solutions.
This circumstance may occur accidentally during surgery with an unexpected patient’s reaction. For this reason, I consider that it is not safe for a surgeon to perform any operation without the participation of an anesthesiologist.
-
4.
Well-balanced vasoconstrictor drugs.
Each surgeon must have as a matter of routine the adequate solution to use during surgery to avoid bleeding. In my practice, I am used to employing local infiltration during breast surgery under general anesthesia under the care of an anesthesiologist. My preferred solution is: 1:200,000 (1 mL of epinephrine (1:1000) and 200 mL of serum), which produces the proper degree of vasoconstriction.
Nevertheless, when mastoplasty is performed under local anesthesia combined with intravenous sedation under the care of an anesthesiologist my solution is: 160 mL of serum + 40 mL of lidocaine (2%) + 1 mL of epinephrine (1/1000). With the use of this volume, it is possible to infiltrate both breasts for mastopexy or even reduction mastoplasty.
-
5.
Constant vigilance to treat adverse reactions.
This is the main reason why a surgeon should work with an anesthesiologist during an operation. If some unexpected reaction is caused by injection of the solution, the surgeon is not adequately prepared for immediate treatment, as he or she is concentrating on the operation.
The use of vasoconstrictors is useful to avoid bleeding during the operation and to prolong the duration of the anesthetic. The dangers of these agents, particularly epinephrine, lies in the use of unnecessarily high concentrations. Each surgeon may have a routine solution that all members of staff are used to so as to observe the preparation and the volume during administration (Figs. 5.13 and 5.14).
After the operation, the patient can usually sit on the operating table, which is useful for performing the bandaging (Fig. 5.12).

After reduction mastoplasty the patient is awake and in a good enough condition to sit on the operating table for application of the dressing. (a) The patient can be seen on the operating table with adhesive tapes on her breasts; her preoperative photos and the anesthesiologist's equipment can also be seen. (b) She is sitting in a good enough condition undergo bandaging around the chest. (c) The bandaging is done


A 26-year-old patient with hypertrophic, asymmetrical, and ptotic breasts underwent reduction mastoplasty. (a, c, e) Photos before surgery. (b, d, f) Photos after reduction mastoplasty under epidural anesthesia combined with intravenous sedation


A 31-year-old patient with hypertrophic, asymmetrical, and ptotic breasts underwent reduction mastoplasty. (a, c, e) Photos before surgery. (b, d, f) Photos after reduction mastoplasty under epidural anesthesia combined with intravenous sedation
4 Complications
Complications related to anesthesia during aesthetic breast surgery may occur because of:
-
(1)
The dose of drug administration
-
(2)
Unexpected metabolic reactions
-
(3)
Allergic reactions
-
(4)
Postural imbalance
-
(5)
Respiratory depression
-
(6)
Cardiac arrhythmias
As long as an anesthesiologist is in charge of the anesthesia he or she must take care of the patient all the time, from the premedication until after the operation while she stays in the recovery room.
In the case of circulatory depression, as indicated by hypotension, the anesthesiologist should immediately check the respiration, pulse, and blood pressure, as tachycardia, tachypnea, and hypotension are the adverse signs most frequently encountered.
The anesthesiologist must check if inadvertent intravenous injection was administered or an incorrect dose of the drug concentration, or the toxic dose of an agent was exceeded, which are some common errors.
A patient should never be left unattended: a means of monitoring the patient’s vital signs must be used at all times. This essential monitoring must be carried out by efficient electronic devices throughout the operation.
No matter whether the operation was performed under general anesthesia, local anesthesia combined with intravenous sedation, or epidural anesthesia, the final step for the anesthesiologist is when the patient goes out of the postoperative recovery room.
Conclusions
Any breast operation must be well evaluated preoperatively by the surgeon from the point of view of the patient’s complaints. The operation must be well planned to be performed at the hospital under the care of an anesthesiologist. Blood tests, heart examination, and others must be carried out preoperatively according to the routine of each surgeon. Premedication is an important step before surgery as it is the first time that the patient speaks to the anesthesiologist. The choice of anesthesia is a matter of a good understanding between the surgeon and the anesthesiologist, and may be general anesthesia; local anesthesia combined with intravenous sedation; or epidural anesthesia combined with intravenous sedation. There are other possibilities for performing mastoplasty, but they are not safe.
References
Avelar JM (1980) Retalho dermo-adiposo-glandular de pedículo superior nas ptoses mamárias (Dermal-adipose-glandular flap with superior pedicle in ptotic breasts). Simpósio Brasileiro de Cirurgia da Mama, São Paulo, August
Avelar J (1993a) In: Avelar JM (ed) Anestesia Loco-Regional em Cirurgia Estética (Loco-regional anesthesia on aesthetic surgery). Editora Hipócrates—Brazil, São Paulo
Avelar JM (1993b) Mastoplastia redutora sob anestesia local (Reduction mastoplasty under local anesthesia). In: Avelar JM (ed) Anestesia Loco-regional em cirurgia estética—(Loco-regional anesthesia on aesthetic surgery). Editora Hipócrates, São Paulo, pp 244–260
Avelar JM, Catunda MM (1985) Anestesia local na cirurgia do contorno corporal (Local anesthesia on body contour surgery). Anais do XII Congresso Brasileiro de Cirurgia Plástica (Annals of the XII Brazilian Congress of Plastic Surgery)—Gramado, RS—Brazil—Novembro, pp 415–416
Gillies H, McIndoe AH (1939) The technique of mammaplasty in conditions of hypertrophy of the breast. Surg Gynecol Obstet 72(68):658
Gillies H, Millard R Jr (1957) The principle and art of plastic surgery. Little Brown, Boston
Huang TT, Parks DH, Lewis SR (1979) Outpatient breast surgery under intercostal block anesthesia. Plast Reconstr Surg 63(3):299–303
Pitanguy I (1961) Aproximação eclética ao problema das mamaplastias (An eclectic approach to breast problems). Rev Bras Cir 41:179–196
Pitanguy I (1975) Abdominal lipectomy. Clin Plast Surg 3:401–410
Pitanguy I (1981) The breast. In: Aesthetic plastic surgery of head and body. Springer-Verlag, Berlin. pp 3–62
Pitanguy I, Garcia LC (1972) Aspectos importantes de técnica pessoal em mamaplastia (Important aspects of personal technique on mastoplasty). Soc Cir Plast Reconstr. sumário, Córdoba, Argentina
Pitanguy I, Cansação Á, Ramos H, Araújo M (1971) Mamaplastias. Estudo comparativo da evolução técnica em torno de 1196 casos pessoais (Mammaplasties comparative study of the technique evolution around 1196 personal cases) Rev Bras Cirurgia Nov/dez: 227–236
Pitanguy I et al (1977) Cirurgias Estéticas Combinadas (Combined aesthetic surgeries). Rev Bras Cir 67(7/8):265–272
Reis Junior A (2006) The first to use surgical anesthesia was not a dentist, but the physician Crawford Williamson Long. Rev Bras Anestesiol 56(3):304–324
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Avelar, J.M. (2018). Anesthesia for Aesthetic Breast Surgery. In: Avelar, J. (eds) Breast Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-54115-0_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-54115-0_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-54114-3
Online ISBN: 978-3-319-54115-0
eBook Packages: MedicineMedicine (R0)