
Abstract
Carpal tunnel syndrome (CTS) is a median nerve mononeuropathy caused by entrapment within the carpal tunnel. Patients often present with paresthesias and dysesthesias initially, progressing to weakness and functional loss if left untreated. On examination, sensory loss and positive provocative tests such as Phalen’s and Tinel’s are common. Severe cases demonstrate atrophy of the muscles innervated by the median nerve distal to the wrist. While diagnosis is largely clinical, electrodiagnostic studies are used to confirm the diagnosis as well determine severity, which is especially important prior to surgery. Conservative management includes rest, therapy, splinting, and use of either oral or injected corticosteroids. However, in advanced disease or cases failing conservative treatment, surgical intervention is necessary.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
Definition
Carpal tunnel syndrome is a constellation of symptoms secondary to median nerve compression under the transverse carpal ligament. It is the most common entrapment neuropathy of the upper extremity [1]. Symptoms include paresthesias in the median nerve distribution distal to the wrist though pain may occasionally radiate proximally into the forearm. There may be further progression to weakness and functional loss [1].
The syndrome is most common in women and often with bilateral involvement, though the dominant hand usually presents first and is more severely affected [2]. Most cases are idiopathic; however, some of the many reported etiologies include trauma, mass effects from tumors, and inflammatory disorders. The idiopathic cases are thought to be caused by overuse and repetitive tasks [3]. Regardless of the etiology, the symptoms are caused by nerve compression resulting in ischemia and demyelination and, in more advanced and severe cases, axonal loss and Wallerian degeneration [3].
Diagnosis
Diagnosis is clinical and is based on a thorough history and physical exam. The first complaint is commonly of paresthesias, dysesthesias, or numbness in the median distribution distal to the wrist. These symptoms are often exacerbated at night and relieved with shaking of the hand, known as the “flick sign” [1]. Patients may complain of pain in the hand/wrist that radiates to the forearm with no neck, shoulder, or elbow involvement [3]. This is an important distinction to rule out other possible pathologies such as a proximal entrapment, brachial plexopathy, or cervical radiculopathy. Patients may also report motor deficits such as dropping objects and difficulty holding objects [2]. All of these symptoms can be exacerbated by daily activities such as prolonged wrist extension/flexion or any repetitive wrist motions.
Following a clinical suspicion of carpal tunnel syndrome, an electrodiagnostic study can provide confirmation, determine severity, and evaluate for coexisting pathology [1]. Diagnostic imaging can be helpful for confirmation as well. Ultrasound is useful as it is safe, fast, and well tolerated [4]. Lastly an injection of corticosteroid and/or anesthetic into the carpal tunnel may assist in confirmation. This intervention is both diagnostic and therapeutic [1].
Differential Diagnosis
-
Median nerve entrapment at the elbow or more proximally (such as at the ligament of Struthers in the upper arm)
-
Brachial plexopathy
-
Cervical radiculopathy
-
Polyneuropathy or peripheral neuropathy
-
Arthritis (wrist, metacarpal thumb joint)
-
De Quervain’s tenosynovitis
-
Tendonitis of the flexor carpi radialis
Physical Exam
-
On examination, it is important to start with a careful inspection of the bilateral hands and wrists, making note of any atrophy (commonly of the thenar eminences or lumbricals) such as in Fig. 26.1. Look for any asymmetry in muscle bulk.

Atrophy of the thenar eminence (https://en.wikipedia.org/wiki/Carpal_tunnel_syndrome)
-
On the motor exam, weakness is most noticeably appreciated in thumb abduction and opposition [3]. There may also be weakness in the median innervated portion of the lumbricals and the flexor digitorum profundus [3, 5].
-
Sensory changes should follow median nerve distribution, which include the first, second, third, and the radial half of the fourth digit (Fig. 26.2). It is important to note that the palmar cutaneous branch, which innervates the palmar sensation, is spared as the branches proximal to the carpal tunnel. However, it may be difficult for patients to clearly describe areas of paresthesia, and many CTS patients do not present with the textbook distribution.

Cutaneous innervation of the hand. The median nerve distribution is shown in green (Source: Henry Gray [6])
-
Provocative tests
-
All of these tests are more specific than they are sensitive [1].
-
Phalen’s maneuver: patient places their wrists at a 90-degree flexion angle (Fig. 26.3). A positive Phalen’s reproduces the patient’s symptoms within 1 min, with an indication of more severe case if reproduced in under 10 s [5].
Fig. 26.3 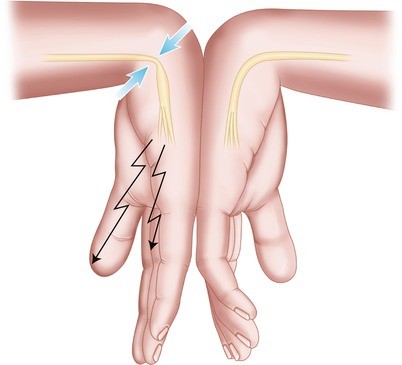
Phalen’s test (www.Imgarcade.com)
-

-
Reverse Phalen’s test (prayer test): similar to Phalen’s but the wrist is held in extension, which reproduces symptoms. This is more specific but less sensitive than Phalen’s [7].
-
Tinel’s sign can be elicited by tapping over the carpal tunnel, although even in unaffected individuals, this may produce paresthesias (Fig. 26.4). Comparison should be made with unaffected side.

Tinel’s sign (www.Imgarcade.com)
-
Median nerve compression test (Durkan test): constant pressure is applied over the carpal tunnel. Test is considered positive if symptoms are reproduced within 30 s [3].
Imaging
-
Ultrasound imaging of the wrist may show compression of the median nerve. On average, an unaffected median nerve will have a cross-sectional area of less than 9 mm. When entrapped in the carpal tunnel, the median area has been shown to increase distal to the site of compression [1, 4].
-
Wrist radiographs may be useful if a traumatic or degenerative cause is suspected [1].
Electrodiagnostics
-
Nerve conduction study.
-
The goal of this test is to show focal slowing or conduction block of the median nerve distal at the carpal tunnel as well as to rule out any more proximal involvement such as median neuropathy at the upper arm, brachial plexopathy, or radiculopathy.
-
Based on findings on nerve conduction study, the severity of CTS is graded using the Canterbury NCS scale [8].
-
-
Electromyography
-
To further assess chronicity and extent of involvement in specific muscles.
-
Electromyography may be normal in mild cases. In moderate to severe cases, EMG may demonstrate active denervation in the abductor pollicis brevis as well as large motor unit amplitudes, indicating chronic pathology.
-
Treatment
-
Conservative treatment is focused on maintaining function and slowing the progression of the disease. This includes relative rest, improved ergonomics, physical/occupational therapy (avoid aggressive strengthening until symptoms abate), and wrist splinting in neutral or five degrees of extension. Splinting is most effective if worn at all times. However, compliance is an obstacle so many patients wear the splints only at night [1].
-
In a recent trial comparing conservative versus surgical management for mild to moderate disease, conservative treatment provided better outcomes in the short term and equal outcomes in the long term [9].
-
Steroids have been shown to be efficacious with either oral prednisone or a corticosteroid injection into the carpal tunnel [1]. However, research has shown an increased improvement in symptoms when comparing injection to oral treatment. [10] Injections usually provide symptomatic relief within 24–48 h [1].
-
For severe cases, when electrodiagnostic testing clearly shows axonal median neuropathy at the wrist or when progression continues after conservative treatment has been tried, surgical decompression with transverse carpal ligament resection has been shown to halt further worsening of the disease. Both open and endoscopic methods are equally efficacious; however, endoscopy has shown slight improvement in postoperative pain and avoidance of a palmar scar [1].
When to Refer
-
Conservative treatment failure.
-
Worsening weakness and atrophy.
-
Functional loss.
-
Severe pain.
-
Significantly worse symptoms in the nondominant hand may indicate different etiology [2].
Referral
-
Physiatrist
-
Hand surgeon
-
Physical or occupational therapist
-
Rheumatologist if rheumatic cause is suspected
References
Frontera W. Essentials of physical medicine and rehabilitation. 2nd ed. Philadelphia: Saunders; 2008.
Braddom R. Physical medicine and rehabilitation. 2nd ed. Philadelphia: Saunders; 2000.
Preston D, Shapiro B. Electromyography and neuromuscular disorders clinical-electrophysiological correlations. 3rd ed. London: Elsevier Saunders; 2013.
Wiesler ER, Choloros GD, Cartwright MS, Smith BP, Rushing J, Walker FO. The use of diagnostic ultrasound in carpal tunnel syndrome. J Hand Surg Am. 2006;31:726–32.
Cuccurullo S. Physical medicine and rehabilitation board review. 2nd ed. New York: Demos Medical; 2010.
Henry Gray. Anatomy of the human body. Bartleby.com: Gray’s Anatomy, Plate 812; 1918. Public Domain.
Irvin M, Novak CB, Mackinnon SE, Winograd JM. Sensitivity and specificity of clinical testing for carpal tunnel syndrome. Can J Plast Surg. 2003;11(2):70–2.
The Canterbury NCS Severity Scale for CTS. Carpal-Tunnel.net, 20 Dec. 2011. Web. <http://www.carpal-tunnel.net/diagnosing/sevscale>. (n.d.)
Penas C F-d-l, Ortega-Santiago R, de la Llave-Rincón AI, Martínez-Perez A, Fahandezh-Saddi Díaz H, Martínez-Martín J, et al. Manual physical therapy versus surgery for carpal tunnel syndrome: a randomized parallel-group trial. J Pain. 2015;16(11):1087–94.
Wong SM, Hui AC, Tang A, Ho PC, Hung LK, Wong KS, et al. Local vs systemic corticosteroids in the treatment of carpal tunnel syndrome. Neurology. 2001;56(11):1565–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter

Cite this chapter
Andrews, R., Isaacson, A., Kanzer, D. (2017). Carpal Tunnel Syndrome. In: Kahn, S., Xu, R. (eds) Musculoskeletal Sports and Spine Disorders. Springer, Cham. https://doi.org/10.1007/978-3-319-50512-1_26
Download citation
DOI: https://doi.org/10.1007/978-3-319-50512-1_26
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-50510-7
Online ISBN: 978-3-319-50512-1
eBook Packages: MedicineMedicine (R0)