
Abstract
Multiple extraintestinal manifestations have been noted in pediatric inflammatory bowel disease (IBD) patients. IBD is a multisystem disease, and care for IBD patients has to factor in potential extraintestinal manifestations, especially since these can be the presenting symptoms of the patient’s disease and can cause substantial issues for patients. This chapter will describe the more common extraintestinal manifestations in pediatric IBD patients.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Extraintestinal manifestations
- Growth failure
- Ankylosing spondylitis
- Sacroiliitis
- Erythema nodosum
- Pyoderma gangrenosum
- Episcleritis
- Uveitis
Introduction
Inflammatory bowel disease (IBD) is not just a disorder of one organ system, but rather a multisystem disease. In addition to the more typical gastrointestinal involvement, which can present with symptoms such as abdominal pain, chronic diarrhea, or bloody stools, several other organs can be involved as well, including the eyes, skin, joints, kidneys, and liver. In fact, these extraintestinal manifestations may be the presenting symptoms and become the predominant source of morbidity for a given patient. These manifestations have been classified in various ways such as their relationship with the degree of inflammation of the underlying bowel disease or by the location of the bowel disease, for example, colonic versus small intestinal [1]. They can also be divided by whether or not they are a consequence of the IBD itself. Extraintestinal manifestations affecting the joints, skin, hepatobiliary system, and eye can be differentiated from those that are complications of the disease such as malabsorption leading to osteoporosis, growth issues, kidney stones, etc.
The pathogenesis of the extraintestinal manifestations, like the etiology of IBD, is unknown. However, possible hypotheses include abnormal immune self-recognition, antibody production against specific extraintestinal organs that cross-react with gastrointestinal antigens, and/or genetic susceptibility. It is postulated that the inflammatory response in patients with IBD leads to the inability of the intestine to act as a selective barrier. Hence, the uptake of bacterial products or dietary antigens can induce circulating immune complexes or a systemic inflammatory response [2]. Another theory involves the cross-reaction with a bacterial epitope leading to autoimmunity directed against an antigen shared among the intestine, skin, synovium, eye, and biliary system [3]. An autoimmune reaction to an isoform of tropomyosin, which is expressed in the eye (non-pigmented ciliary epithelium), skin (keratinocytes), joints (chondrocytes), biliary epithelium, and the gut, is speculated as the focal point for this theory [4]. Similarly, extraintestinal manifestations may share a common pathway with the bowel disease in that recruitment of mucosal memory and/or effector T cells to various tissues via the expression of endothelial adhesion molecules that are usually restricted to the gut may lead to destruction from the influx of inflammatory cells [5]. One mechanism does not explain all of the different extraintestinal symptoms described in IBD patients. This is supported by the lack of uniform response to treatment. For example, one-half of patients with Crohn disease had complete resolution of their extraintestinal manifestations with adalimumab treatment. There was a significant reduction in arthralgias, arthritis, oral aphthous ulcers, and erythema nodosum, but not ankylosing spondylitis, iritis, or uveitis [6].
There is a strong genetic influence on extraintestinal manifestations, with reports of 70% concordance between parent–child pairs and 83% concordance between siblings [7, 8]. The human leukocyte antigen (HLA) system is postulated as a link between IBD and certain extraintestinal manifestations, especially ocular and articular manifestations [7]. HLA-A2, -DR1, and -DQw5 are more commonly associated with extraintestinal comorbidities in Crohn disease. On the other hand, genotypes HLA-DRB1, -B27, and -B58 are linked with extraintestinal manifestations of ulcerative colitis. Primary sclerosing cholangitis as well as other autoimmune disorders (e.g. celiac disease, autoimmune hepatitis, myasthenia gravis) have been associated with IBD patients with haplotype HLA-B8/DR3, while HLA-B27 is reported in 50–80% of IBD patients with ankylosing spondylitis [4].
The incidence of developing any extraintestinal manifestation in IBD is estimated to be as high as 40% in predominately adult studies, and it can be the presenting symptom in one out of four patients with IBD [9, 10]. Two pediatric studies have shown similar rates. In a retrospective study of over 1,600 pediatric IBD patients, the incidence of extraintestinal manifestations was 29% at 15 years post diagnosis [11]. These complications were more common in older patients, and 6% of the patients had extraintestinal symptoms prior to diagnosis. In another prospective study of over 1,000 pediatric IBD patients, the incidence of extraintestinal manifestations was 28%, with the majority (87%) occurring in the first year after diagnosis [12]. Interestingly, patients with more severe disease had a higher likelihood of having an extraintestinal manifestation. Further, the presence of one extraintestinal manifestation confers a risk to develop other manifestations [10].
Over 130 extraintestinal manifestations have been reported in the literature associated with IBD, but fortunately, most of these are rare [13]. Several excellent comprehensive reviews are available on the extraintestinal manifestations of IBD [8, 13, 14, 15, 16, 17, 18, 19]. This chapter will focus on the more common extraintestinal manifestations found in the pediatric population and present them by the affected system and descending order of prevalence (Table 10.1).
Growth Failure
Extraintestinal manifestations of pediatric IBD patients cannot be discussed without first mentioning growth failure, which is estimated to occur in 30% of children with Crohn disease and in 5–10% of those with ulcerative colitis [9]. Children can present with an obvious lack of growth, such as a height below the 5th percentile for age, or growth changes can be more subtle with a gradual flattening of the child’s height velocity which is only evident upon plotting multiple height measurements on a growth chart and comparison to midparental height. Some children can have delays in bone maturation and pubertal development. It is important to not merely assume that growth failure is a consequence of gastrointestinal manifestations, as decreases in weight and height velocities can precede any clinical evidence of bowel disease [20]. Thus, the concept of viewing growth failure as an independent manifestation of IBD will help health care providers develop a higher index of suspicion for the diagnosis of IBD in children presenting in this manner, even if they do not have gastrointestinal complaints.
IBD-associated growth failure could be secondary to deficient nutrient intake, poor digestion and absorption, as well as increased metabolic demands; however, the most likely etiology remains chronic caloric insufficiency [21]. Unfortunately, certain treatments for IBD, such as chronic corticosteroids, can have deleterious effects on overall growth, and these need to be weighed against the detrimental effects of the inflammatory process on growth. In addition to the consideration of immunomodulator (such as 6-mercaptopurine/azathioprine or methotrexate) and tumor necrosis factor alpha (TNFα) antagonists earlier in the disease course of pediatric patients, administration of oral or enteral formula feedings should be considered to rehabilitate the growth-stunted patient. A more extensive review can be found in the chapter devoted to growth issues in pediatric IBD.
Joint Manifestations
Joint inflammation is a commonly seen extraintestinal manifestation of IBD in both adults and children, with arthritis or joint pain occurring in 16–33% of children with IBD [9, 22, 23]. Similar to most other extraintestinal manifestations, symptoms of joint inflammation may occur before or after the development of bowel disease. Besides joint inflammation, one in five pediatric patients report enthesitis, inflammation at the bony insertion sites of ligaments, tendons, and fascia [24]. Joint manifestations can be divided into an axial form (involvement of the axial spine and sacroiliac joints) and a peripheral form (involvement of larger joints such as the knees, ankles, hips, wrists, and elbows).
The axial form of joint involvement includes ankylosing spondylitis and sacroiliitis. Ankylosing spondylitis, which is associated with the HLA-B27 antigen, is more commonly associated with ulcerative colitis and occurs in less than 2% of IBD patients. Symptoms include back stiffness, pain, and eventually stooped posture as well as peripheral joint complaints. Almost all of these patients will have involvement in their sacroiliac joints. On the other hand, asymptomatic sacroiliitis is more common with an estimated incidence of 10–52% [7]. Sacroiliitis is rarely diagnosed, especially in the early stages, unless sought after with bone scans or noted on computed tomography enterography [25]. Isolated sacroiliitis seems not to be associated with HLA-B27 [4]. Asymptomatic HLA-B27 negative patients with normal spinal mobility do not require specific treatment. Though ankylosing spondylitis has been shown to respond to sulfasalazine in multiple double-blind studies, none of the studies addressed ankylosing spondylitis in IBD patients [26]. Small studies have demonstrated a role of TNFα antagonist therapy in patients with IBD and ankylosing spondylitis [23]. Physical therapy and an exercise program to stop the progression of any disability and deformity remain a mainstay of treatment as well.
Peripheral joint inflammation is most frequently reported with Crohn disease and is most typically associated with colonic inflammation, although it can also be associated with small bowel disease [7]. The patient usually presents with erythema, swelling, and decreased range of motion in an asymmetric pauciarticular pattern. Fortunately, joint deformity is uncommon. The arthritis tends to worsen during times of increasing bowel disease, and there is an association with other extraintestinal manifestations such as those of the skin, mouth, and ocular systems. In fact, patients with involvement of these systems can share serological markers such as elevations in antibody levels against exocrine pancreas compared to other IBD and non-IBD patients [27].
Primary treatment of the bowel inflammation with 5-aminosalicylate medications, corticosteroids, immunomodulating agents, or TNFα antagonists is the first course of action for peripheral joint inflammation [9]. Resolution is commonly achieved with this approach in <8 weeks [22]. Studies have shown that infliximab is efficacious in the treatment of spondyloarthropathies, such as the articular and musculoskeletal findings in IBD [7]. Treatments with non-steroidal anti-inflammatory agents and cyclooxygenase-2-inhibitors have the potential for gastrointestinal mucosal injury and should be avoided if possible. In refractory cases, consideration is given to methotrexate and intraarticular corticosteroid injections.
Bone Disease
There has been increasing interest in identifying osteopenia and osteoporosis in patients with IBD, especially given that IBD commonly presents during adolescence and young adulthood when bone mass is being rapidly attained. In adult populations, the overall prevalence of osteoporosis in IBD is estimated between 4 and 40%, with increasing prevalence in older patients [4]. A large population-based adult study reported an osteoporosis prevalence of 15% and relative risk of 1.4 for fractures in IBD patients compared to the general population [28]. Prevalence of osteopenia and osteoporosis in the pediatric population is estimated between 8 and 30%, based on several smaller studies [11, 29]. The increased risk of eventually developing osteoporosis in IBD patients, especially those with Crohn disease, is secondary to multiple factors, including inadequate intake or malabsorption of calcium and vitamin D, corticosteroid use, low estrogen states in females, and negative effects of circulating proinflammatory cytokines [30]. This osteoporosis can make the patients prone to bone fracture, bone deformities, and chronic pain.
Diagnosis of osteopenia/osteoporosis is made with dual-energy x-ray absorptiometry (DEXA), which measures bone mineral density in the spine, femoral neck, or other bones rapidly and with low amounts of radiation. Treatment with calcium and vitamin D may prevent further deterioration of bone, but not necessarily help in the recovery of lost bone density, though some pediatric studies have suggested bone recovery in children with IBD on treatments [31]. Prevention has not been well studied in IBD patients, but it would be prudent to ensure intake of at least the recommended daily requirement for age of calcium and vitamin D, proper exercise, and minimization of corticosteroid usage to maximize the pediatric patient’s potential in achieving an appropriate peak bone mass. The role of bone-protecting agents in IBD, especially pediatrics, is unknown so far.
Other bone complications in IBD patients include osteonecrosis of the femoral head, hypertrophic osteoarthropathy, and chronic recurrent multifocal osteomyelitis (CRMO). Osteonecrosis of the femoral head is usually associated with patients who have received chronic steroids and have complaints of hip or knee pain. Clubbing or hypertrophic osteoarthropathy is another bone manifestation associated with IBD, especially with small intestinal Crohn disease. The etiology, though unknown, is postulated to involve increased blood flow to the fingers, and hence increased connective tissue growth secondary to circulating cytokine production [7]. Chronic recurrent multifocal osteomyelitis (CRMO), rarely described in children with IBD, is an aseptic inflammatory bone disease that typically affects the long bones and clavicles [32].
Oral Lesions
Oral lesions can arise at anytime in patients with IBD and at any age, but they occur more commonly in children and are often independent of the intestinal disease severity [33]. Though the incidence can vary, the highest report rate was 48% in a pediatric age group study [34]. Recurrent aphthous lesions are the most common oral lesions associated with IBD, with a reported incidence of approximately 8–14% in pediatric IBD patients with higher rates in Crohn disease compared to ulcerative colitis [11–13]. Aphthous lesions tend to parallel intestinal disease, though they often can predate intestinal symptoms. Other oral lesions can consist of lip swelling, fissures, and gingivitis, which can demonstrate granulomas on histology [35]. Orofacial granulomatosis is a rare syndrome with chronic swelling of the lips and lower half of the face combined with oral ulcerations, and hyperplastic gingivitis that has been reported in three dozen Crohn cases [36]. Orofacial granulomatosis can be seen in other disorders such as foreign body reaction, tuberculosis, sarcoidosis, and idiopathic causes which share similar histopathological features [33]. Another rare disorder seen in association with ulcerative colitis patients is pyostomatitis vegetans which can present with oral and cutaneous findings in the axillae, genital areas, and scalp. The oral lesions consist of multiple neutrophil-filled and eosinophil-filled pustules on erythematous bases which can erode and fuse to form shallow ulcers that have been described as being “snail track” configuration [37]. Oral lesions in IBD patients could also be a result of nutritional deficiencies, specifically low levels of zinc, folic acid, niacin, and vitamin B-12 [33].
Treatment of oral lesions is usually reserved for those causing significant discomfort, and may involve topical, intralesional or systemic corticosteroids, dapsone, or preparations directed at the bowel disease including immunomodulators, TNFα antagonists, and thalidomide [33, 38].
Skin Lesions
Cutaneous manifestations of IBD can be classified into three principal groups: granulomatous, reactive, and secondary to nutritional deficiency. Granulomatous skin manifestations have the same histological features as the bowel disease and can include perianal and peristomal ulcers and fistulas, oral granulomatous ulcers, epidermolysis bullosa acquisita, and metastatic Crohn disease. The latter is a rare complication that manifests as subcutaneous nodules or ulcers mainly in the lower extremities, and occasionally can occur in the genital areas. It appears unrelated to bowel activity and can be treated successfully with corticosteroids, antibiotics, azathioprine, methotrexate, and infliximab [7].
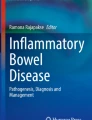
Of all the skin manifestations associated with IBD, erythema nodosum (Fig. 10.1) and pyoderma gangrenosum (Fig. 10.2) are the most common. In the pediatric patient, erythema nodosum, which is more commonly associated with Crohn disease than with ulcerative colitis, is encountered more frequently [9, 11]. Erythema nodosum presents as tender, subcutaneous, erythematous nodules, usually on the extremities, especially the lower legs, and the majority of patients with this skin manifestation will have associated joint pain or develop arthritis. Children may appear systemically ill with fever. Over days to weeks, the nodules will flatten, turn brown or gray, and can be mistaken for bruises. Histologically, erythema nodosum is a septal panniculitis consisting of a lymphohistiocytic infiltrate. The prevalence in all IBD patients, adult and pediatric, is estimated between 3% and 15% [28]. Exacerbations of erythema nodosum correlate most often with increased intestinal inflammation; hence, treatment toward the bowels is considered a primary form of management. Recent reports in children have shown good response to infliximab [39].

Erythema nodosum (Courtesy of Dr. Susan M. Rabizadeh)

Pyoderma gangrenosum (Courtesy of Dr. Rachel Nussbaum, Johns Hopkins University)
Pyoderma gangrenosum is an ulcerating lesion often correlating with exacerbations of the bowel disease. However, it can persist for long periods, while the intestinal inflammation is clinically quiescent. Fortunately, it is relatively rare with a reported incidence of 2% in UC patients and a smaller number in Crohn patients [39]. The lesions are often painful and located on the lower extremities. Histopathology reveals endothelial injury with fibrinoid necrosis of blood vessels and marked neutrophilic and lymphocytic infiltrates. Treatment is difficult, and patients may require large doses of systemic corticosteroids or immunomodulators as well as topical ulcer care. Infliximab has shown to be effective in refractory cases; however, some extreme cases might require grafting [7, 39].
Sweet’s syndrome is another very rare reactive cutaneous disorder associated with IBD. It is a neutrophilic dermatosis presenting with painful erythematous plaques or nodules often associated with fever and leukocytosis. Usually, there is good response to corticosteroids, and a study has demonstrated benefit of cyclophosphamide in steroid refractory patients [40].
Psoriasis is seen commonly in patients with IBD [41]. In addition, therapy-related psoriasiform skin lesions have been reported in patients undergoing TNFα antagonist therapy. Anti-IL-12/IL-23 therapy may have a role in the treatment of these patients from an intestinal and skin standpoint [41].
Nutritional issues, such as trace mineral and vitamin deficiencies, occur in children with IBD, especially Crohn disease; however, skin disorders secondary to these are unusual. There are rare reported cases of acrodermatitis enteropathica, pellagra, and scurvy, secondary to zinc, niacin, and vitamin C deficiency, respectively.
Vulvar lesions have also been associated with IBD in patients presenting with vulvar ulcers, labial swelling, exophytic lesions, condylomatous lesions, and abnormalities on pap smear. Most often, the histopathology demonstrates noncaseating vulvar granulomas, but dysplasia and carcinoma have also been reported [42].
Eye Lesions
The most common eye manifestations of IBD are episcleritis and uveitis [9]. These are often associated with other extraintestinal manifestations, especially arthritis and erythema nodosum. Episcleritis (Fig. 10.3), inflammation of the blood-rich episclera, tends to parallel bowel activity and is often confused with conjunctivitis as the patients present with eye redness and burning. Episcleritis does not impair vision and usually responds clinically to topical corticosteroids. If visual impairment is present, the possibility of scleritis, which can occur with protracted intestinal disease, needs to be considered, and an emergent evaluation by an ophthalmologist is required to evaluate for retinal detachment or optic nerve swelling.

Episcleritis (Courtesy of Dr. Rachel Nussbaum, Johns Hopkins University)
Uveitis, unlike episcleritis, is usually independent of the bowel activity and inflammation. Anterior uveitis involves inflammation of the iris and the ciliary body. Symptoms can include acute or subacute eye pain, headache, photophobia, and blurred vision, or occasionally decreased vision; however, many patients may be asymptomatic. Complications of uveitis can be serious and include iris atrophy, synechiae, pigment deposits, glaucoma, cataracts, and permanent visual deficits. Attention must be paid for early signs of uveitis, which can include a cellular or proteinaceous exudate of inflammatory cells in the anterior chamber of the eye. An evaluation of 147 children with IBD who had no ophthalmological complaints revealed a prevalence of uveitis of 6.1% in patients with Crohn disease [43]. Like scleritis, acute anterior uveitis is an ophthalmological emergency. Treatment involves covering the eye to reduce pain and photophobia, pupillary dilatation, and the use of topical or systemic corticosteroids.
Liver Disease
Liver pathology, including hepatitis, fatty liver, cholelithiasis, amyloidosis, and primary sclerosing cholangitis, is found in <5–10% of patients with IBD [9, 11]. Screening with periodic checks of serum aminotransferases, alkaline phosphatase, gamma glutamyltransferase, and bilirubin is necessary, as many of the children with liver disease are asymptomatic. A more extensive review of this extraintestinal manifestation can be found in another chapter devoted to liver disease in pediatric IBD.
Hematological Abnormalities
Anemia, thrombocytosis, and leukocytosis are common hematological abnormalities in IBD patients and can be seen in up to half the patients with active disease [9]. Usually, the anemia is secondary to iron, vitamin B12, and folic acid deficiency, as well as anemia of chronic disease. The thrombocytosis is postulated to result from circulating inflammatory cytokines that stimulate platelet production. Similarly, leukocytosis can occur as a result of generalized inflammation. On the other hand, patients should be monitored for leukopenia with certain therapies such as use of thiopurine immunomodulators (e.g. 6-mercatopurine or azathioprine) or methotrexate. Further information can be found in the laboratory evaluation in pediatric IBD chapter.
Other Extraintestinal Manifestations
Many other systems, listed below, have had reported involvement in IBD, but they have been reported to occur in <1% of pediatric IBD patients [9].
Vascular
Patients with IBD have been reported to have a threefold increased risk of venous thrombosis compared to matched controls [44]. Interestingly, this increased risk is specific for IBD, as it is not seen with other inflammatory conditions such as rheumatoid arthritis or other bowel disorders such as celiac disease. Deep venous thrombosis and pulmonary embolism are the most common complications resulting from an overall increased coagulation. Coagulation factors may be elevated as part of an acute phase response. Factor V Leiden, a genetic disorder characterized by an impaired anticoagulant response to protein C leading to a prothrombotic state, may be increased in Crohn disease patients [44]. Furthermore, IBD patients might have higher levels of homocysteine, which can be a potential cause of thrombosis [44]. Another vascular complication, arteritis of small or large vessels, has been reported in children with IBD [45].
Pancreatitis
The incidence of pancreatic involvement in IBD varies but is estimated to be 0.7–1.6% in children [46]. The most likely etiologies are medications, anatomical, immunological, or gallstones secondary to ileal disease. Although patients with IBD appear to have a small increased risk for idiopathic pancreatitis, the most common cause of pancreatitis in IBD appears to be associated with medications such as 5-aminosalicylate preparations or 6-mercaptopurine. As this is presumed to be an idiosyncratic reaction, discontinuation of the medication is indicated. Although pancreatic autoantibodies have been found in up to 40% of Crohn disease patients, their significance remains unclear. In one series, patients with Crohn disease who were pancreatic antibody-positive had a higher rate of pancreatic exocrine insufficiency than those who were antibody-negative [4]. Furthermore, chronic pancreatitis has also been reported in a series of six adult IBD patients, five of whom had changes on pancreatic pathology samples [47].
Renal
IBD patients, especially those with extensive ileal disease or ileal resection with significant fat malabsorption or fluid losses, are at risk for developing calcium oxalate and uric acid stones. Glomerulonephritis with immune complex deposition can also be seen which can progress to severe renal disease. Other renal diseases, described in children with IBD, include renal artery stenosis, amyloidosis leading to renal failure, ureteral compression, and perinephritic abscesses secondary to abscesses, or inflammation surrounding the terminal ileum [48].
Pulmonary
Pulmonary manifestations associated with IBD are reported less frequently in children than adults, though the scope of disorders is similar. Reactive airway disease, bronchitis, bronchiectasis, tracheal obstruction, granulomatous lung disease, interstitial or hypersensitivity pneumonitis, and bronchiolitis obliterans are being reported at an increasing frequency [4, 9, 49–51]. However, the latter two have been associated with 5-aminosalicylate products and methotrexate treatment [4, 51]. Similar to other extraintestinal manifestations, pulmonary disease can predate the bowel disease by months or years. Most pulmonary manifestations respond to corticosteroids via an inhaled, oral, or intravenous route.
Neurological
Peripheral nerve disorders, cardiovascular disorders, myopathy, multiple sclerosis, optic neuritis, and epilepsy have been described in IBD patients [52]. Peripheral neuropathies are the most common neurological disorders reported, while cardiovascular disorders with neurological morbidities have been documented in up to 4% of patients [53]. A retrospective cross-sectional study of adult patients with IBD reported an odds ratio of 1.67 for developing multiple sclerosis, optic neuritis, or a demyelinating disorder [4]. An interesting future focus will center around the role of medication treatments for IBD and neurological adverse events especially given the risk of progressive multifocal leukoencephalopathy related to the anti-alpha 4 integrin antibody natalizumab.
Cardiac
Rarely, children with IBD can develop myopericarditis and pleuropericarditis with symptoms of chest pain and dyspnea. Cardiac manifestations are not necessarily associated with active bowel disease and respond to corticosteroids and nonsteroidal anti-inflammatory agents, which need to be used with caution in IBD patients. An active area of research is the risk of cardiovascular events in patients with IBD. A recent study showed an increased incidence in coronary artery disease in adults with IBD [54]. Interestingly, the IBD patients had significantly lower rates of traditional coronary artery disease risk factors such as hypertension, diabetes, obesity, and dyslipidemia. Further work will help determine the affect of various treatments on decreasing risk of cardiac disease.
Summary
Given that Crohn disease and ulcerative colitis are associated with numerous extraintestinal manifestations, it is clearly evident that IBD is a multisystem disease that stretches beyond the gastrointestinal tract. Knowledge about extraintestinal manifestations is critical, as patients can present with these instead of more classic bowel symptoms. Furthermore, the extraintestinal manifestations of IBD can be a cause of major morbidity in patients and need to be considered and addressed at all points of care.
References
Lichtman SN, Sartor RB. Extraintestinal manifestations of inflammatory bowel disease: clinical aspects and natural history. In: Targan S, Shanahan F, editors. Inflammatory bowel disease: from bench to bedside. Baltimore: Williams & Wilkins; 1994.
Levine JB, Lukawski-Trubish D. Extraintestinal considerations in inflammatory bowel disease. Gastroenterol Clin North Am. 1995;24:633.
Bhagat S, Das KM. A shared and unique peptide in the human colon, eye, and joint detected by a monoclonal antibody. Gastroenterology. 1994;107:103.
Rothfuss KS, Stange EF, Herrlinger KR. Extraintestinal manifestations and complications in inflammatory bowel disease. World J Gastroenterol. 2006;12:4819.
Adams DH, Eksteen B. Aberrant homing of mucosal T cells and extra-intestinal manifestations of inflammatory bowel disease. Nat Rev Immunol. 2006;6:244.
Lofberg R, Louis EV, Reinish W, Robinson AM, Kron M, Camez A, Pollack PF. Adalimumab produces clinical remission and reduces extraintestinal manifestations in Crohn disease: results from CARE. Inflamm Bowel Dis. 2012;18:1–9.
Danese S, Semeraro S, Papa A, Roberto I, Scaldaferri F, Fedeli G, Gasbarrini G, Gasbarrini A. Extraintestinal manifestations in inflammatory bowel disease. World J Gastroenterol. 2005;11:7227.
Vavricka S, Schoepfer A, Scharl M, Lakatos PL, Navarini A, Rogler G. Extraintestinal manifestations of inflammatory bowel disease. Inflamm Bowel Dis. 2015;21:1982–92.
Oliva-Hemker M. More than a gut reaction: extraintestinal complications of IBD. Contemp Pediatr. 1999;16:45.
Vavricka SR, Brun L, Ballabeni P, Pittet V, Vavricka BMP, Zeitz J, Rogler G, Schoepfer AM, Swiss IBD Cohort Study Group. Frequency and risk factors for extraintestinal manifestations in the Swiss inflammatory bowel disease cohort. Am J Gastroenterol. 2011;106:110–9.
Jose FA, Garnett EA, Vittinghoff E, Ferry GD, Winter HS, Baldassano RN, Kirschner BS, Cohen SA, Gold BD, Abramson O, Heyman MB. Development of extraintestinal manifestations in pediatric patients with inflammatory bowel disease. Inflamm Bowel Dis. 2009;15:63–8.
Dotson JL, Hyams JS, Markowitz J, LeLeiko NS, Mack DR, Evans JS, Pfefferkorn MD, Griffiths AM, Otley AR, Bousvaros A, Kugathasan S, Rosh JR, Keljo D, Carvalho RS, Tomer G, Mamula P, Kay MH, Kerzner B, Oliva-Hemker M, Langton CR, Crandall W. Extraintestinal manifestations of pediatric inflammatory bowel disease and their relation to disease type and severity. JPGN. 2010;51:140–5.
Hyams JS. Extraintestinal manifestations of inflammatory bowel disease in children. J Pediatr Gastroenterol Nutr. 1994;19:7.
Kethu SR. Extraintestinal manifestations of inflammatory bowel disease. J Clin Gastroenterol. 2006;40:467.
Urlep D, Mamula P, Baldassano R. Extraintestinal manifestations of inflammatory bowel disease. Minerva Gastroenterol Dietol. 2005;51:147.
Loftus EV. Management of extraintestinal manifestations and other complications of inflammatory bowel disease. Curr Gastroenterol Rep. 2004;6:506.
Hoffmann RM, Kruis W. Rare extraintestinal manifestations of inflammatory bowel disease. Inflamm Bowel Dis. 2004;10:140.
Su CG, Judge TA, Lichtenstein GR. Extraintestinal manifestations of inflammatory bowel disease. Gastroenterol Clin North Am. 2002;31:307.
Jose FA, Heyman MB. Extraintestinal manifestations of inflammatory bowel disease. JPGN. 2008;46:124–33.
Kanof ME, Lake AM, Bayles TM. Decreased height velocity in children and adolescents before the diagnosis of Crohn disease. Gastroenterology. 1988;95:1523.
Conklin LS, Oliva-Hemker M. Nutritional considerations in pediatric inflammatory bowel disease. Expert Rev Gastroenterol Hepatol. 2010;4:305–17.
Passo MH, Fitzgerald JF, Brandt KD. Arthritis associated with inflammatory bowel disease in children—relationship of joint disease to activity and severity of bowel lesion. Dig Dis Sci. 1986;31:492.
Cardile S, Romana C. Current issues in pediatric inflammatory bowel disease-associated arthropathies. World J Gastroenterol. 2014;20(1):45–52.
Horton DB, Sherry DD, Baldassano RN, Weiss PF. Enthesitis is an extraintestinal manifestation of pediatric inflammatory bowel disease. Ann Paediatr Rheumatol. 2012;1(4):214–21.
Paparo F, Bacigalupo L, Garello I, Biscaldi E, Cimmino MA, Marinaro E, Rollandi GA. Crohn disease: prevalence of intestinal and extraintestinal manifestations detected by computed tomography enterography with water enema. Abdom Imaging. 2012;37(3):326–37.
Juillerat P, Mottet C, Froehlich F, Felley C, Vader J, Burnand B, Gonvers J, Michetti P. Extraintestinal manifestations of Crohn disease. Digestion. 2005;71:31–6.
Lakatos PL, Altorjay I, Szamosi T, Palatka K, Vitalis Z, Tumpek J, Sipka S, Udvardy M, Dinya T, Lakatos L, Kovacs A, Molnar T, Tulassay Z, Miheller P, Barta Z, Stocker W, Papp J, Veres G, Papp M, Hungarian IBD Study Group. Pancreatic autoantibodies are associated with reactivity to microbial antibodies, penetrating disease behavior, perianal disease, and extraintestinal manifestations, but not with NOD2/CARD15 or TLR4 genotype in a Hungarian IBD cohort. Inflamm Bowel Dis. 2009;15:365–74.
Bernstein CN. Osteoporosis and other complications of inflammatory bowel disease. Curr Opin Gastroenterol. 2002;18:428.
Gokhale R, Favus MJ, Karrison T, et al. Bone mineral density assessment in children with inflammatory bowel disease. Gastroenterology. 1998;114:902.
Hyams JS, Wyzga N, Kreutzer DL, et al. Alterations in bone metabolism in children with inflammatory bowel disease: an in vitro study. J Pediatr Gastroenterol Nutr. 1997;24:289.
Gasparetto M, Guariso G. Crohn’s disease and growth deficiency in children and adolescents. World J Gastroenterol. 2014;20(37):13219–33.
Bousvaros A, Marcon M, Treem W, Waters P, Issenman R, Couper R, Burnell R, Rosenberg A, Rabinovish E, Kirschner B. Chronic recurrent multifocal osteomyelitis associated with chronic inflammatory bowel disease in children. Dig Dis Sci. 1999;44:2500–7.
Fatahzadeh M, Schwartz RA, Kapila R, Rochford C. Orofacial Crohn disease: an oral enigma. Acta Dermatoveneral Croat. 2009;17:289–300.
Lankarani KB, Sivandzadeh GR, Hassanpour S. Oral manifestation in inflammatory bowel disease: a review. World J Gastroenterol. 2013;19(46):8571–9.
Plauth M, Jenss H, Meyle J. Oral manifestations of Crohn disease. J Clin Gastroenterol. 1991;13:29.
Grilich C, Bogenrieder T, Palitzsch KD, Scholmerich J, Lock G. Orofacial granulomatosis as initial manifestation of Crohn disease: a report of two cases. Eur J Gastroenterol Hepatol. 2002;13:873–6.
Storwick GS, Prihoda MB, Fulton RJ, et al. Pyodermatitis-pyostomatitis vegetans: a specific marker for inflammatory bowel disease. J Am Acad Dermatol. 1994;31:336.
Lynde CB, Brue AJ, Rogers RS. Successful treatment of complex aphthous with colchicine and dapsone. Arch Dermatol. 2009;145:273–6.
Kugathasan S, Miranda A, Nocton J, Drolet BA, Raasch C, Binion DG. Dermatologic manifestations of Crohn disease in children: response to infliximab. J Pediatr Gastroenterol Nutr. 2003;37:150–4.
Meinhardt C, Buning J, Fellermann K, Lehnert H, Schmidt KJ. Cyclophosphamide therapy in Sweet’s syndrome complicating refractory Crohn disease – efficacy and mechanism of action. J Crohns Colitis. 2011;6:633–7.
Hagen JW, Swoger JM, Grandinetti LM. Cutaneous manifestations of Crohn disease. Dermatol Clin. 2015;33:417–31.
Foo WC, Papalas JA, Robboy SJ, Selim MA. Vulvar manifestations of Crohn disease. Am J Dermatopathol. 2011;33:588–93.
Hofley P, Roarty J, McGinnity G, et al. Asymptomatic uveitis in children with chronic inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 1993;17:397.
Purnak T, Yuksel O. Overview of venous thrombosis in inflammatory bowel disease. Inflamm Bowel Dis. 2015;21:1195–203.
Mader R, Segol O, Adawi M, Trougoboff P, Nussinson E. Arthritis or vasculitis as presenting symptoms of Crohn disease. Rheumatol Int. 2005;25:401–5.
Cardile S, Randazzo A, Valenti S, Romano C. Pancreatic involvement in pediatric inflammatory bowel diseases. World J Pediatr. 2015;11(3):207–11.
Barthet M, Hastier P, Bernard JP, et al. Chronic pancreatitis and inflammatory bowel disease: true or coincidental association? Am J Gastroenterol. 1999;94:2141–8.
Kuzmic AC, Kolacek S, Brkljacic B, Juzjak N. Renal artery stenosis associated with Crohn disease. Pediatr Nephrol. 2001;16:371–3.
Camus P, Piard F, Ashcroft T, et al. The lung in inflammatory bowel disease. Medicine. 1993;72:151.
Al-Binali AM, Scott B, Al-Garni A, Montgomery M, Robertson M. Granulomatous pulmonary disease in a child: an unusual presentation of Crohn disease. Pediatr Pulmonol. 2003;36:76–80.
Haralambou G, Teirstein AS, Gil J, Present D. Bronchiolitis obliterans in a patient with ulcerative colitis receiving mesalamine. Mt Sinai J Med. 2001;68:384–8.
Lossos A, River Y, Eliakim A, et al. Neurologic aspects of inflammatory bowel disease. Neurology. 1995;45:416.
Zois CD, Katsanos KH, Kosmidou M, Tsianos EV. Neurologic manifestations in inflammatory bowel disease: current knowledge and novel insights. J Crohns Colitis. 2010;4:115–24.
Yarur AJ, Deshpande AR, Pechman DM, Tamariz L, Abreu MT. Inflammatory bowel disease is associated with an increased incidence of cardiovascular events. Am J Gastroenterol. 2011;106:741–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Rabizadeh, S., Oliva-Hemker, M. (2017). Extraintestinal Manifestations of Pediatric Inflammatory Bowel Disease. In: Mamula, P., Grossman, A., Baldassano, R., Kelsen, J., Markowitz, J. (eds) Pediatric Inflammatory Bowel Disease. Springer, Cham. https://doi.org/10.1007/978-3-319-49215-5_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-49215-5_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-49213-1
Online ISBN: 978-3-319-49215-5
eBook Packages: MedicineMedicine (R0)