
Abstract
This chapter describes the two main disease entities affecting the spinal cord vasculature, spinal cord ischemia, and spinal vascular malformation.
Spinal cord ischemia differs significantly from cerebral ischemia patients in terms of age, clinical presentation and course, risk factors, and underlying pathology. Clinical severity depends on the lesion extent and the lesion level. Recovery is most often incomplete and about 50 % of patients remain wheelchair bound. The etiology of spinal cord ischemia can be divided into three entities, all of which have different diagnostic algorithms, different preventive, acute/rehabilitative strategies and different outcomes: (a) spontaneous, (b) complication of an underlying acute disease, and (c) complication of aortic diagnostic/therapeutic procedures. Spontaneous spinal cord ischemia is often attributed to the typical cerebral ischemia risk factors. However, diagnostic workup needs to be broader including underlying inflammatory causes (infectious, parainfectious, autoimmune). At the same time, diagnostic imaging in the acute phase is more challenging compared to cerebral ischemia, which hampers efforts for acute therapeutic interventions such as thrombolysis. As further treatment option, in particular after aortic surgery, lowering of the intraspinal pressure by lumbar drainage to increase intraspinal perfusion pressure can be considered.
In most instances, spinal vascular malformations consisting of spinal dural arteriovenous fistulas, arteriovenous malformations, and cavernous angiomas cause a more slowly progressive disease manifestation as opposed to the sudden onset in spinal cord ischemia. The underlying pathophysiological mechanism is based on arterial blood shunted into perimedullar veins, which causes venous congestion in the spinal cord parenchyma. Depending on the type of malformation, effective neurosurgical and interventional treatment options are available. The prognosis heavily depends on an early diagnosis and treatment, which may allow to at least partially reverse neurological dysfunction.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Both spinal cord ischemia and spinal vascular malformation are considered rare diseases. In case of spinal cord ischemia, exact epidemiological numbers are missing. According to the literature, spinal cord ischemia accounts for 1 % of all ischemic events within the central nervous system. In Germany, 196,000 first-ever ischemic strokes occur every year [1]. Based on this number, almost 2000 cases each year would suffer from spinal cord injury. Considering that the most frequent cause of para- or tetraplegia – traumatic spinal cord injury – already accounts for roughly 2000 new cases each year in Germany suggests that the incidence of spinal cord ischemia is much lower. However, exact numbers are missing. Likewise, the exact incidence of spinal vascular malformations is unknown. In various publications, the incidence for spinal dural arteriovenous fistulas, the most common type of spinal vascular malformation, is reported between five and ten cases per one million. The source for this estimate cannot be confirmed.
2 Vascularization
Knowledge about the arterial supply of the spinal cord is still far from being complete. Due to the small diameters of respective vessels (maximum diameter in the artery of Adamkiewicz is 1.2 mm; all other vessels are mostly in the range between 0.1 and 0.8 mm), precise in vivo studies are difficult. Most of our current knowledge related to spinal cord vascular supply is based on postmortem studies after microinjections of staining fluids and microradiological assessments [2].
During embryonic development the anterior spinal artery develops from the anastomosis of ascending and descending branches of 31 bilateral segmental anterior radicular arteries. In the adult, the majority of these segmental feeders of anterior spinal artery obliterate. Only around 6 of these feeders remain in the adult. Around 2–3 radicular arteries can be found at cervical level, 2–3 at thoracic level, and 0–1 at the lumbosacral level [2] (see chapter 2).
The vast collateral vascular network around and within the spinal cord – despite the fact that during development the majority of segmental arteries are obliterated – accounts for the rare incidence of ischemic events within the spinal cord. More recent studies in pigs clearly indicate the presence of a robust collateral network, which helps to maintain spinal cord perfusion even after interruption of relevant segmental arteries [3]. After infusion of acrylic resin and subsequent curing of the resin, the selectively visualized spinal vasculature shows extensive collaterals between the segmental arteries feeding into the anterior spinal artery on the one hand and vastly interconnecting vessels outside the spinal canal supplying the erector spinae, iliopsoas, and associated muscle vasculature posteriorly on the other hand. Moreover, multiple longitudinal anastomoses along the vertebral column exist, which receive additional supply from the subclavian artery rostrally and the hypogastric arteries caudally [4]. According to the literature, such a comparably robust collateral vascular network exists in humans [3]. The rather few vessels providing spinal cord perfusion anteriorly versus the robust vessel network for the paraspinal muscles suggest that paraspinal muscle activity can impose a steal effect and thus threaten spinal cord perfusion.
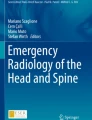
The ventrally located anterior spinal artery and two posterior spinal arteries directly supply the spinal cord (Fig. 5.1). Along the length of the spine, these vessels receive input from the subclavian artery via the vertebral artery, the thyrocervical trunk, and the costocervical trunk. Furthermore, several segmental arteries from the intercostal arteries and the lumbar artery containing the arteria radicularis magna (artery of Adamkiewicz) feed into the spinal cord vasculature (Fig. 5.2). More caudally, the hypogastric arteries support the spinal cord through the lateral sacral and iliolumbar arteries. The artery of Adamkiewicz arises on the left side of the aorta between the T9 and L1 segments, to anastomose with the anterior spinal artery. The artery of Adamkiewicz is typically cranially oriented due to cranial movement of the spinal cord against the vertebral column. Once at the cord surface, the artery of Adamkiewicz branches into a small ascending vessel and a large caudally oriented vessel, which gets formed after a hairpin curve of the artery of Adamkiewicz. It supplies the lower two thirds of the spinal cord. Posterior spinal arteries supply the dorsal third of the spinal cord – mainly the dorsal columns. Central arteries provide the vascular supply ventrally in a centrifugal pattern (central system), whereas the pial plexus feeds into the cord into a centripetal fashion supplying more superficial and dorsal regions of the spinal cord (peripheral system). The pial plexus forms an efficient anastomosis between the anterior and posterior circulation along the entire length of the spinal cord. Intercostal arteries reach the spine via an anterior and posterior radicular artery. The anterior radicular artery divides into an ascending and descending anterior spinal artery. Therefore, the anterior spinal artery represents an anastomotic channel between ascending and descending branches of neighboring anterior radicular arteries [2]. One should keep in mind that only in few instances do the anterior and posterior radicular arteries pass the dura to reach the surface of the medulla. Most of the feeding radicular arteries become obliterated during development.

Vascularization of the spinal cord: The main blood supply for the lower thoracic and lumbar spinal cord is derived from the Adamkiewicz artery feeding into the anterior spinal artery (ASA) [31]. The dorsal one third of the spinal cord receives blood supply through the posterior spinal arteries (PSA). The central arteries (central a.) provide the central vascular supply to the ventral horn, anterior portion of the dorsal horn and dorsal columns, the inner half of the anterior and lateral columns, and base of the dorsal columns in a centrifugal pattern. The pial arterial plexus (pial a. plexus, peripheral system) supplies the outer portion of the anterior and lateral columns and the posterior portion of the dorsal horn and dorsal columns in a centripetal fashion (Figure used with kind permission from Nicholas Theodore, M.D.)

Longitudinal organization of arterial blood supply in the spinal cord. Segmental arteries (segmental a.) derived from the aorta reach the spinal cord surface and form the anterior spinal artery (ASA) [31]. The largest segmental artery, typically located between the L1 and L2 level on the left, is termed great radicular artery or artery of Adamkiewicz (Adamkiewicz a.). Central artery (central a.), posterior spinal artery (PSA) (Figure used with kind permission from Nicholas Theodore, M.D.)
The venous system is divided into intrinsic and extrinsic systems. The intrinsic veins are divided into sulcal and radial veins, and the extrinsic veins consist of the anterior and posterior spinal veins. The anterior median spinal vein follows the anterior spinal artery and continues to the filum terminale vein. One posterior median vein, the greatest spinal vein, is accompanied by two posterolateral veins.
The extrinsic system is in contact with the spinal pia mater and includes the pial venous network, the longitudinal collectors, and the radicular veins. This configuration produces large lateral and dorsoventral anastomotic systems. Spinal veins drain into the anterior and posterior radiculomedullary veins, which in turn drain into the paravertebral and intervertebral plexuses. These venous plexuses drain into the segmental veins, draining into the ascending lumbar veins, azygos system, and pelvic venous plexuses.
3 Spinal Cord Ischemia
Spinal cord ischemia accounts for 5–8 % of all acute myelopathies [5] and 1–2 % of all ischemic events within the central nervous system [6].
Pathophysiology
Acute cerebral ischemias are most often caused by either atherosclerotic plaques, cardiac, or arterio-arterial embolism. The situation in the spinal cord is different. Here main causes are pathologies and interventions related to the aorta. Furthermore, infection leading to epidural thrombosis with secondary spinal cord infarction, hypercoagulable state, vasculitis (panarteritis nodosa, antiphospholipid antibody syndrome, systemic lupus erythematosus), epidural transforaminal injections, and cocaine consumption can induce spinal cord ischemia. Degenerative spine disease, for example, a vertebral disk, can directly compress a radicular artery [7]. Alternatively, material from the disk can enter the vascular system and cause so-called fibrocartilage embolism, which has been confirmed histologically. In children and young adults, spinal ischemia following scoliosis surgery has been reported. There it is most likely to be caused by traction movement of the spine. A confirmed cause is surgical occlusion of segmental arteries in the course of scoliosis surgery [8]. Nevertheless, the incidence seems to be low despite frequent occlusion of segmental arteries during respective surgeries. A retrospective study of 1090 patients undergoing corrective spinal deformity surgery reported only four cases with neurological deficits, which were attributed to vascular insufficiency due to vessel ligation [9]. Hyperextension of the thoracic spinal cord has been proposed as a mechanism to cause compression with consecutive occlusion and/or vasospasm and as a result spinal cord infarction in so-called surfer’s myelopathy. Quite a number of cases have been reported, typically novice surfers lying and paddling on the board in a supine position for prolonged periods of time [10].
Severe hypotension, cardiac arrest, or, rarely, spinal venous pathology preceding transient ischemic attacks affecting the spinal cord are rare.
Most of spinal cord ischemias are related to therapeutic interventions – either open repair of descending thoracic aortic pathologies or thoracic endovascular aortic repair (TEVAR) – to invasively repair aortic dissection or aneurysm. The incidence of spinal cord ischemia appears to be slightly lower with open repair strategies (between 3 and 15 %), most likely promoted by aortic cross-clamping, reperfusion injury, and acute hemodynamic changes [11]. The incidence of spinal cord following TEVAR varies widely. A recent retrospective monocentric analysis [12] from an established center reports an incidence of spinal cord ischemia following TEVAR as high as 31 % (total of 72 patients). Looking only at cases, where proper peri- and postoperative preventive measures were implemented (maintaining sufficient blood pressure, CSF drainage), the incidence decreased to almost 24 %. In contrast, in a meta-analysis of more than 4000 patients undergoing TEVAR, the rate of spinal cord ischemia was reported as low as 3.9 % [13]. A retrospective analysis of 424 patients undergoing TEVAR revealed a total of 12 patients (2.8 %) suffering from spinal cord ischemia [11]. Onset of ischemia was usually delayed by 10.6 h with a single case showing a paraparesis roughly 10 days after the intervention. The delayed onset of spinal cord ischemia has been attributed to postoperative hypotension, thrombosis, hematoma, embolization, and elevated CSF pressure. Of note, half of the spinal cord ischemia patients had previous open or endovascular aortic repair. As independent risk factors to develop ischemia, chronic renal insufficiency and extent C endovascular coverage (entire descending thoracic aorta from the left subclavian artery to the diaphragm) were identified. Means to raise spinal cord perfusion, before or after symptoms of spinal cord ischemia became apparent (raising arterial blood pressure, lumbar drainage to reduce cerebrospinal fluid pressure), were suggested to ameliorate neurological deficits and to contribute to more substantial recovery in the long term. Surprisingly, 9 out of 12 patients completely recovered from paraparesis (incomplete sensorimotor deficits), whereas 3 out of 12 patient at least incompletely recovered from paraplegia. Only one patient did not recover at all.
Based on the pattern of spinal cord infarction, defined etiologies have been suggested in a case series of 27 spontaneously occurring spinal cord ischemias [14]. Their mean age was 56 years with 11 men and 16 women. They were divided in an anterior, posterior spinal artery pattern, central or transverse manifestations. Concomitant infarction of the vertebral body was observed in one patient. The manifestation typically occurred within minutes up to several hours and was preceded only in two cases by transient ischemic attack (TIA)-like symptoms. Back or neck pain was observed in two thirds of the patients. The authors propose that arterial hypotension causes a central all the way up to a transverse spinal cord lesion pattern. On the other hand, anterior or posterior unilateral or bilateral infarctions are likely caused by mechanical affection of their corresponding vessel – the radicular arteries. This was based on the coincidence of “mechanical factors” referred to as “spine disease.” 75 % of the patients with anterior or posterior infarcts displayed disk pathology (protrusion) coinciding frequently with the infarct region. Respective mechanical factors can be aggravated by movement of the spine, preceding the occurrence of infarction in a number of patients with anterior/posterior infarction pattern. Of course, fibrocartilage embolism, as described by a number of case reports, and confirmed postmortem histologically cannot be excluded as an underlying mechanism. Overall, recovery in this series of spontaneous spinal cord ischemia cases was remarkably positive with complete or incomplete recovery in 70 % of the patients. In comparison, retrospective studies with spinal cord ischemia patients induced by aortic pathology (with or without surgery) revealed that at least 50 % of the patients showed an unfavorable outcome with permanent wheelchair dependency [5].
Diagnostics
MRI represents the gold standard to visualize ischemic changes. Nevertheless, MRI of the spinal cord can be rather challenging, which is attributed to the need for strong gradients, the small size of the spinal cord, and flow artifacts among others. Axial and sagittal T1-, T2-, STIR-, and diffusion-weighted images are recommended. Contrast enhancement is absent in the initial stage and can therefore help to delineate the pathology from inflammatory or neoplastic causes. Subsequently, contrast enhancement can be observed in the majority of spinal cord ischemia cases – typically more than 2 days after disease onset [15]. In the acute stage, restriction of diffusion and hyperintense signal changes in T2 and STIR sequences can be observed. However, depending also on the quality of the scan, MRI can be without any relevant changes. According to a longitudinal analysis with serial MR scans over time, signal changes in T2-weighted images are typically observed within 2 days from disease onset; the earliest respective change was seen already 14 h after disease onset [15]. Occlusions of the anterior spinal artery can cause predominant infarction of the anterior horn and surrounding white matter uni- or bilaterally, whereas occlusion of the posterolateral artery affects the dorsal horn and the dorsal columns. Concomitant infarction of the vertebral body – associated with hyperintense signal changes in the vertebra and the adjacent disk – is due to the shared vascularization of the spinal cord and the vertebrae [14].
As pointed out above, MRI can be unremarkable in the early phase after spinal cord ischemia. In this case, an infectious/inflammatory cause of spinal cord disease has to be addressed requiring a CSF workup. The general conception is that the CSF in spinal cord ischemia is pretty much normal except for a moderate protein increase. Systematic findings about CSF results in spinal cord ischemia are sparse. In a case series of 13 patients with spontaneous spinal cord ischemia, a mean cell count of 35.4 cells/mm3 (range 1–160) and a mean protein level of 0.72 g/l (range 0.4–1.39) have been reported [16]. Accordingly, moderate CSF pleocytosis does not rule out spinal cord ischemia entirely.
Therapy
In respect to evidence-based treatment for spontaneously occurring spinal cord ischemia, no randomized controlled clinical studies exist to date. Rule number one is to identify and treat the underlying cause if possible. Prophylactic treatment with a platelet inhibitory drug such as acetylsalicylic acid is commonly recommended. Thrombolytic treatment with recombinant tissue plasminogen activator (rt-PA) is not established in spinal cord ischemia. Few case reports describe a favorable outcome, which is not sufficient to recommend this therapeutic approach [17, 18]. It is challenging to confirm the diagnosis spinal cord ischemia before the treatment window for rt-PA closes. Due to a missing rationale and evidence, steroids should not be administered.
In respect to treatment and prophylaxis following surgical aortic repair, numerous studies have been performed. It is widely accepted that blood pressure needs to be stabilized immediately. At the same time, spinal cord pressure should be lowered by means of CSF drainage. A meta-analysis investigating 46 studies with a total of 4936 patients, who underwent TEVAR, did not reveal a significant benefit for routine or selective prophylactic lumbar CSF drainage [13]. In contrast, for open aortic repair strategies, the benefit of routine CSF drainage has been confirmed in meta-analyses and a randomized controlled trial [19].
Segmental artery occlusion in the course of anterior spine surgery – mostly related to scoliosis surgery – can induce spinal cord ischemia in rare instances [9]. Preoperative spinal angiography might be useful in determining the exact location of the Adamkiewicz artery and thus allows exact planning of the surgical approach to prevent a lesion of this very important artery. In 100 preoperative angiographies, the Adamkiewicz artery was located between the segments T8 and L3 (in 50 % at the T8/T9 level) and in 75 % on the left side. This information led to ten side changings and three modifications of surgical technique with segmental vessel preservation. In none of the 100 patients, neurological deficits suggesting spinal cord ischemia were observed postoperatively [20].
4 Spinal Vascular Malformations
Spinal vascular malformations are divided into spinal dural arteriovenous fistulas (sdAVF), arteriovenous malformations (sAVM), and cavernous angiomas. Both sdAVF and sAVM account for roughly 4 % of all intraspinal lesions.
4.1 Spinal Dural Arteriovenous Fistula
Spinal dural arteriovenous fistula (sdAVF) or type I sAVM is the most common type of a spinal vascular malformation accounting for 80 % of all spinal vascular malformations (Fig. 5.3a). The incidence is estimated around 5–10 per one million [21]. Predominantly affected are men with a mean age of 60. It is thought that sdAVF is most likely an acquired disease condition, caused by infection, syringomyelia, trauma, or surgery. 90 % of all sdAVFs are located in the thoracolumbar region [21].

Spinal vascular malformations. (a) Spinal dural arteriovenous fistula (sdAVF): typically varicosely expanded veins along the dorsal surface of the spinal cord. (b) Spinal arteriovenous malformation (sAVM) type II: Feeders from the anterior and the posterior spinal artery are illustrated. The nidus is located, both intra- and extramedullary. (c) The sAVM type IV is located around the conus medullaris on the pial surface intradurally. (d) sAVM type III, which do not respect tissue borders, are located intra- and extradurally [26]
Pathophysiology
Root veins penetrate the dura, which contributes to the vessel wall. There, arterial blood is shunted into perimedullar veins causing congestion within the veins and subsequent edema within the spinal cord. Usually solitary, rarely 2, never more than 2 fistulas per patient can be detected. Consecutively, variously expanded veins along the dorsal surface of the spinal cord can be observed. The related venous congestion causes a myelopathy. The fistula is located at the level of the spinal root.
Clinical Presentation
The hallmark of the disease is slowly progressing neurological dysfunction, in particular sensory (superficial and deep sensation) dysfunction and signs of neurogenic bladder and bowel dysfunction [22]. Frequently, at the time of diagnosis, locomotor impairment is observed. The slowly progressing disease course frequently delays the proper diagnosis – on average 23 months from first symptoms until the correct diagnosis has been made [22]. Sometimes, a stepwise worsening, rarely an acute deterioration, occurs. At disease onset pain – irradiating backache, which may be misinterpreted as degenerative vertebral disease – or claudicatio spinalis are not uncommon. Typically, bed rest provides relief of symptoms, whereas activity aggravates symptoms. If untreated, the disease will result in sensorimotor complete paraplegia including severe bowel and bladder dysfunction.
Diagnostics
Prime diagnostic tool is MRI to detect the congestion myelopathy or perimedullar ectatic veins (flow void in T2-weighted images). Contrast-enhanced MR angiography can help to identify the nidus. More specific analysis of vascular feeders requires conventional angiography. In case MRI is not possible, myelography can be an option to detect enlarged blood vessels in sdAVF, showing enlarged vessels as tortuous filling defects within the subarachnoid contrast dye. MRI shows congestion myelopathy expanding for over 6–7 segments [23]. The rostro-caudal extent of the myelopathy does not correlate with severity of symptoms or location of the fistula [24]. Contrast enhancement may mislead toward a spinal neoplasm. The dilated coronal plexus veins have a nodular, more shaggy appearance, as opposed to less tortuous plexus veins with a more oblong orientation found as a normal variant. Conventional spinal angiography represents the gold standard to identify the exact vascular pathology, in particular the feeding artery and the venous drainage. The disadvantage is that spinal angiography is time-consuming, sometimes requiring more than one session. Ideally, contrast-enhanced MR angiography indicates the fistula site, which helps to save iodinated contrast agent and radiographic exposure time. Alternatively, multislice CT angiography can help to localize the fistula site [25].
In spinal cavernous angiomas, T1-weighted images show hypointense and T2-weighted images hyperintense signal changes. Hemosiderin-sensitive sequences help to clearly identify the cavernous angiomas. Conventional angiography helps to specify an unknown mass lesion or other kinds of vascular pathologies [26].
Therapy
Effective treatment of sdAVF can be achieved surgically or through an endovascular approach. Surgical techniques include hemilaminectomy, identifying the abnormally enlarged shunting radicular vein, and either clipping or coagulating it close to its exit point from the dura. Endovascular embolization uses liquid adhesive embolic agents to interrupt the intradural shunting vein. The endovascular approach is minimally invasive, and the treatment of the fistula can often be performed in combination with the diagnostic procedure. The length of hospitalization is usually shorter [27]. Nevertheless, the overall outcome is not affected by the chosen treatment modality [28]. In particular motor symptoms and pain respond, rarely bowel and bladder dysfunction. However, a recent meta-analysis shows a clear advantage of primary surgical treatment of sdAVF over endovascular treatment in terms of initial fistula closure and fistula recurrence [29]. Successful treatment (lack of initial treatment failure and lack of recurrence) can be achieved in 96.6 % (588 out of 609 patients) with surgery versus 72.2 % (363 out of 503 patients) with endovascular therapy.
4.2 Spinal Arteriovenous Malformations
Spinal arteriovenous malformations (sAVM), which are mostly located at cervical spinal cord level, account for 15–20 % of all spinal vascular malformations. The average age in type II sAVM is 20–40 years. Type III and IV sAVM become apparent in adolescence and early adulthood (Fig. 5.3b–d).
Pathophysiology
In type II sAVM, multiple arterial feeders take their origin from anterior and posterior spinal arteries. Therefore, arterial pressure is usually high. Drainage occurs through the venous plexus. The nidus is mostly confined to a spinal cord segment sitting partly intra- and partly extramedullary. An intramedullary or subarachnoidal hemorrhage or a venous congestion leads to mostly acute clinical symptoms. Type III sAVM is characterized by a diffuse nidus enlarging the spinal cord. Clinical symptoms are triggered by hemorrhage or myelopathy related to the venous congestion. Type IV sAVM is located around the conus medullaris on the pial surface intradurally. As described for type III sAVM, the malformation becomes apparent by hemorrhage or venous congestion with subsequent myelopathy or radiculopathy.
Diagnostics
See respective paragraph for spinal dural arteriovenous fistula.
Therapy
In type II sAVM, decompression surgery alone (laminectomy) does not yield a favorable outcome. Surgical and endovascular therapeutic interventions can be considered to remove/extinguish the sAVM. However, outcome appears to be more favorable with endovascular therapy requiring in many cases repeated interventions [26]. Without specific treatment the overall prognosis is poor. Type III sAVMs can rarely be resected, whereas in type IV sAVM, successful surgical resection is feasible [26].
4.3 Spinal Cavernous Angioma
Spinal cavernous angiomas represent rare disease conditions, which manifest around the age of 40. Compared to intraspinal locations, intracranial cavernous angiomas are ten times more frequent [26].
Pathophysiology
Cavernous angiomas consist of telangiectasias, which change in shape and size through repeated bleedings. They can be located within or outside of the spinal cord parenchyma, rarely, epidurally.
Clinical Presentation
Back pain and progressive neurological symptoms (intraparenchymal angioma) are caused by repeated bleeding and/or microthrombosis. In case of a slowly progressive disease course, the diagnosis can be delayed up to 4 years. If symptoms manifest acutely, the diagnosis will be established promptly.
Diagnostics
See respective paragraph for spinal dural arteriovenous fistula.
Therapy
The main aim should be to surgically remove symptomatic cavernous angiomas; however, the perioperative risk has to be weighed carefully against disease progression [30].
Conclusion
Spinal cord vascular pathologies can present as acute onset (spinal cord ischemia) all the way to a chronically progressive disease course. Clinical symptoms are not specific in respect to the etiology. In particular slowly progressing symptoms as typically observed in sdAVM can dramatically delay the proper diagnosis and thus postpone specific treatment. The sooner appropriate measures are taken – endovascular or surgical elimination of the fistula – the earlier neurological dysfunction can be contained, and further worsening including bowel and bladder dysfunction can be avoided. In spinal cord ischemia, early diagnosis can be challenging despite the acute presentation of severe neurological dysfunction and not infrequently made just by exclusion of other compressive and non-compressive causes of spinal cord disease. Unfortunately, effective therapeutic interventions (systemic administration of recombinant tissue plasminogen activator, mechanical thrombus retrieval), which are available after acute cerebral ischemia, are not established in spinal cord ischemia.
References
Heuschmann PU, Busse O, Wagner M, Endres M, Villringer A, Rother J, Kolominsky-Rabas PL, Berger K, Gesell DS, Schlaganfall SD (2010) Frequency and care of stroke in Germany. Aktuelle Neurologie 37(7):333–340
Melissano G, Bertoglio L, Rinaldi E, Leopardi M, Chiesa R (2015) An anatomical review of spinal cord blood supply. J Cardiovasc Surg (Torino) 56(5):699–706
Etz CD, Kari FA, Mueller CS, Silovitz D, Brenner RM, Lin HM, Griepp RB (2011) The collateral network concept: a reassessment of the anatomy of spinal cord perfusion. J Thorac Cardiovasc Surg 141(4):1020–1028
Griepp EB, Griepp RB (2010) The collateral network concept: minimizing paraplegia secondary to thoracoabdominal aortic aneurysm resection. Tex Heart Inst J 37(6):672–674
Nedeltchev K, Loher TJ, Stepper F, Arnold M, Schroth G, Mattle HP, Sturzenegger M (2004) Long-term outcome of acute spinal cord ischemia syndrome. Stroke 35(2):560–565
Sandson TA, Friedman JH (1989) Spinal cord infarction. Report of 8 cases and review of the literature. Medicine (Baltimore) 68(5):282–292
Pau A, Cossu M, Turtas S, Zirattu G (1989) Spinal cord dysfunction from lumbar disk herniation. Acta Neurol (Napoli) 11(6):439–443
Lewis SJ, Gray R, Holmes LM, Strantzas S, Jhaveri S, Zaarour C, Magana S (2011) Neurophysiological changes in deformity correction of adolescent idiopathic scoliosis with intraoperative skull-femoral traction. Spine (Phila Pa 1976) 36(20):1627–1638
Bridwell KH, Lenke LG, Baldus C, Blanke K (1998) Major intraoperative neurologic deficits in pediatric and adult spinal deformity patients. Incidence and etiology at one institution. Spine (Phila Pa 1976) 23(3):324–331
Nakamoto BK, Siu AM, Hashiba KA, Sinclair BT, Baker BJ, Gerber MS, McMurtray AM, Pearce AM, Pearce JW (2013) Surfer’s myelopathy: a radiologic study of 23 cases. AJNR Am J Neuroradiol 34(12):2393–2398
Ullery BW, Cheung AT, Fairman RM, Jackson BM, Woo EY, Bavaria J, Pochettino A, Wang GJ (2011) Risk factors, outcomes, and clinical manifestations of spinal cord ischemia following thoracic endovascular aortic repair. J Vasc Surg 54(3):677–684
Dias NV, Sonesson B, Kristmundsson T, Holm H, Resch T (2015) Short-term outcome of spinal cord ischemia after endovascular repair of thoracoabdominal aortic aneurysms. Eur J Vasc Endovasc Surg 49(4):403–409
Wong CS, Healy D, Canning C, Coffey JC, Boyle JR, Walsh SR (2012) A systematic review of spinal cord injury and cerebrospinal fluid drainage after thoracic aortic endografting. J Vasc Surg 56(5):1438–1447
Novy J, Carruzzo A, Maeder P, Bogousslavsky J (2006) Spinal cord ischemia: clinical and imaging patterns, pathogenesis, and outcomes in 27 patients. Arch Neurol 63(8):1113–1120
Alblas CL, Bouvy WH, Lycklama ANGJ, Boiten J (2012) Acute spinal-cord ischemia: evolution of MRI findings. J Clin Neurol 8(3):218–223
de Seze J, Stojkovic T, Breteau G, Lucas C, Michon-Pasturel U, Gauvrit JY, Hachulla E, Mounier-Vehier F, Pruvo JP, Leys D, Destee A, Hatron PY, Vermersch P (2001) Acute myelopathies: clinical, laboratory and outcome profiles in 79 cases. Brain 124(Pt 8):1509–1521
Restrepo L, Guttin JF (2006) Acute spinal cord ischemia during aortography treated with intravenous thrombolytic therapy. Tex Heart Inst J 33(1):74–77
Etgen T, Hocherl C (2016) Repeated early thrombolysis in cervical spinal cord ischemia. J Thromb Thrombolysis 42(1):142–145
Coselli JS, LeMaire SA, Koksoy C, Schmittling ZC, Curling PE (2002) Cerebrospinal fluid drainage reduces paraplegia after thoracoabdominal aortic aneurysm repair: results of a randomized clinical trial. J Vasc Surg 35(4):631–639
Charles YP, Barbe B, Beaujeux R, Boujan F, Steib JP (2011) Relevance of the anatomical location of the Adamkiewicz artery in spine surgery. Surg Radiol Anat 33(1):3–9
Jellema K, Canta LR, Tijssen CC, van Rooij WJ, Koudstaal PJ, van Gijn J (2003) Spinal dural arteriovenous fistulas: clinical features in 80 patients. J Neurol Neurosurg Psychiatry 74(10):1438–1440
Atkinson JL, Miller GM, Krauss WE, Marsh WR, Piepgras DG, Atkinson PP, Brown RD Jr, Lane JI (2001) Clinical and radiographic features of dural arteriovenous fistula, a treatable cause of myelopathy. Mayo Clin Proc 76(11):1120–1130
Gilbertson JR, Miller GM, Goldman MS, Marsh WR (1995) Spinal dural arteriovenous fistulas: MR and myelographic findings. AJNR Am J Neuroradiol 16(10):2049–2057
Cenzato M, Versari P, Righi C, Simionato F, Casali C, Giovanelli M (2004) Spinal dural arteriovenous fistulae: analysis of outcome in relation to pretreatment indicators. Neurosurgery 55(4):815–822; discussion 822–823
Lai PH, Pan HB, Yang CF, Yeh LR, Hsu SS, Lee KW, Weng MJ, Wu MT, Liang HL, Chen CK (2005) Multi-detector row computed tomography angiography in diagnosing spinal dural arteriovenous fistula: initial experience. Stroke 36(7):1562–1564
Eicker S, Turowski B, Steiger HJ, Hanggi D (2010) Diagnostic work-up and therapy of spinal vascular malformations: an update. Nervenarzt 81(6):719–726
Narvid J, Hetts SW, Larsen D, Neuhaus J, Singh TP, McSwain H, Lawton MT, Dowd CF, Higashida RT, Halbach VV (2008) Spinal dural arteriovenous fistulae: clinical features and long-term results. Neurosurgery 62(1):159–166; discussion 166–167
Steinmetz MP, Chow MM, Krishnaney AA, Andrews-Hinders D, Benzel EC, Masaryk TJ, Mayberg MR, Rasmussen PA (2004) Outcome after the treatment of spinal dural arteriovenous fistulae: a contemporary single-institution series and meta-analysis. Neurosurgery 55(1):77–87; discussion 87–88
Bakker NA, Uyttenboogaart M, Luijckx GJ, Eshghi OS, Mazuri A, Metzemaekers JD, Groen RJ, Van Dijk JM (2015) Recurrence rates after surgical or endovascular treatment of spinal dural arteriovenous fistulas: a meta-analysis. Neurosurgery 77(1):137–144; discussion 144
Zevgaridis D, Medele RJ, Hamburger C, Steiger HJ, Reulen HJ (1999) Cavernous haemangiomas of the spinal cord. A review of 117 cases. Acta Neurochir (Wien) 141(3):237–245
Martirosyan NL, Feuerstein JS, Theodore N, Cavalcanti DD, Spetzler RF, Preul MC (2011) Blood supply and vascular reactivity of the spinal cord under normal and pathological conditions. J Neurosurg Spine 15(3):238–251
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Weidner, N. (2017). Spinal Cord Vascular Disease. In: Weidner, N., Rupp, R., Tansey, K. (eds) Neurological Aspects of Spinal Cord Injury. Springer, Cham. https://doi.org/10.1007/978-3-319-46293-6_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-46293-6_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-46291-2
Online ISBN: 978-3-319-46293-6
eBook Packages: MedicineMedicine (R0)