
Abstract
In the scientific papers there are various mechatronic devices, with smart sensors, biofeedback systems and high end components. These system are mostly designed like replacement after amputation. The second are aim to exoskeleton concept, where the human capability is increased. Our rehabilitation device aim to area of temporary rehabilitation or recondition. The conventional motorized splint has limited possibilities for advance control and typically has no diagnostic functions.
Access provided by CONRICYT-eBooks. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
The rehabilitation process is very important process, with two basic aspects. At first, the return of the post traumatic patient to active life, which have financial aspects for him as well as for the society and psychical aspect, that active movement and physical load produce endorphins that help patient to be motivated and also influence him and his surroundings.
The conventional physiotherapeutic care is irreparable, in one hand, because physical contact and human care also helps the patient psychical mood at the other the skilled personnel use own perception system and own muscular system to use proper forces and movement limits according to actual possibilities of the patient. The mechatronics systems in rehabilitation are more and more popular nowadays; the motivation is mainly physiotherapist overload and independent validation of rehabilitation progress.
2 The Anatomy and Modelling of Knee Joint
The knee is the biggest joint in human body with quite complicated anatomical structure, include bones, cartilages, muscles and ligament, skin and other structures. There are tree bones are femur, tibia and patella (Fig. 1).

Skeletal and musculovascular description of knee joint [1]
This joint can be segmented into femorotibial and femorpaterlar part. The femorotibial jon hase medial and lateral part with meniscus divided to femoromenikal and meniskotibial part.
In the literature there are many models of joints generally and knee joints as well. The releology model is one of used and this model is easy to understand to people with technical knowledge, because it is based on terms like stress, stench, viscosity, plasticity and deformation. This description has usually time varying parameters, therefore the overall description is more difficult to e.g. metallic material description [2].
The knee joint is one of the most loaded joint in human body. The flat ground walking is described in many papers, the load depends a little on movement stereotype [3].
The phases of the motion can be described by diagram. The motion start with heel strike (HS), than slide flexion to reduce the shock during impact to floor up to maximum stance flexion MSF, and then extension to maximum stance extension MSE. In this part of the motion the most of the torque is applied. After this phase, the two “passive” phases are followed which moves leg to start position to next heel strike to start new cycle. These swings operates with leg mass, not with human body mass, therefore the torque are lower. This description is suitable only for flat surface, in case of stairs or even knee bend exercise is load much higher then Fig. 2. The next problem is in locomotion speed, where dynamic of movement influence overall energy.

Motion diagram of one step [3]
The movement stereotype are slightly different person to person too, but overall gait cycle description in general is well known. In our further design we focus to rehabilitation device, the highest demands are similar or lower to regular flat gait.
3 Rehabilitation Devices
The post traumatic therapy is very important phase in healing, there are two general goals, to increase the limited movement abbilitity to pre traumatic state. The bending limits are extended in proper way, e.g. the people can place the leg to next stair. The second goal is enhance the performance of the joint, where pretraumatic limits are reached at least with little limitation, e.g. the people is able to move the mass to healed leg and go up-stairs without help. The dynamic movement, running, volleyball spikes are really long term processes. The combine injury with neural system illness is a problem, the special devices combine locomotion and functional electrostimulation is applied. The multichannel electro stimulators are capable to emulate electrical signal in channels to create the step forward. In our case we focused to simple mechatronic device, which can helps with rehabilitation and measure the progress of exercises.
There are several types of exoskeletons on the market, which are worth to mention. For instance ReWalk, which is wearable robotic exoskeleton, which belongs between untethered, active, lower-body exoskeletons. ReWalk is licensed by the FDA in the USA, it has CE mark and it is licensed in Canada. This exoskeleton has motors at knee and hip joints and it’s designed for people suffering from spinal cord injury. Suit should enable people with this kind of injury to stand, turn around, walk and even run or climb stairs. Unfortunately the climb stairs function is not currently available in the US. ReWalk offers two versions of exoskeleton, personal for use at home and rehabilitation for use at specialized ReWalk clinics. Both devices are controlled by remote wrist-worn control (Fig. 3).

ReWalk exoskeletons [4]
4 Design of Rehabilitation Splint
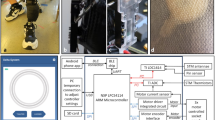
The key element of rehabilitation splint is electric motor. We have selected Maxon motor ECDC flat motor. This motor has high moment of inertia to other non-flat motors, but low profile, with is important for mechanical design. The output torque is about 0.5 Nm and speed less than 3000 RPM. The motor is equipped with harmonic gearbox with ratio 100. It means, that we are able to fulfill the load during gait cycle with one motor. The encoder system is built-in and has 3600 puls/turn resolution. The motor controller is Maxon Epos 2, that is not programmable motion controller, but there is option to control the drive via CANopen. The main control system can be arrange like PC based system or industrial controller. We have used the entry level PLC made X20CP1380. The main benefit of this system is low power consumption and wide spread of input and output modules.
In our first design of rehabilitation splint we assume to use two motors, each from one side of the splint and use drives without gearboxes for low torque rehabilitation. In current version with gearbox we suppose to use only one drive for knee, node id2, the second motor node id3 will be implemented for hip joint.
Mechanical design depends on the type of the device. Currently, there are two types of exoskeleton like devices being developed. Both are designated for rehabilitation, both are untethered and for the lower-body. First has two EC flat motor concentric with a knee joint. Second has one motor, which is located on the outside of a knee joint. Another motor is located at the hip joint. Work on the second kind of design is still in progress and it’s not part of this paper. Both designs uses Maxon EC flat motors combined with Maxon harmonic gearboxes. Such harmonic drives and motors allows the design to be light and compact with appropriate dynamics.
There are currently two pre-designs of wearable robotic orthoses with two motors being concentric at the knee joint. Design of orthosis (Fig. 4 left) is based on composite materials, such as carbon fiber, which could be shaped to achieve ergonomic surfaces as on the CAD model below. Another advantage of such materials is indisputably strength/weight ratio, which could be very high compared to metallic materials. The alternative solution (Fig. 4 right) is based on cheaper metallic materials and cheaper manufacturing process.

Robotic orthosis composite and metallic variant
The final version of the design is modular, which means that modules with gearbox and motor can be easily replaced by joint with bearing. The orthosis can be easily adjusted for left or right leg and the motor is on outer side of the orthosis. The configuration of positive motion and other adjustment is made in configuration menu.
5 Control of Rehabilitation Splint
The control algorithm has several operation modes. The first of them is simple passive mode. The splint is fixed to patient knee and after that the patient and physiotherapist set motion limits, the maximal flexion and extension. The limit values are displayed in HMI interface and can be freely modified.
The next operation mode is conventional motorized splint mode, where number of cycles is set. The velocity and acceleration of this motion can be adjusted according to patient feeling. The special feature is the continual torque measurement, where e.g. spasm can be detected.
The other operation mode is the releology diagnostic mode, where the load is applied to patient leg and the output data are torque characteristic of the knee.
This characteristic has hysteresis shape and the hysteresis can be used for performance description.
The multi task system is one feature of used PLC system, however in our case we use only two task. One for drive control via CANopen thru PDO objects. The basic configuration via SDO object is made in special program this program is in longer task. The visualization realized in 400 ms task class. The response of the visualization interface in not very impressive thanks to low computing power of PLC, where the visualization is processed in idle time. The key communication interface is CANopen. The Maxon Epos and used Maxon Epos2 used CANopen, Epos3 is EtherCAT based. The CANopen communication is quite simple and thanks to process data object are important data cyclically updated. The PDO configuration can be made inside Automation Studio.
6 Conclusion
The control software uses position control and torque diagnostic is made, the mechanical design is made in two variants. The manufacturing process in now in progress. The overall concept is validated in no load operation. In the future must there must be designed the battery pack and model is ready for higher model predictive control to utilize the orthosis to actual motion stereotype, walk, stairs and run.
References
The knee joint [online]: Jointace C2 [cit. 2016-02-28]. Available from:http://jointacec2.com/the-knee-joint/
Martinez-Villalpando, E.C., Herr, H.: Agonist-antagonist active knee protehesis: a preliminary study in level–ground walking. J. Rehabil. Res. Dev. 46, 361 (2009)
Sifta P, Bittner V.: Measurement of reologic properties of soft tissue (muscle tissue) by device called myotonometer. In: 6th World Congress of Biomechanics (WCB 2010), vol. 31, p. 1020 (2010) WOS:0003067161100260
ReWalk 6.0 [online]: © 2016 ReWalk Robotics [cit. 2016-02-28]. Available from:http://rewalk.com/
Acknowledgments
The results of this project were obtained through the financial support of the Ministry of Education, Youth and Sports in the framework of the targeted support of the “National Programme for Sustainability I LO1201” and the OPR&DI project “Centre for Nanomaterials, Advanced Technologies and Innovation CZ.1.05/2.1.00/01.0005”.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this paper
Cite this paper
Cernohorsky, J., Cadek, M. (2017). Smart Rehabilitation Splint. In: Beran, J., Bílek, M., Žabka, P. (eds) Advances in Mechanism Design II. Mechanisms and Machine Science, vol 44. Springer, Cham. https://doi.org/10.1007/978-3-319-44087-3_50
Download citation
DOI: https://doi.org/10.1007/978-3-319-44087-3_50
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-44086-6
Online ISBN: 978-3-319-44087-3
eBook Packages: EngineeringEngineering (R0)