
Abstract
Cyanosis in neonate infants may be caused by cardiac malformations such as transposition of the great arteries, tetralogy of Fallot, pulmonary and tricuspid atresia, hypoplastic left heart syndrome, common arterial trunk, Ebstein’s anomaly of the tricuspid valve, total anomalous pulmonary venous return and congestive cardiomyopathy. All mentioned malformations can be diagnosed by three basic sections: the parasternal long-axis and short-axis views and the subcostal or apical four-chamber view. If these three sections are normal, cyanotic heart diseases can be excluded. In the case of a cyanotic congenital heart disease, one or two sections are pathologic.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
24.1 Introduction
Differential diagnosis of the cyanotic neonate includes cardiovascular diseases, persistent pulmonary hypertension (PPHN), hyperviscosity syndrome, neonatal infections, especially pulmonary infections, and other pulmonary diseases.
Pulmonary diseases such as neonatal pneumonia, pneumothorax and diaphragmatic hernia can be excluded by physical examination, chest X-ray and elevated pCO2 in blood gas analysis.
Neonatal infection, hemoconcentration and hyperviscosity syndromes can be ruled out by a thorough blood work and the measurement of the haemoglobin level.
Cardiac malformations causing cyanosis have to be excluded by echocardiography (Adams et al. 1989; Anderson et al. 1987; Freedom et al. 1992; Lai et al. 2009; Schumacher and Bühlmeyer 1989; Snider et al. 1997; Skinner et al. 2000). Cyanosis is most likely to be a cardiac cause when:
-
1.
The haemoglobin level is normal.
-
2.
Physical examination and X-ray suggest the absence of pulmonary disease.
-
3.
Arterial pCO2 is low or normal.
-
4.
Arterial pO2 and saturation is low.
24.2 Cardiac Malformations Associated with Cyanosis
Three different categories of cyanotic cardiac malformations have to be differentiated (Skinner et al. 2000):
-
1.
Reduced pulmonary blood flow due to obstruction or absence of connection within the right heart (e.g. tricuspid atresia, pulmonary atresia and hypoplastic pulmonary arteries)
-
2.
Nonserial connections due to discordant connections (e.g. transposition of the great arteries or anomalous pulmonary venous connection)
-
3.
Common mixing lesions (e.g. common arterial trunk and single ventricle)
Eleven different cardiac malformations associated with cyanosis have to be differentiated and excluded (Table 24.1). Frequent congenital heart malformations associated with cyanosis are tetralogy of Fallot (TOF), transposition of the great arteries (TGA), pulmonary atresia (PA) with or without ventricular septum defect (PAiVS) and the hypoplastic left heart syndrome (HLHS) (Adams et al. 1989; Anderson et al. 1987; Freedom et al. 1992; Goldberg and Rychik 2009; Lai et al. 2009; Schumacher and Bühlmeyer 1989; Snider et al. 1997; Skinner et al. 2000). Rare congenital malformations associated with cyanosis are tricuspid atresia (TA), common arterial trunk (TAC), double outlet right ventricle (DORV), Ebstein’s anomaly of the tricuspid valve, total anomalous pulmonary venous return and congestive cardiomyopathy (Adams et al. 1989; Anderson et al. 1987; Freedom et al. 1992; Goldberg and Rychik 2009; Lai et al. 2009; Schumacher and Bühlmeyer 1989; Snider et al. 1997; Skinner et al. 2000). Most of the cardiac malformations mentioned above cause central cyanosis; congestive cardiomyopathy may cause peripheral cyanosis due to bad peripheral perfusion.
In all cases of cyanosis, cyanotic heart disease has to be ruled out. If no paediatric specialist for echocardiography is available, for example, during weekend and during night, it is important for the neonatologist to get a hint for cyanotic heart disease or to exclude it. With basic knowledge of echocardiography, the above-mentioned cyanotic congenital malformations can be excluded if three basic views are normal.
24.3 What Views Are Necessary for the Exclusion or Diagnosis of Cyanotic Heart Disease?
A complete echocardiographic examination includes the parasternal, apical, subcostal and suprasternal long- and short-axis views (Lai et al. 2009; Snider et al. 1997; Skinner et al. 2000). This affords the detailed knowledge of a paediatric cardiologist in echocardiography.
The exclusion of the different cyanotic congenital heart malformations mentioned above is possible with a basic echocardiographic programme.
The aim of the following chapter is the description of three basic planes (parasternal long- and short-axis views and apical or subcostal four-chamber view) through the heart. If these views are normal, the neonatologist can exclude all major cardiac malformations associated with cyanosis. This minimal echocardiographic programme can easily be performed by the neonatologist with basic experience in echocardiography:
-
Parasternal long-axis view through the left ventricle (Fig. 24.1)
Fig. 24.1 
(a) Parasternal long-axis view in a healthy newborn infant. AO aorta, LA left atrium, LV left ventricle, RV right ventricle. (b) Colour-coded Doppler sonogram of the inflow in the left ventricle which is displayed red. AO aorta, LA left atrium, LV left ventricle, RV right ventricle. (c) Colour-coded Doppler sonogram of the outflow from the left ventricle into the aorta which is displayed blue. AO aorta, LA left atrium, LV left ventricle, RV right ventricle
-
Parasternal short-axis view through the right ventricle and the pulmonary artery and (Fig. 24.8)
-
Apical or subcostal four-chamber view through the atria and ventricles (Fig. 24.13)

These views allow the following statements:
-
1.
Has the patient two or only one ventricle?
-
2.
What is the size of both ventricles (normal size, hypoplastic, single ventricle?) and how do they work?
-
3.
What is the function of the atrioventricular valves (AV)? Are they stenotic, atretic or incompetent?
-
4.
Where do the aorta and pulmonary artery originate from the heart? (malalignment VSD?)
-
5.
How is the arrangement of the aorta and the pulmonary artery? Are there signs of transposition of the great arteries? (ventriculoarterial concordance or discordance?)
-
6.
What is the function of the semilunar valves? Is there stenosis or atresia of the semilunar valves?
-
7.
Are there hints for total or partial anomalous pulmonary venous connection?
If all three planes are normal and if the flow (colour Doppler) in different segments of the heart is normal, cyanotic heart disease can be excluded. In the case of distinctive features of congenital heart disease associated with cyanosis, a thorough cardiac investigation by an experienced paediatric cardiologist has to be performed.
24.3.1 Parasternal Long-Axis View Through the Left Heart
To get the parasternal long-axis view through the left ventricle, the transducer is placed in the second and third intercostal space. The plane runs between the right shoulder and the left hip. The scanning plane transects the heart along its longitudinal axis from the basis and root of the aorta towards the apex. This section provides an image from the left heart structures including the left atrium, the mitral valve, the left ventricle with the ventricular septum and the aortic root (Fig. 24.1a). This image is the standard view for M-mode echocardiographic measurements of the left atrial and left ventricle dimensions and function. Besides the judgement of the two-dimensional anatomic structures, the contractility of the left ventricle and the movement of the mitral and aortic valve can be judged in real time or M-mode. With colour Doppler, normal inflow into the left ventricle (red) and outflow out of the left ventricle (blue) can be seen (Fig. 24.1b, c).
A normal parasternal long-axis view through the left ventricle with a normal-shaped left ventricle with normal contractility and a normal aortic root associated with normal inflow and outflow from the left ventricle excludes the following congenital cardiac malformations:
-
Hypoplastic left heart syndrome (HLHS) (Fig. 24.2a, b) (Deeg 1994a; Goldberg and Rychik 2009; Moniotte and Barrea 2009; Skinner et al. 2000; Snider et al. 1997)
Fig. 24.2 
(a) Parasternal long-axis view in a patient with hypoplastic left heart syndrome. AO hypoplastic aorta, LA left atrium, LV hypoplastic left ventricle, RV normal-size right ventricle. (b) M-mode echocardiogram in a patient with hypoplastic left heart syndrome. Very small left ventricle (LV) with bad contractility. LA left atrium, RV right ventricle. (c) Colour-coded Doppler sonogram of the flow in the left heart of a patient with hypoplastic left heart syndrome. The image shows an echogenic surface of the endocardium typical to fibroelastosis of the endocardium. The image shows a mosaic of turbulent flow within the ascending aorta (AO). Additionally mitral regurgitation can be shown demonstrating that the mitral valve is also patent but severely stenotic. AO aorta, LA left atrium, LV left ventricle, RV right ventricle
-
Congestive cardiomyopathy of the left ventricle (Fig. 24.3) (Colan 2007; Maron 2006; Matitiau 1994; Spencer 2009)
-
Total anomalous pulmonary venous return (TAPVC) (Fig. 24.3)
Fig. 24.3 
M-mode of the left ventricle in an infant with congestive cardiomyopathy (multiple trabeculations due to noncompaction cardiomyopathy). Dilatation of the left ventricle with bad contractility (shortening fraction 18%!). LA left atrium, LV left ventricle, RV right ventricle
-
Pulmonary atresia with ventricular septum defect (PAIVS) (Deeg 1994c; Hanley et al. 1993; Levine 2009)
-
Double outlet right ventricle (DORV)
-
Common arterial trunk (TAC) (Fig. 24.5c) (Deeg 1995; Rice 1982)
-
D-transposition of the great arteries (d-TGA) (Fig. 24.6) (Deeg 1997; Lai et al. 2009; Seward et al. 1987; Silverman and Snider 1982; Skinner et al. 2000; Snider et al. 1997)


24.3.1.1 Hypoplastic Left Heart Syndrome
-
In cases of hypoplastic left heart syndrome, the mitral and aortic valves are severely stenotic or atretic, and the left ventricle is very small and shows bad contractility (Deeg 1994a; Goldberg and Rychik 2009; Moniotte and Barrea 2009; Skinner et al. 2000; Snider et al. 1997) (Fig. 24.2). The apex of the heart is formed by the right ventricle (normally left ventricle). The diameter of the aortic root measures less than 6 mm. Colour-coded Doppler sonography and spectral Doppler can distinguish between mitral and aortic atresia and severe stenosis (Fig. 24.2c). In cases of valvular stenosis, transvalvular flow or even valve regurgitation can be shown (Fig. 24.2c). In cases of mitral atresia or aortic atresia, no transvalvular flow can be seen.
24.3.1.2 Congestive Cardiomyopathy
-
Congestive cardiomyopathy is characterized by a dilated left ventricle with bad contractility (Fig. 24.3) (Colan 2009). M-mode through the left ventricle shows the dilated ventricle with markedly reduced contractility: the shortening fraction is considerably below the normal value for neonates of 28 %. Different forms of congestive cardiomyopathy can be differentiated: in noncompaction cardiomyopathy (formerly called spongy myocard), the left ventricle has no smooth endocardial lining but shows multiple trabeculations similar to the right ventricle (Fig. 24.3a).
24.3.1.3 Total Anomalous Pulmonary Venous Connections
-
Total anomalous pulmonary venous connections (TAPVC) are characterized by a small left atrium, mitral valve and a small left ventricle in parasternal long-axis view (Fig. 24.4) (Table 24.2). The right ventricle however appears large. In contrast to the hypoplastic left heart syndrome (HLHS), the contractility of the left ventricle is normal. In contrast to HLHS, the apex of the heart is formed by the small left ventricle. Colour and spectral Doppler show normal inflow into and outflow from the left ventricle. Although TAPVC cannot be diagnosed in the parasternal long-axis view by sure, a normal parasternal long-axis view through a normal sized left ventricle with normal inflow and outflow excludes TAPVC. In all infants with apparently small left atrium and ventricle in the parasternal long-axis view, total anomalous pulmonary venous connection has to be excluded in the four-chamber view or the suprasternal short-axis view. In TAPVC, the confluence of the pulmonary veins with the left atrium during development of the heart has failed. Fusion can occur with any systemic vein: the portal vein, the coronary sinus, the right atrium or the ascending vertical vein. According to the location of the venous connection, three different forms of TAPVC have to be differentiated:
Fig. 24.4 
Total anomalous pulmonary venous return. The parasternal long-axis view shows a small left atrium (LA) and left ventricle (LV). In contrast to the small structures of the left heart, the right ventricle (RV) is large. AO aorta (Courtesy of Prof. Dr. M. Hofbeck, Tübingen)
Table 24.2 Overview about the different echocardiographic views in which the 11 cyanotic malformations are best seen -
Supracardiac TAPVC
-
Cardiac TAPVC
-
Infracardiac TAPVC
-

24.3.1.4 Malalignment Ventricular Septum Defect
The demonstration of a continuity of the interventricular septum with the anterior wall of the aorta excludes all diseases of the Fallot group such as tetralogy of Fallot (TOF), pulmonary atresia with ventricular septum defect (PAiVS), common arterial trunk (TAC) and double outlet right ventricle (DORV) (Fig. 24.5a). This whole group is characterized by a malalignment ventricular septum defect with an overriding systemic artery (frequently the aorta) which gets its blood from the left and right ventricle (Fig. 24.5b) (Deeg 1994c; Deeg 1995). Differential diagnosis between the various diseases of this group affords flow measurements within the right ventricular outflow tract and the main pulmonary artery in the parasternal short-axis view (Figs. 24.9c, d and 24.10b, c).

Parasternal long-axis view in patients with malalignment ventricular septum defects (a, b) tetralogy of Fallot and (c) common arterial trunk). (a) 2D image. (b) Colour-coded Doppler sonogram. The images show the malalignment ventricular septum defect with an overriding aorta. The aorta gets blood from the left and right ventricle (AAO). AO overriding aorta, LA left atrium, LV left ventricle, RV right ventricle. (c) Suprasternal long-axis view through the aortic arch in a patient with common arterial “trunk”: the image shows that the artery which originates from the heart, the common arterial trunk (TAC), gives origin to the ascending aorta (AAO) and another artery, the pulmonary trunk (markers). DAO descending aorta
24.3.1.5 Tetralogy of Fallot (TOF)
-
TOF is characterized by a malalignment VSD, an overriding aorta, a subpulmonary obstruction and right ventricular hypertrophy (Deeg 1994c). In TOF turbulent transvalvular flow across the pulmonary valve can be found with colour and spectral Doppler, whereas in PAiVS no transvalvular flow across the pulmonary valve can be shown (Figs. 24.9c, d, 24.10b, c and 24.11). TOF has many variations which have to be evaluated by a thorough echocardiographic investigation (JD Waldman and G Holmes in Skinner 2000). The following malformations have to be differentiated:
-
1.
Degree of the subpulmonary obstruction
-
2.
Size, patency and presence of the pulmonary valve (special form: TOF with absent pulmonary valve)
-
3.
Size of the pulmonary arteries
-
4.
Sources of collateral blood flow
-
5.
Additional VSDs (difficult to diagnose as the pressures in the right and left ventricle are equal)
-
6.
Size of an associated ASD
-
7.
Associated mitral valve stenosis (rare)
-
1.
24.3.1.6 Truncus Arteriosus Communis (TAC)
-
In truncus arteriosus communis (TAC), a single artery, the common arterial trunk, originates from the heart (Deeg 1995; Rice 1982). It gives rise to the systemic, pulmonary and coronary circulations. TAC is always associated with a large subarterial malalignment VSD (Deeg 1995; Rice 1982). In TAC no origin of the pulmonary artery from the right ventricle can be shown. One or two pulmonary arteries originate from the side of the large common arterial trunk (Fig. 24.5c). The truncal valve in the short-axis view may have four or five leaflets which are often thickened. Colour and pulsed Doppler investigations should be performed to reveal associated truncal valve regurgitation and stenosis. The quality of the valve is crucial for the outcome (Skinner et al. 2000). Commonly associated lesions, which have to be excluded, are:
-
1.
Truncal valve stenosis or regurgitation
-
2.
Mitral stenosis
-
3.
Additional VSDs
-
4.
Interrupted aortic arch
-
1.
24.3.1.7 Transposition of the Great Arteries (TGA)
-
In healthy individuals, parasternal long-axis view provides only visualization of the aorta. Normally the aorta and pulmonary artery cross over each other and can never be displayed on the same image. If the aorta and pulmonary artery can be demonstrated simultaneously and are arranged parallel to each other, the patient has d-transposition of the great arteries (d-TGA) (Fig. 24.6) (Skinner et al. 2000; Snider et al. 1997). In healthy infants, it is never possible to obtain such an image because of the cross-over relationship of the great arteries. In cases of d-TGA, the aorta originates anterior from the right and the pulmonary artery posterior from the left ventricle (Fig. 24.6). The anteriorly situated artery, which originates from the right ventricle, passes over into the aortic arch which gives rise to the head and neck arteries and does not bifurcate characterizing it as the aorta (Fig. 24.6c). Additionally the coronary arteries originate from the anterior artery at its base, identifying it as the aorta. The vessel that originates posterior from the left ventricle is oriented to the back and bifurcates immediately defining it as the pulmonary artery (Fig. 24.6).
Fig. 24.6 
(a, b) Parasternal long-axis view in a patient with d-transposition of the great arteries. Parallel origin of aorta and pulmonary artery from the heart. Both arteries can be displayed simultaneously. The aorta (AO) originates anteriorly from the right ventricle (RV). The pulmonary artery (PA) originates posteriorly from the left ventricle (LV). (c, d) Suprasternal long-axis view through the great vessels originating from the heart. The anterior vessel continues in an arch and gives origin to the arteries of the upper extremities and the head (ascending aorta). The posterior artery is oriented posteriorly and divides in two branches (pulmonary artery). AO ascending aorta, LA left atrium, LV left ventricle, PA pulmonary artery, RV right ventricle. *open duct
-
Oxygenation occurs by mixing of systemic venous and pulmonary venous blood at atrial or ventricular levels. If a VSD is absent and the ASD is restrictive, immediate balloon atrio-septostomy is indicated as systemic arterial oxygenation via the open duct is only marginal.

24.3.1.8 Hypoplastic Right Heart – Tricuspid Atresia and Pulmonary Atresia with Intact Ventricular Septum
Cardiac malformations with a hypoplastic right heart can usually not diagnosed in the parasternal long axis view. Malformations with hypoplastic right ventricles can be suspected in the parasternal long axis view if the right ventricle is extremely small (Fig.24.7). In tricuspid atresia and in pulmonary atresia with intact ventricular septum only remnants of the right ventricle can be seen in the parasternal long axis view (Fig.24.7a, b). The definite diagnosis however affords the parasternal short axis and the four chamber view.

Parasternal long-axis view through the left ventricle in hypoplastic right heart syndrome. (a) Pulmonary atresia with intact ventricular septum. Hypoplasia of the right ventricle (RV). Normal structures of the left heart. In contrast to normal images, only a tiny right ventricle (RV) is displayed. AO aorta, LA left atrium, LV left ventricle. (b) Tricuspid atresia with small ventricular septum defect. Hypoplasia of the right ventricle (markers). AO aorta, LA left atrium, LV left ventricle
24.3.1.9 Conclusion
A normal parasternal long-axis view with normal inflow into and outflow from the left ventricle excludes eight of the above-mentioned eleven cyanotic heart diseases:
-
1.
Hypoplastic left heart syndrome
-
2.
Total anomalous pulmonary connection
-
3.
Congestive cardiomyopathy
-
4.
Tetralogy of Fallot
-
5.
Pulmonary atresia with ventricular septal defect
-
6.
Double outlet right ventricle
-
7.
Common arterial trunk
-
8.
Transposition of the great arteries
24.3.2 Parasternal Short-Axis View Through the Right Heart
The short axis runs 90° to the long-axis view. It cuts the heart transversely. The plane is directed from the right hip to the left shoulder. It is obtained from the parasternal long-axis view by rotating the transducer clockwise through 90°. Tilting the probe allows different structures to be visualized. The standard cut provides an image through the aortic root and the right heart as it wraps around it (“circle and sausage” formation) (Fig. 24.8a). The right atrium, tricuspid valve, right ventricular inflow and outflow tract, the pulmonary valve and the pulmonary artery can be shown (Fig. 24.8a). Normal inflow into the right ventricle is displayed red (Fig. 24.8b), and normal outflow from the right ventricle into the pulmonary artery is displayed blue (Fig. 24.8c).

(a) Parasternal short-axis view through the right heart (circle and sausage; circle = aortic root; sausage = right heart). The right heart wraps around the aortic root. AO aorta, LA left atrium, PA pulmonary artery, RA right atrium, RV right ventricle, TK tricuspid valve. (b) Colour Doppler of the inflow into the right ventricle in the parasternal short-axis view. The inflow into the right ventricle is displayed red. AO ascending aorta, LA left atrium, PA pulmonary artery, RA right atrium, RV right ventricle. (c) Colour Doppler of the outflow into the pulmonary artery in the parasternal short-axis view. The normal flow in the pulmonary artery is displayed blue. AO ascending aorta, LA left atrium, PA pulmonary artery, RA right atrium, RV right ventricle
24.3.2.1 Tricuspid Atresia
-
In cases of tricuspid atresia, the right ventricle is severely hypoplastic (Adams et al. 1989; Anderson et al. 1987; Deeg 1994b; Freedom et al. 1992; Goldberg and Rychik 2009; Lai et al. 2009; Schumacher and Bühlmeyer 1989; Snider et al. 1997; Skinner et al. 2000). The tricuspid valve cannot be shown on 2D images. The valve is replaced by an echogenic membrane or is completely missing. No transvalvular flow from the right atrium into the right ventricle can be shown with colour or spectral Doppler. There is always an atrial septal defect through which the venous blood flows from the right to the left atrium. Without an atrial communication, tricuspid atresia is not compatible with life. Colour Doppler shows right to left shunt through the atrial septum defect. The pulmonary arteries get their blood from the right ventricle by an associated ventricular septum defect. The size of the right ventricle depends on the size of the associated ventricular septum defect. A small VSD is associated with a severely hypoplastic right ventricle and a large VSD may be associated with a nearly normal-size right ventricle. The size of the pulmonary arteries depends also on the size of an associated ventricular septum defect. The size of an associated ventricular septal defect determines the severity of an associated outlet obstruction from the right ventricle. Small ventricular septum defects are associated with more or less severe right ventricle outlet obstructions and severe hypoplasia of the pulmonary arteries (Fig. 24.9).
Fig. 24.9 
Parasternal short-axis view in pulmonary stenosis. (a) Parasternal short-axis view through the right ventricular outflow tract and pulmonary artery in tricuspid atresia and pulmonary stenosis. Atretic tricuspid valve (TA), which is displayed as an echogenic membrane. Small ventricular septum defect. Hypoplastic right ventricle (RV), valvular pulmonary stenosis and hypoplastic pulmonary artery (PA). AO aorta, LA left atrium, RA right atrium. (b) Colour Doppler of the flow in the hypoplastic pulmonary artery shows accelerated flow due to valvular stenosis displayed as a mosaic of different colours. AO aorta, PA pulmonary artery. (c) Doppler sonographic flow measurement in the pulmonary artery in a patient with minimal pulmonary stenosis of 16 mm Hg

Associated malformations are transposition of the pulmonary arteries, VSD and right ventricular outflow obstructions.
In cases of severe pulmonary stenosis, the pulmonary arteries are more or less hypoplastic (Figs. 24.9 and 24.10a, b), and the flow in the pulmonary artery is displayed in a mosaic pattern (Figs. 24.9b and 24.10c). In all cases of pulmonary stenosis, the pressure gradient over the right ventricular outflow tract can be calculated with CW Doppler to estimate the severity of the stenosis (Figs. 24.9c and 24.10d).

Parasternal short-axis view in tetralogy of Fallot. (a, b) Parasternal short-axis view through the right ventricular outflow tract in tetralogy of Fallot. Hypoplastic pulmonary artery. AAO ascending aorta, LPA left pulmonary artery, PA pulmonary artery, PV pulmonary valve, RPA right pulmonary artery, RV right ventricle, RVOT right ventricular outflow tract. (c) Colour-coded Doppler sonogram of the flow in the hypoplastic pulmonary artery (PA). The flow is displayed in a mosaic pattern characteristic of pulmonary stenosis and transvalvular flow. (d) Continuous wave Doppler of the flow in the pulmonary artery: accelerated turbulent flow with a pressure gradient of 60–70 mm Hg
In summary the size of the atrial and ventricular septum defect determines the size of the right ventricle and the pulmonary arteries. Associated right ventricular outflow obstructions as well as the ventriculoarterial connections (associated TGA or not) have to be evaluated.
24.3.2.2 Pulmonary Atresia
-
In pulmonary atresia the pulmonary arteries usually are hypoplastic (Fig. 24.11a). No transvalvular flow can be shown by colour-coded Doppler sonography or spectral Doppler (Fig. 24.11b, c). Turbulent blood flow in the pulmonary arteries is displayed in a mosaic pattern (Fig. 24.11b). The retrograde perfusion of the pulmonary artery by an open arterial duct or systemic-pulmonary collaterals is displayed red (Fig. 24.11c). Two forms of pulmonary atresia (PA) have to be differentiated:
Fig. 24.11 
Pulmonary atresia with intact ventricular septum defect. (a) Parasternal short-axis view through the hypoplastic right ventricle and hypoplastic pulmonary artery in pulmonary atresia with intact ventricular septum. AO aorta, LA left atrium, PA hypoplastic pulmonary artery, RA right atrium, RV hypoplastic right ventricle with thick muscle wall, TV tricuspid valve. (b) Colour flow in the pulmonary artery in a patient with pulmonary atresia. Mosaic flow pattern in the pulmonary artery. No transvalvular flow through the right ventricular outflow tract (RVOT) can be shown. (c) Retrograde perfusion of the pulmonary artery in a patient with pulmonary atresia. The retrograde perfusion is displayed red (normally the flow is blue). No transvalvular flow can be shown
-
PA with intact ventricular septum (PAiVS)
-
PA with ventricular septum defect (PAVSD)
The two forms differ in the size of the right ventricle and the pulmonary artery. The right ventricle in patients with PAiVS is extremely hypoplastic (Deeg 1994b). PAVSD on the other side usually has a more or less normal-size right ventricle as the right ventricle has normal inflow and can pump its blood via the VSD into the aorta (Deeg 1994c). Patients with PAVSD have smaller pulmonary arteries than infants with PAiVS (Deeg 1994b, c).
-

24.3.2.3 Truncus Arteriosus Communis
-
If no right ventricular outflow tract can be shown in the parasternal short-axis view, common arterial trunk has to be excluded. In the case of a common arterial trunk, one or two pulmonary arteries originate from the side of the common arterial trunk in a high parasternal short-axis view (Fig. 24.12) (Deeg 1995; Rice 1982).
24.3.2.4 Tetralogy of Fallot and Critical Pulmonary Stenosis
-
Tetralogy of Fallot and critical pulmonary stenosis are characterized by small (hypoplastic) pulmonary arteries a thickened pulmonary valve and an accelerated transvalvular flow which is displayed as a mosaic (Fig. 24.10a, b, c). CW Doppler allows quantification of the severity of the stenosis by calculation of the pressure gradient using the modified Bernoulli equation (Δp = 4 × V 2) (Fig. 24.10d).
A special form of TOF is associated with an absent pulmonary valve. Patients have a malalignment VSD with an overriding aorta. In contrast to TOF, there is no subpulmonary stenosis, as the pulmonary valve is absent. This causes to-and-fro blood flow in the right ventricular outflow tract and severe dilatation of the pulmonary arteries and the right ventricle. In contrast to the dilatation of the structures of the right heart, the left ventricle and aorta seem underdeveloped, although they have a normal size. After birth the dilated pulmonary arteries can compress the bronchi and cause severe respiratory distress and cyanosis.
24.3.2.5 Pulmonary Atresia
-
Pulmonary atresia is characterized by hypoplastic pulmonary arteries (Fig. 24.11a) perfused in a retrograde fashion by an open PDA and/or systemic-pulmonary collateral arteries (Fig. 24.11b, c). Retrograde perfusion is displayed red (Fig. 24.11c). In cases of accelerated flow, the artery is displayed as a mosaic without demonstrable transvalvular flow (Fig. 24.11b). In tetralogy of Fallot, critical pulmonary stenosis and pulmonary atresia, the more or less hypoplastic pulmonary arteries originating from the right ventricle can be shown by careful echocardiographic investigation (Figs. 24.10a, b and 24.11a).
24.3.2.6 Common Arterial Trunk
In common arterial trunk, the origin of the pulmonary artery from the right ventricle cannot be demonstrated. In common arterial trunk, one or two pulmonary arteries originate from the common arterial trunk (Fig. 24.12) (Deeg 1995; Rice 1982). For the demonstration of the origin of the pulmonary arteries, the suprasternal long or short axis should be performed.

Parasternal short-axis view through the common arterial trunk in a patient with common arterial trunk (TAC). The right (RPA) and left (LPA) pulmonary arteries originate from the common trunk
24.3.2.7 Conclusion
A normal-size right ventricle and normal-size pulmonary arteries with a normal inflow and outflow through the right ventricular outflow tract (colour and pulsed wave Doppler) exclude malformations with obstructions of the right ventricular inflow and outflow tract and the pulmonary artery such as:
-
1.
Tricuspid atresia
-
2.
Tetralogy of Fallot
-
3.
Pulmonary atresia with ventricular septum defect
-
4.
Pulmonary atresia with intact ventricular septum
-
5.
Critical pulmonary stenosis
-
6.
Common arterial trunk
24.3.3 Apical or Subcostal Four-Chamber View
The four-chamber view is 90° to the parasternal long- and short-axis view. Four-chamber views are possible from the apical or subcostal positions. To obtain the apical four-chamber view, the transducer is placed over the apex of the heart. The plane runs through the left shoulder and the right nipple. The size of the “four chambers” (left and right atrium and ventricle) as well as contractility of the ventricles can be estimated (Fig. 24.13a). Additionally the atrioventricular valves can be judged. Normally the tricuspid valve is slightly deeper attached at the ventricular septum than the mitral valve. The inflow of the pulmonary veins into the left atrium can be imaged at the upper border of the left atrium. Colour Doppler provides information of the inflow in both ventricles (Fig. 24.13b). Flow from the atria into the ventricles is displayed red in the apical four-chamber view (Fig. 24.13c). Atresia of the atrioventricular valves (HLHS, TA) can be demonstrated as well as severe valve regurgitation (Ebstein’s anomaly of the tricuspid valve).

Apical four-chamber view. (a) Apical four-chamber view in a healthy neonate. LA left atrium, LV left ventricle, MK mitral valve, PV pulmonary veins, RA right atrium, RV right ventricle, TK tricuspid valve. (b) Inverted subcostal four-chamber view through both atria in a neonate with a small atrial septum defect. LA left atrium, PV pulmonary veins, RA right atrium. (c) Colour Doppler of the inflow in both ventricles. The normal inflow in both ventricles is displayed red. LA left atrium, LV left ventricle, RA right ventricle, RV right ventricle
The four-chamber views provide information of the size and function of both ventricles. Additionally the size and function of the AV valves can be judged. Valvular atresia and severe valvular regurgitation can be seen.
The four-chamber view is normal in TOF and in all other malformations associated with a malalignment VSD and an overriding systemic artery, as the VSD and the overriding artery are located anteriorly to the plane of examination.
A normal apical four-chamber view excludes 6 of the 11 cyanotic cardiac malformations:
-
Hypoplastic left heart syndrome (HLHS) (Deeg 1994a; Goldberg and Rychik 2009; Moniotte and Barrea 2009; Skinner et al. 2000; Snider et al. 1997)
-
Tricuspid atresia with hypoplastic right ventricle (TA) (Deeg 1994b)
-
Pulmonary atresia with intact ventricular septum (PAiVS) (Deeg 1994b)
-
Ebstein’s anomaly of the tricuspid valve
-
Total anomalous pulmonary venous connection (TAPVC)
-
Congestive cardiomyopathy (Colan 2007; Maron 2006; Matitiau 1994; Spencer 2009)
24.3.3.1 Hypoplastic Left Heart Syndrome (HLHS)
-
In cases of hypoplastic left heart syndrome (HLHS), the left ventricle is extremely small and shows insufficient or no contractility (Fig. 24.14a) (Adams et al. 1989; Anderson et al. 1987; Freedom et al. 1992; Goldberg and Rychik 2009; Moniotte and Barrea 2009; Schumacher and Bühlmeyer 1989; Snider et al. 1997; Skinner et al. 2000). The better end of HLHS merges with the poorer end of critical aortic stenosis (Skinner et al. 2000). The mitral and aortic valves are severely stenotic or atretic. In cases of severe stenosis, transvalvular flow or regurgitation can be shown by colour or spectral Doppler, whereas atresia is characterized by missing transvalvular flow (Fig. 24.14b).
Fig. 24.14 
Hypoplastic left heart syndrome. (a) Apical four chamber view. Very small left ventricle with echogenic inner surface, suspicious of endocardial fibroelastosis. Restrictive foramen ovale which bulges from the left to the right atrium (markers). LA left atrium, LV left ventricle, RA right atrium, RV right ventricle. (b) Colour-coded Doppler sonogram in a patient with hypoplastic left heart syndrome. The image shows no flow from the left atrium (LA) to the left ventricle (LV) due to mitral atresia. The left atrium empties through a small foramen ovale. RA right atrium, RV right ventricle

24.3.3.2 Total Anomalous Venous Connection
-
Total anomalous venous connections are characterized by a small left atrium and ventricle, whereas the right ventricle is large (Fig. 24.15). In contrast to hypoplastic left heart syndrome, colour Doppler shows normal inflow into and outflow from the left ventricle and normal contractility of the small left ventricle (Skinner et al. 2000). The demonstration of one or several pulmonary veins which drain into the left atrium excludes total anomalous pulmonary venous return (TAPVR). It is not necessary to show all pulmonary veins. In cases of TAPVR, no pulmonary vein enters the left atrium. In TAPVR the left atrium and left ventricle are very small (Fig. 24.15). Patients with TAPVR always have an atrial septum defect with obligatory right to left shunt. A left to right shunt through an open atrial septum defect and a normal-sized left heart excludes TAPVR. Drainage of the pulmonary veins takes place in three different ways which have to be distinguished: supracardiac, cardiac or infracardiac (Adams et al. 1989; Anderson et al. 1987; Freedom et al. 1992; Goldberg and Rychik 2009; Lai et al. 2009; Schumacher and Bühlmeyer 1989; Snider et al. 1997; Skinner et al. 2000). In the supracardiac form, the confluence of the pulmonary veins connects superiorly to an anomalous vertical vein which drains into the innominate vein which is severely dilated. In the cardiac form, the pulmonary veins drain in the coronary sinus or directly into the right atrium. In the infracardiac form the confluence of the pulmonary veins drain into a descending vertical vein which runs into the portal vein. The differentiation affords detailed echocardiographic knowledge of a paediatric cardiologist, experienced with echocardiography (Lai et al. 2009; Snider et al. 1997; Skinner et al. 2000). It will not be discussed in detail here (see chapter 18 on Anomalous pulmonary Venous connections).
Fig. 24.15 
Total anomalous pulmonary venous return. The apical four-chamber view shows a small left heart and a dilated right heart. LA left atrium, LV left ventricle, RA right atrium, RV right ventricle (Courtesy of Prof. Dr. M. Hofbeck, Tübingen)

24.3.3.3 Tricuspid Atresia
-
In tricuspid atresia and pulmonary atresia with intact ventricular septum, the right ventricle is extremely small and shows insufficient contractility (Figs. 24.16 and 24.17) (Adams et al. 1989; Anderson et al. 1987; Freedom et al. 1992; Goldberg and Rychik 2009; Lai et al. 2009; Schumacher and Bühlmeyer 1989; Snider et al. 1997; Skinner et al. 2000). Patients with tricuspid atresia have no tricuspid valve (Fig. 24.16a, c, d). In other cases, the valve is replaced by an echogenic membrane (Figs. 24.16a and 24.17a). Colour Doppler shows missing flow from the right atrium into the right ventricle (Figs. 24.16c and 24.17b). Tricuspid atresia affords a more or less large atrium septum defect by which blood is drained from the right atrium into the left atrium (Fig. 24.17b). If a ventricular septum defect exists, the lungs are perfused by the ventricular communication (Fig. 24.16d). In these cases, the associated hypoplasia of the pulmonary arteries is only moderate. In tricuspid atresia without a ventricular septum defect, severe right ventricular hypoplasia and pulmonary stenosis or pulmonary atresia are obligatory.
Fig. 24.16 
Tricuspid atresia with small ventricular septum defect. (a) The tricuspid valve is replaced by an echogenic membrane (arrow). The hypoplastic right ventricle is perfused by an associated small ventricular septum defect (markers). LA left atrium, LV left ventricle, RA right atrium, RV right ventricle. (b) Tricuspid atresia with large ASD. Colour Doppler of the flow from the right atrium (RA) into the left atrium (LA) which is displayed blue. The right atrium empties through the large atrial septum defect (markers) into the left atrium. (c) Colour-coded Doppler sonography in tricuspid atresia. No flow from the right atrium (RA) into the right ventricle (RV) can be shown. Normal flow from the left atrium (LA) into the left ventricle (LV). (d) Colour-coded Doppler sonogram of the flow through the ventricular septum defect in a patient with tricuspid atresia. LA left atrium, LV left ventricle, RA right atrium, RV right ventricle, MI mitral insufficiency
Fig. 24.17 
Tricuspid atresia with no ventricular septum defect. (a) Apical four-chamber view (day 5). The right ventricle is extremely hypoplastic as the patient has no ventricular septum defect. The tricuspid valve is replaced by an echogenic membrane (asterisk). The right atrium (RA) is connected with the left atrium (LA) by a large atrial septum defect. The left ventricle (LV) is normal. (b) Colour Doppler of the flow across the large atrial septum defect. As the tricuspid valve is atretic, a pure right to left shunt, displayed red (markers), can be shown. LA left atrium, LV left ventricle, RA right atrium, * hypoplastic right ventricle. (c): Apical four-chamber view in a patient with tricuspid atresia with a small ventricular septum defect. Atretic tricuspid valve (asterisk). Large atrial septum defect. Hypoplastic right ventricle (RV). LA left atrium, LV left ventricle, RA right atrium


24.3.3.4 Pulmonary Atresia with Intact Ventricular Septum
-
In pulmonary atresia with intact ventricular septum, the right ventricle is severely hypoplastic with a small ventricular cavity and hypertrophic poor contractile myocardium (Fig. 24.18a). The tricuspid valve may be atretic or even stenotic. Colour-coded Doppler sonography can distinguish between severe stenosis and atresia. In tricuspid atresia, no flow from the right atrium to the right ventricle can be shown (Figs. 24.16c, d and 24.17b). Cases of severe stenosis are characterized by transvalvular flow or tricuspid insufficiency (Fig. 24.18c). In patients with moderate to severe tricuspid regurgitation, the hypoplasia of the right ventricle is only moderate. Tricuspid insufficiency can be used to measure the pressure gradient between the right atrium and ventricle, which is at or above the systemic pressure. Colour Doppler shows no flow within the right ventricular outflow tract and no transvalvular flow in the parasternal short axis view (Fig. 24.11b, c). Retrograde flow can be displayed by colour Doppler as a mosaic of different colours by an open duct or systemic-pulmonary collaterals (Fig. 24.11b, c). In contrast to patients with primary pulmonary hypertension, ductal flow is entirely left to right. An important difference to patients with pulmonary atresia with VSD is that the pulmonary arteries are usually well formed. There is always a right to left shunt over an open atrial septum defect, as survival is not possible without an interatrial communication. Echocardiography in patients with PAiVS should evaluate the following abnormalities (Levine 2009):
Fig. 24.18 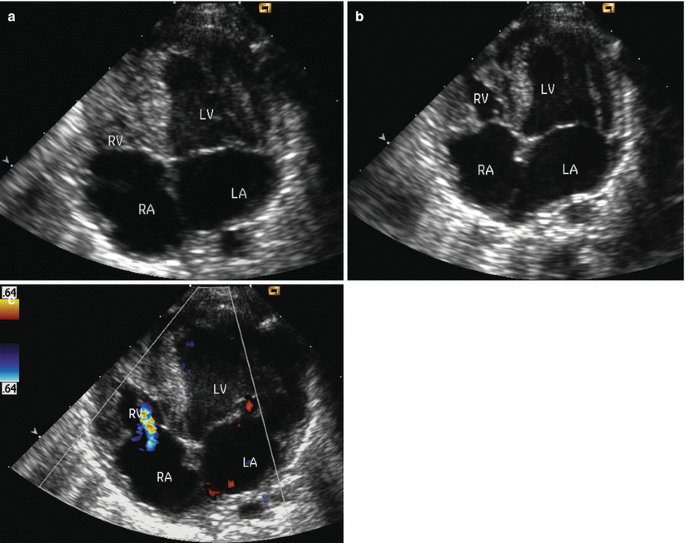
Pulmonary atresia with intact ventricular septum. (a) Apical 4-chamber view. Thick right ventricle (RV) without a significant cavity displayed in systole. LA left atrium, LV left ventricle, RA right atrium. (b) Pulmonary atresia with intact ventricular septum. Thick right ventricle with small cavity (RV) displayed in diastole (peach without stone). LA left atrium, LV left ventricle, RA right atrium. (c) Colour-coded Doppler sonogram in a patient with pulmonary atresia with intact ventricular septum. Flare from the right ventricle (RV) to the right atrium (RA) due to tricuspid insufficiency. LA left atrium, LV left ventricle

-
1.
Size of the cavity of the right ventricle
-
2.
Size of the atrial septal defect
-
3.
Size and function of the tricuspid valve
-
4.
Length of the atretic segment of the right ventricular outflow tract
-
5.
Collateral flow via an open duct or systemic-pulmonary collaterals
-
6.
Side of the aortic arch
24.3.3.5 Ebstein’s Anomaly of the Tricuspid Valve
-
Ebstein’s anomaly of the tricuspid valve is characterized by abnormally low-positioned tricuspid valve leaflets (Fig. 24.19a). Frequently the septum leaflet of the tricuspid valve is adherent to the inner wall of the right ventricle and the ventricular septum. The four-chamber view reveals that the tricuspid valve arises from far lower down the right ventricle than normal. The usual small offset of the mitral and tricuspid valve is greatly exaggerated. The tricuspid valve usually is severely insufficient (Fig. 24.19b). Tricuspid insufficiency can be shown with colour-coded Doppler sonography (Fig. 24.19b). Tricuspid regurgitation raises right atrial pressure. The cavity of the right ventricle is very small, restricting arterial forward flow, whereas the size of the right atrium is markedly increased. The right atrium consists of the “atrialized” portion of the right ventricle and the real right atrium. The area between the true tricuspid annulus, corresponding to the AV-groove, and the coaptation plane of the tricuspid valve leaflets is the “atrialized” right ventricle. The “atrialized” portion of the right ventricle contracts with the right ventricle but is in free communication with the right atrium. This causes to-and-fro flow into the atrium increasing right atrial pressure and impeding forward flow through the right heart and pulmonary artery. The severity of tricuspid regurgitation can be shown by colour-coded Doppler echocardiography (Fig. 24.19b).
The size of the true right ventricle and the pulmonary outflow tract, which can be obstructed by the dysplastic and downward-placed tricuspid valve, must be carefully investigated.
Infants with Ebstein’s anomaly of the tricuspid valve who present with cyanosis in the neonatal period have severe disease and a poor prognosis (Fig. 24.19).

Ebstein’s anomaly of the tricuspid valve. (a) Apical four-chamber view in a patient with Ebstein’s anomaly of the tricuspid valve. Very small right ventricle (RV). Enormously enlarged right atrium (RA) due to apical displacement of the tricuspid valve (TV). Especially the septal leaflet of the tricuspid valve is adherent to the ventricular septum. LA left atrium, LV left ventricle, MV mitral valve. (b) Colour-coded Doppler sonogram in Ebstein’s anomaly of the tricuspid valve. Severe tricuspid regurgitation (mosaic pattern). LA left atrium, LV left ventricle, RA right atrium, RV right ventricle
24.3.3.6 Conclusion
Two normal-size atria and ventricles with normal inflow into the corresponding ventricles exclude all malformations which are associated with severe ventricular hypoplasia, with severe atrioventricular valve stenosis or insufficiency and congestive cardiomyopathy such as:
-
1.
Tricuspid atresia
-
2.
Total anomalous pulmonary venous return
-
3.
Critical pulmonary stenosis and pulmonary atresia with intact ventricular septum
-
4.
Ebstein’s anomaly of the tricuspid valve
-
5.
Congestive cardiomyopathy
-
6.
Hypoplastic left heart syndrome
24.3.4 Summary
The rapid differential diagnosis of the various causes of cyanosis in neonatology includes the diagnosis or exclusion of congenital heart diseases. With three basic echocardiographic views (parasternal long- and short-axis and four-chamber views), all congenital heart malformations can be excluded. All neonatologists should know the elementary basics of echocardiography. This includes the above-mentioned three echocardiographic views which are easy to obtain. If the three sections are normal, cyanotic heart disease can be excluded. If abnormalities are found, a detailed echocardiographic examination by an experienced paediatric cardiologist or neonatologist should be performed.
References
Adams FH, Emmanouillides GC, Riemenschneider TA (1989) Moos’ Heart disease in infants, children and adolescents, 4th edn. Williams & Wilkins, Baltimore
Anderson RH, Macartney FJ, Shinebourne EA, Tynan M (1987) Pediatric cardiology, vol 2. Churchill Livingstone, Edinburgh
Colan SD (2007) Classification of cardiomyopathies. Prog Pediatr Cardiol 23:5–15
Colan SD (2009) Classification of cardiomyopathies. Prog Pediatr Cardiol 23:5–15
Deeg KH (1994) Echokardiographische Diagnose komplexer angeborener Herzfehler mit Ventrikelhypoplasie. I. Herzfehler mit hypoplastischem linken Ventrikel. der Kinderarzt 25:937–945
Deeg KH (1994) Echokardiographische Diagnose komplexer angeborener Herzfehler mit Ventrikelhypoplasie. II. Herzfehler mit hypoplastischem rechten Ventrikel. der Kinderarzt 25:1035–1048
Deeg KH (1994) Echokardiographische Diagnose komplexer angeborener Herzfehler mit überreitender Systemarterie. I. Fallot Tetralogie und Pulmonalatresie mit Ventrikelseptumdefekt 25:1526–1539
Deeg KH (1995) Echokardiographische Diagnose komplexer angeborener Herzfehler mit überreitender Systemarterie. II. Truncus arteriosus communis 26:56–63
Deeg KH (1997) Herz. In: Deeg KH, Peters H, Schuhmacher R, Weitzel D (eds) Die Ultraschalluntersuchung des Kindes, 2nd edn. Springer, Berlin, pp 139–211
Freedom RM, Benson LN, Smallhorn JF (1992) Neonatal heart disease. Springer, Berlin
Goldberg DJ, Rychik J (2009) Hypoplastic left heart syndrome. In: Lai WW, Mertens LL, Cohen MS, Geva T (eds) Echocardiography in pediatric and congenital heart disease. From the fetus to adult. Wiley-Blackwell, Oxford, pp S.315–338
Hanley FL, Sade RM, Blackstone EH et al (1993) Outcomes in neonatal pulmonary atresia with intact ventricular septum. A multi-institutional study. J Thorac Cardiovasc Surg 105:406–423
Lai WW, Mertens LL, Cohen MS, Geva T (2009) Echocardiography in pediatric and congenital heart disease. From the fetus to adult. Wiley-Blackwell, Oxford
Levine JC (2009) Pulmonary atresia with intact ventricular septum. In: Lai WW, Mertens LL, Cohen MS, Geva T (eds) Echocardiography in pediatric and congenital heart disease. From the fetus to adult. Wiley-Blackwell, Oxford, pp 264–282
Lindinger A, Schwedler G, Hense HW (2010) Prevalence of congenital heart defects in newborns in Germany: results of the first registration year of the PAN study. Klin Padiatr 222:321–326
Maron BJ (2006) Contemporary definitions and classification of the cardiomyopathies an American heart association scientific statement from the council on clinical cardiology, heart failure and transplantation committee; quality of care and outcomes research and functional genomics and translational biology interdisciplinary working groups; and council on epidemiology and prevention. Circulation 113:1807–1816
Matitiau A (1994) Infantile dilated cardiomyopathy. Relation of outcome to left ventricular mechanics, hemodynamics, and histology at the time of presentation. Circulation 90:1310–1318
Moniotte StLJ, Barrea C (2009) Functionally univentricular heart. In: Lai WW, Mertens LL, Cohen MS, Geva T (Hrsg) Echocardiography in pediatric and congenital heart disease. From the fetus to adult. Wiley-Blackwell, Oxford, S 459–475
Rice MJ, Seward JB, Hagler DJ (1982) Definitive diagnosis of truncus arteriosus by two dimensional echocardiography. Mayo Clin Proc 57:476–481
Schumacher G, Bühlmeyer K (1989) Diagnostik angeborener Herzfehler, 2nd edn. Perimed, Erlangen
Seward JB, Tajik AJ, Edwards WD, Hagler DJ (1987) Two dimensional echocardiographic atlas. Congenital heart disease, vol I. Springer, New York
Silverman NH, Snider AR (1982) Two dimensional echocardiography in congenital heart disease. Appleton, Norwalk
Skinner J, Alverson D, Hunter S (2000) Echocardiography for the neonatologist. Churchill Livingstone, Edinburgh
Snider AR, Serwer GA, Ritter SB (1997) Echocardiography in pediatric heart disease, 2nd edn. Mosby Year Book, St. Louis
Spencer CT (2009) Dilated cardiomyopathy and myocarditis. In: Lai WW, Mertens LL, Cohen MS, Geva T (eds) Echocardiography in pediatric and congenital heart disease. From fetus to adult. Wiley Blackwell, Chichester, pp 559–580
Waldman JD, Holmes G (2000) The cyanosed newborn: excluding structural heart disease. In: Skinner J, Alverson D, Hunter S (eds) Echocardiography for the neonatologist. Churchill Livingstone, Edinburgh, pp 181–195
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Deeg, KH. (2017). Echocardiographic Differential Diagnosis of Cyanotic Infants. In: Doppler Echocardiography in Infancy and Childhood. Springer, Cham. https://doi.org/10.1007/978-3-319-42919-9_24
Download citation
DOI: https://doi.org/10.1007/978-3-319-42919-9_24
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-42917-5
Online ISBN: 978-3-319-42919-9
eBook Packages: MedicineMedicine (R0)