
Abstract
Impedance-pH monitoring is the most complete reflux test, allowing a full assessment of all reflux episodes, independent of their acidity. It allows assessment of esophageal clearance and of mucosal integrity by means of two recently proposed quantitative impedance parameters, namely, the post-reflux swallow-induced peristaltic wave (PSPW) index and the mean nocturnal baseline impedance (MNBI). Following a reflux episode, secondary peristalsis removes around 90 % of the refluxate (volume clearance); however, esophageal pH is restored only after a swallow elicited by an esophagosalivary reflex delivering salivary bicarbonate (chemical clearance). The PSPW index allows assessment of chemical clearance following acid as well as weakly acidic refluxes with lower values detected in erosive than in non-erosive reflux disease, both significantly lower than in functional heartburn. Impairment of mucosal integrity, even in the absence of macroscopic damage, determines low diurnal and nocturnal baseline impedance. The MNBI consists of the mean of three 10-min nighttime periods, accurately reflecting the 6-h nocturnal bedtime period: lower values have been found in PPI-responsive heartburn patients with normal conventional impedance-pH parameters when compared to PPI refractory cases. The PSPW index and the MNBI have recently been shown to increase the diagnostic yield of impedance-pH monitoring in patients with reflux disease as compared to healthy controls, affording a significant diagnostic gain over pH-only criteria. PSPW index and MNBI should be assessed at least in doubtful cases, and diagnosis of reflux disease should not be dismissed when abnormal values are found. Whether PSPW index and MNBI can predict positive response to anti-reflux interventions remains open issue to be addressed in future studies.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Proton Pump Inhibitor Therapy
- Reflux Episode
- Laparoscopic Fundoplication
- Reflux Event
- Functional Heartburn
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
The principles of impedance were first applied to the gastrointestinal tract in 1991. MII testing was approved by the US Food and Drug Administration for esophageal functional testing in 2002. Impedance measures change in resistance (Ohms) of alternating electrical current passing through pairs of metal rings on a catheter. In the empty esophagus, baseline current is conducted between the rings by ions on the mucosa. Because impedance catheters have multiple sets of impedance-measuring rings, bolus movement and direction (antegrade or retrograde) can be assessed [1].
MII-pH monitoring is performed using a polyvinyl catheter (diameter 2.3 mm) equipped with an antimony pH electrode and several cylindrical electrodes, with a length of 4 mm, placed at intervals of about 2 cm to measure the electrical impedance of the esophageal contents at multiple levels along the longitudinal axis of the esophagus [2]. Each pair of adjacent electrodes represents an impedance-measuring segment corresponding to one recording channel. The catheter is positioned with the pH electrode 5 cm above the LES and the six impedance recording channels at 3, 5, 7, 9, 15, and 17 cm above the manometrically defined lower esophageal sphincter (LES). The overall recording time lasts 24 h.
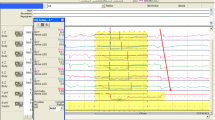
MII-pH provides a detailed characterization of each reflux event including chemical (acid and non-acid reflux) and physical properties (liquid, mixed, gas) [3] (Fig. 14.1). To date, nonacid reflux represents the majority of reflux episodes in patients with gastroesophageal reflux disease (GERD) on proton pump inhibitor (PPI) therapy [4, 5]. Indeed, the total number of reflux episodes is not affected by the acid-suppressive therapy, and weakly acidic refluxes account for approximately 90 % of all reflux episodes on PPI thus representing a potential mechanism underlying failure of PPI treatment in patients with reflux-related symptoms [6, 7]. Moreover, MII-pH monitoring, as well as pH-metry alone, provides the opportunity to assess the temporal relationship between the occurrence of refluxes and the onset of symptoms [8, 9]. The relationship between symptoms and reflux events can be evaluated with symptom index (SI) and symptom association probability (SAP) that are the most commonly employed symptom indices being used [9].

Example of two different reflux events: (a) acid reflux event that involves both distal and proximal channels with a contemporary drop of esophageal pH below 4; (b) non-acid reflux event that involves distal channels only, the pH does not drop below 4. Z1-Z6 impedance detection channels
Based on esophageal pH monitoring, NERD patients with a physiological esophageal acid exposure time (AET) and a close temporal relationship between symptoms and reflux events have been defined as hypersensitive to acid stimuli. On the other hand, in line with Rome III criteria, patients with heartburn, normal upper endoscopy, physiological AET, negative correspondence between symptoms and refluxes, and who fail to respond to PPIs are defined as functional heartburn (FH) [10–12]. In this regard, the advent of MII-pH monitoring improved the diagnostic yield of GERD patients mainly by identifying a positive SAP or SI with weakly acidic or weakly-alkaline refluxes [13–19] both in PPI-responsive and in PPI-refractory patients [20, 21]. Indeed, pH-only monitoring and response to PPI therapy underestimate GERD when with MII-pH criteria [20, 22, 23].
On the other hand, all available diagnostic tests for GERD have some limitations. MII-pH drawbacks are mainly due to the day-to-day variability of the test [24–26]. Additionally, the reflux-symptom correlation in patients with GERD who do not respond to PPI therapy is actually calculated with SI or SAP also if their validity is still uncertain [27, 28]. Recently Zerbib et al. [29] described that MII-pH findings are not always able to predict response to PPIs in patients with reflux-related typical symptoms when the test is performed off-PPI therapy.
Regarding the clinical utility of pathophysiological investigations in patients with heartburn, we described a group of patients (more than 19 % of the whole population enrolled) with heartburn totally suppressed by PPI therapy, in which GERD was not diagnosed with conventional MII-pH criteria [30]. These data suggest that PPI response alone should not always be considered sufficient for GERD diagnosis [30]. Notably, patients with non-erosive reflux disease (NERD) are pathophysiologically heterogeneous and should be accurately studied by means of MII-pH to define the best therapeutic approach [31]. Indeed, a meta-analysis showed that reportedly low response rate in NERD is likely the result of inclusion within this umbrella term of patients with reflux-unrelated heartburn [32].
Recently, the ability of MII-pH testing to better understand GERD’s pathophysiology has been improved through the introduction of up-and-coming parameters such as the post-reflux swallow-induced peristaltic wave (PSPW) index, which stand for the efficacy of esophageal chemical clearance [33], and the nocturnal baseline impedance values (MNBI), which indicates impairment of esophageal mucosa integrity [34].
Frazzoni [33], firstly, defined PSPW as an antegrade 50 % drop in impedance relative to the pre-swallow baseline originating in the most proximal impedance sites, reaching all the distal impedance sites, and followed by at least 50 % return to the baseline in all the distal impedance sites (bolus exit) (Fig. 14.1) [35]. Post-reflux swallows not reaching the distal impedance sites and/or not followed by return to the baseline were excluded. To limit overlap with spontaneous swallowing (64 swallows h−1, approximately 1 min−1) [36] and considering the latency period of salivary gland response to esophageal acidification (10–15 s) [37], only PSPWs occurring within 30 s from the end of reflux episodes were taken into account (Fig. 14.2).

Impedance-pH tracing showing a weakly acidic reflux followed by a swallow-induced peristaltic wave (arrow)
Impairment of esophageal chemical clearance could represent specific mechanism involved in GERD pathophysiology. PSPW index has been showed to be significantly lower in patients with reflux esophagitis and NERD than in healthy controls or in patients functional heartburn (FH), i.e., with reflux-unrelated heartburn. Moreover, this parameter is not altered after medical or surgical therapy [33]. Moreover, Frazzoni et al. [38] showed that patients with PPI-refractory heartburn/regurgitation and refractory reflux esophagitis were associated with a more severe impairment of chemical clearance but similar levels of acid exposure when compared with those patients with healed reflux esophagitis. Adequate acid suppression was found in the majority of patients with refractory reflux esophagitis who did not record any benefit from further PPI escalation [38]. These data confirmed that both contact time of esophageal mucosa with acidic/weakly acidic refluxate and impairment of chemical clearance (PSPW index) play a relevant role in the pathogenesis of refractory reflux esophagitis.
Frazzoni et al. [39] also evaluated the PSPW index in patients with short-segment Barrett’s esophagus with or without mucosal dysplasia. They observed that the PSPW index was significantly lower in patients with than in patients without dysplasia at the time of surveillance (15 %, vs. 32 %; p = 0.001) and at the time of diagnosis too. Statistical analysis showed that a PSPW index <26 % was predictive of incident dysplasia with a 75 % accuracy.
First of all, Farrè and coworkers [34] tested for the first time the hypothesis that multichannel intraluminal impedance (MII) might be a suitable tool for the assessment of esophageal mucosal integrity, by performing in vivo experiments of acid perfusion in rabbits and humans. They also analyzed impedance-pH tracings from patients with GERD. These authors showed that impedance baseline values reflect the status of the esophageal mucosa both in an animal model and in healthy volunteers, indicating that MII is a useful tool to evaluate the esophageal mucosa integrity. They confirmed that patients with erosive and non-erosive esophagitis had a lower impedance baseline compared to healthy volunteers [34].
Further, Kessing et al. [40] described lower values of baseline impedance levels in distal esophagus in patients with abnormal esophageal AET rather than in healthy volunteers (HVs). The authors described a negative correlation between baseline impedance levels and esophageal AET [40]. Woodland et al. [41] observed that, within both NERD and FH, patients who showed a positive acid sensitivity test had lower baseline impedance than those who did not. Of note, the authors found that a subgroup of patients with FH, despite having a normal MII-pH study and a negative response to proton pump inhibitors (PPIs), had baseline impedance values very similar to those of patients with NERD.
These studies evaluated baseline impedance values during the upright period of 24-h MII-pH analysis. Frequently these authors described some difficulties to obtain data on baseline impedance values excluding frequent swallows and reflux events. We recently dedicated our interest in baseline impedance values, and we decided to calculate the baseline value during overnight rest. It seemed easier and less affected from sampling errors. During sleeping esophageal mucosa collapses on the MII-pH probe, allowing a more accurate assessment of the real impedance in the esophageal mucosa. Nocturnal baseline impedance was assessed from the most distal impedance channel. Three 10-min time periods (around 1.00 am, 2.00 am, and 3.00 am) were selected, and the mean baseline for each period was computed with the aid of the software. Time periods including swallows, refluxes, and pH drops were avoided. The mean of the three measurements was manually calculated to obtain a parameter that we defined mean nocturnal baseline impedance (MNBI). In a large group of patients with GERD typical symptoms, negative endoscopy, and normal pathophysiological characteristics (normal AET and number of refluxes, negative SI and SAP), we observed that patients with a good symptom relief after PPI therapy had lower baseline impedance values than PPI-refractory patients with normal pathophysiological characteristics (FH) [42]. FH patients showed similar baseline value than HVs. Moreover, we observed similar results analyzing PSPW index: it was lower in responders than in nonresponders and in HVs. A direct linear correlation between PSPW and baseline impedance values was found [42].
After that preliminary study, de Bortoli et al. [43] decided to extend these analyses to patients with a 24-h MII-pH diagnosis of hypersensitive esophagus (HE) (normal AET and number of reflux events but positive correlation between symptoms and refluxes as established by both positive SI and SAP analyses) [43]. The authors confirmed previous results observed with MNBI and PSPW index: both parameters were lower in patients with HE and those with positive response to PPI therapy but normal pathophysiological findings (FH-PPI responder) compared to healthy controls and FH-PPI non-responders. These results suggest that both MNBI and PSPW index can be helpful to diagnose GERD in patients with heartburn even when SI and SAP are negative or inconclusive [43].
More recently Frazzoni and coworkers [44] aimed to assess the diagnostic accuracy of MNBI and PSPW index in a large multicenter case series of patients with PPI-responsive heartburn. All patients were evaluated after discontinuing PPI-therapy for 1 month. The authors retrospectively studied 68 patients with erosive esophagitis and 221 patients with NERD and compared their result with those observed in 50 healthy controls. In receiver operating characteristic analysis, the area under curve of the PSPW index (0.977; 95 % confidence interval, 0.961–0.993) was significantly greater than that of the other impedance-pH parameters in identifying patients with reflux disease (P < .001). The PSPW index and the MNBI resulted able to identify patients with erosive reflux disease with the highest level of sensitivity (100 % and 91 %, respectively), as well as the 118 pH-positive (99 % and 86 %) and 103 pH-negative (77 % and 56 %) cases of NERD. The PSPW index and the MNBI identified pH-negative NERD with the highest level of sensitivity; values were 82 % and 52 % for the 65 SAP-positive and/or SI-positive cases and 68 % and 63 % for the 38 SAP-negative and SI-negative cases. Diagnoses of NERD were confirmed by pH-only criteria, including those that were positive on the basis of the SAP or SI, for 165 of 221 cases (75 %) and by impedance-pH criteria for 216 of 221 cases (98 %) (P = .001). The authors concluded that the PSPW index and the MNBI increase the diagnostic yield of impedance pH monitoring of patients with reflux disease [44].
Similar results were described by Kandulsky et al. [45]; they observed that baseline impedance values might differentiate patients with ERD or NERD from patients with FH (78 % sensitivity and 71 % specificity) in a population of patients with proton pump inhibitor-refractory reflux related symptoms. Low levels of baseline impedance were associated with greater esophageal acid exposure and dilation of intercellular spaces, confirming that baseline impedance should be considered as a marker of mucosal integrity [45].
Currently, PPI resistance is the real challenge in GERD [46]. However, it has been claimed that between 10 and 40 % of patients with typical reflux symptoms (heartburn/regurgitation) remain symptomatic on a standard dose of PPIs, and many of them will continue to experience symptoms on even high doses of PPIs [47].
What constitutes refractory GERD remains an area of controversy. Most investigators believe that only patients with GERD who exhibit partial or lack of response to PPIs twice daily should be considered as PPI failures [47]. Furthermore, regurgitation persists in many patients despite PPI therapy [48], often awakening patients at night.
Management of PPI-refractory GERD patients is a challenging task. Baclofen could be helpful as add-on therapy with PPIs, but its use is limited by poor tolerability [49] and it is not approved for GERD management. In patients with documented GERD who do not respond sufficiently to PPI therapy, laparoscopic Nissen fundoplication represents the currently suggested treatment modality to overcome PPI failures [50].
Frazzoni et al. [51] aimed to assess reflux parameters in refractory GERD patients before and after EsophyX or laparoscopic fundoplication and their relationship with symptoms. The authors evaluated patients on PPI therapy before intervention and off PPI therapy 3 months after intervention by means of MII-pH monitoring. Distal and proximal refluxes were significantly reduced postoperatively in the surgical but not in the endoscopic (EsophyX) group. The esophageal acid exposure time was normal in 50 % of cases after EsophyX and in 100 % of cases after surgery (P = 0.033). They concluded that EsophyX fundoplication was significantly less effective than laparoscopic fundoplication in improving reflux parameters and in inducing symptom remission in patients with refractory GERD [51].
The same working group [52] aimed to evaluate reflux parameters and their relationship with symptoms before and after laparoscopic fundoplication, on and off PPI therapy, respectively, in patients with PPI-unresponsive heartburn/regurgitation and with a positive symptom-reflux association and/or abnormal reflux parameters detected on PPI therapy. The authors described that esophageal AET (100 %) as well as the number of total (77 %) and proximal reflux (95 %) events and of acid (92 %) and weakly acidic (65 %) refluxes decreased significantly after surgery in patients with refractory GERD. The authors concluded that laparoscopic fundoplication improves acid and weakly acidic reflux parameters when compared with PPI therapy and strongly support that surgical option should be considered in PPI failures patients with GERD confirmed with pathophysiological test [52].
In a recent study, normal reflux parameters and sustained symptom remission at a 3-year follow-up, i.e., GERD cure, were achieved with laparoscopic fundoplication in 90 % of patients with PPI-refractory GERD as diagnosed by on-PPI impedance-pH monitoring [53]. Interestingly, this study shows that weakly acidic refluxes are the main determinants of PPI refractoriness: preoperatively, positive symptom/reflux indexes and abnormal reflux parameters were mainly associated with weakly acidic refluxes; postoperatively, persistent remission of heartburn/regurgitation was associated with total/subtotal abolition of weakly acidic refluxes [53].
On-PPI impedance-pH monitoring is warranted in all PPI-refractory patients before laparoscopic fundoplication in order to establish a cause-and-effect relationship between reflux and heartburn/regurgitation persisting despite PPI therapy; indeed, no reflux pattern can be demonstrated associated with PPI failure at off-PPI testing [29]. Impedance-pH monitoring should always be preceded by esophageal manometry to rule out severe esophageal motility disorders. Surgery is indicated in patients with abnormal impedance-pH parameters and/or positive symptom-reflux associations. When symptom reflux correlation (SI/SAP) fails, PSPW index and MNBI appear ready for prime time. Their applicability and reproducibility are very high, [44] and few additional minutes only are required for their calculation during visual analysis of tracings. Currently, visual analysis of impedance-pH tracings is necessary because automated software analysis is not accurate enough [54]. PSPW index and MNBI appear particularly useful when GERD diagnosis is in doubt, i.e., when esophageal AET and the number of total refluxes are normal and SAP and SI are negative or discordant, or the patient denies symptoms during the impedance-pH study or admits poor accuracy in symptom recording: in these instances, when PSPW index and/or MNBI values are abnormal, GERD diagnosis cannot be dismissed (Fig. 14.3). SAP and SI should not be abandoned, however, as there is some evidence that they can predict positive outcome following laparoscopic fundoplication [53, 55, 56]. Whether PSPW index and MNBI can predict response to anti-reflux interventions remain an open issue to be addressed in future studies.

Diagnostic algorithm for patients with typical reflux symptoms
To conclude, MNBI and PSPW index might be considered up-and-coming parameters that can be helpful to better investigate patients with GERD-related symptoms, particularly when symptom-reflux association indexes fail to do it. These parameters make pathophysiological sense and certainly deserve a chance in redeeming the clinical value of ambulatory pH-impedance testing. For sure, further researches are needed to determine if normal MNBI and PSPW index in the setting of normal pH and normal conventional impedance parameters would be the benchmark for diagnosis of functional esophageal symptoms. Other confounders in the assessment of these parameters need to be evaluated, for instance, the contribution of abnormal motor function or esophageal dilation. Recently Gyawali [57] suggested that software tools need to be developed by companies marketing pH-impedance to simplify calculation of these parameters, as both MNBI and PSPW index need to be rigorously studied and potentially adapted for clinical use in the short term.
References
Dolder M, Tutuian R. Laboratory based investigations for diagnosing gastroesophageal reflux disease. Best Pract Res Clin Gastroenterol. 2010;24(6):787–98. Epub 2010/12/04. eng.
Bredenoord AJ, Pandolfino JE, Smout AJ. Gastro-oesophageal reflux disease. Lancet. 2013;381(9881):1933–42. Epub 2013/03/13. eng.
Zentilin P, Iiritano E, Dulbecco P, Bilardi C, Savarino E, De Conca S, et al. Normal values of 24-h ambulatory intraluminal impedance combined with pH-metry in subjects eating a Mediterranean diet. Dig Liver Dis. 2006;38(4):226–32. Epub 2006/02/17. eng.
Frazzoni M, Savarino E, Manno M, Melotti G, Mirante VG, Mussetto A, et al. Reflux patterns in patients with short-segment Barrett’s oesophagus: a study using impedance-pH monitoring off and on proton pump inhibitor therapy. Aliment Pharmacol Ther. 2009;30(5):508–15. Epub 2009/06/13. eng.
Boeckxstaens GE, Smout A. Systematic review: role of acid, weakly acidic and weakly alkaline reflux in gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2010;32(3):334–43. Epub 2010/05/25. eng.
Mainie I, Tutuian R, Shay S, Vela M, Zhang X, Sifrim D, et al. Acid and non-acid reflux in patients with persistent symptoms despite acid suppressive therapy: a multicentre study using combined ambulatory impedance-pH monitoring. Gut. 2006;55(10):1398–402. Pubmed Central PMCID: 1856433, Epub 2006/03/25. eng.
Zerbib F, Roman S, Ropert A, des Varannes SB, Pouderoux P, Chaput U, et al. Esophageal pH-impedance monitoring and symptom analysis in GERD: a study in patients off and on therapy. Am J Gastroenterol. 2006;101(9):1956–63. Epub 2006/07/20. eng.
Savarino E, Zentilin P, Tutuian R, Pohl D, Gemignani L, Malesci A, et al. Impedance-pH reflux patterns can differentiate non-erosive reflux disease from functional heartburn patients. J Gastroenterol. 2012;47(2):159–68. Epub 2011/11/01. eng.
Bredenoord AJ, Weusten BL, Smout AJ. Symptom association analysis in ambulatory gastro-oesophageal reflux monitoring. Gut. 2005;54(12):1810–7. Pubmed Central PMCID: 1774780, Epub 2005/11/15. eng.
Fass R, Fennerty MB, Vakil N. Nonerosive reflux disease–current concepts and dilemmas. Am J Gastroenterol. 2001;96(2):303–14. Epub 2001/03/10. eng.
Martinez SD, Malagon IB, Garewal HS, Cui H, Fass R. Non-erosive reflux disease (NERD)–acid reflux and symptom patterns. Aliment Pharmacol Ther. 2003;17(4):537–45. Epub 2003/03/08. eng.
de Bortoli N, Martinucci I, Bellini M, Savarino E, Savarino V, Blandizzi C, et al. Overlap of functional heartburn and gastroesophageal reflux disease with irritable bowel syndrome. World J Gastroenterol WJG. 2013;19(35):5787–97. Pubmed Central PMCID: 3793133, Epub 2013/10/15. eng.
Savarino E, Zentilin P, Tutuian R, Pohl D, Casa DD, Frazzoni M, et al. The role of nonacid reflux in NERD: lessons learned from impedance-pH monitoring in 150 patients off therapy. Am J Gastroenterol. 2008;103(11):2685–93. Epub 2008/09/09. eng.
Shay S, Tutuian R, Sifrim D, Vela M, Wise J, Balaji N, et al. Twenty-four hour ambulatory simultaneous impedance and pH monitoring: a multicenter report of normal values from 60 healthy volunteers. Am J Gastroenterol. 2004;99(6):1037–43. Epub 2004/06/08. eng.
Sifrim D, Castell D, Dent J, Kahrilas PJ. Gastro-oesophageal reflux monitoring: review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut. 2004;53(7):1024–31. Pubmed Central PMCID: 1774114, Epub 2004/06/15. eng.
Blondeau K, Tack J. Pro: impedance testing is useful in the management of GERD. Am J Gastroenterol. 2009;104(11):2664–6. Epub 2009/11/06. eng.
Bredenoord AJ, Weusten BL, Timmer R, Conchillo JM, Smout AJ. Addition of esophageal impedance monitoring to pH monitoring increases the yield of symptom association analysis in patients off PPI therapy. Am J Gastroenterol. 2006;101(3):453–9. Epub 2006/02/09. eng.
Savarino E, Pohl D, Zentilin P, Dulbecco P, Sammito G, Sconfienza L, et al. Functional heartburn has more in common with functional dyspepsia than with non-erosive reflux disease. Gut. 2009;58(9):1185–91. Pubmed Central PMCID: 2719081, Epub 2009/05/23. eng.
de Bortoli N, Martinucci I, Savarino E, Franchi R, Bertani L, Russo S et al. Lower pH values of weakly acidic refluxes as determinants of heartburn perception in gastroesophageal reflux disease patients with normal esophageal acid exposure. Dis Esophagus. 2016;29(1):3–9. Epub 2014/09/13. Eng.
Frazzoni M, Conigliaro R, Mirante VG, Melotti G. The added value of quantitative analysis of on-therapy impedance-pH parameters in distinguishing refractory non-erosive reflux disease from functional heartburn. Neurogastroenterol Motil. 2012;24(2):141–6, e87.
Frazzoni M, Conigliaro R, Melotti G. Weakly acidic refluxes have a major role in the pathogenesis of proton pump inhibitor-resistant reflux oesophagitis. Aliment Pharmacol Ther. 2011;33(5):601–6. Epub 2011/01/05. eng.
Savarino E, Tutuian R, Zentilin P, Dulbecco P, Pohl D, Marabotto E, et al. Characteristics of reflux episodes and symptom association in patients with erosive esophagitis and nonerosive reflux disease: study using combined impedance-pH off therapy. Am J Gastroenterol. 2010;105(5):1053–61. Epub 2009/12/10. eng.
Savarino E, Marabotto E, Zentilin P, Frazzoni M, Sammito G, Bonfanti D, et al. The added value of impedance-pH monitoring to Rome III criteria in distinguishing functional heartburn from non-erosive reflux disease. Dig Liver Dis. 2011;43(7):542–7. Epub 2011/03/08. eng.
Savarino E, Zentilin P, Frazzoni M, Cuoco DL, Pohl D, Dulbecco P, et al. Characteristics of gastro-esophageal reflux episodes in Barrett’s esophagus, erosive esophagitis and healthy volunteers. Neurogastroenterol Motil. 2010;22(10):1061–e280. Epub 2010/06/19. eng.
Zentilin P, Dulbecco P, Savarino E, Giannini E, Savarino V. Combined multichannel intraluminal impedance and pH-metry: a novel technique to improve detection of gastro-oesophageal reflux literature review. Dig Liver Dis. 2004;36(9):565–9. Epub 2004/10/06. eng.
Pandolfino JE, Vela MF. Esophageal-reflux monitoring. Gastrointest Endosc. 2009;69(4):917–30, 30 e1. Epub 2009/03/03. eng.
Hershcovici T, Wendel CS, Fass R. Symptom indexes in refractory gastroesophageal reflux disease: overrated or misunderstood? Clin Gastroenterol Hepatol. 2011;9(10):816–7. Epub 2011/07/28. eng.
Slaughter JC, Goutte M, Rymer JA, Oranu AC, Schneider JA, Garrett CG, et al. Caution about overinterpretation of symptom indexes in reflux monitoring for refractory gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2011;9(10):868–74. Epub 2011/07/26. eng.
Zerbib F, Belhocine K, Simon M, Capdepont M, Mion F, Bruley des Varannes S, et al. Clinical, but not oesophageal pH-impedance, profiles predict response to proton pump inhibitors in gastro-oesophageal reflux disease. Gut. 2012;61(4):501–6. Epub 2011/10/15. eng.
de Bortoli N, Martinucci I, Savarino E, Bellini M, Bredenoord AJ, Franchi R, et al. Proton pump inhibitor responders who are not confirmed as GERD patients with impedance and pH monitoring: who are they? Neurogastroenterol Motil. 2014;26(1):28–35. Epub 2013/09/03. eng.
Savarino E, Zentilin P, Savarino V. NERD: an umbrella term including heterogeneous subpopulations. Nat Rev Gastroenterol Hepatol. 2013;10(6):371–80. Epub 2013/03/27. eng.
Weijenborg PW, Cremonini F, Smout AJ, Bredenoord AJ. PPI therapy is equally effective in well-defined non-erosive reflux disease and in reflux esophagitis: a meta-analysis. Neurogastroenterol Motil. 2012;24(8):747–57, e350. Epub 2012/02/09. eng.
Frazzoni M, Manta R, Mirante VG, Conigliaro R, Frazzoni L, Melotti G. Esophageal chemical clearance is impaired in gastro-esophageal reflux disease–a 24-h impedance-pH monitoring assessment. Neurogastroenterol Motil. 2013;25(5):399–406, e295. Epub 2013/01/31. eng.
Farre R, Blondeau K, Clement D, Vicario M, Cardozo L, Vieth M, et al. Evaluation of oesophageal mucosa integrity by the intraluminal impedance technique. Gut. 2011;60(7):885–92. Epub 2011/02/10. eng.
Tutuian R, Vela MF, Balaji NS, Wise JL, Murray JA, Peters JH, et al. Esophageal function testing with combined multichannel intraluminal impedance and manometry: multicenter study in healthy volunteers. Clin Gastroenterol Hepatol. 2003;1(3):174–82.
Bredenoord AJ, Weusten BL, Timmer R, Smout AJ. Reproducibility of multichannel intraluminal electrical impedance monitoring of gastroesophageal reflux. Am J Gastroenterol. 2005;100(2):265–9.
Shafik A, El-Sibai O, Shafik AA, Mostafa R. Effect of topical esophageal acidification on salivary secretion: identification of the mechanism of action. J Gastroenterol Hepatol. 2005;20(12):1935–9. Epub 2005/12/13. eng.
Frazzoni M, Bertani H, Manta R, Mirante VG, Frazzoni L, Conigliaro R, et al. Impairment of chemical clearance is relevant to the pathogenesis of refractory reflux oesophagitis. Dig Liver Dis. 2014;46(7):596–602.
Frazzoni M, Bertani H, Conigliaro R, Frazzoni L, Losi L, Melotti G. Neoplastic progression in short-segment Barrett’s oesophagus is associated with impairment of chemical clearance, but not inadequate acid suppression by proton pump inhibitor therapy. Aliment Pharmacol Ther. 2014;40(7):835–42. Epub 2014/08/05. eng.
Kessing BF, Bredenoord AJ, Weijenborg PW, Hemmink GJ, Loots CM, Smout AJ. Esophageal acid exposure decreases intraluminal baseline impedance levels. Am J Gastroenterol. 2011;106(12):2093–7. Epub 2011/08/17. eng.
Woodland P, Al-Zinaty M, Yazaki E, Sifrim D. In vivo evaluation of acid-induced changes in oesophageal mucosa integrity and sensitivity in non-erosive reflux disease. Gut. 2013;62(9):1256–61. Epub 2012/06/23. Eng.
Martinucci I, de Bortoli N, Savarino E, Piaggi P, Bellini M, Antonelli A, et al. Esophageal baseline impedance levels in patients with pathophysiological characteristics of functional heartburn. Neurogastroenterol Motil. 2014;26(4):546–55. Epub 2014/01/18. eng.
de Bortoli N, Martinucci I, Savarino E, Tutuian R, Frazzoni M, Piaggi P et al. Association between baseline impedance values and response proton pump inhibitors in patients with heartburn. Clin Gastroenterol Hepatol. 2015;13(6):1082–8. Epub 2014/12/17. Eng.
Frazzoni M, Savarino E, de Bortoli N, Martinucci I, Furnari M, Frazzoni L, et al. Analyses of the post-reflux swallow-induced peristaltic wave index and nocturnal baseline impedance parameters increase the diagnostic yield of patients with reflux disease. Clin Gastroenterol Hepatol. 2016;14(1):40–6. Epub 2015/07/01. Eng.
Kandulski A, Weigt J, Caro C, Jechorek D, Wex T, Malfertheiner P. Esophageal intraluminal baseline impedance differentiates gastroesophageal reflux disease from functional heartburn. Clin Gastroenterol Hepatol. 2015;13(6):1075–81.
Cicala M, Emerenziani S, Guarino MP, Ribolsi M. Proton pump inhibitor resistance, the real challenge in gastro-esophageal reflux disease. World J Gastroenterol. 2013;19(39):6529–35. Pubmed Central PMCID: 3801364.
Fass R, Sifrim D. Management of heartburn not responding to proton pump inhibitors. Gut. 2009;58(2):295–309. Epub 2009/01/13. eng.
Broeders JA, Rijnhart-de Jong HG, Draaisma WA, Bredenoord AJ, Smout AJ, Gooszen HG. Ten-year outcome of laparoscopic and conventional nissen fundoplication: randomized clinical trial. Ann Surg. 2009;250(5):698–706. Epub 2009/10/06. eng.
Sifrim D, Zerbib F. Diagnosis and management of patients with reflux symptoms refractory to proton pump inhibitors. Gut. 2012;61(9):1340–54. Epub 2012/06/12. eng.
Kahrilas PJ, Shaheen NJ, Vaezi MF, American Gastroenterological Association I, Clinical P, Quality Management C. American Gastroenterological Association Institute technical review on the management of gastroesophageal reflux disease. Gastroenterology. 2008;135(4):1392–413, 413 e1–5.
Frazzoni M, Conigliaro R, Manta R, Melotti G. Reflux parameters as modified by EsophyX or laparoscopic fundoplication in refractory GERD. Aliment Pharmacol Ther. 2011;34(1):67–75.
Frazzoni M, Conigliaro R, Melotti G. Reflux parameters as modified by laparoscopic fundoplication in 40 patients with heartburn/regurgitation persisting despite PPI therapy: a study using impedance-pH monitoring. Dig Dis Sci. 2011;56(4):1099–106. Epub 2010/08/26. eng.
Frazzoni M, Piccoli M, Conigliaro R, Manta R, Frazzoni L, Melotti G. Refractory gastroesophageal reflux disease as diagnosed by impedance-pH monitoring can be cured by laparoscopic fundoplication. Surg Endosc. 2013;27(8):2940–6. Epub 2013/02/26. Eng.
Roman S, Bruley des Varannes S, Pouderoux P, Chaput U, Mion F, Galmiche JP, et al. Ambulatory 24-h oesophageal impedance-pH recordings: reliability of automatic analysis for gastro-oesophageal reflux assessment. Neurogastroenterol Motil. 2006;18(11):978–86.
Patel A, Sayuk GS, Gyawali CP. Parameters on esophageal pH-impedance monitoring that predict outcomes of patients with gastroesophageal reflux disease. Clin Gastroenter Hepatol. 2015;13(5):884–91. Epub 2014/08/28. Eng.
Desjardin M, Luc G, Collet D, Zerbib F. 24-hour pH-impedance monitoring on therapy to select patients with refractory reflux symptoms for antireflux surgery. A single center retrospective study. Neurogastroenterol Motil. 2016;28(1):146–52.
Gyawali CP. Redeeming clinical value of esophageal pH impedance monitoring. Clin Gastroenterol Hepatol. 2016;14(1):47–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
de Bortoli, N., Frazzoni, M., Savarino, E. (2017). The Diagnostic Yield of Novel Parameters in Reflux Monitoring. In: Conigliaro, R., Frazzoni, M. (eds) Diagnosis and Endoscopic Management of Digestive Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-42358-6_14
Download citation
DOI: https://doi.org/10.1007/978-3-319-42358-6_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-42356-2
Online ISBN: 978-3-319-42358-6
eBook Packages: MedicineMedicine (R0)