
Abstract
Israel is a nation of immigrants from many countries. From 1989 to 1998, the Israeli population of 4.5 million rose about 20 % primarily from the nearly one million Soviet immigrants, mostly from Russia and the Ukraine, who entered the country. A large proportion of the Russian-speaking immigrants had training and education in a variety of technical and professional fields, and success was an important component of their world view and culture. However, there were immigrants who arrived in Israel with drug abuse problems and others became addicted during the absorption process. Presently, Russian-speaking immigrants are 13 % of the Israel population, but about 25 % of the illicit drug users in the country. Difficulties with the process of acculturation have been linked to the development of emotional and behavioral problems including mental illness, delinquency, and alcohol and drug abuse. And, alcohol and drug use emerges as a coping mechanism to mitigate the stresses that immigrants encounter in the host society. This chapter examines the dynamic and highly complex process of acculturation that can lead to mental health and addiction related problems. A number of conceptual models of acculturation are presented applicable to many different people in many different countries.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Since 1991, with the fall of the Soviet Union and removal of exit barriers, over a million people immigrated from the former Soviet Union (FSU) to Israel. A large proportion of the FSU immigrants had training and education in technical and professional fields (Philippov, 2010). Additionally, there were immigrants who arrived in Israel with drug abuse problems and others became addicted during the absorption process (Isralowitz, Reznik, Spear, Brecht, & Rawson, 2007). FSU immigrants are 11 % of the Israeli population but about 25 % of the estimated 30,000 illicit drug users in the country (Isralowitz et al., 2007). The FSU drug users are mostly from Russia and the Ukraine; others originated from Georgia and the Caucasus region that includes Azerbaijan and the Russian Federation republics of Dagestan, Chechnya, and Ingushetia (see Fig. 8.1). FSU immigrants came from an environment that has poor health indicators and life expectancies caused, in part, from high rates of alcoholism, heroin use, and infectious disease (Hofmann, 2012). Russia, for example, has 2.5 million drug addicts and over 5.1 million drug users; and HIV infection rates are up to 61 % among drug users in some regions of the country linked, in part, to injecting drugs. Both hepatitis B virus (HBV) and hepatitis C virus (HCV) infections are highly prevalent among injection drug users. It is logical to believe there are uniform data about the health issues among FSU immigrants in Israel and other absorbing countries. However, a review of professional literature reveals scant information about drug use, risk behaviors, police reports, and service utilization (Guarino, Moore, Marsch, & Florio, 2012; Isralowitz, Straussner, & Rosenblum, 2006). This chapter focuses on acculturation as a factor related to drug use, infectious disease, and health among FSU immigrants who became addicted before or after immigration to Israel.

Ethnic origins among FSU immigrant drug users
2 Pre-immigration Stage
“Emigration is defined as leaving one’s native country, or country of origin, and settling in another. It is related to immigration, but from the perspective of the sending country…. [the action is] based on a variety of motivations including religious, political, and economic” (Loue & Sajatovic, 2012, pp. 598–599). The reasons and motives of immigration may be described in terms of “push-pull” factors. Push factors include unemployment; oppression due to political, religious, or ethnic affiliations; lack of opportunities for personal development, employment, or marriage; and disasters such as floods, earthquakes, fire, war, or epidemics. Pull factors include improved opportunities for employment, higher income, or education, higher environment and living conditions, medical services, and more (Bansal, Taylor, & James, 2005). Additional factors for immigration include personality and psychosocial variables (e.g., behavioral norms, obligations, attitudes, values) that may facilitate or hinder immigration decisions (Moon, 1995). Many norms, attitudes, and values that influence immigration decision-making are reflective of a national mentality (e.g., attitudes toward themselves and attitudes toward country of origin among Russian-speaking people) (Abulkhanova, 1997). This factor, known as “mooring,” along with “push-pull” issues makes up a major paradigm of migration research (Bansal et al., 2005). Using the push, pull, mooring (PPM) model, four types of reasoning (i.e. realist, runaway, romantic, and Zionism) help explain why FSU people immigrate to Israel (Reznik & Isralowitz, 2011) (see Fig. 8.2).

Immigrant classification. Reznik and Isralowitz, modification of figure from Abulkhanova (1997)
Type 1: “Realist.” This is a relatively problem-free category of immigrants. Some people of this group had drug or alcohol use problems before their immigration and try to give up their harmful habits understanding its negative impact on their plans to get on with a productive and positive new life. However, difficulties related to interfamily relations or a change of their social status may trigger a return to their harmful behavior.
Type 2: “Runaway.” In this case, migrants include those who “failed” in their “home” country or had to “run away” from it for any one of many reasons. Personal attitudes of mistrust and suspicion toward their home country may result in moving on to a new country where addiction problems are better addressed. Consequently, this group tends to include disappointed immigrants who think their immigration was a mistake. They do not bother learning the language of the host, do not look for work; and, do not care about learning a new profession. Over time, the health and well-being of such people deteriorate. Drugs and/or alcohol is used as an escape from the “harsh” realities they face as immigrants.
Type 3: “Romantic.” This period before emigration is characterized by romantic and idealized attitudes toward the new country where everything, including personal and social problems, is fine. The new country is associated with opportunities of education, affluence, treatment of addiction and health problems, and care of the elderly. The host country is viewed in a “paternal, supportive, and caring” context for migrants. When reality sets in and expectations are not met, immigrants of this category may start to use drugs to cope with disappointment.
Type 4: “Zionist.” This type of immigrants is characterized by a bonding between self and Israel. Immigration can be explained by ideological or religious motives. “Zionists,” who support a nationalist movement of a home land for Jewish people, their culture, and religion, are aware of possible problems and difficulties in the new country but it does not stop them from immigrating.
3 Acculturation: Theoretical Perspectives
The term “acculturation” is used to define a set of changes, both at the psychological and social level, which immigrants usually experience in order to facilitate their own settlement to host societies. At the individual level, the term acculturation denotes a complex series of psychological and interpersonal changes that occur when an immigrant experiences a first-hand encounter with a new culture. These encounters may precipitate psychological adaptations (e.g., changes in behaviors and beliefs, identities, values, and attitudes) that are made in order to thrive in the new cultural environment (Encyclopedia of Immigrants Health, 2014, p. 149).
Early models and theories of acculturation saw it as a linear process with immigrants moving unidirectionally from unassimilated to assimilated (i.e. the melting pot). It is now recognized that (a) acculturation is a multidimensional process, (b) complete acculturation requires several generations, and (c) acculturation results are not always positive (Chun, Balls Organista, & Marín, 2003; Unger et al., 2004). Additional views of acculturation reflect the complexity of this process (Alegría et al., 2008; Rudmin, 2003; Schwartz, Unger, Zamboanga, & Szapocznik, 2010) including its planning stages prior to departure, the acculturation process per se, and assessment/evaluation of the adjustment process.
The fourfold theory of acculturation is a popular model contributing to understanding the process (Berry, 1997; Rudmin, 2003). This theory presumes that a person can appreciate, practice, and/or identify with two different cultures (native culture and host culture) independently of one another. As shown in Fig. 8.3, each culture can have a positive or negative influence on a person’s attitudes, preferences, attachment, identification, and other conditions that may be evidenced by the presence or absence of certain behaviors, language use, ethnic names, dress, eating habits, and other observable manifestations of culture—their acceptance or rejection (Berry, 1997; Rudmin, 2003).

Acculturation strategies. Used with permission from John Wiley and Sons: Berry, J. (1997). Immigration, acculturation, and adaptation. Applied Psychology: An International Review, 46(1), 5–34
-
Drawing from this theoretical model (Berry, 1997), the four acculturation strategies noted above have been evidenced by alcohol- and drug-using FSU and Ethiopian immigrants to Israel during the last 25 years or so (Fedorova, 2012; Reznik & Isralowitz, 2011; specifically, pp. 117–120).
-
Separation relates to the desire of immigrants to retain their cultural traditions and lifestyles characteristic of their country of origin. They have minimal contact with representatives of a new culture. Such immigrants often aggregate into certain communities of people of a single ethnic origin. Their status in this case is “I am OK but in a country that is alien.”
-
Marginalization presupposes the renunciation of certain cultural conditions and the inability to adjust to another culture and accept new norms, values, and settings. Marginalization of some immigrants is a serious challenge for many countries. Their personal status is “an alien in an alien country.”
-
Assimilation presupposes a willingness to overcome cultural distance at the expense of partial or full renunciation of former cultural identity. Immigrants try to quickly learn the language and change their behavior, eating habits, appearance, and more. They start to actively communicate with the host population. Their status in this case is “an alien in their own country.”
-
Integration includes the ability to retain former cultural identity and acceptance of the new culture. Such immigrants feel quite comfortable in both cultural environments. Their condition can be described as of “being in their own country.”
According to Berry (2005), immigrants of the integrated acculturation strategy are least stressed reflecting the ability to access resources and a wide array of coping skills. Those marginalized, on the other hand, tend to be the most stressed. Immigrants in the assimilation and separation groups tend to be somewhere in between. In a study of Russian-speaking immigrants who came to Israel as children or who were born in Israel to their immigrant parents, most do not feel being Israeli or being from the FSU (Lobich, 2007). A similar situation in Germany has been reported of young migrants from Russia who are seen as high at risk for drug and alcohol addiction as well as criminality (Hoffmann, 2007).
4 Immigration, Acculturation, and Meaning of Life
Research shows the meaning of life linked to positive acculturation; it is a protective measure against the pathological behaviors including depression, anxiety, and suicidal tendencies associated with negative acculturation among immigrants (Crumbaugh, Wood, & Wood, 1980; Pan, Fu Keung Wong, Lai Wan Chan, & Joubert, 2008; Wilchek-Aviad, 2014). Also, it is a factor associated with drug use as well as its prevention and treatment (Crumbaugh, 1981; Crumbaugh, Wood, & Wood, 1980; Henrion, 2002; Holmes, 1991; Hutzell, 1984; Koster, 1991; Nicholson et al., 1994; Schulenberg, Hutzell, Nassif, & Rogina, 2008). Marsh, Smith, Piek, and Saunders (2003) found meaninglessness life associated with alcohol (and other drug uses); and it has been linked to cigarette smoking (Konkolÿ Thege, Bachner, Martos, & Kushnir, 2009).
Reflecting on the work of Viktor Frankl (1968), it is possible to gain insight of people caught up in the immigration process—their success, failure, positive understanding of life, or despair (see Fig. 8.4). These conditions can be applied to understanding drug use among immigrants (Fedorova, 2012; Reznik & Isralowitz, 2011).

Results of immigration. Used with permission from: Frankl, V (1968). Psychotherapy and Existentialism: Selected Papers on Logotherapy. New York: Washington Square Press, Inc., via Viktor Frankl Book Rights. Langwiesgasse 6, A 1140 Vienna
Zone 1 “Meaning and Success” includes immigrants who successfully adapt to new sociocultural conditions.
Zone 2 “Despair and Success” includes those who achieve something in the new country but have a low level of psychological comfort. They may have lost a sense of meaning about their existence that leads to an “existential vacuum” and possible “noogenic neurosis”—a type of neurosis caused by the loss of meaning (Frankl, 1968). For immigrants from Zone 2, alcohol and/or drug use is often a means to reduce the vacuum and neurosis.
Zone 3 “Failure and Despair” reflects immigrants with collapsed hopes for a dignified future and stable life. Unsuccessful adaptation and loss of meaning in life drive many immigrants to depression and inability to cope with life without the use of drugs and/or alcohol. This group is most in need of social and health services.
Zone 4 “Failure and Meaning” includes people who are ready to overcome difficulties to achieve their goals. Despite the fact that they have not yet achieved success, they can be the winners in any endeavor.
5 Immigration as a Multistage Process
Immigration is a multistage process consisting of preparation, acculturation, assessment, and evaluation phases (Reznik & Isralowitz, 2011) (see Fig. 8.5). Based on the discussion above, it may be possible to select appropriate intervention strategies to support immigrant clients providing there is a readiness by the host country to adjust its social institutions to the needs of ethnic groups. Overcoming acculturation stress is not just an individual’s problem but rather it is one of all those involved in the general migration process—from the local community and its people to various helping services and organizations.

Immigration and acculturation. From Reznik and Isralowitz (2011)
6 Acculturation and Drug Use: A Brief Review
Difficulties with the process of acculturation have been linked to the development of emotional and behavioral problems including mental illness, delinquency, and alcohol and drug abuse (Oetting & Beauvais, 1991; Rogler, Cortes, & Malgady, 1991). Cortes et al. (2003) state that alcohol and drug use emerges as a coping mechanism to mitigate the stresses that immigrants encounter in the host society. This dynamic and highly complex process can lead to personal stress and interpersonal conflicts (Akhtar, 1995; Gaw, 1993; Lu, Lim, & Mezzich, 1995; Sandhu, Portes, & McPhee, 1996). FSU immigrants, regardless of the absorbing country, have faced the challenge of acculturation and there is a lack of information about those who are drug users (Isralowitz, 2002; Isralowitz et al., 2007; Isralowitz & Reznik, 2013).
7 Acculturation and Addiction Among FSU Immigrants: A Prospective Study
FSU-born male drug users were surveyed in Israeli treatment centers from 2002 to 2012. Among this study group, 52 % (n = 282) were addicted before and 48 % (n = 258) after immigration. The sampling procedure was cross sectional and geared to collecting psychosocial data to estimate drug abuse in the country.
Interviewers made scheduled visits to four treatment sites and invited individuals to participate in the study. The treatment sites included an intake center, a detoxification clinic, a methadone clinic, and a day-treatment facility. These sites represent the types of treatment facilities available throughout the country. Data were collected in a voluntary, anonymous, and confidential manner complying with human subject guidelines of the participating drug treatment facilities and Ben-Gurion University. A staff member responsible for the interview was available to help understand the questions if necessary.
Instruments For this study, all drug use, psychosocial, and health data were based on participants’ self-report. The primary data collection tool was the Addiction Severity Index (ASI) , 5th Edition (McLellan et al., 1992). Participants were asked to report medical problems including hepatitis C (HCV), HIV/AIDS, and tuberculosis (TB). In Israeli treatment centers, patients are routinely tested for HCV, HIV/AIDS, and TB and given their results by clinic staff. Other data collection instruments used were adult version of the Substance Survey Instrument (SUSI) that consists of 56 questions about personal background characteristics, substance use patterns, and related problem behavior. Additional measures included questions about age at immigration and time spent in the country; the causes, motives, conditions, and circumstances of emigration; the process of acculturation/adaptation; and, immigration successes and failures including the Short Acculturation Scale (SAS) (Marin, Sabogal, Marin, Otero-Sabogal, & Perez-Stable, 1987). These instruments are described by Isralowitz, Affifi, and Resnik (2016). Cronbach alpha reliability scores of the instruments used were ASI (0.71), SUSI (0.88), and SAS (0.91)Footnote 1.
7.1 Results
7.1.1 Pre-immigration Stage
Analysis of interviews showed that the majority of respondents (60 %), in terms of motives, causes, and circumstances of emigration, can be categorized as “fugitives.” Causes of flight were dispersed including economic difficulties, threat to life (Chechnya and Transnistria wars), ethnic pogroms and conflicts in Azerbaijan and the Central Asian Republics, and unwillingness to serve in the army and/or problems with police, the courts, and jail.
Those that can be labeled “romantics” made up 30 % of the study respondents including those who moved to Israel in the 1990s thinking this might be their “last chance” to get out before border closes again, better life conditions exist in Israel, there is an opportunity to receive treatment for drug and/or alcohol treatment, an opportunity exists to visit another country without cost, and there is a possibility to participate in a youth educational or vocational program sponsored by the countryFootnote 2.
A smaller group of the study respondents can be categorized as “realists.” As mentioned above, they understand that drug and/or alcohol use can undermine their plans in the new country. However, when faced with difficulties related to family relations or the change of their social status, they could “break” returning to addiction. This was the case for 10 % of the study group 7–8 years after immigration. Not a single person in the study reported immigration to Israel as a “Zionist.”
7.1.2 Acculturation
Among the majority of immigrants interviewed, poor knowledge of Hebrew and the lack of close friends in Israel reflect conditions of marginalization.
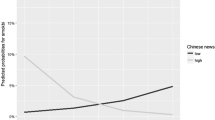
The 12-item Short Acculturation Scale (SAS) addresses factors about language use, media, and ethnic social relations. The scale utilizes a 5-point Likert scale. For items assessing language and media preference, the score ranges from “only Russian” (score = 1) to “only Hebrew” (score = 5). For items assessing ethnic social relations, the score ranges from “all FSU immigrants” (score =1) to “all Israeli” (score =5). Total scores range from 1 to 5. An overall average of 2.99 should be used as a bench mark to differentiate the less and more acculturated respondents. In other words, a respondent is less acculturated if the average score is between 1 and 2.99 and more acculturated if the average score is greater than 2.99 (Davis & Engel, 2011). Study results show the overall average of 1.99 (SD = 0.59) for the 12 item SAS. Only 7.5 % of the sample had a rate of acculturation higher than 2.99.
Immigration at an early age and length of time in Israel were linked to higher values of acculturation. Immigration status (i.e. alone or with partner/parents) is associated with the rate of acculturation. Other findings show positive acculturation connected with work status and whether the drug treatment facility has Russian-speaking personnel. Additional analyses show drug use before immigration is the central factor that negatively affects successful immigration among FSU addicts (Isralowitz & Reznik, 2013).
8 Discussion and Conclusion
Analyses from interviews and data show the typical FSU addict is male, single (71 %); 32 years old, living in Israel for 18 years with no close friends (65 %); poor health and a chronic disease (76 %); fear, anxiety, and depression (72 %); and having poor knowledge of Hebrew that is not used in everyday life. The average FSU addict has a profession (79 %), but is unemployed or underemployed (57 %) and has spent time in jail/prison (59 %).
Since the mass immigration of Russian-speaking immigrants to Israel beginning in the late 1980s, research has been conducted evidencing the difficulty of leaving behind a familiar language, culture, and community and its connection with increased risk of psychosocial problems, acculturation, risk-taking behavior, and drug use (Isralowitz, 2002; Reznik & Isralowitz, 2011).
Policy and program decision-makers in Israel have talked about the need for special services to Russian-speaking addicts as well as separate services. However, little has been done to address the issue, and over time, there is growing evidence of acculturation and a diminished need for separate services based on group status (i.e. Russian-speaking immigrant drug users) (Isralowitz & Reznik, 2013, 2014; Isralowitz, Reznik, & Pruginin, 2016). Specifically, there is little long-term evidence that separate programs for special populations are superior to mainstream efforts; but, that does not mean the special needs of immigrant populations, including those related to acculturation , should be ignored (Yehudai, Sarid, Reznik, Findley, & Isralowitz, 2016).
9 Future Directions
This chapter points to the need for additional research of the relationship between acculturation and psychological and behavior outcomes associated with drug use. Such research needs to take into account multiple theoretical models of acculturation addressing stress, assimilation, biculturalism , and other factors as a pliable process in which individuals do not necessarily relinquish the values, behaviors, and attitudes prescribed by their culture of origin in order to adopt those of the host culture.
Notes
- 1.
The Substance Use Survey Instrument (SUSI) may be obtained from the Ben-Gurion University Regional Alcohol and Drug Abuse Research (RADAR) Center by contacting Professor Richard Isralowitz at richard@bgu.ac.il. The SUSI is available in English, Hebrew, and Arabic.
- 2.
This is the most dramatic subgroup. Start of drug use led to immediate dismissal from the program. After dismissal the young man found himself alone in a strange country and did not always have the opportunity (or desire) to return to their country.
References
Abulkhanova, K. (1997). Russian mentality: Cross-cultural and typological approaches. In K. Abulkhanova, A. Brushhnsky, & M. Volovikova (Eds.), Russian mentality: The issues of psychological theory and practice (pp. 7–37). Moscow: Institute of psychology RAS (Russian).
Akhtar, S. (1995). A third individuation: Immigration, identity and the psychoanalytic process. Journal of the American Psychological Association, 43(4), 1051–1084.
Alegría, M., Canino, G., Shrout, P., Woo, M., Duan, N., Vila, D., et al. (2008). Prevalence of mental illness in immigrant and non-immigrant U.S. Latino groups. American Journal of Psychiatry, 165(3), 359–369.
Bansal, H., Taylor, S., & James, Y. (2005). “Migrating” to new service providers: Toward a unifying framework of consumers’ switching behaviors. Journal of the Academy of Marketing Science, 33(1), 96–115.
Berry, J. (1997). Immigration, acculturation, and adaptation. Applied Psychology: An International Review, 46(1), 5–34.
Berry, J. (2005). Acculturation: Living successfully in two cultures. International Journal of Intercultural Relations, 29(6), 697–712.
Chun, K., Balls Organista, P., & Marín, G. (Eds.). (2003). Acculturation: Advances in theory, measurement, and applied research. Washington, DC: American Psychological Association.
Cortes, D., Deren, S., Andia, J., Colon, H., Robles, R., & Sung-Yeon, K. (2003). The use of the Puerto Rican biculturality scale with Puerto Rican drug users in New York and Puerto Rico. Journal of Psychoactive Drugs, 35(2), 197–207.
Crumbaugh, J. (1981). Logotherapy: New help for problem drinkers. The International Forum for Logotherapy, 4(1), 29–34.
Crumbaugh, J., Wood, W., & Wood, W. (1980). Logotherapy: New help for problem drinkers. Chicago, IL: Nelson-Hall.
Davis, L., & Engel, R. (2011). Measuring race and ethnicity. New York: Springer.
Fedorova, O. (2012). Transcultural drug work. A handbook for practitioners working with drug users from different ethnic and cultural backgrounds. Strasbourg, France: Council of Europe–Pompidou Group.
Frankl, V. (1968). Psychotherapy and Existentialism: Selected papers on logotherapy. New York: Washington Square Press.
Gaw, A. (Ed.). (1993). Culture, ethnicity, and mental illness. Washington, DC: American Psychiatric Press.
Guarino, H., Moore, S., Marsch, L., & Florio, S. (2012). The social production of substance abuse and HIV/HCV risk: An exploratory study of opioid–using immigrants from the Former Soviet Union living in New York City. Substance Abuse Treatment, Prevention, and Policy, 7(2), 1–14.
Henrion, R. (2002). Alcohol use disorders: Alcohol dependence. The International Forum for Logotherapy, 25(1), 30–38.
Hoffmann, K. (2007). Spätaussiedler und ihre Angehörigen als Patienten im Maßregelvollzug./Migrants from the former Soviet Union born in German families and their relatives as patients in forensic units. Psychiatrische Praxis, 34(7), 320–324.
Hofmann, E. (2012). The burden of culture? Health outcomes among immigrants from the Former Soviet Union in the United States. Journal of Immigrant and Minority Health, 14(2), 315–322.
Holmes, R. (1991). Alcoholics Anonymous as group logotherapy. The International Forum for Logotherapy, 14(1), 36–41.
Hutzell, R. (1984). Logoanalysis for alcoholics. The International Forum for Logotherapy, 7(1), 40–45.
Isralowitz, R. (2002). Drug use, policy and management (2nd ed.). Westport, CT: Auburn House.
Isralowitz, R., Afifi, M., & Reznik, A. (2016). Toward uniform data collection and monitoring of Israeli and Palestinian adolescent drug use. In R. Isralowitz & P. A. Findley (Eds.), Mental health and addiction care in the Middle East (pp. 47–58). New York: Springer.
Isralowitz, R., & Reznik, A. (2013). Russian speaking Immigrants: Drug use, infectious disease and related health behavior. Journal of Immigrant and Minority Health, 15, 851–857.
Isralowitz, R., & Reznik, A. (2014). Ethiopian origin high risk youth: A cross cultural examination of alcohol use, binge drinking and problem behavior. Journal of Ethnicity in Substance Abuse, 13(2), 179–184.
Isralowitz, R., Reznik, A., Spear, S., Brecht, M., & Rawson, R. (2007). Severity of heroin use in Israel: Comparisons between native Israelis and Former Soviet Union immigrants. Addiction, 102(4), 630–637.
Isralowitz, R., Reznik, A. & Pruginin, I. (2016). Quality of life among Former Soviet Union and Israeli origin methadone Users, Journal of Ethnicity in Substance Abuse, forthcoming.
Isralowitz, R., Straussner, L., & Rosenblum, A. (2006). Drug abuse, risks of infectious diseases and service utilization among Former Soviet Union Immigrants: A view from New York City. Journal of Ethnicity in Substance Abuse, 5(1), 91–96.
Konkolÿ Thege, B., Bachner, Y., Martos, T., & Kushnir, T. (2009). Meaning in life: Does it play a role in smoking? Substance Use & Misuse, 44(11), 1566–1577.
Koster, M. (1991). A view of logotherapy from the alcoholic field. The International Forum for Logotherapy, 14(2), 103–105.
Lobich, V. (2007). Third of young immigrants reported: We used drugs. Retrieved October 5, 2014 (Hebrew), from http://www.ynet.co.il/Ext/Comp/ArticleLayout/CdaArticlePrintPreview/1,2506,L-3450605,00.html#n
Loue, S., & Sajatovic, M. (Eds.). (2012). Encyclopedia of immigrant health. New York: Springer.
Lu, F., Lim, R., & Mezzich, J. (1995). Issues in the assessment and diagnosis of culturally diverse individuals. American Psychiatric Press Review of Psychiatry, 14, 477–510.
Marin, G., Sabogal, F., Marin, B., Otero-Sabogal, R., & Perez-Stable, E. (1987). Development of a short acculturation scale for Hispanics. Hispanic Journal of Behavioral Sciences, 9(2), 183–205.
Marsh, A., Smith, L., Piek, J., & Saunders, B. (2003). The Purpose in Life Scale: Psychometric properties for social drinkers and drinkers in alcohol treatment. Educational and Psychological Measurement, 63(5), 859–871.
McLellan, A., Kushner, H., Metzger, D., Peters, F., Smith, I., Grissom, G., et al. (1992). The fifth edition of the Addiction Severity Index. Journal of Substance Abuse Treatment, 9(3), 199–213.
Moon, B. (1995). Paradigms in migration research: Exploring “moorings” as a schema. Progress in Human Geography, 19(4), 504–524.
Nicholson, T., Higgins, W., Turner, P., James, S., Stickle, F., & Pruitt, T. (1994). The relation between meaning in life and the occurrence of drug abuse: A retrospective study. Psychology of Addictive Behaviors, 8(1), 24–28.
Oetting, E., & Beauvais, F. (1991). Orthogonal cultural identification theory: The cultural identification of minority adolescents. International Journal of the Addictions, 25(5A–6A), 655–685.
Pan, J.-Y., Fu Keung Wong, D., Lai Wan Chan, C., & Joubert, L. (2008). Meaning of life as a protective factor of positive affect in acculturation: A resilience framework and a cross-cultural comparison. International Journal of Intercultural Relations, 32(6), 505–514.
Philippov, M. (2010). Ex-Soviets in the Israeli political space: Values, attitudes, and elective behavior. College Park, MD: Gildenhorn Institute of Israel Studies/University of Maryland.
Reznik, A., & Isralowitz, R. (2011). Immigrants and drugs: Demographic, statistical and cultural analysis. Moscow: Ves Mir (Russian).
Rogler, L., Cortes, D., & Malgady, R. (1991). Acculturation and mental health status among Hispanics: Convergence and new directions for research. American Psychologist, 46(6), 585–597.
Rudmin, F. (2003). Critical history of the acculturation psychology of assimilation, separation, integration, and marginalization. Review of General Psychology, 7(1), 3–37.
Sandhu, D., Portes, P., & McPhee, S. (1996). Assessing cultural adaptation: Psychometric properties of the Cultural Adaptation Pain Scale. Journal of Multicultural Counseling and Development, 24(1), 15–25.
Schulenberg, S., Hutzell, R., Nassif, C., & Rogina, J. (2008). Logotherapy for clinical practice. Psychotherapy: Theory, Research, Practice, Training, 45(4), 447–463.
Schwartz, S., Unger, J., Zamboanga, B., & Szapocznik, J. (2010). Rethinking the concept of acculturation. American Psychologist, 65(4), 237–251.
Unger, J., Baezconde-Garbanati, L., Shakib, S., Palmer, P., Nezami, E., & Mora, J. (2004). A cultural psychology approach to “drug abuse” prevention. Substance Use & Misuse, 39(10–12), 1779–1820.
Wilchek-Aviad, Y. (2014). Meaning in life and suicidal tendency among immigrant (Ethiopian) youth and native-born Israeli youth. Journal of Immigrant and Minority Health, 17(4), 1041–1048.
Yehudai, M., Sarid, O., Reznik, A., Findley, P., & Isralowitz, R. (2016). Substance abusing mothers: Toward an understanding of parenting and risk behavior. In R. Isralowitz & P. A. Findley (Eds.), Mental health and addiction care in the Middle East (pp. 59–80). New York: Springer.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Reznik, A., Isralowitz, R. (2016). Immigration, Acculturation, and Drug Use. In: Isralowitz, R., Findley, P. (eds) Mental Health and Addiction Care in the Middle East. Advances in Mental Health and Addiction. Springer, Cham. https://doi.org/10.1007/978-3-319-41556-7_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-41556-7_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-41554-3
Online ISBN: 978-3-319-41556-7
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)