
Abstract
The standard therapy for patients with unrespectable stage III non-small-cell lung cancer (NSCLC) is the combination of chemotherapy and radiotherapy. Although the concurrent use of both treatment modalities has been shown to be superior to sequential therapy, the role for additional chemotherapy, either as induction or as consolidation, remains unclear. Targeted therapy has met limited success in the treatment of unselected patients with stage III NSCLC. New studies using induction therapy with erlotinib or crizotinib for molecularly selected patients and consolidation therapy with checkpoint inhibitors are currently ongoing, and the results are eagerly awaited.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Lung cancer is both the most commonly diagnosed malignancy and cause of cancer death in the United States for men and women combined, with 240,000 new cases and 162,000 deaths estimated for the year 2015 [1]. Among patients with lung cancer, approximately 85 % have one of the non-small-cell lung cancer (NSCLC) histologies [2]. Stage III NSCLC was present in approximately 27 % of patients according to the sixth edition of the American Joint Commission on Cancer (AJCC) [3]. However, the proportion of stage III is currently lower due to the reclassification of the approximately 15–20 % of those with malignant pleural effusion to stage M1a in the seventh edition of AJCC [4, 5]. Stage III lung cancer is a heterogeneous disease, with several broad subgroups including T3N1 and selected cases of T4N0-1 which may be treated with surgery followed by adjuvant chemotherapy, T1-3N2 which is potentially resectable but usually treated with chemoradiation, and patients with invasive T4 or N3, which are unresectable and treated with chemoradiation [6].
2 Chemoradiotherapy
2.1 Initial Studies with Chemoradiotherapy
The role of chemotherapy in the management of locally advanced NSCLC was established with the results of the Cancer and Leukemia Group B (CALGB) 8433 trial, which randomly assigned 155 patients with stage III NSCLC to sequential chemotherapy with cisplatin (100 mg/m2 on days 1 and 29) and vinblastine (5 mg/m2 weekly for 5 weeks) followed by radiotherapy with 60 Gy over six weeks, starting on day 50, or radiotherapy alone [7]. The response rate was 46 % for sequential chemoradiation and 35 % for radiation alone (p = 0.092). The addition of chemotherapy significantly prolonged the median failure-free survival (PFS; 8.2 vs. 6.0 months; p = 0.041), overall survival (OS; 13.8 vs. 9.7 months; p = 0.006), and 3-year OS (23 % vs. 11 %) compared to radiation therapy alone. Chemo radiotherapy was more commonly associated with serious infection (7 % vs. 3 %) and significant weight loss (14 % vs. 6 %), but there were no treatment-related deaths in either arm.
Several trials have been conducted in an attempt to establish the optimal way to deliver chemotherapy and radiation. The Radiation Therapy Oncology Group (RTOG) 9410 trial randomly assigned 610 patients to sequential cisplatin (100 mg/m2 on days 1 and 29) and vinblastine (5 mg/m2 weekly for 5 weeks) followed by radiotherapy 60 Gy starting on day 50, the same regimen with concurrent radiation starting on day 1, or concurrent radiation with 69.6 at 1.2 Gy twice daily beginning on day 1 with cisplatin (50 mg/m2 on days 1, 8, 29, and 36) and oral etoposide (50 mg twice daily on days 1, 2, 5, and 6 for 10 weeks) [8]. The median OS for arms 1 to 3 was 14.6, 17.0, and 15.6 months. Concurrent chemoradiation conferred a slightly better 5-year survival rate compared to sequential chemoradiation (16 % vs. 10 %; hazard ratio [HR] 0.812; 95 % confidence interval [CI] 0.663–0.996; p = 0.046). Acute grade 3–5 adverse events, mostly esophagitis, mucositis, nausea, and vomiting, were more commonly seen in the concurrent therapy arms. Late toxicities were similar among the three groups.
A meta-analysis of six randomized trial comparing concurrent to sequential chemoradiation in locally advanced NSCLC showed a significant improvement in median OS with the concurrent strategy (HR 0.84; 95 % CI 0.74–.95; p = 0.004) [9]. The absolute survival benefit was 5.7 % at 3 years, and 4.5 % at 5 years. Compared to the sequential strategy, concurrent chemoradiation was associated with increased grade 3–4 acute esophageal toxicity (18 % vs. 4 %; p <0.001).
2.2 Paclitaxel-Based Studies
The phase II Locally Advanced Multimodality Protocol (LAMP) study tested the regimen of paclitaxel and carboplatin combined with radiotherapy in stage III NSCLC [10]. A total of 276 patients were randomly assigned to sequential arm with two cycles of paclitaxel (200 mg/m2) and carboplatin (AUC = 6) followed by radiotherapy with 63 Gy, induction arm with two cycles of induction paclitaxel (200 mg/m2) and carboplatin (AUC = 6) followed by weekly paclitaxel (45 mg/m2) and carboplatin (AUC = 2) with concomitant radiotherapy 63 Gy, or consolidation arm with weekly paclitaxel (45 mg/m2) and carboplatin (AUC = 2) with concurrent RT 63 Gy followed by two cycles of consolidation paclitaxel (200 mg/m2) and carboplatin (AUC = 6). At a median follow-up of 39.6 months, the median OS of the sequential, induction, and consolidation arms was 13.0, 12.7, and 16.3 months, respectively. The 3-year survival rates were almost identical among the three arms (17 % for sequential, 15 % for induction, 17 % for consolidation). Median PFS and 1-year progression-free rates were, respectively, 9.0 months and 54 % for the sequential arm, 6.7 months and 46 % for the induction arm, and 8.7 months and 46 % for the consolidation arm. The consolidation arm was associated with increased rates of grade 3–4 esophagitis, lung toxicities, and myelosuppression.
The RTOG 0617 was a phase III study evaluating the role of high-dose versus standard-dose radiotherapy and the effect of additional cetuximab [11]. Patients with unresectable stage III NSCLC were randomly assigned to either standard-dose radiotherapy (60 Gy) with or without cetuximab, or high-dose radiotherapy (74 Gy) with or without cetuximab. All patients received concurrent paclitaxel (45 mg/m2) and carboplatin (AUC = 2) with radiation followed by consolidation paclitaxel (200 mg/m2) and carboplatin (AUC = 6) for two cycles. For patients randomized to receive cetuximab, cetuximab was administered at 400 mg/m2 on day 1 followed by 250 mg/m2 weekly that continued through consolidation treatment. A total of 544 patients were enrolled. Standard-dose radiation was associated with improved median OS (28.7 vs. 20.3 months; HR 1.38; 95 % CI 1.09–1.76; p = 0.004) compared to high-dose radiotherapy, with the latter causing increased rates of severe esophagitis (21 vs. 7, %; p <0.0001). The addition of cetuximab did not improve the median OS (25 vs. 24 months; HR 1.07; 95 % CI 0.84–1.35; p = 0.29) or median PFS (median 10.8 vs. 10.7 months and 27.5 %; HR 0.99; 95 % CI 0.80–1.22; p = 0.89) compared to chemotherapy alone. However, in a planned subset analysis, patients with over-expression of EGFR (H-score ≥200) had improved median OS with the use of cetuximab (42.0 vs. 21.2 months; HR 1.72; 95 % CI 1.04–2.84; p = 0.032). Since the study did not suggest a survival benefit with high-dose radiotherapy or cetuximab in the overall population with stage III NSCLC, concurrent paclitaxel and carboplatin with standard-dose radiotherapy followed by two cycles of consolidation paclitaxel and carboplatin remains one of the standard treatments for unresectable stage III NSCLC.
2.3 Etoposide-Based Studies
The phase II Southwest Oncology Group (SWOG) 9019 trial evaluated the regimen of cisplatin and etoposide with radiotherapy [12]. Patients with stage III NSCLC were treated with cisplatin (50 mg/m2 on days 1, 8, 29, and 36) and etoposide (50 mg/m2/day on days 1–5, and 29–33) along with concurrent radiation 45 Gy. In the absence of disease progression, patients then received further radiotherapy to a total dose of 61 Gy with 2 additional cycles of cisplatin and etoposide. The median OS for the 50 enrolled patients was 15 months, with 3-year OS and 5-year OS of 17 and 15 %, respectively. Major adverse events include neutropenia (grade 4 in 32 %), anemia (grade 3–4 in 28 %), esophagitis (grade 3–4 in 20 %), and respiratory infection (grade 3–4 in 8 %). This study established the role of cisplatin and etoposide with concurrent radiotherapy as one of the standard treatments for locally advanced NSCLC.
In the phase II SWOG 9504 study, patients with stage IIIB NSCLC received the same chemoradiation regimen used in SWOG 1909, with two cycles of consolidation docetaxel (75 mg/m2) 4–6 weeks after completion of chemoradiation in the absence of tumor progression [13]. The response rates, median PFS, and median OS for the 83 patients accrued were 67 %, 16 months, and 26 months, respectively. The 3-year survival was 37 %. Neutropenia (74 %), infection (21 %), and esophagitis (17 %) were the most common severe adverse events. Four patients died of treatment-related toxicities, two from pneumonitis and two from infection.
2.4 Pemetrexed-Based Studies
The phase II CALGB 30407 study examined the role of concurrent chemoradiation with pemetrexed and carboplatin with or without cetuximab in patients with stage III NSCLC [14]. Patients were randomly assigned to four cycles of pemetrexed (500 mg/m2) and carboplatin (AUC = 5) with concomitant radiation 70 Gy or the same chemoradiation regimen with the addition of cetuximab (400 mg/m2 loading dose followed by 250 mg/m2 weekly for 12 weeks). All patients received four cycles of consolidation pemetrexed (500 mg/m2). Among the 101 enrolled, 65 % had non-squamous histologies. The median OS for patients treated with and without cetuximab was 25.2 and 21.2 months, respectively. Toxicities were similar between the two treatment arms. Common grade 3 and greater adverse events include myelosuppression, esophagitis, dysphagia, pneumonitis, dehydration, nausea, and vomiting. This study demonstrated the feasibility of concurrent chemoradiation with carboplatin and pemetrexed, with no benefits from the addition of cetuximab.
Choy and colleagues compared cisplatin to carboplatin during pemetrexed-based chemoradiation regimen in a phase II trial [15]. When the study first opened, patients with squamous cell histology were eligible. After the preferential efficacy of pemetrexed in non-squamous histology was revealed in a phase III study [16], the protocol was amended in 2008 to exclude squamous cell histology. A total of 98 patients with unresectable stage III NSCLC were randomly assigned to receive pemetrexed (500 mg/m2) in combination with carboplatin (AUC = 5) or cisplatin (75 mg/m2). Concurrent radiotherapy was delivered to a total dose of 64 to 68 Gy. Patients also received three cycles of consolidation pemetrexed. The cisplatin arm was associated with increased median OS (27 vs. 18.7 months), 2-year OS (58.4 % vs. 45.4 %), and median PFS (13.1 vs. 8.8 months). Due the small sample size and study design, the comparison between the two regimens was not performed. Nevertheless, both regimens were considered active and well tolerated. Dehydration was the most common grade 3–4 non-hematologic toxicity in both arms (6.5 % in the carboplatin arm and 9.6 % in the cisplatin arm). Esophagitis was experienced in 4.3 % in the carboplatin group and 5.7 % in the cisplatin group. The carboplatin arm had more severe hematologic adverse events compared to the cisplatin arm (anemia 10.9 % vs. 7.7 %; febrile neutropenia 4.3 % versus 0 %; thrombocytopenia 8.6 % vs. 5.7 %, respectively).
2.5 Comparison of Chemotherapy Regimens
The two most commonly used chemotherapy regimens in combination with radiotherapy in stage III NSCLC are cisplatin plus etoposide and carboplatin plus paclitaxel. In a small study conducted by Dr. Wang and colleagues, 65 patients with stage III NSCLC were randomized to cisplatin plus etoposide or carboplatin plus paclitaxel during concurrent radiotherapy with 60 Gy [17]. Cisplatin and etoposide was associated with increased median OS (20.2 vs. 13.5 months) and 3-year OS (33.1 vs. 13 %, p = 0.04).
In a retrospective analysis using the Department of Veterans Affairs Central Cancer Registry, 1,842 patients treated with either cisplatin plus etoposide or carboplatin plus paclitaxel with concomitant radiation from 2001 to 2010 were identified [18]. Cisplatin plus etoposide was used in 27 % of patients and was associated with increased median OS in univariable analysis (17.3 vs. 14.6 months, HR 0.88; 95 % CI 0.79–.98, p = 0.02). Nevertheless, since the population of patients receiving cisplatin plus etoposide had a higher proportion of overall favorable features such as younger age, less weight loss, and better comorbidity scores, a propensity score-match data set was performed. With this analysis, the improvement in OS from cisplatin plus etoposide did not reach statistical significance (HR 0.97; 95 % CI 0.85–1.10). The rates of hospitalization (2.4 vs. 1.7; p <0.001), outpatient visits (17.6 vs. 12.6; p <0.001), infections (47.3 vs. 39.4 %; p = 0.002), acute kidney disease/dehydration (30.5 % vs. 21.2 %; p <0.001), and mucositis plus esophagitis (18.6 % vs. 14.4 %; p = 0.0246) were increased in the cisplatin plus etoposide regimen compared to carboplatin plus paclitaxel.
The PROCLAIM study is a phase III trial comparing cisplatin plus pemetrexed to cisplatin plus etoposide during concurrent chemoradiotherapy [19]. Patients with stage III NSCLC were randomly assigned to receive three cycles of cisplatin (75 mg/m2) and pemetrexed (500 mg/m2) every 3 weeks or cisplatin (50 mg/m2 on days 1, 8, 29, and 36) plus etoposide (50 mg/m2 on days 1–5 and 29–33) during concurrent radiotherapy with 66 Gy. After concomitant chemoradiation, patients received further consolidation chemotherapy with four cycles of pemetrexed in the cisplatin plus pemetrexed arm or a choice of 3 regimens in the cisplatin plus etoposide arm. The cisplatin plus pemetrexed was associated with a numerically superior response rate (36 % vs. 33 %, p = 0.458), median PFS (11.4 vs. 9.8 months; HR 0.86; 95 % CI 0.71–1.04), and median OS (26.8 vs. 25.0 months; HR 0.98; 95 % CI 0.79–1.20; p = 0.831), although none reached statistical significance. The pemetrexed arm was associated with decreased rates of severe neutropenia (24.4 % vs. 44.5 %) and esophagitis (15.5 % vs. 20.6 %). This study demonstrated that cisplatin plus pemetrexed with concurrent radiotherapy was as effective as cisplatin plus etoposide, but with a better safety profile.
2.6 Consolidation Chemotherapy
Although several studies include the use of consolidation chemotherapy, its role in the management of patients with unresectable stage III NSCLC remains undefined (Table 1).
In the HOG/USO study, the chemoradiation followed by consolidation docetaxel, as used in the SWOG 9504 regimen, was compared to chemoradiation alone [20]. Although the planned accrual was for 259 patients, the trial was closed early, after enrollment of 203 patients, when an interim analysis suggested evidence of futility. Compared to observation, the docetaxel arm was associated with similar median OS (21.2 vs. 23.2 months, p = 0.883) and 3-year OS (27.1 % vs. 26.1 %). Consolidation docetaxel was associated with increased rates of febrile neutropenia and grade 3–5 pneumonitis (9.6 % vs. 1.4 %). Five percent of patients in the docetaxel arm died of grade 5 toxicities.
The phase III GILT study examined the role of consolidation cisplatin and oral vinorelbine after concurrent chemoradiotherapy [21]. Patients received two cycles of oral vinorelbine (50 mg/m2 on days 1, 8, and 15) and cisplatin (20 mg/m2 on days 1–4) every 4 weeks with concomitant radiotherapy at 66 Gy. Patients without disease progression were further randomized to two cycles of consolidation therapy with oral vinorelbine (60–80 mg/m2 on days 1 and 8) and cisplatin (80 mg/m2 on day 1) every 3 weeks versus observation. A total of 279 patients were enrolled. The overall response rate of chemoradiation was 60.7 %. Consolidation chemotherapy did not improve median PFS (6.4 vs. 5.5 months, p = 0.63) or median OS (20.8 vs. 18.5 months, p = 0.87). The 4-year survival rates were 25.3 and 21.4 % for the consolidation and the observation arm, respectively. Concurrent chemoradiation caused esophagitis in 8.6 %, nausea in 5.0 %, fatigue in 3.3 %, and pneumonia/pneumonitis in 2.6 %. Neutropenia and anemia were the most common severe hematologic toxicities (neutropenia in 11.2 % and anemia in 3.2 %). Consolidation chemotherapy caused more neutropenia (11.7 % vs. 5.7 %), anemia (3.5 % vs. 1.1 %), nausea (4.7 % vs. 2.9 %), and fatigue (2.3 % vs. 1.0 %) compared to observation.
The KCSG-LU05-04 trial was a phase III study examining the efficacy of consolidation cisplatin plus docetaxel following concurrent chemoradiation with the same regimen [22]. Concurrent chemoradiation entailed weekly cisplatin (20 mg/m2) and docetaxel (20 mg/m2) for 6 weeks with 66 Gy of radiotherapy. Consolidation docetaxel was given at 35 mg/m2 on days 1 and 8 every 3 weeks for three cycles. A total of 437 patients in Korea, China, and Taiwan were randomly assigned to concurrent chemoradiation alone versus chemoradiation followed by consolidation docetaxel. Although numerically superior, the improvement in median PFS (9.1 vs. 8.1 months, HR 0.91; 95 % CI 0.73–1.12; p = 0.36) and median OS (20.6 vs. 21.8 months; HR 0.91; 95 % CI 0.72–1.25; p = 0.44) did not reach statistical significance. The most common grade 3–4 toxicities in the chemoradiotherapy phase were esophagitis (9.5 %), infection (6.4 %), anorexia (4.0 %), and anemia (5.4 %). Consolidation chemotherapy induced more neutropenia (6.9% vs. 2.9 %), febrile neutropenia (1.8% vs. 0 %), fatigue (4.6 versus 0 %), and anorexia (3.5 versus 1.2 %) compared to observation.
In a pooled analysis including 3,479 patients from 41 studies, consolidation chemotherapy did not prolong median OS compared to observation alone (19.0 vs. 17.9 months; HR 0.94; 95 % CI 0.81–1.09; p = 0.40) [23]. The 3-year survival rates were also similar between the consolidation and the observation group (27.0 % vs. 24.8 %). Grade 3-5 neutropenia, esophagitis, pneumonitis, and treatment-related deaths were similar in the two study groups.
With the lack of established benefit from consolidation chemotherapy in 3 randomized Clincal trials and a pooled analysis, the American Society for Radiation Oncology (ASTRO) guideline recommended against routine use of consolidation chemotherapy after concurrent chemoradiation [24]. However, patients who did not receive full doses of systemic chemotherapy during radiotherapy can be considered for consolidation chemotherapy.
3 Molecularly Targeted Therapy
Several targeted drugs used in advanced stage NSCLC have been tried in patients with locally advanced disease. Bevacizumab, a monoclonal antibody against vascular endothelial growth factor receptor (VEGFR), is an approved therapy for patients with advanced non-squamous NSCLC [25]. The use of bevacizumab during chemoradiation, however, was associated with increased risk of bleeding and development of trachea–esophageal fistula [26]. Due to the severe toxicities, bevacizumab is no longer being investigated during chemoradiotherapy.
The epidermal growth factor receptor has been studied in patients with stage III NSCLC with trial including both the monoclonal antibody cetuximab and the tyrosine kinase inhibitors gefitinib and erlotinib. In the NEAR trial, 30 patients who were unfit or unwilling to receive chemoradiation received weekly cetuximab during radiotherapy followed by 13 weeks of consolidation [27]. The treatment was well tolerated, and the outcomes including median OS of 19.5 months and 2-year OS of 34.9 % are comparable to those obtained from standard chemoradiation. Using a similar design except for the consolidation cetuximab, the N0422 study showed a median OS of 15.1 months in 57 patients with stage III NSCLC who were elderly or had poor performance status [28]. The Swedish Lung Cancer Group trial examined the role of concurrent weekly cetuximab in combination with thoracic radiation therapy (68 Gy over 7 weeks), following 2 cycles of induction chemotherapy with cisplatin and docetaxel [29]. The clinical benefit rate at 12 months was 30 % and median OS was 17 months. Grade 3 esophagitis was seen in 1.4 % and grade 3 skin toxicity in 4.2 %. Ramalingam and colleagues conducted a multicenter single-arm phase II trial in which 40 patients with unresectable IIIA or IIIB NSCLC were treated with thoracic radiotherapy to a dose of 73.5 Gy in 35 fractions over 7 weeks in combination with weekly cetuximab, which was continued during consolidation therapy with carboplatin and paclitaxel for a maximum of 26 doses [30]. The median OS, primary endpoint of the study, was 19.4 months. Cetuximab addition to chest radiation and consolidation chemotherapy was well tolerated with 3 patients experiencing a grade 3 rash. No grade 3 or 4 esophagitis was observed. EGFR gene copy number by fluorescence in situ hybridization (FISH) was not predictive of outcomes in this study. The safety of cetuximab in combination with definitive chemoradiation in NSCLC has also been demonstrated by the Radiation Therapy Oncology Group (RTOG) 0324 and Cancer and Leukemia Group B (CALGB) 30407 trials, where toxicities observed in the arms with combined chemotherapy and cetuximab were comparable to those with chemotherapy alone [14, 31].
The Southwest Oncology Group (SWOG) S0023 trial was designed to evaluate whether the addition of gefitinib maintenance therapy improved overall survival following concurrent chemoradiation with cisplatin and etoposide followed by three cycles of consolidation docetaxel [32]. A total of 243 molecularly unselected patients with stage III NSCLC were randomized to receive gefitinib or placebo following concurrent chemoradiation with cisplatin and etoposide and consolidation docetaxel. Although gefitinib was well tolerated, survival was worse in the gefitinib arm, predominantly due to tumor progression. The Japanese Cooperative Oncology Group (JCOG) 0402 study examined the role of induction chemotherapy followed by gefitinib and concurrent thoracic radiation in patients with unresectable adenocarcinoma, selected by light or never smoking status only, and did not meet predefined criteria for feasibility due to increased toxicity mostly with grade 3 and 4 liver enzyme elevations [33]. In a phase II study including 46 unselected patients with stage III NSCLC treated with erlotinib 150 mg daily during standard chemoradiation with weekly carboplatin plus paclitaxel followed by two cycles of consolidation with chemotherapy alone, the median and 5-year OS were encouraging at 36.5 months and 39.5 %, respectively [34]. Of note, there were 4 patients with EGFR mutation and 5 patients with unknown EGFR status in the study, precluding the evaluation of the effects of this mutation in the outcome.
The RTOG 1306 is a phase II study evaluating the role of targeted agents in molecularly selected patients with locally advanced NSCLC. In this study, patients with stage III EGFR-mutant lung cancer and ALK-positive NSCLC will be randomized to 12 weeks of induction erlotinib (EGFR-mutant) or crizotinib (ALK-positive) followed by chemoradiation, or chemoradiation alone (Fig. 1) [35].

RTOG 1306 schema Targeted therapy Erlotinib for EGFR mutation or crizotinib for ALK fusion for 12 weeks. If CT scan after 6 weeks of targeted therapy does not show PR, patients should proceed directly to chemoradiation Chemotherapy cisplatin plus etoposide or carboplatin plus paclitaxel Radiation 60 Gy in 30 fractions with intensity-modulated radiation therapy (IMRT) or 3D conformal radiation therapy (3D-CRT)
4 Immunotherapy
In patients with stage III disease, the largest experience with immunotherapy is with tecemotide (liposomal BLP25), a peptide-based vaccine consisting of synthetic mucin 1 (MUC-1) lipopeptide combined with the adjuvant monophosphoryl lipid A and three lipids forming a liposomal product. In a phase II study, 171 patients with stage IIIB or IV NSCLC who had no tumor progression after the initial therapy were randomized to tecemotide 100 µg weekly for 8 weeks followed by maintenance every 6 weeks until tumor progression or observation [36]. Although there was no benefit from the vaccine in the study population, a post hoc analysis showed increased median (not reached vs. 13.3 months) and 2-year OS (60 % vs. 36.7 %) in the tecemotide group. The encouraging results in patients with stage III NSCLC led to the START trial, a phase III study where 1,513 patients were randomized to receive tecemotide versus placebo following definitive chemoradiation [37]. Although tecemotide was not associated with improved median OS in the entire patient population (25.6 vs. 22.3 months, HR 0.88, 95 % CI 0.75–1.03, p = 0.12), it improved median OS in a subset analysis of patients treated with concurrent chemoradiation (30.8 vs. 20.6 months; HR 0.78; 95 % CI 0.64–0.95, p = 0.01). In the updated analysis with a median follow-up of 58 months, the addition of tecemotide was associated with increased median OS in patients treated with concurrent chemoradiation (29.8 vs. 20.8 months, HR 0.81; 95 % CI 0.68–0.98, p = 0.026) but not in those treated with sequential therapy (20.7 vs. 25.5 months, HR 1.04; 95 % CI 0.82–1.31, p = 0.76) [38]. Soluble MUC and antinuclear antibodies were associated with improved survival in patients treated with tecemotide. Two large randomized studies testing tecemotide in patients treated with concurrent chemoradiation, START2 and INSPIRE, were discontinued after the results from the EMR 63325-009 study, which showed no benefit from the addition of tecemotide to chemoradiation.
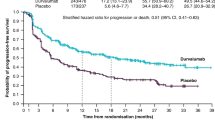
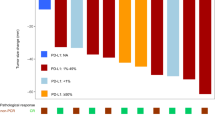
Checkpoint inhibitors represent a promising new approach to the treatment of NSCLC, with nivolumab and pembrolizumab approved for patients with previously treated advanced stage NSCLC [39–41]. The role of immune checkpoint inhibitors in patients with locally advanced NSCLC is currently being investigated. Both anti-programmed death 1 (PD-1) and anti-programmed death cell ligand 1 (PDL-1) antibodies are being investigated as consolidation therapy after standard chemoradiation for patients with stage III NSCLC [42].
5 Conclusions
The cure rates for patients with locally advanced NSCLC remain suboptimal with standard chemoradiation. There are several acceptable chemotherapy regimens to be used during concurrent radiotherapy, and the escalation of the radiation dose is not associated with improved outcomes. Consolidation chemotherapy, although commonly used, has not shown improvement in survival compared to chemoradiation alone and should be considered only in selected cases. The role for targeted therapy in molecularly selected patients is currently being evaluated in this potentially curative patient population, although its applicability is limited by the low probability of patients harboring targetable driver gene abnormalities. There are ongoing studies testing consolidation therapy with checkpoint inhibitors, and the results are eagerly awaited.
References
Siegel RL, Miller KD, Jemal A (2015) Cancer statistics, 2015. CA Cancer J Clin 65(1):5–29
Govindan R, Page N, Morgensztern D et al (2006) Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol: Official J Am Soc Clin Oncol 24(28):4539–4544
Morgensztern D, Ng SH, Gao F, Govindan R (2010) Trends in stage distribution for patients with non-small cell lung cancer: a national cancer database survey. J Thorac Oncol: Official Publ Int Assoc Study of Lung Cancer 5(1):29–33
Morgensztern D, Waqar S, Subramanian J, Trinkaus K, Govindan R (2012) Prognostic impact of malignant pleural effusion at presentation in patients with metastatic non-small-cell lung cancer. J Thorac Oncol: Official Publ Int Assoc Study of Lung Cancer 7(10):1485–1489
Goldstraw P, Crowley J, Chansky K et al (2007) The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol: Official Publ Int Assoc for the Study of Lung Cancer 2(8):706–714
Ettinger DS, Akerley W, Borghaei H et al (2012) Non-small cell lung cancer. J Nat Compr Cancer Network: JNCCN 10(10):1236–1271
Dillman RO, Seagren SL, Propert KJ et al (1990) A randomized trial of induction chemotherapy plus high-dose radiation versus radiation alone in stage III non-small-cell lung cancer. The New England J Med 323(14):940–945
Curran WJ Jr, Paulus R, Langer CJ et al (2011) Sequential versus concurrent chemoradiation for stage III non-small cell lung cancer: randomized phase III trial RTOG 9410. J Natl Cancer Inst 103(19):1452–1460
Auperin A, Le Pechoux C, Rolland E et al (2010) Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol: Official J Am Soc Clin Oncol 28(13):2181–2190
Belani CP, Choy H, Bonomi P et al (2005) Combined chemoradiotherapy regimens of paclitaxel and carboplatin for locally advanced non-small-cell lung cancer: a randomized phase II locally advanced multi-modality protocol. J Clin Oncol: Official J Am Soc Clin Oncol 23(25):5883–5891
Bradley JD, Paulus R, Komaki R et al (2015) Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. Lancet Oncol 16(2):187–199
Albain KS, Crowley JJ, Turrisi AT 3rd et al (2002) Concurrent cisplatin, etoposide, and chest radiotherapy in pathologic stage IIIB non-small-cell lung cancer: a Southwest Oncology Group phase II study, SWOG 9019. J Clin Oncol: Official J Am Soc Clin Oncol 20(16):3454–3460
Gandara DR, Chansky K, Albain KS et al (2003) Consolidation docetaxel after concurrent chemoradiotherapy in stage IIIB non-small-cell lung cancer: phase II Southwest Oncology Group Study S9504. J Clin Oncol: Official J Am Soc of Clin Oncol 21(10):2004–2010
Govindan R, Bogart J, Stinchcombe T et al (2011) Randomized phase II study of pemetrexed, carboplatin, and thoracic radiation with or without cetuximab in patients with locally advanced unresectable non-small-cell lung cancer: Cancer and Leukemia Group B trial 30407. J Clin Oncol: Official J Am Soc of Clin Oncol 29(23):3120–3125
Choy H, Schwartzberg LS, Dakhil SR et al (2013) Phase 2 study of pemetrexed plus carboplatin, or pemetrexed plus cisplatin with concurrent radiation therapy followed by pemetrexed consolidation in patients with favorable-prognosis inoperable stage IIIA/B non-small-cell lung cancer. J Thorac Oncol: Official Publication Int Assoc Study of Lung Cancer 8(10):1308–1316
Scagliotti GV, Parikh P, von Pawel J et al (2008) Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J Clin Oncol: Official J Am Soc Clin Oncol 26(21):3543–3551
Wang L, Wu S, Ou G et al (2012) Randomized phase II study of concurrent cisplatin/etoposide or paclitaxel/carboplatin and thoracic radiotherapy in patients with stage III non-small cell lung cancer. Lung Cancer 77(1):89–96
Santana-Davila R, Devisetty K, Szabo A et al (2015) Cisplatin and etoposide versus carboplatin and paclitaxel with concurrent radiotherapy for stage III non-small-cell lung cancer: an analysis of Veterans Health Administration data. J Clin Oncol: Official J Am Soc Clin Oncol 33(6):567–574
Senan S, Brade AM, Wang L et al (2015) Final overall survival (OS) results of the phase III PROCLAIM trial: Pemetrexed (Pem), cisplatin (Cis) or etoposide (Eto), Cis plus thoracic radiation therapy (TRT) followed by consolidation cytotoxic chemotherapy (CTX) in locally advanced nonsquamous non-small cell lung cancer (nsNSCLC). ASCO Meet Abs. 2015;33(15_suppl):7506
Hanna N, Neubauer M, Yiannoutsos C et al (2008) Phase III study of cisplatin, etoposide, and concurrent chest radiation with or without consolidation docetaxel in patients with inoperable stage III non-small-cell lung cancer: the Hoosier Oncology Group and U.S. Oncology. Journal of Clincal Oncology: Official Journal of the American Society of. Clin Oncol 26(35):5755–5760
Huber RM, Engel-Riedel W, Kollmeier J et al (2012) GILT study: oral vinorelbine (NVBo) and cisplatin (P) with concomitant radiotherapy (RT) followed by either consolidation (C) with NVBo plus P plus best supportive care (BSC) or BSC alone in stage (st) III non-small cell lung cancer (NSCLC): final results of a phase (ph) III study. ASCO Meet Abs. 2012;30(15_suppl):7001
Ahn JS, Ahn YC, Kim JH et al (2015) multinational randomized phase iii trial with or without consolidation chemotherapy using docetaxel and cisplatin after concurrent chemoradiation in inoperable stage iii non-small-cell lung cancer: KCSG-LU05-04. J Clin Oncol
Tsujino K, Kurata T, Yamamoto S et al (2013) Is consolidation chemotherapy after concurrent chemo-radiotherapy beneficial for patients with locally advanced non-small-cell lung cancer?: A pooled analysis of the literature. J Thorac Oncol 8(9):1181–1189
Bezjak A, Temin S, Franklin G et al (2015) Definitive and adjuvant radiotherapy in locally advanced non–small-cell lung cancer: american society of Clincal oncology Clincal practice guideline endorsement of the american society for radiation oncology evidence-based Clincal practice guideline. J Clin Oncol. 2015;33(18):2100–2105
Sandler A, Gray R, Perry MC et al (2006) Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. The New England J Med 355(24):2542–2550
Spigel DR, Hainsworth JD, Yardley DA et al (2010) Tracheoesophageal fistula formation in patients with lung cancer treated with chemoradiation and bevacizumab. J Clin Oncol 28(1):43–48
Jensen AD, Munter MW, Bischoff HG et al (2011) Combined treatment of nonsmall cell lung cancer NSCLC stage III with intensity-modulated RT radiotherapy and cetuximab: the NEAR trial. Cancer 117(13):2986–2994
Jatoi A, Schild SE, Foster N et al (2010) A phase II study of cetuximab and radiation in elderly and/or poor performance status patients with locally advanced non-small-cell lung cancer (N0422). Annals of Oncol: Official J Euro Soc Med Oncol/ESMO 21(10):2040–2044
Hallqvist A, Wagenius G, Rylander H et al (2011) Concurrent cetuximab and radiotherapy after docetaxel-cisplatin induction chemotherapy in stage III NSCLC: satellite–a phase II study from the Swedish Lung Cancer Study Group. Lung Cancer 71(2):166–172
Ramalingam SS, Kotsakis A, Tarhini AA et al (2013) A multicenter phase II study of cetuximab in combination with chest radiotherapy and consolidation chemotherapy in patients with stage III non-small cell lung cancer. Lung Cancer 81(3):416–421
Blumenschein GR Jr, Paulus R, Curran WJ et al (2011) Phase II study of cetuximab in combination with chemoradiation in patients with stage IIIA/B non-small-cell lung cancer: RTOG 0324. J Clin Oncol: Official J Am Soc Clin Oncol 29(17):2312–2318
Kelly K, Chansky K, Gaspar LE et al (2008) Phase III trial of maintenance gefitinib or placebo after concurrent chemoradiotherapy and docetaxel consolidation in inoperable stage III non-small-cell lung cancer: SWOG S0023. J Clin Oncol 26(15):2450–2456
Niho S, Ohe Y, Ishikura S et al (2012) Induction chemotherapy followed by gefitinib and concurrent thoracic radiotherapy for unresectable locally advanced adenocarcinoma of the lung: a multicenter feasibility study (JCOG 0402). Annals of Oncol: Official J Euro Soc Med Oncol/ESMO 23(9):2253–2258
Komaki R, Allen PK, Wei X et al (2015) Adding Erlotinib to Chemoradiation Improves Overall Survival but Not Progression-Free Survival in Stage III Non-Small Cell Lung Cancer. Int J Radiat Oncol Biol Phys 92(2):317–324
Devarakonda S, Morgensztern D, Govindan R (2013) Molecularly targeted therapies in locally advanced non-small-cell lung cancer. Clin lung Cancer 14(5):467–472
Butts C, Murray N, Maksymiuk A et al (2005) Randomized phase IIB trial of BLP25 liposome vaccine in stage IIIB and IV non-small-cell lung cancer. J Clin Oncol: Official J Am Soc Clin Oncol 23(27):6674–6681
Butts C, Socinski MA, Mitchell PL et al (2014) Tecemotide (L-BLP25) versus placebo after chemoradiotherapy for stage III non-small-cell lung cancer (START): a randomised, double-blind, phase 3 trial. Lancet Oncol 15(1):59–68
Mitchell P, Thatcher N, Socinski MA, et al (2015) Tecemotide in unresectable stage III non-small-cell lung cancer in the phase III START study: updated overall survival and biomarker analyses. Ann Oncol
Brahmer J, Reckamp KL, Baas P et al (2015) Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. The New England J Med 373(2):123–135
Sul J, Blumenthal GM, Jiang X, He K, Keegan P, Pazdur R (2016) FDA approval summary: Pembrolizumab for the treatment of patients with metastatic non-small cell lung cancer whose tumors express programmed death-ligand 1. Oncologist 21(5):643–650
Kazandjian D, Suzman DL, Blumenthal G, Mushti S, He K, Libeg M, Keegan P, Pazdur R. FDA approval summary: Nivolumab for the treatment of metastatic non-small cell lung cancer with progression on or after platinum-based chemotherapy. Oncologist 2016 May; 21(5):634-642
Mamdani H, Jalal SI, Hanna N (2015) Locally advanced non-small cell lung cancer: Optimal chemotherapeutic agents and duration. Curr Treat Options Oncol 16(10):364
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Du, L., Waqar, S.N., Morgensztern, D. (2016). Multimodality Therapy for NSCLC. In: Reckamp, K. (eds) Lung Cancer. Cancer Treatment and Research, vol 170. Springer, Cham. https://doi.org/10.1007/978-3-319-40389-2_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-40389-2_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-40387-8
Online ISBN: 978-3-319-40389-2
eBook Packages: MedicineMedicine (R0)