
Abstract
Ventilators, or more precisely, the modes they deliver, can be classified by the variables that are controlled (e.g., pressure or volume), as well as those that start (or trigger), sustain (or limit), and end (cycle) inspiration and those that maintain the expiratory support (or baseline pressure). Microprocessor and sensor technology has increased the quality and quantity of ventilator output feedback available (Fig. 10.1). These advances in technology have led to several different targeting schemes that warrant further classification (Chap. 44).
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
-
I.
Ventilators, or more precisely, the modes they deliver, can be classified by the variables that are controlled (e.g., pressure or volume), as well as those that start (or trigger), sustain (or limit), and end (cycle) inspiration and those that maintain the expiratory support (or baseline pressure). Microprocessor and sensor technology has increased the quality and quantity of ventilator output feedback available (Fig. 10.1). These advances in technology have led to several different targeting schemes that warrant further classification (Chap. 44).
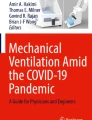
Fig 10.1 
Application of the equation of motion to the respiratory system. A common waveform for each control variable is shown. Pressure, volume, flow, and time are also used as phase variables that determine the characteristics of each ventilator cycle (e.g., trigger sensitivity, inspiratory time, baseline pressure). This emphasizes that each control variable may have a different set of control and phase variables, depending on the mode of ventilation desired (Adapted from Chatburn RL. Classification of mechanical ventilator. In: Branson RD, Huess DR, Chatburn RL, editors. Respiratory care equipment. Philadelphia: JB Lippincott; 1995. P. 280, with permission)
-
II.
Breath Control Variables . A mode of ventilation can be classified as either a form of pressure control or volume control, meaning that either pressure or volume are used as feedback control variables by the mechanism that controls breath delivery. The theoretical foundation for identifying a control variable is the equation of motion for the respiratory system. A simple version for this purpose (representing a passive patient) is as follows:
$$ {P}_{\mathrm{vent}}=E\times V(t)+R\times \dot{V}(t) $$Where P vent is the pressure generated by the ventilator to drive inspiration, E = elastance (ΔP/ΔV), V(t) = volume as a function of time (t), and \( \dot{V}(t) \) is flow as a function of time. If the ventilator controls the left hand side of the equation, i.e., the pressure waveform parameters are preset, then the mode is pressure control. This includes modes for which the peak inspiratory pressure is preset or it is automatically adjusted by the ventilator to be proportional to the patient’s inspiratory effort. If the ventilator controls the right hand side of the equation, i.e., both tidal volume and inspiratory flow are preset, the control variable is volume.
-
A.
Pressure control
To deliver pressure control modes, the ventilator controls the airway pressure waveform such that: (1) airway pressure, making it rise above the body surface pressure (i.e., positive pressure ventilator); or (2) body surface pressure, making it fall below the airway pressure (i.e., negative pressure ventilation); or (3) inspiratory pressure is made to be proportional to inspiratory effort, as sensed by the ventilator, as a signal generated by the diaphragm (e.g., flow or electrical voltage). As the equation of motion indicates, pressure is the independent variable, while volume and flow are dependent variables, whose values are determined by elastance (or compliance) and resistance .
-
B.
Volume control
To deliver volume control, the ventilator regulates flow according to a preset value (in a variety of preset flow waveforms) for a preset time, yielding a preset tidal volume. As the equation of motion indicates, flow (and volume, as it is simply the integral of flow) are the independent variables, and thus airway pressure depends upon elastance (or compliance) and resistance. Control of tidal volume can be useful in circumstances of rapidly changing lung mechanics.
-
C.
Time control
There are modes of ventilation for which neither pressure nor flow/volume is preset. All that is preset are the inspiratory and expiratory times. Hence, we say the control variable is time and the mode is a form of time control (vs. volume or pressure control). High frequency oscillatory ventilation and intrapulmonary percussive ventilation are examples of modes classified as time control.
-
A.
-
III.
Ventilator Cycle Phase Variables
The ventilatory cycle has four phases: (1) the change from expiration to inspiration (trigger); (2) inspiratory limit; (3) the change from inspiration to expiration (cycle); and (4) expiration (baseline pressure) (Fig. 10.2). With spontaneous breaths, the start and end of inspiration are determined by the patient independent of any ventilator settings. Spontaneous breaths may be assisted (as in pressure support) or unassisted. With mandatory breaths, the patient does not control the timing of the entire breath. A mandatory breath is by definition assisted.
Fig. 10.2 
Criteria for determining the phase variables during a ventilator-supported breath (Adapted from Chatburn RL. Classification of mechanical ventilator. In: Branson RD, Huess DR, Chatburn RL, editors. Respiratory care equipment. Philadelphia: JB Lippincott; 1995. P. 280, with permission)
-
A.
Trigger
-
1.
Inspiration begins when one or more monitored variables in the equation of motion (i.e., pressure, volume, flow, and time) reaches a preset threshold.
-
2.
Trigger events may be either patient-initiated or ventilator-initiated .
-
3.
The most common trigger variables are time (i.e., after a pre-defined time, the ventilator is triggered to start inspiration, as in intermittent mandatory ventilation) and pressure (i.e., when an inspiratory effort is detected as a change in the end expiratory pressure, the ventilator is triggered to start inspiration as in patient-triggered ventilation). Flow-triggering involves less patient effort and is more commonly used in neonatal/infant ventilators. Neurally adjusted ventilatory assist (NAVA, Chap. 50) triggers a ventilator breath by monitoring electrical signals from the diaphragm.
-
1.
-
B.
Limit
-
1.
Pressure, volume, and flow increase during inspiration.
-
2.
A limit variable restricts the inspiratory increase to a pre-set value but does not limit the duration.
-
3.
Many modes delivered by neonatal ventilators are pressure-limited .
-
1.
-
C.
Cycle
-
1.
Inspiration stops (or is cycled off) when a monitored variable reaches a pre-set threshold.
-
2.
Cycling events may be either patient-initiated or ventilator-initiated.
-
3.
Many neonatal ventilators, including high-frequency ventilators, are time-cycled (ventilator-initiated).
-
4.
Changes in airway pressure, volume, flow, or electrical signals from the diaphragm may also be used to terminate the inspiratory phase (patient-initiated).
-
1.
-
D.
Baseline
The baseline variable maintains expiratory pressure and expiratory lung volume (e.g., positive end expiratory pressure).
-
A.
-
IV.
Ventilatory Modes
Because neonatal ventilators now offer dozens of modes, it is necessary to have a classification system (taxonomy, Chap. 44) to understand ventilator capabilities. Modes are classified using three basic characteristics. First is the control variable (described above). Second is the “breath sequence” or pattern of mandatory and/or spontaneous breaths. If all breaths are mandatory we say the breath sequence is continuous mandatory ventilation (CMV). If spontaneous breaths are possible between mandatory breaths, the sequence is intermittent mandatory ventilation (IMV) . Finally, if all breaths are spontaneous, the sequence is continuous spontaneous ventilation (CSV) (Table 10.1). The third component of a mode classification system adds detail that allows us to distinguish among similar modes. This is the targeting scheme (described below). Thus, to classify a mode, we specify the control variable, the breath sequence, and the targeting scheme. For example, the most common mode use with neonates has historically been called “time cycled, pressure limited .” Formally, this mode is classified as pressure control intermittent mandatory ventilation with set-point targeting, appreciated as PC-IMVs.
Table 10.1 Targeting schemes -
V.
Targeting Scheme (Fig. 10.3)
Fig. 10.3 
Venn diagram illustrating how the mode taxonomy can be viewed in terms of discriminating features and defining features (From Chatburn RL, El-Khatib M, Mireles-Cabodevila E. A taxonomy for mechanical ventilation: 10 fundamental maxims. Respiratory Care. 2014;59(11):1747–63, with permission from the American Academy of Respiratory Care). CMV conventional mandatory ventilation, IMV intermittent mandatory ventilation, CSV continuous spontaneous ventilation, VC volume control, PC pressure control, P ett CO 2 end-tidal partial pressure of carbon dioxide, a adaptive targeting, s set-point targeting
A target is a pre-determined goal of ventilator output. The targeting scheme describes the relationship between the selected ventilator settings and the ventilator output as detected by feedback control systems. Targets can be set between-breaths or within-breaths. Within each ventilatory mode there are also several targeting schemes that can be distinguished, although some ventilators use more than one targeting scheme. The currently available targeting schemes and their abbreviations (in parentheses) are as follows:
-
A.
Set-point (s)
Operator sets all the parameters of the pressure wave form or volume and flow waveforms.
-
B.
Dual (d)
Switches between volume control and pressure control during a single inspiration.
-
C.
Servo (r)
Ventilator output (pressure or volume) automatically follows a varying input (inspiratory effort).
-
D.
Adaptive (a)
Ventilator automatically sets one target (pressure) in order to achieve another monitored target (volume) .
-
E.
Bio-variable (b)
Ventilator randomly selects inspiratory pressure or volume to mimic the variability of normal breathing.
-
F.
Optimal (o)
Ventilator automatically adjusts the targets of the ventilatory pattern to either minimize or maximize a monitored target (e.g., work of breathing).
-
G.
Intelligent (i)
Ventilator automatically adjusts the targets of the ventilatory pattern using artificial intelligence programs.
-
A.



Suggested Reading
Carlo WA, Greenough A, Chatburn RL. Advances in conventional mechanical ventilation. In: Boynton BR, Carlo WA, Jobe AH, editors. New therapies for neonatal respiratory failure: a physiologic approach. Cambridge, England: Cambridge University Press; 1994. p. 131–51.
Chatburn RL. Classification of mechanical ventilators. In: Branson RD, Hess DR, Chatburn RL, editors. Respiratory care equipment. Philadelphia: J. B. Lippincott Company; 1995. p. 264–93.
Chatburn RL. Understanding mechanical ventilators. Expert Rev Respir Med. 2010;4(6):809–19.
Chatburn RL, Mireles-Cabodevila E. Closed-loop control of mechanical ventilation: description and classification of targeting schemes. Respir Care. 2011;56(1):85–102.
Chatburn RL, El-Khatib M, Mireles-Cabodevila E. A taxonomy for mechanical ventilation: 10 fundamental maxims. Respir Care. 2014;59(11):1747–63.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Travers, C.P., Carlo, W.A., Ambalavanan, N., Chatburn, R.L. (2017). Classification of Mechanical Ventilation Devices. In: Donn, S., Sinha, S. (eds) Manual of Neonatal Respiratory Care. Springer, Cham. https://doi.org/10.1007/978-3-319-39839-6_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-39839-6_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-39837-2
Online ISBN: 978-3-319-39839-6
eBook Packages: MedicineMedicine (R0)