
Abstract
Fungal infections of the skin are the fourth most common of all conditions that cause human ill health, and as expected they include some of the most common of all human disease s such as ringworm or dermatophytosis, superficial Candida infections, and pityriasis versicolor. These are infections seen in all climates. Some such as tinea corporis are more common in the tropics, whereas foot infection is seen in all countries, and onychomycosis or fungal nail infection has a higher prevalence in the colder northern climates. All are treatable with topical or orally active antifungal drugs. In recent years there have been significant advances in their management so that most infections can be cured by either short-term topical therapy or in extensive disease states by a more prolonged course of an oral antifungal such as terbinafine, itraconazole, griseofulvin, or fluconazole. The newer antifungal drugs have not been fully evaluated as potential treatments for these conditions. Most occur in otherwise healthy individual, although oral Candida infections usually present in patients with an underlying abnormality or immunodeficiency including HIV/AIDS. Although treatment has been available for many years, antifungal resistance has only proved to be a problem in oral candidosis.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
8.1 Introduction
The fungi are recognized causes of disease in all regions of the world [1]. The most common of these infections are superficial mycoses, and these include diseases such as dermatophytosis or ringworm and candidosis. However, disabling, and potentially fatal, deep, or systemic fungal infections can also occur although many are geographically restricted to specific environments; others are opportunistic infections that develop in the ill and immunosuppressed. Fungi are eukaryotes which have a similar structure to that of mammalian cells although they also have a polysaccharide-based cell wall. Fungi grow in one of two different ways [2]. In some growth forms, known as yeasts, single cells reproduce by a process of bud formation that gives rise to single daughter cells. Other morphological forms, the mycelial or mold fungi, grow as chains of cells which appear as strands of cells, hyphae. These mycelial cells generally do not separate. Other fungi, the dimorphic fungi, exist as either yeasts or mycelia at different stages of their life cycles, a process that is often temperature dependant. In order to survive, fungi propagate by forming specialized reproductive structures or spores (conidia). These vary in morphology according to growth conditions, the most elaborate being produced only under conditions of laboratory culture. However, they may also form vegetative conidia called arthrospores which are usually located within a hyphal chain in vivo. These are thick walled cells that are able to resist periods of desiccation and poor nutrition. Arthrospores are formed by dermatophytes in vivo, for instance, in epidermis or nail, and their formation may affect the ability of antifungal drugs to destroy cells. Other superficial fungi have different structural adaptations. For instance, Malassezia species on the skin are also equipped with a thick cell wall which is grooved on the inside. Again it is thought to enable the organism to survive on the skin surface, and after treatment these cell walls are often retained even though the cell cytoplasm has been destroyed by an antifungal drug.
Fungi can cause human disease in a number of different ways, through the production of toxins or mycotoxins, through sensitizing antigens (allergens), or by the invasion of tissue. Invasive diseases caused by fungi are known collectively as the mycoses: the superficial, subcutaneous, or systemic mycoses. The superficial mycoses have been ranked as the fourth most common of all human diseases, largely because they are common at all age groups, in all climates and are often chronic unless treated. The distribution of superficial mycoses is affected by a number of factors [3] such as the presence of the organisms in the environment, host immunity, frequency, and route of exposure.
8.2 Superficial Mycoses
Superficial infections caused by fungi are common globally [3]. In addition the distribution of some is dependent on local climatic conditions or the existence of endemic foci of specific species seen, for instance, in tinea imbricata or tinea capitis. The main superficial infections are dermatophytosis or ringworm, superficial candidosis, and pityriasis (tinea) versicolor. However, other conditions such as foot or hand infections caused by Neoscytalidium dimidiatum as well as the hair shaft infections, white and black piedra, and tinea nigra are also seen.
8.3 Dermatophytosis (Ringworm)
The dermatophyte or ringworm fungi are frequent causes of superficial infection [2]. These mold fungi can invade the epidermis but their growth remains confined to the stratum corneum, the hair shaft, or the nail plate. There are three pathogenic genera of dermatophyte in humans: Trichophyton, Microsporum, and Epidermophyton. These organisms normally cause exogenous infections that originate from a source external to the patient. Human infections originate from one of three different sources—other humans, animals, or soil, known, respectively, as anthropophilic, zoophilic, or geophilic.
8.3.1 Epidemiology
In most countries dermatophytoses are common [3–6]. The main types of infection seen are tinea pedis, tinea corporis, tinea cruris, and tinea capitis. Tinea pedis is very common and in temperate climates may affect some 15 % of the population; it is less common in many parts of the tropics. Occlusion of the feet with shoes or socks predisposes to infection, although a higher proportion of the populace may have asymptomatic infections of the skin plantar skin. In communities where there is heavy industry, such as mining or petroleum refining, the incidence of foot infections may be much higher, because of the ease of spread between workers who use industrial foot wear, such as heavy boots, and communal showering facilities. There are a number of different organisms which can cause web space infections of the foot, known as athlete’s foot, ranging from dermatophytes to Candida or Neoscytalidium species and Gram-negative bacteria, and erythrasma, a Gram-positive bacterial infection. Populations of microorganisms on the feet, particularly those affecting the interdigital spaces, may vary over time and one may replace another to cause infection [7, 8]; the term “dermatophytosis complex” has been coined to describe this phenomenon where the dermatophytes are replaced, usually with Gram-negative bacteria such as Pseudomonas species. Dermatophyte infections of the feet may occur at all ages but usually start in childhood at 5–6 years of age reaching a peak in early adult life.
Tinea corporis or dermatophytosis of the trunk is usually a sporadically occurring condition as the opportunities for spread of infection are less. Often the infection originates from an animal with which the patient has contact. The most common sources are domestic pets such as cats or dogs which can be infected with Microsporum canis. However, other sources of infection are rodents, horses, cattle, and other mammals. Infection with fungi of animal origin (zoophilic infection) depends on exposure to an appropriate and infected animal source. In other areas tinea corporis is usually an anthropophilic infection arising from contact with other infected humans, e.g., tinea imbricata due to T. concentricum or tinea corporis due to T. rubrum. Some are occupationally transmissible. For instance, sportsmen and sportswomen who come into close physical contact such as wrestlers are susceptible to transmitted dermatophytes such as T. tonsurans [9], although usually an infected site is the site of contact, e.g., the face or neck area.
The epidemiology and clinical features of onychomycosis and tinea capitis are discussed in separate chapters (Chaps. 9 and 10).
8.3.2 Pathogenesis
The fungi invade the skin after adhering to stratum corneum cells and producing keratinases or proteases such as subtilisins [10, 11]. Factors which encourage fungal invasion include increased environmental humidity and CO2 content, both of which may occur in a tropical environment and in the presence of occlusion, e.g., by shoes. Less is known about those factors which determine human susceptibility, although generally it is thought that most individuals are susceptible to infection. Recently susceptibility to deep dermatophyte infections has been linked to mutations of the CARD 9 gene but as yet how susceptibility in normal populations is regulated remains a mystery [12]. The presence of antimicrobial peptides such as defensins in human epidermis plays a role in prevention of dermatophyte invasion [10]. In addition, patients with persistent dermatophytosis affecting the palms and soles are significantly more likely to have an atopic background, with a personal or family history of eczema and asthma, than others. Resistance is largely mediated via nonspecific factors such as an increase in epidermal turnover and epidermally derived peptides or by the specific activation of T cell-mediated immunity. Patients with the acquired immune deficiency syndrome (AIDS), for instance, although not apparently showing an increased incidence of infection, may have clinically atypical and extensive lesions [13]. However, even patients with an intact immune system often have a poor immunological response to dermatophyte fungi, possibly through modulation in the expression of immune responses by dermatophyte products.
8.3.3 Clinical Features
By convention, the normal term for dermatophytosis is tinea, followed by the Latin for the appropriate part of the body affected (tinea capitis, head; tinea cruris, groin, etc.).
8.3.3.1 Tinea Corporis
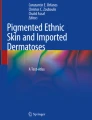
This presents with a scaly and itchy rash affecting the trunk or proximal limbs [2]. The typical lesion is a circular scaling patch with some central clearance. However, in many lesions the main abnormalities, scaling or papule/pustule formation, are seen at the edge of the lesion where an intact or broken rim can just be made out. In zoophilic infection, the lesions can be raised, indurated, and very inflamed. Pustules are sometimes seen. Tinea corporis lesions may be very large and affect a wide area on the back and chest, and, in pigmented skin, postinflammatory hyperpigmentation may mark the outline of the infected area even where there is little inflammation. In patients with HIV/AIDS, the normal pattern of symptoms and signs may be altered considerably, with extensive or follicular forms being seen in some patients. The common causes of tinea corporis are Trichophyton rubrum and Microsporum canis. Generally M. canis is more inflammatory and circumscribed, whereas T. rubrum infections may be very extensive and cover large areas, often with little inflammation (Fig. 8.1). The outline of the lesion in T. rubrum infections may be difficult to trace, although parts of the outer rim of the lesions can be distinguished as described above.

Diffuse tinea corporis caused by Trichophyton rubrum
Tinea imbricata is a specific type of tinea corporis caused by the fungus Trichophyton concentricum. It is endemic in remote and humid tropical areas in the West Pacific and parts of Malaysia, India, Brazil (Amazonas), and Mexico [14]. Lesions are characterized by the development of multiple concentric rings of scales which may cover a large area of the body from childhood (Fig. 8.2).

Tinea imbricata
8.3.3.2 Tinea Cruris
Dermatophytosis affecting the groin—tinea cruris—is a sporadic infection which may be common in most humid or tropical countries. It is almost always caused by anthropophilic species of dermatophytes, mainly Trichophyton rubrum and Epidermophyton floccosum. Sometimes these infections may become common in certain groups such as soldiers or prisoners. The usual lesion is an itchy rash with a raised border extending from the groin down the upper thigh and on occasions into the natal cleft. In women and men, it may extend around the waist area affecting the buttocks and upper thighs. In T. rubrum infections, other areas, particularly the soles or interdigital spaces on the feet, are often involved at the same time.
8.3.3.3 Tinea Pedis
Dermatophytosis affecting the feet is very common in most temperate climates; and although less common in tropical countries, it nonetheless occurs anywhere where shoes are worn. The most common sites of infection are the interdigital spaces or the soles [15, 16]. The main symptom of interdigital infection is itching. The skin is usually cracked and the main areas affected are the third and fourth interdigital spaces (Fig. 8.3). The web spaces may also appear macerated, and, if there are severe erosive changes, particularly if there is greenish discoloration of the area, Gram-negative bacteria such as Pseudomonas species may be implicated [7] as secondary invaders. This is the dermatophytosis complex type of infection, and these patients often have painful rather than itchy feet. Both Candida and erythrasma, Corynebacterium minutissimum, may cause maceration and whitening of the interdigital skin. Neoscytalidium and, less commonly Fusarium, species mimic dermatophytosis in the interdigital space usually presenting with itching and cracking of the skin. When T. mentagrophytes affects the interdigital spaces, it may cause more severe itching and the formation of vesicles or bullae (Fig. 8.4). These more inflammatory infections may also trigger an “id” reaction where the patients develop vesicular eczema (pompholyx) on the feet and the hands, the changes being more prominent on the foot where the infection started. These are immunologically mediated reactions to the presence of the dermatophyte infection, and the secondary lesions do not contain dermatophyte hyphae.

Interdigital tinea pedis caused by Trichophyton rubrum

Vesicular tinea pedis caused by Trichophyton mentagrophytes
When the infection is located on the soles, plantar tinea pedis, the main signs are scaling which often presents in tiny circular patches. Usually there is little inflammation and itching may be minimal. The infection generally becomes apparent when it spreads to involve the lateral borders of the feet, “moccasin-type infection” (Fig. 8.5). Here the scaling is easily seen on the lateral margins of the foot and may spread to involve the dorsal surface of the feet. This pattern is typical of T. rubrum infection but it can also be caused by Neoscytalidium species. Once again when T. mentagrophytes affects the soles, it may lead to the formation of bullae.

Moccasin tinea pedis caused by Trichophyton rubrum
8.3.3.4 Other Sites of Infection
Dermatophyte infections can affect the palms of the hands, tinea manuum, rather in the same way as they do the soles. Often only one hand is affected and the scaling remains confined to the palmar surface, although with extensive infection, it can affect the dorsum of the hands. Trichophyton rubrum is the usual cause.
Dermatophytosis of the face or tinea faciei is often difficult to diagnose as the changes may be subtle with little inflammation [16]. However, generally at least part of the outline of the infection can be seen. Some patients with tinea faciei complain of increased itching and sensitivity to sun exposure.
When the infection involves the beard area, tinea barbae, deep pustule formation and itching accompany the infection although the outline of the ring is often seen. In very severe cattle ringworm infection, caused by T. verrucosum, the infection in the beard area may be painful and very extensive.
8.3.4 Laboratory Diagnosis
Clinical diagnosis of dermatophytosis is not completely reliable, and ideally the presence of infection should be confirmed by demonstrating the organisms in skin scrapings taken from lesions [2]. Scrapings are generally best removed with a blunt scalpel from the edge of lesions or by using the reverse side of a scalpel blade. For diagnosis they are mounted in 5–10 % potassium hydroxide and are then microscopically examined. The organisms are seen in scrapings as chains of cells forming hyphae. In addition, they can be cultured on mycological media such as Sabouraud’s agar, and their gross and microscopic morphology is used to distinguish the different species. At present molecular techniques play little part in the diagnosis of dermatophytosis of the skin [17].
8.3.5 Management of Dermatophyte Infections
The treatment of dermatophyte infections is now comparatively simple, and cure rates range from 80 to 90 %. There is a wide range of antifungal agents which can be used in both topical and oral formulations [18–20]. All these are effective in a substantial majority of patients, provided that they are used regularly and as instructed. In assessing therapeutic response, there has been a trend to favor the use of complete clinical cure as a primary end point for clinical trials; secondary end points are a complete mycological cure or combined mycological and clinical cure or clinical improvement [20, 21]. These assessments have an impact on the interpretation of studies as the older studies often used complete clinical cure or 90 % improvement as primary end points. In some forms of dermatophytosis such as interdigital tinea pedis or onychomycosis (see Chap. 10), complete clinical recovery is often not achieved during the time period of the study as the timing of improvements in the pathological changes lags behind that for disappearance of the organism.
The approach currently adopted to treatment of dermatophytosis affecting the skin is to use topical treatments for well-circumscribed infections or infections of limited extent and oral treatments for extensive infections or those affecting hair or nails where, despite many attempts to design new topical applications with a high degree of penetration to the infected site, there has yet to be a breakthrough in local therapy. A further issue of importance in the management of dermatophytosis is compliance with treatment as many patients find repeated applications time consuming and difficult, and there is a high rate of noncompliance with longer topical treatment regimens [22]. For this reason some antifungals have been assessed in trials for once rather than the more usual twice-daily application. It is difficult to comment, therefore, on their relative effectiveness as a function of the frequency of application, as many of those licensed for twice-daily use have not been formally studied in once-daily treatment regimens and may be similarly effective.
8.3.5.1 Topical Applications (Table 8.1)
A great variety of topical applications have been used for the treatment of ringworm infections [19, 23–41]. They have the advantage of being relatively free from adverse effects. Allergic contact dermatitis is rare. Irritant effects may occur with any of them, especially on raw skin and in fissures between the toes, but generally are not common. However, benzoic acid compound ointment (Whitfield’s ointment), full strength, is particularly irritant and is not used on tender skin sites, such as the scrotum or the groin area. Magenta paint (Castellani’s paint) is still used in some cases of inflammatory tinea pedis, particularly when bacterial infection coexists, although potassium permanganate followed by a topical antifungal is preferred for exudative or weeping foot lesions. Other cream or powder preparations that can be purchased without prescription include tolnaftate or zinc undecenoate. Haloprogin is another antifungal which, although it is not extensively used, is an effective topical treatment.
Imidazole preparations for topical use, such as clotrimazole, miconazole, econazole, and ketoconazole, are now well established as effective treatments in ringworm infections with an extremely low incidence of adverse reactions; other drugs in this group, isoconazole, tioconazole, and sulconazole, are equally effective. Newer preparations such as sertaconazole [28, 37], luliconazole [20], and isoconazole [23] are available in some countries. Generally the azole antifungals are available in cream, solution, or spray formulations at a concentration of 1 %. Most are used twice daily for 2–4 weeks although some, such as bifonazole, are licensed for once-daily use. The most recent Cochrane review of topical treatments for foot infections indicates little difference in efficacy between these different azole compounds.
The major alternative treatment is the topical formulation of terbinafine [22]. Terbinafine applied locally in dermatophytosis has been shown to produce responses in some dermatophyte infections, e.g., interdigital tinea pedis, after very short periods of application, e.g., 1–7 days. Also 1 week of topical terbinafine was found to be more effective than 4 weeks of clotrimazole in tinea pedis. There is also a topical formulation of terbinafine which is designed for use in infections of the foot and across the sole in a film-forming solution which is used as a single application only [41]. The solution is applied and left to dry for 3–4 min. Other allylamines such as naftifine [33] and butenafine [34] are also effective. Ciclopirox is available in some countries as a topical application for use in dermatophytosis [26].
There has been considerable recent work on developing new formulations of topically active antifungal drugs to improve efficacy. The single application terbinafine film-forming solution was discussed above but other approaches to new formulations include both gels and sprays. Work has also been carried out to assess whether application of a co-treatment with 40 % urea would enhance clinical efficacy [36]. Few of these approaches have been adopted into clinical practice.
8.3.5.2 Oral Antifungals
The mode of action, pharmacology, and adverse events related to the oral antifungal medications are discussed in Chapter. This section is concerned with the specific use of these drugs in dermatophyte infections.
Terbinafine
Terbinafine is a member of the allylamine antifungal group, which acts by the inhibition of squalene epoxidase in the formation of the fungal cell membrane. When given orally, it is rapidly laid down in the stratum corneum, and it persists in nails at high concentrations for several months. These may exceed the minimum inhibitory concentration for a long period after the end of therapy. Terbinafine is given orally in a dosage of 250 mg/day for dermatophytosis. It has produced rapid and long-lasting remissions in dry-type tinea pedis and tinea cruris, as well as tinea corporis. A smaller tablet form of 125 mg is available in some countries for treatment of children.
Itraconazole
This is an orally absorbed triazole. It has similar activity to the imidazole, ketoconazole, but without the heightened risk of hepatotoxicity. Its mode of action is through the inhibition of the cytochrome P-450-dependent demethylation stage in the formation of ergosterol on the fungal cell membrane. It is active against a wide range of dermatophytes and is effective in regimens of 100 mg for 15 days in tinea cruris and corporis or 30 days in dry-type tinea pedis. The currently preferred regimen uses 400 mg/day, given as two daily doses of 200 mg. In tinea corporis, 1 week of therapy at this dosage is sufficient and in dry-type tinea pedis 2 weeks. Occasionally, longer periods of treatment are needed.
Griseofulvin [13]
This is a metabolic product derived from species of Penicillium, which was first isolated from P. griseofulvum. Its activity, which is fungistatic, is largely restricted to dermatophyte infections. The usual human regimen is 10 mg/kg/day given in tablet form. There is a solution form for children although this is no longer available in many countries. Treatment duration varies between 2 and 4 weeks for tinea corporis or cruris. The use of griseofulvin has largely been superseded in many countries by terbinafine or itraconazole, except in tinea capitis (Chap. 9).
Ketoconazole
This orally active imidazole is a broad-spectrum antifungal agent. In ringworm infections requiring systemic treatment, it offers an alternative agent and is given in a 200–400 mg/day regimen with food (for adults). Hepatitis is a proven complication, occurring in approximately 1 in 10,000 patients. Because of this, ketoconazole is not used in Europe and the USA for superficial infections.
Fluconazole
Fluconazole is an orally active triazole antifungal used for the treatment of dermatophyte and Candida infections as well as systemic mycoses. It can also be given as daily treatment of 100 mg 2–4 weeks in dermatophyte infections of the skin. It can also be used in a regimen of 150 mg/week for 2–3 weeks for tinea corporis and tinea cruris and somewhat longer for dry-type tinea pedis. There are fewer interactions than with itraconazole but, like the latter, side effects are rare and mainly confined to gastrointestinal discomfort.
There is little data at present on the use of posaconazole and voriconazole in dermatophytosis affecting the skin. New oral drugs such as pramiconazole, ravuconazole, and albaconazole have been tested by clinical trial in specific dermatophyte infections but at present have not been marketed for these indications.
8.3.6 Treatments in Practice
The different clinical forms of dermatophyte infection require different approaches to treatment. Generally, topical therapies are used for localized or mild infections and oral antifungals for the more extensive infections [23]. The oral azoles, such as fluconazole or itraconazole and terbinafine, are now the preferred oral treatments for extensive or severe dermatophytosis rather than griseofulvin; they are also used in severe steroid-treated dermatophyte infections which often develop follicular or pustular changes (Fig. 8.6).

Steroid-treated tinea corporis
8.3.6.1 Tinea Corporis
Localized or nonextensive tinea corporis responds to topical therapy applied twice daily, usually for about a month. Topical terbinafine often works in a shorter time (e.g., 2 weeks) than topically applied azoles. But because of the difficulty in accurately locating the extent of infection in more widespread infections of recent onset, oral terbinafine or itraconazole will generally be preferred, and these clear the condition in 2–3 weeks, depending on the dosage used. With griseofulvin, longer periods of treatment are effective. In tinea imbricata, the most appropriate duration of the treatment regimen is not clear although 2 weeks of terbinafine has been found to be effective.
There is a form of persistent tinea infection usually caused by T. rubrum at sites in the groin or the trunk which, while responding initially to treatment with either terbinafine or itraconazole, relapses quickly. Different treatment regimens have been tried including combinations of azole or allylamine oral medications plus topical azoles or allylamines. At present there is no effective remedy in these cases. In contrast tinea infections of the skin in immunosuppressed patient including those with HIV/AIDS usually respond to treatment although it is often necessary to double the normal dose.
8.3.6.2 Tinea Barbae
Tinea barbae or infections of the beard usually respond satisfactorily to itraconazole or terbinafine, sometimes in combination with topical therapy over a period of 4–6 weeks. Long-term follow-up is recommended, as late recurrences occur.
8.3.6.3 Tinea Facei
In localized cases, promptly diagnosed, topical therapy works well, especially with terbinafine or one of the imidazoles. When steroid therapy has modified the underlying infection, oral terbinafine or itraconazole is generally preferred. Most cases will clear in 3 or 4 weeks, certainly in 6 weeks, but long-standing infections may occasionally need longer periods of treatment.
8.3.6.4 Tinea Pedis
For very mild toe cleft changes, one of the topical antifungal preparations is generally used. With toe cleft changes that are more than trivial, a cream is preferred to a powder and any of the preparations discussed previously can be used for minor forms of tinea pedis. Imidazole preparations are cheap and are usually effective in up to 30 days, but topical terbinafine can be used for a period of 7 days; most antifungals are given twice daily, exceptions include bifonazole which is a once-daily treatment. The film-forming solution of terbinafine is applied once across the soles of the fee and is effective for both dry-type sole and interdigital infections. If the toe clefts are very inflamed and secondary bacterial infection is likely, potassium permanganate tablets dissolved in water used as a soak in a basin for 15–20 min twice daily can ease secondary infection. If there is any evidence of serious bacterial infection, swabs should be taken to confirm the identity of the organism. With dermatophytosis complicated by Gram-negative bacterial infection, both infections should be treated. Many topical antiseptic preparations such as povidone or hydrogen peroxide (Crystacide) products are active against the bacteria, while topical formulations of imidazoles or terbinafine can be used for the fungal infection. None of the topical antifungals has activity against Gram-negative bacteria, although most azoles, apart from ketoconazole, have moderate efficacy against Gram-positive bacteria such as Staph aureus. If there is clinical evidence of cellulitis, patients should receive a systemic antibacterial antibiotic.
In dry-type tinea pedis, which is usually caused by T. rubrum, terbinafine or itraconazole are the preferred treatments. Speed of recovery is faster and relapse rates less than with griseofulvin. Treatments using terbinafine 250 mg/day for 2 weeks or itraconazole 400 mg/day for 1–2 weeks are usually given.
8.3.6.5 Tinea Cruris
Topical therapy is usually effective within 2–4 weeks. Tolnaftate, terbinafine, and the imidazoles are well tolerated in the flexural areas, and if the diagnosis is in doubt, terbinafine and the imidazoles have the advantage of being effective topically against Candida as well. Where the condition has resisted topical treatment, or has spread more widely to the pubic area, the natal cleft, or the buttocks, and where topical steroids have been used, systemic treatment is advisable. Oral terbinafine or itraconazole usually produces remission in 1–2 weeks. Some patients relapse even after this therapy and a longer course of therapy may be necessary.
8.3.6.6 Tinea Manuum
Ringworm infections of the palm are not easy to clear, and oral therapy is always needed. Itraconazole and terbinafine are both effective in this condition. Most cases clear with 2–4 weeks of treatment although it may be advisable to review the results a few months after the end of treatment.
8.3.7 Prevention
Prevention of dermatophytosis is not practicable except in situations where there is a high risk of spread to other individuals. Infected individuals using gyms or public swimming paths should be encouraged to seek treatment.
8.4 Superficial Candidosis
Superficial infections due to Candida species are common [42] and include oral and vaginal as well as skin infections. The principal pathogen is C. albicans, although other species such as C. tropicalis, C. parapsilosis, C. krusei, and C. glabrata may also cause human infections. The disease is seen worldwide, although some clinical varieties such as interdigital candidosis are more common in warm climates.
8.4.1 Epidemiology
Candida albicans is a normal commensal of the mouth, gastrointestinal tract, and vagina. Carriage rates vary but 15–60 % of normal individuals have commensal carriage in the mouth. Somewhat lower percentages have colonization of the gastrointestinal tract or vagina [43]. Colonization does not usually affect the skin. Candidosis of the skin is seen in association with diabetes mellitus (groins) and obesity (interdigital). But not all patients have a predisposing risk factor, and women with vaginal candidosis usually have no underlying heath problem. Oral candidosis is a common problem in immunocompromised patients including those with HIV/AIDS not receiving antiretrovirals [44].
Survival of the organisms in these sites depends on a variety of factors, including their ability to adhere to mucosal cells and compete with commensal bacteria. Factors which disturb this balance favor either elimination or growth and subsequent invasion by the organism. For instance, use of antibiotics eliminates other members of the commensal flora of the mouth and bowel and allows Candida to invade. Depression of either T lymphocyte or neutrophil-mediated immunity allows the organisms to grow and invade following inhibition of normal control mechanisms [42]. As with dermatophytes, antimicrobial peptide products expressed in the epidermis are inhibitory to Candida species. By contrast, in most skin infections, a key element in invasion appears to be occlusion which encourages infection, rather than any defect of host immunity.
8.4.2 Clinical Features
The main clinical forms of superficial disease are oropharyngeal, vaginal, and cutaneous candidosis. In addition, chronic mucocutaneous candidiasis is a rare chronic skin and mucosal infection of predisposed patients. Systemic candidosis is a potentially life-threatening infection generally confined to compromised patients; it occasionally presents with skin signs.
8.4.2.1 Oral Candidosis [45, 46]
There are different clinical forms which depend partially on the underlying predisposing factors.
-
1.
Acute pseudomembranous candidosis. This presents with one or more patches of creamy or white pseudomembrane on an erythematous base. The infection is sore and taste may be altered. The common sites affected are the buccal epithelium on the cheeks, the gums, or the palate. In immunocompromised patients, the dorsum of the tongue may be affected; extension to the pharynx or the esophagus may occur, and stricture is a complication of persistent or relapsing infection.
-
2.
Acute erythematous candidosis (“antibiotic sore tongue”). There are soreness and atrophic erythematous mucous membranes, particularly on the dorsum of the tongue. It may follow pseudomembranous candidosis. It is especially associated with antibacterial antibiotic therapy, but is also seen in HIV-positive subjects and patients taking inhaled steroids.
-
3.
Chronic pseudomembranous candidosis. This does not differ clinically from the acute pseudomembranous variety but, as the name suggests, lesions are persistent. It is mainly seen in immunocompromised patients.
-
4.
Chronic erythematous candidosis (denture sore mouth). Erythema and soreness in the epithelium in the denture-bearing area are common and most are caused by candidosis. It is likely that other factors such as chronic irritation and bacterial colonization have a role in the pathogenesis of this condition. It is most common on the palate and gums. AIDS patients with erythematous candidosis usually have chronic infections.
-
5.
Chronic plaque-like candidosis (chronic hyperplastic candidiasis; Candida leukoplakia). This presents with chronic irregular white plaques that occur in the mouth, commonly on the cheek or the tongue. Symptoms are mild. Unlike the pseudomembrane of oral thrush, this plaque cannot be easily removed. Smokers appear to be particularly prone to develop this form of oral candidosis and true leukoplakia can develop in the area affected.
-
6.
Chronic nodular candidosis. This is a rare form, which produces a white and cobbled appearance. It is most often seen in patients with chronic mucocutaneous candidosis.
Other forms of oral candidosis include angular cheilitis which presents with soreness at the angles of the mouth extending outward in the folds of the facial skin. In atopics Staph aureus can cause a similar appearing syndrome. Candida can also secondarily infect other oral conditions such as ulcerative lichen planus, leukokeratosis, and white-sponge nevus.
8.4.2.2 Candida Intertrigo
This occurs with infection of the skin surface in body fold areas, due to Candida species usually C. albicans [42]. It is often a primary event although it may also be secondary to adjacent infection; for instance, the skin of the groin may be involved secondary to vaginal infection when there is spread of infection to the vulva and the perineum. In this case a prominent red rash in the groin and on the upper surface of the thighs may appear, together with satellite pustules and papules outside the ring margin of the infection. The same can occur in other sites such as beneath the breasts and around the umbilicus. In some cases, there is no underlying skin abnormality, although groin candidosis in males and females is more common in diabetic subjects. Eczema or psoriasis of the skin flexures may also be accompanied by secondary candidosis, and again the presence of satellite pustules is an important diagnostic clue.
8.4.2.3 Interdigital Candidosis
Infection of the finger- or toe-web spaces by Candida is more common in hot climates or in patients with long-standing interdigital disease, and it may also form part of the dermatophytosis complex discussed previously as a secondary infection following interdigital dermatophytosis. It is a common type of fungal foot infection in military groups in the tropics. Lesions are white with soggy-looking skin which is superficially eroded. Lesions between the fingers are mainly seen in women and a relationship between repeated washing and cooking has been suggested; it is also more common in those who are overweight. Here the interdigital skin becomes macerated and fissured.
8.4.2.4 Candida Infection and Nappy Dermatitis
Nappy rash in infants is a form of irritant eczema which is often secondarily infected with, among other organisms, C. albicans. The presence of yeasts may be suspected by the appearance of satellite pustules, and this can be confirmed by culturing the organisms from swabs of the area.
8.4.2.5 Vulvovaginal Candidosis
This condition affects around 75 % of women of childbearing age at least once and presents with itching and soreness and with a thick, creamy white discharge. In many patients there is erythema of the vaginal mucosa together with the discharge, but on occasions the only sign is erythema. Most women with vulvovaginal candidosis have no evidence of any underlying disease. The rash may extend onto the perineum and into the groins. The perianal area is often affected. In extensive cases, satellite pustules may be seen peripherally.
Candida vulvovaginitis may become recurrent, and in around 4 % of women with the infection, it becomes a chronic or chronically relapsing condition. In chronic cases, the vaginal mucosa is often glazed and atrophic. There may be considerable vaginal soreness or irritation as well as pain during intercourse.
It is important in patients with chronic symptoms to evaluate the presence of Candida during repeated episodes, to establish that recurrence of signs of disease is associated with recurrence of Candida as other causes of vaginosis or Chlamydia infection may be causing the symptoms.
8.4.2.6 Candida Balanitis
The skin of the glans penis may develop a Candida infection usually when the sexual partner has a symptomatic infection. In mild cases, transient tiny sore papules or pustules develop on the glans penis a few hours after intercourse and rupture, leaving a peeling edge. In more severe and chronic cases, the inflammatory erythematous changes become persistent over the glans and the prepuce. There may be associated involvement of the groins.
8.4.2.7 Chronic Mucocutaneous Candidosis [47, 48]
The rare syndrome of chronic mucocutaneous candidosis (CMC) usually presents in childhood or infancy with oral, nail, and cutaneous candidosis which recurs despite treatment. Other chronic skin infections such as warts (papillomaviruses) and dermatophytosis may also develop. Some forms also present in adult life.
The oral lesions are usually of the chronic pseudomembranous or plaque types. But in addition the skin may be covered with hyperkeratotic plaques particularly where the infection has spread to the face or scalp. The fingernail changes involve the nail plates, nail folds, and periungual skin, all of which may be severely damaged.
A large number of immunological abnormalities have been described in association with this condition, but with few exceptions, these have been found to change with time and therapy. In most cases infection forms part of the autoimmune polyendocrinopathy, candidosis, and ectodermal dystrophy syndrome with associated hypoadrenalism, or hypoparathyroidism; the common defect is a mutation in the autoimmune regulator (AIRE) genes [47]. A second variety occurs with autoimmune thyroid disease [48] and is associated with mutations in the STAT1 gene. Extensive immunological investigation of children with CMC is not necessary unless they have very severe or recurrent infections or a history suggestive of abnormal responses to other infections, such as chickenpox or severe staphylococcal boils. Here it is worth excluding functional leukocyte abnormalities, such as chronic granulomatous disease, although such patients usually have a history of internal infection. With the exception of bronchiectasis, most patients with CMC do not have internal disease, although the most severely affected patients may later develop systemic infections such as tuberculosis. All cases should be screened for endocrinopathy, and if this is negative on first testing, it should be repeated if necessary annually, as the Candida infection often predates endocrine dysfunction.
8.4.3 Laboratory Diagnosis
The diagnosis of superficial candidosis can be confirmed by direct microscopy (see dermatophytosis) of skin scrapings or swabs [42]. Both yeasts and hyphae can be seen. Candida species can be distinguished by culture and by assimilation and fermentation reactions. Although molecular diagnostic tests have been developed, few are available commercially.
8.4.4 Treatment in Practice
Candida infections of the skin respond well to a range of antifungals available in cream, powder, or solution forms [42, 49, 50]. Antifungal agents not discussed under dermatophytosis are the topical forms of the polyene antifungal drugs such as nystatin, amphotericin B, and natamycin [51]. These are available in different countries although the topical polyene most widely found is nystatin which is produced in cream form but also as lozenges for oral infection and as a vaginal tablet.
Other useful antifungals for candidosis are azole drugs (econazole, clotrimazole, ketoconazole, miconazole). Generally superficial infections due to Candida of the skin and mucous membranes respond well to these treatments.
The most commonly used oral treatments for candidosis are the two triazoles, fluconazole [52], and itraconazole [53]. The usual daily doses are itraconazole 100–200 mg and fluconazole 100–400 mg. A formulation of itraconazole in cyclodextrin solution is better absorbed in severely immunocompromised patients where there is wide individual variation in absorption of the drug. Resistance to fluconazole is an emerging issue which has been reported in HIV/AIDS or CMC patients receiving long-term therapy. Within an infected area such as the mouth, there may be both sensitive and resistant strains of Candida isolated showing that there is heterogeneity of the population in an infection [54]. Characteristically patients at risk from drug resistance are those with persistent infection requiring long-term suppressive treatment and who are immunosuppressed. Primary drug resistance to fluconazole has been recorded with some C. albicans species and with C. krusei, C. dubliniensis, and C. glabrata. However, Candida resistance is less common in patients under treatment for candidosis who are receiving highly active antiretroviral (HAART) therapy [55]. Other azoles active against Candida species include voriconazole and posaconazole [56, 57]. Both have been used for severe oropharyngeal and esophageal infection in the seriously ill. In addition caspofungin and anidulomycin, intravenous fungal cell wall inhibitors [58], are other anti-Candida agents used in systemic or esophageal infections.
Flucytosine is an oral agent that is absorbed from the gut and is relatively safe and active against those sensitive strains of Candida [42]. Resistance may develop during treatment, and this drug is now only occasionally used for candidosis as a sole treatment.
8.4.4.1 Oral Candidosis
In infants, suspensions of nystatin, amphotericin, or miconazole gel for 2–3 times a day are usually effective in treating oral candidosis. A mucoadhesive oral form of miconazole is also effective as treatment [59]. In adult patients with dentures, removal of these combined with careful cleansing at night is important in ensuring success [60]. Amphotericin or nystatin lozenges, oral nystatin suspension or miconazole oral gel, or mucoadhesive tablets are effective treatments in non-immunocompromised patients. The duration of the treatment varies with the patients underlying condition: 10–14 days may be enough in acute cases in the immunologically normal. For treatment of chronic infections, such as those with hyperplastic or chronic erythematous candidosis, the responses to topical therapy are poor, and orally absorbed drugs such as fluconazole (100–200 mg/day) or itraconazole (100–200 mg/day) are more effective. Voriconazole and posaconazole are alternatives.
Oral candidosis in patients with HIV/AIDS, not receiving antiretrovirals, or CMC, usually fails to respond to topical polyene or azole therapy. Fluconazole and itraconazole are the drugs of choice. If possible, therapy should be given in short courses, because of the risk of resistance with continuous therapy. Treatment is continued until there is clinical recovery. The solution formulation of itraconazole is an alternative to the capsule form, and a new and more consistently absorbed itraconazole formulation (SubaCap) is available in some countries. Posaconazole and voriconazole are alternative treatments.
8.4.4.2 Genital Candidosis
Acute vulvovaginitis can be treated with a single-dose topical preparation (pessary, ovule), such as clotrimazole, econazole, or isoconazole. Longer courses of treatment with azoles (e.g., 14 days), as well as the polyenes, such as nystatin, can also be used. Single-dose oral treatment with fluconazole 150 mg is widely available without prescription and is convenient; an alternative single does treatment is itraconazole 600 mg [61]. There is no completely dependable method of curing recurrent vaginal candidosis [62], although solutions includes using long-term suppressive treatment in pulses with itraconazole and fluconazole both being used.
Candida balanitis usually responds to topical antifungals applied several times a day, but if there is a source of infection in the sexual partner, this should be treated appropriately.
8.4.4.3 Flexural Candidosis
Candida intertrigo requires topical therapy (azole or polyene creams) given for 2 weeks, but treatment may be continued for longer periods. Drying the infected site is also important. For instance, in some patients with moist Candida intertrigo, potassium permanganate soaks are effective. In finger- or toe-web infections, topical antifungal therapy is appropriate.
8.4.4.4 Rashes in the Napkin or Nappy Area
Rashes in the napkin area in infants should be investigated for Candida, and, if present, this can be treated topically with an antifungal often combined with hydrocortisone. The antifungal should be combined with a general regimen for napkin or diaper dermatitis, with frequent napkin changes.
8.4.4.5 Paronychia and Onychomycosis
Candida paronychia respond to prolonged topical therapy with frequent applications of polyenes, imidazoles, or antiseptics such as 4 % thymol in chloroform. Lotions are probably preferable to creams as they are easier to apply to the nail-fold area. There have been few studies of either itraconazole or fluconazole although they are effective in many cases of paronychia. Antifungal treatment should be followed by general measures, such as adequate drying of the hands. Other factors such as irritant or allergic contact dermatitis may play a part in the continuing inflammation. In many cases the addition of a topical corticosteroid is a logical approach.
8.4.4.6 Chronic Mucocutaneous Candidosis
Treatment of this condition depends on antifungal chemotherapy although attempts have been made to restore T-cell function by the use of different measures such as transfer factor, or grafting compatible lymphocytes from blood or marrow, and nonspecific measures such as restoration of normal iron stores when these are low. Systemic anti-Candida therapy with fluconazole, itraconazole, or posaconazole is usually necessary, and treatment may have to be prolonged and repeated.
When the patient is in clinical remission, maintenance therapy should be avoided if possible because of the risk of antifungal resistance. But controlling infection is advisable as many patients develop deeper lesions in the pharynx and esophagus which may lead to the formation of strictures. Intermittent therapy with oral antifungals such as fluconazole is the usual approach. Nonabsorbed oral medications such as miconazole gel and nystatin are also worth trying although these are often less effective than the absorbed oral drugs. There is sometimes a role for alternative medicines such as posaconazole or intravenous caspofungin, an echinocandin cell wall antagonist. Endocrine deficiencies should be treated, although such treatment by itself has no clinical effect on the candidosis. Endocrine screening tests should be repeated, even if initially negative, as patients with endocrinopathy may develop endocrine disease years after the first appearance of candidosis. Where indicated, parents should be given genetic counseling. The possibility of coexisting dermatophytosis should not be forgotten, but it usually responds satisfactorily to oral treatment with itraconazole or terbinafine.
8.5 Neoscytalidium Infections
Neoscytalidium dimidiatum, a plant pathogen found in the tropics and subtropics, and N. hyalinum, which has only been isolated from humans, cause infections of the skin which mimic the dry-type infections caused by Trichophyton rubrum [63, 64]. These infections have mainly been reported in immigrants from tropical areas to temperate countries, although infection in the tropics may be more common than previously believed. Studies from Nigeria, for instance, have suggested that this is a common infection in both dermatological outpatients and industrial groups such as mine workers. Infections have been reported from West and East Africa, India and Pakistan, Thailand, Hong Kong, and several countries in Latin America.
The infection presents with scaling of soles and palms (Fig. 8.7) and cracking between the toe webs. Nail dystrophy is common and onycholysis without significant thickening is often seen; some patients have nail-fold swelling. The clinical features of N. dimidiatum and N. hyalinum infections are indistinguishable.

Neoscytalidium hyalinum infection of the palms
It is important to recognize these infections because they are common in some areas and do not respond to most antifungal drugs. The laboratory diagnosis is similar to that used in dermatophytosis—skin scrapings and culture. The appearance of these fungi in skin scrapings is characteristic as they are sinuous and irregular. They cannot be cultured on media containing cycloheximide.
Treatment of these infections is difficult as they do not respond in a predictable way to topical or oral antifungal drugs. Responses of skin infection in individual patients have been recorded with a number of compounds such as Whitfield’s ointment, econazole, or terbinafine, although relapse is common.
8.6 Malassezia Yeast Infections
The Malassezia (lipophilic) yeasts are skin-surface commensals which have also been associated with certain human diseases, the most common of which are pityriasis versicolor, Malassezia folliculitis and seborrhoeic dermatitis, and dandruff [65, 66]. In addition these organisms rarely cause systemic infections, usually in prematurely born infants receiving intravenous lipid infusions. There are a number of Malassezia species, of which the main ones are M. sympodialis, M. globosa, M. restricta, M. slooffiae, M. furfur, and M. obtusa which are oval or round yeasts and their distribution on the skin surface differs. M globosa and M sympodialis are the most common and most widely distributed of these yeasts. The formation of short stubby hyphae by round yeasts on the skin surface is a feature of the development of pityriasis versicolor.
8.6.1 Pityriasis Versicolor
The pathogenesis of pityriasis versicolor is still poorly understood. The disease occurs in young adults and older individuals but is less common in childhood. Most cases are caused by M. globosa. Pityriasis versicolor is a common disease in otherwise healthy patients. However, it has also been associated with Cushing’s syndrome and immunosuppression associated with organ transplantation, but not with HIV/AIDS. The infection is very common in the tropics, and incidence rates of over 70 % have been reported in some studies. Generally this disease is associated with warm climates and sun exposure. Studies of the immunology of pityriasis versicolor suggest that one potential reason for persistence of the infection is inhibition of the induced immune responses due to a lipid associated with Malassezia species.
8.6.1.1 Clinical Features
The rash consists of multiple hypo- or hyperpigmented, occasionally red, macules which are distributed across the upper trunk and back which coalesce with time (Fig. 8.8). The lesions are asymptomatic or mildly itchy and scaly. The hypopigmented lesions may be confused with vitiligo, but the presence of scaling and partial loss of pigment is, however, typical of pityriasis versicolor. In some individuals, there is more erythema and the lesions may resemble those of seborrhoeic dermatitis (see below) (Fig. 8.9); in these cases the infection is often recalcitrant and difficult to treat adequately, whereas usually treatment is straightforward and effective. Rare forms of pityriasis versicolor include atrophic, or anetoderma-like, lesions and an atypical variety which presents with scaly patches that are irregularly distributed around the waist area or upper part of the limbs.

Pityriasis versicolor

Pityriasis versicolor (erythematous type)
Lesions can also be highlighted by shining a wood’s light on the area. They fluoresce with a yellowish light, although this is generally a weak response and complete darkness and a powerful light source are necessary. Scrapings taken from the lesions will show the characteristic organisms, which consist of clusters of round yeasts closely associated with short stubby hyphae. These are normally viewed in 10 % potassium hydroxide-treated mounts, as with dermatophytosis. This infection is usually caused by Malassezia globosa but neither cultural nor molecular diagnostic methods are necessary for diagnosis.
8.6.2 Malassezia Folliculitis
A second condition associated with Malassezia yeasts is an itchy folliculitis on the back and upper trunk which often appears after sun exposure usually in teenagers or young adults; it is more prevalent in males. Lesions are itchy papules and pustules which are often widely scattered on the shoulders and back. The condition has to be distinguished from acne as it does not respond to the same range of treatments. But itching is prominent and there are no comedones.
8.6.3 Seborrhoeic Dermatitis
A third common condition associated with Malassezia species is seborrhoeic dermatitis. While this cannot be considered an infection because there is no tissue invasion, there is strong and growing evidence that in this condition, Malassezia species such as M. globosa or M. restricta produce breakdown products including oleic acid or immune signaling molecules such as indolocarbazole or malassezin, which play a role in triggering inflammation in the skin which results in the rash of seborrhoeic dermatitis [67]. It is still not clear why this is common in patients with Parkinsonism or with HIV/AIDS. However, a key part of treatment is the use of antifungal drugs active against Malassezia.
The characteristic distribution of seborrhoeic dermatitis includes scaling affecting the scalp either diffusely or in patches, scaling and erythema of the eyebrows, nasolabial folds, external ears, and presternal panel of the anterior chest. Other affected areas include additional sites on the face and the axillae or groins. The rash is covered with greasy scales and may be very itchy. Isolated scaling of the scalp without other signs of disease, dandruff, is thought to be a mild variant of seborrhoeic dermatitis.
One other condition associated with Malassezia and which may improve with the use of antifungal agents is a head and neck eczema seen in atopic patients which usually presents in early adult life.
8.6.4 Treatment in Practice
One of the main features of the treatment of pityriasis versicolor is that a wide range of different antifungal drugs is effective in the short term against this infection [49, 68–70]. Usually assessments have been made at between 2 weeks to 1 month post therapy and cure rates of over 85 % are achievable. Some drugs which are not known to have antifungal properties but which may affect the environment, which supports Malassezia such as adapalene, have also been used [71]. Topically applied azole antifungals such as miconazole, clotrimazole, ketoconazole, and sertaconazole work well in pityriasis versicolor, and there is no difference in results achieved by different antifungal compound [72]; generally imidazole creams are used. Topically applied allylamines such as terbinafine 1 % cream, naftifine, or butenafine are also effective in pityriasis versicolor. Likewise topical ciclopirox is effective. The usual time to recovery with all treatments is 2–3 weeks. The main problem with the use of topical antifungals is the practical difficulty in applying creams to a wide and ill-defined surface area. An alternative solution is to use a formulation which can be spread easily across a wide surface area ketoconazole shampoo which, by virtue of its composition, is easier to apply or an alternative formulation in mousse form, ketomousse [73]. Ketoconazole shampoo is left on the skin after lathering the preparation into the skin for at least 5 min before showering. Ketoconazole shampoo has not been formally evaluated in pityriasis versicolor, but two or three applications of the shampoo over a week appear to clear most infections.
A second approach is the application of 2.5 % selenium sulfide in a detergent base (Selsun® shampoo) [74]. It is applied to all the affected areas and left overnight. In many cases, it is necessary to apply the material regularly (e.g., every other night over 2 weeks). It is irritant and it also stains clothes and bedding. Alternatives include 20 % sodium hyposulphite solution and 50:50 propylene glycol in water. The latter has also been used intermittently as long-term suppressive therapy to prevent relapse.
Oral itraconazole is also very effective in cases of pityriasis versicolor, mainly for extensive or recalcitrant cases [72]. This approach has the advantage of simplicity and convenience for the patient. Itraconazole is active against pityriasis versicolor in a total dosage of 800–1,000 mg usually given over 5 days; a single dose of itraconazole at 400 mg has also been used but long-term results are not known. Fluconazole can also be used [66]. Ketoconazole is also effective although now little used.
On a practical point, patients should be warned that depigmentation may take several months, as otherwise they will often report treatment failure, even when the organisms have been destroyed, simply because the hypo- or hyperpigmentation persists for several months.
The other common clinical problem is relapse and in certain patients relapse can be rapid; also there are some patients who regularly develop pityriasis versicolor when exposed to climatic conditions which are suitable for the development of this infection. There are no studies of methods of managing these apart from the long-term use of propylene glycol. However, one method of approaching the latter problem where patients reacquire pityriasis versicolor when revisiting an overseas climate is to give treatment once weekly during their overseas stay with ketoconazole shampoo or an equivalent.
The best treatment for Malassezia folliculitis is itraconazole given orally at a dose of 100 mg daily for 2–3 weeks rather than topical treatment, to which this infection seldom responds [75].
In seborrhoeic dermatitis, there have been a few studies of the efficacy of azole antifungals. In a systematic review [76] on the subject, there was evidence that medications containing ketoconazole applied topically either to the scalp or facial skin were effective. Likewise there are also studies with bifonazole and selenium sulfide that demonstrate efficacy [76]. In practice other azoles appear to be effective and in extensive cases oral itraconazole can be used usually for 10–14 days to induce a remission. Relapses are managed with a topical azole containing cream or shampoo. Alternatives includes topical corticosteroids or topical tacrolimus. The practical problem with this condition is that it relapses often on a regular basis and patients should be made aware of this.
8.7 Rarer Superficial Infections
White piedra is a chronic infection of the hair shafts caused by a yeast, Trichosporon beigelii. This disease can be seen in temperate and tropical areas. It is generally sporadic and rare and the infection is mainly seen in genital hair. It may also affect the axilla and scalp [77]. The lesions are soft yellowish nodules around the hair shaft but it is usually asymptomatic. Black piedra caused by Piedraia hortae is a rare asymptomatic infection confined to the tropics [78]. Here, scalp hairs are surrounded by a dense black concretion containing spores, forming a small nodule. Both infection are best treated with topical imidazole solution or creams for 2–3 weeks.
Tinea nigra is an infection of palmar or plantar skin caused by a black yeast, Phaeoannellomyces werneckii. It is mainly seen in the tropics but can present in Europe and the USA. The main differential diagnosis is an acral melanoma as it presents as a flat pigmented mark on the hands or feet. If the lesion is scraped with a glass slide or scalpel, it can be shown to be scaly. Lesions are usually solitary. The presence of pigmented hyphae in skin scrapings is typical. Tinea nigra responds to a variety of treatments including Whitfield’s ointment and azole creams. Topical butenafine has also been used with success.
References
Anaissie EJ, McGinnis MR, Pfaller MA. Clinical mycology. 2nd ed. London: Churchill Livingstone Elsevier; 2009.
Midgley G, Clayton YM, Hay RJ. Diagnosis in colour: medical mycology. London: Mosby-Wolfe; 1997.
Ameen M. Epidemiology of superficial fungal infections. Clin Dermatol. 2010;28:197–201.
Amer M, Taha M, Tossan Z, El-Garf A. The frequency of causative dermatophytes in Egypt. Int J Dermatol. 1981;20:431–4.
Bhardway G, Hajini GH, Khan IA, et al. Dermatophytosis in Kashmir, India. Mykosen. 1987;30:135–8.
Karaoui R, Selim M, Mousa A. Incidence of dermatophytosis in Kuwait. Sabouraudia. 1979;17:131–7.
Howell SA, Clayton YM, Phan QG, Noble WC. Tinea pedis: the relationship between symptoms and host characteristics. Microbiol Ecol Health Dis. 1988;1:131–8.
Leyden JJ, Kligman AM. Interdigital athletes foot: the interaction of dermatophytes and residual bacteria. Arch Dermatol. 1978;114:1466–72.
Ilkit M, Ali Saracli M, Kurdak H, Turac-Bicer A, Yuksel T, Karakas M, Schuenemann E, Abdel-Rahman SM. Clonal outbreak of Trichophyton tonsurans tinea capitis gladiatorum among wrestlers in Adana. Turkey Med Mycol. 2010;48:480–5.
Brasch J. Current knowledge of host response in human tinea. Mycoses. 2009;52:304–11.
Grumbt M, Monod M, Staib P. Genetic advances in dermatophytes. FEMS Microbiol Lett. 2011;320:79–86.
Lanternier F, Pathan S, Vincent QB, et al. Deep dermatophytosis and inherited CARD9 deficiency. N Engl J Med. 2013;369:1704–14.
Al-Sogair SM, Moawad MK, Al-Humaidan YM. Fungal infection as a cause of skin disease in the Eastern Province of Saudi Arabia: tinea pedis and tinea manuum. Mycoses. 1991;34:339–44.
Hay RJ, Reid S, Talwat E, MacNamara K. Endemic tinea imbricata: a study on Goodenough Island, PNG. Trans R Soc Trop Med. 1984;78:246–51.
Hay RJ. Fungal infections. Clin Dermatol. 2006;24:201–12.
Pernicario C, Peters MS. Tinea faciale mimicking seborrheic dermatitis in a patient with AIDS. N Engl J Med. 1986;314:315–6.
Gräser Y, Czaika V, Ohst T. Diagnostic PCR of dermatophytes – an overview. J Dtsch Dermatol Ges. 2012;10:721–6.
Gupta AK, Sauder DN, Shear NH. Antifungal agents: an overview. J Am Acad Dermatol. 1994;30(Part I):677–98. (Part II):911–933.
Crawford F, Hollis S. Topical treatments for fungal infections of the skin and nails of the foot. Cochrane Database Syst Rev. 2007;(3):CD001434. doi: 10.1002/14651858.CD001434.pub2.
Rotta I, Ziegelmann PK, Otuki MF, et al. Efficacy of topical antifungals in the treatment of dermatophytosis: a mixed-treatment comparison meta-analysis involving 14 treatments. JAMA Dermatol. 2013;149:341–9.
Bell-Syer SE, Khan SM, Torgerson DJ. Oral treatments for fungal infections of the skin of the foot. Cochrane Database Syst Rev. 2012(10):CD003584. doi: 10.1002/14651858.CD003584.pub.
Weinberg JM. Increasing patient adherence in antifungal infection treatment. J Clin Aesthet Dermatol. 2009;2:38–42.
Veraldi S, Persico MC, Schianchi R. Isoconazole nitrate vs isoconazole nitrate and diflucortolone valerate in the treatment of tinea inguinalis: results of a multicenter retrospective study. J Drugs Dermatol. 2012;11:e70–3.
Jerajani H, Janaki C, Kumar S, Phiske M. Comparative assessment of the efficacy and safety of sertaconazole (2%) cream versus terbinafine cream (1%) versus luliconazole (1%) cream in patients with dermatophytoses: a pilot study. Indian J Dermatol. 2013;58:34–8.
Ramam M, Prasad HR, Manchanda Y, Khaitan BK, Banerjee U, Mukhopadhyaya A, Shetty R, Gogtay JA. Randomised controlled trial of topical butenafine in tinea cruris and tinea corporis Indian. J Dermatol Venereol Leprol. 2003;69:154–8.
Gupta AK, Bluhm R. Ciclopirox (Loprox) gel for superficial fungal infections. Skin Therapy Lett. 2004;9:4–5.
Bakos L, Brito AC, Castro LC, Gontijo B, Lowy G, Reis CM, Ribeiro AM, Souza FH, Villar Mdo L, Zaitz C. Open clinical study of the efficacy and safety of terbinafine cream 1% in children with tinea corporis and tinea cruris. Pediatr Infect Dis J. 1997;16:545–8.
Borelli C, Klövekorn G, Ernst TM, Bödeker RH, Korting HC, Neumeister C. Comparative study of 2% sertaconazole solution and cream formulations in patients with tinea corporis, tinea pedis interdigitalis, or a corresponding candidosis. Am J Clin Dermatol. 2007;8:371–8.
Greer DL, Weiss J, Rodriguez DA, Hebert AA, Swinehart JM. A randomized trial to assess once-daily topical treatment of tinea corporis with butenafine, a new antifungal agent. J Am Acad Dermatol. 1997;37:231–5.
Gupta AK, Einarson TR, Summerbell RC, Shear NH. An overview of topical antifungal therapy in dermatomycoses. A North American perspective. Drugs. 1998;55:645–74.
Bonifaz A, Saúl A. Comparative study between terbinafine 1% emulsion-gel versus ketoconazole 2% cream in tinea cruris and tinea corporis. Eur J Dermatol. 2000;10:107–9.
Budimulja U, Bramono K, Urip KS, Basuki S, Widodo G, Rapatz G, Paul C. Once daily treatment with terbinafine 1% cream (Lamisil) for one week is effective in the treatment of tinea corporis and cruris. A placebo-controlled study. Mycoses. 2001;44:300–6.
Plaum S, Verma A, Fleischer Jr AB, Olayinka B, Hardas B. Detection and relevance of naftifine hydrochloride in the stratum corneum up to four weeks following the last application of naftifine cream and gel, 2%. J Drugs Dermatol. 2013;12:1004–8.
Tanuma H, Doi M, Ohta Y, Abe M, Kume H, Mukai H, Katsuoka K. Butenafine hydrochloride (Mentax) cream for the treatment of hyperkeratotic type tinea pedis and its transfer into the horny layer, with or without concomitant application of 20% urea ointment (Keratinamin). Mycoses. 2001;44:287–99.
Kikuchi I, Tanuma H, Morimoto K, Kawana S. Usefulness and pharmacokinetic study of oral terbinafine for hyperkeratotic-type tinea pedis. Mycoses. 2008;51:523–31.
Elewski BE, Haley HR, Robbins CM. The use of 40% urea cream in the treatment of moccasin tinea pedis. Cutis. 2004;73:355–7.
Borelli C, Korting HC, Bödeker RH, Neumeister C. Safety and efficacy of sertaconazole nitrate cream 2% in the treatment of tinea pedis interdigitalis: a subgroup analysis. Cutis. 2010;85:107–11.
Rotta I, Sanchez A, Gonçalves PR, Otuki MF, Correr CJ. Efficacy and safety of topical antifungals in the treatment of dermatomycosis: a systematic review. Br J Dermatol. 2012;166:927–33.
Brown M, Evans C, Muddle A, Turner R, Lim S, Reed J, Traynor M. Efficacy, tolerability and consumer acceptability of terbinafine topical spray versus terbinafine topical solution: a phase IIa, randomised, observer-blind, comparative study. Am J Clin Dermatol. 2013;1:413–9.
Evans EG. Tinea pedis: clinical experience and efficacy of short treatment. Dermatology. 1997;194 Suppl 1:3–6.
Ortonne JP, Korting HC, Viguié-Vallanet C, Larnier C, Savaluny E. Efficacy and safety of a new single-dose terbinafine 1% formulation in patients with tinea pedis (athlete’s foot): a randomized, double-blind, placebo-controlled study. J Eur Acad Dermatol Venereol. 2006;20:1307–13.
Edwards JE. Candida species. In: Mandell GL, Bennett JE, Dolin R, editors. Principles and practice of infectious diseases. 5th ed. Philadelphia: Churchill Livingstone; 2014. In Press.
Odds FC. Candida and candidosis. London: Baillière Tindall; 1988.
Torssander J, Morfeldt-Mauson L, Biberfeld G, et al. Oral candida albicans in HIV infection. Scand J Infect. 1987;189:291–5.
Samaranayake LP, Yaacob HB. Classification of oral candidosis. In: Samaranayake LP, MacFarlane TW, editors. Oral candidosis. London: Wright; 1990. p. 15–21.
Khongkunthian P, Grote M, Isaratanan W. Oral manifestations in 45 HIV-positive children from Northern Thailand. J Oral Pathol Med. 2001;30:549–52.
Perheentupa J. Autoimmune polyendocrinopathy–candidiasis–ectodermal dystrophy. J Clin Endocrinol Metabol. 2006;91:2843–50.
Coleman R, Hay RJ. Chronic mucocutaneous candidosis associated with hypothyroidism: a distinct syndrome. Br J Dermatol. 1997;136:24–9.
Clayton YM, Knight AG. A clinical double blind trial of topical miconazole and clotrimazole against superficial fungal infection and erythrasma. Clin Exp Dermatol. 1976;1:225–9.
Subissi A, Monti D, Togni G, Mailland F. Ciclopirox: recent nonclinical and clinical data relevant to its use as a topical antimycotic agent. Drugs. 2010;70:2133–5.
Ellepola AN, Samaranayake LP. Oral candidal infections and antimycotics. Crit Rev Oral Biol Med. 2000;11:172–98.
Grant SM, Clissold SP. Fluconazole: a review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in superficial and systemic mycoses. Drugs. 1990;39:877–916.
Grant SM, Clissold SP. Itraconazole: a review of its pharmacodynamic and pharmacokinetic properties and therapeutic use in superficial and systemic mycoses. Drugs. 1989;37:310–44.
Sun J, Qi C, Lafleur MD, Qi QG. Fluconazole susceptibility and genotypic heterogeneity of oral Candida albicans colonies from the patients with cancer receiving chemotherapy in China. Int J Oral Sci. 2009;1:156–62.
Detels R, Tarwater P, Phair JP, et al. Effectiveness of potent antiretroviral therapies on the incidence of opportunistic infections before and after AIDS diagnosis. AIDS. 2001;15:347–55.
Ianas V, Matthias KR, Klotz SA. Role of posaconazole in the treatment of oropharyngeal candidiasis. Infect Drug Resist. 2010;3:45–51.
Gligorov J, Bastit L, Gervais H, Henni M, Kahila W, Lepille D, Luporsi E, Sasso G, Varette C, Azria D, Candidoscope Study Group. Prevalence and treatment management of oropharyngeal candidiasis in cancer patients: results of the French CANDIDOSCOPE study. Int J Radiat Oncol Biol Phys. 2011;80:532–9.
Sganga G, Pepe G, Cozza V, Nure E, Lirosi MC, Frongillo F, Grossi U, Bianco G, Agnes S. Anidulafungin--a new therapeutic option for Candida infections in liver transplantation. Transplant Proc. 2012;44:1982–5.
Bensadoun RJ, Daoud J, El Gueddari B, Bastit L, Gourmet R, Rosikon A, Allavena C, Céruse P, Calais G, Attali P. Comparison of the efficacy and safety of miconazole 50-mg mucoadhesive buccal tablets with miconazole 500-mg gel in the treatment of oropharyngeal candidiasis: a prospective, randomized, single-blind, multicenter, comparative, phase III trial in patients treated with radiotherapy for head and neck cancer. Cancer. 2008;112:204–11.
Skupien JA, Valentini F, Boscato N, Pereira-Cenci T. Prevention and treatment of Candida colonization on denture liners: a systematic review. J Prosthet Dent. 2013;110:356–62.
Pitsouni E, Iavazzo C, Falagas ME. Itraconazole vs fluconazole for the treatment of uncomplicated acute vaginal and vulvovaginal candidiasis in nonpregnant women: a metaanalysis of randomized controlled trials. Am J Obstet Gynecol. 2008;198:153–60.
Beikert FC, Le MT, Koeninger A, Technau K, Clad A. Recurrent vulvovaginal candidosis: focus on the vulva. Mycoses. 2011;54:e807–10.
Hay RJ, Moore MK. Clinical features of superficial fungal infections caused by Hendersonula toruloidea and Scytalidium hyalinum. Br J Dermatol. 1984;110:677–83.
Machouart M, Menir P, Helenon R, Quist D, Desbois N. Scytalidium and scytalidiosis: what’s new in 2012? J Mycol Med. 2013;23:40–6.
Midgley G. The lipophilic yeasts: state of the art. Med Mycol. 2000;38 Suppl 1:9–16.
Crespo Erchiga V, Delgado FV. Malassezia species in skin diseases. Curr Opin Infect Dis. 2002;15:133–42.
Magiatis P, Pappas P, Gaitanis G, et al. Malassezia yeasts produce a collection of exceptionally potent activators of the Ah (dioxin) receptor detected in diseased human skin. J Invest Dermatol. 2013;133:2023–30.
Budimulja U, Paul C. One-week terbinafine 1% solution in pityriasis versicolor: twice-daily application is more effective than once-daily. J Dermatolog Treat. 2002;13:39–40.
Abdul Bari MA. Comparison of superficial mycosis treatment using Butenafine and Bifonazole nitrate clinical efficacy. Glob J Health Sci. 2012;5:150–4.
Gold MH, Bridges T, Avakian E, Plaum S, Pappert EJ, Fleischer Jr AB, Hardas B. An open-label study of naftifine hydrochloride 1% gel in the treatment of tinea versicolor. Skinmed. 2011;9:283–6.
Shi TW, Ren XK, Yu HX, Tang YB. Roles of adapalene in the treatment of pityriasis versicolor. Dermatology. 2012;224:184–8.
Hu SW. Bigby M Pityriasis versicolor: a systematic review of interventions. Arch Dermatol. 2010;146:1132–40.
Di Fonzo EM, Martini P, Mazzatenta C, Lotti L, Alvino S. Comparative efficacy and tolerability of Ketomousse (ketoconazole foam 1%) and ketoconazole cream 2% in the treatment of pityriasis versicolor: results of a prospective, multicentre, randomised study. Mycoses. 2008;51:532–5.
Hull CA, Johnson SM. A double-blind comparative study of sodium sulfacetamide lotion 10% versus selenium sulfide lotion 2.5% in the treatment of pityriasis (tinea) versicolor. Cutis. 2004;73:425–9.
Farschian M, Yaghoobi R, Samadi K. Fluconazole versus ketoconazole in the treatment of tinea versicolor. J Dermatolog Treat. 2002;13:73–6.
Naldi L. Seborrhoeic dermatitis. Clin Evid (Online). 2010;2010. pii:1713.
Adam BAT, Soo-Hoo TS, Chong KC. Black piedra in West Malaysia. Austr J Dermatol. 1977;18:45–7.
Rossetto AL, Cruz RC. Tinea nigra: successful treatment with topical butenafine. An Bras Dermatol. 2012;87:939–41.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Hay, R.J. (2016). Fungal Infections of the Skin. In: Ólafsson, J., Hay, R. (eds) Antibiotic and Antifungal Therapies in Dermatology. Springer, Cham. https://doi.org/10.1007/978-3-319-39424-4_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-39424-4_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-39422-0
Online ISBN: 978-3-319-39424-4
eBook Packages: MedicineMedicine (R0)