
Abstract
In this chapter we define pigmented lesions and their differences between melanocytic lesions. Physicians are continuously consulted regarding tumors or tumor-like lesions of the skin, because of their high frequency and the public concern regarding skin cancer. Furthermore, their importance lies predominantly in the cosmetic defect they may create or in their occasional association with systemic disease. Considering these facts, it is important establish their types, origins, features, differences, and instruments for diagnosis and treatment.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Pigmented lesions
- Melanocytic nevi
- Skin tumors
- Congenital melanocytic nevi
- Halo nevus
- Nevus spilus
- Becker’s nevus
- Freckles
- Lentigines
- Mongolian spots
- Blue nevi
- Spitz nevus
- Reed tumor
- Recurrent nevus
- Atypical nevus
Introduction
Pigmented moles and nevi are the most common neoplasms found in humans [1]. The incidence of melanocytic nevi in newborns is slightly more than 1% [2]. The incidence increases in infancy and adulthood, with a peak at puberty and adolescence. The size and pigmentation of these lesions also increase during adolescence, pregnancy, or after estrogen and corticosteroid therapy. Between the second and third decades of life, most Caucasians acquire their maximum number of lesions, and later in life most lesions tend to fade and eventually disappear.
Skin tumors can be differentiated into several groups: epidermal surface; epidermal appendages; fibrous, neural, vascular, fatty, muscular, and osseous tissues; melanocytic; and malignant. The term nevus refers to a circumscribed congenital abnormality of any type present at birth. When this term is used, it is important to include a qualifying adjective (epidermal, melanocytic, pigmented, vascular) to specify the particular cell of origin. Being in common use this term is also used in a loose manner to refer to a benign tumor of pigmented cells [1].
In contrast, moles are pigmented cutaneous lesions not present at birth that are apparently hereditarily predetermined. In general, moles appear during childhood and adolescence and are flat or slightly elevated. In adulthood they tend to be polypoid or dome-shaped, sessile, or papillomatous [1].
Pigmented lesions may comprise melanocytes or nevus cells. Both are of neural origin. A melanocyte is a dendritic cell that produces melanin and transfers it to the keratinocytes and hair cells, supplying the pigment to skin and hair. It originates in the neural crest and early in fetal life it migrates with the nerves to the skin. Many types of skin lesions may appear because of the melanocytic cells remaining in the dermis after birth, such as Mongolian spots, blue nevi, and the nevi of Ota and Ito [1].
Theories suggest that nevus cells arise from a bipotential precursor cell that develops into a melanoblastic or schwannian nevoblast. In this theory, the nevoblasts develop into epidermal nevus cells that give rise to the junctional and compound nevi. In addition, the schwannian nevoblasts develop into neural nevi cells and intradermal nevi [3]. In the most popular theory, nevus cells have a dual derivation and develop from the melanocytes in the epidermis and Schwann cells of the neural sheath [4]. A line of Schwann cells in the peripheral nerves appear to form a pathway between the central nervous system and the skin. These cells migrate to the dermis and give rise to a number of dermal tumors. Nevus cells, therefore, may locate at the dermal–epidermal junction (junction nevi), within the dermis (intradermal nevi), or be a combination of both (compound nevi) [1].
In the clinical evaluation the most important step is to differentiate the pigmented lesions from others. Using this approach it is often difficult to establish the melanocytic origin. Lesions such as basocellular carcinoma or seborrheic keratosis sometimes require better knowledge about other methods of evaluation, such as dermoscopy and pathology. Although dermoscopy and confocal microscopy are discussed in detail in a specific chapter elsewhere in this book, the description of lesions in this chapter some mentions details about these instruments. Some structures described in dermoscopy, such as aggregated globules, typical pigmented network, pseudonetwork, branched streaks, and parallel pattern, are the most important features for the diagnosis of benign melanocytic lesions [5]. Pathology is the gold-standard method of diagnosis to differentiate melanocytic from nonmelanocytic lesions, and anatomopathologic characteristics for each lesion will be described. The use of immunohistochemistry as a complementary method of diagnosis can improve this evaluation.
Nevocellular or Common Pigmented Nevi
Concepts
Nevocellular or pigmented nevi are lesions comprising nevus cells. Based on the location of the nevus cells, they are subdivided and described as junctional, intradermal, or compound lesions. Intradermal moles and nevi only have nests cells in the dermis. In junctional nevi, nevus cell nests are confined to the dermal–epidermal junction, and compound nevi have nevus cells nests in both locations.
Clinical Presentation and Diagnosis
Pigmented nevi have a wide range of clinical appearances and locations. The prevalence varies with age, race, and perhaps genetic and environmental factors. Few nevi are present at birth or childhood; they progressively increase in number, reaching a peak at the third and fourth decades of life, and then disappear with age. The most important factors related to number, development, and growth of nevi are skin color, race, genetic and familial occurrence, sun exposure, systemic immunosuppression, pregnancy, and hormonal diseases [6].
Pigmented nevi are usually well circumscribed, round or ovoid, regular and symmetric with a size ranging between 2 and 6 mm. They may occur anywhere on the skin surface (Fig. 60.1) and vary from flat to slightly elevated or dome shaped, nodular, verrucous, polypoid, or papillomatous. Junctional nevi are commonly hairless macules with color ranging from light to dark brown or brownish black. Most of them are circular, elliptical, or oval with few variations in colors and shapes. They are more common in children and located on palms, soles, and genitalia [1]. Compound nevi are more common in older children and adults, tend to be elevated with shades of brown, and may have coarse hairs within the lesion. In adolescence they frequently tend to increase in thickness and pigmentation. Intradermal nevi are seen most frequently in adults after the third decade of life and tend to fade with maturation, when nevus cells are often destroyed and replaced by fibrous or fatty tissue. They are usually dome shaped, sessile, or pedunculated and range in size from a few millimeters to 1 cm or more. The color varies from nonpigmented to brown or black [1].

Melanocytic nevi
Depending of the characteristics of the nevi, sometimes it may be very difficult to distinguish them from other lesions such as seborrheic keratosis, dermatofibromas, and neurofibromas. The most important differential diagnoses are dysplastic nevi and melanoma. Common nevi usually appear to be smaller and show clinical characteristics such as symmetry, regularity in shape, and well-defined borders. Furthermore, colors such as red, blue, gray, and black are more common in dysplastic nevi and melanomas.
Congenital Melanocytic Nevi
Concepts
Congenital melanocytic nevi are moles present at birth. They consist of intraepidermal, dermal, or both benign melanocytic proliferations with a wide range of sizes, locations, and clinical appearances. Although it has been suggested that the increased incidence of malignant melanoma in large nevi may be related to the increased number of cells, studies suggest that small congenital nevi also have an increased risk of malignant degeneration [7]. Small congenital nevi (less than 1.5 cm in diameter), occur in 1% of all newborns and have an estimated lifetime risk of developing melanoma of 2.6–4.9% [8]. The risk of developing melanoma in medium-sized congenital nevi (measuring 1.5–20 cm in diameter) is uncertain; and large or giant congenital pigmented nevi, measuring greater than 20 cm in diameter, are believed to have 6.3% lifetime risk for developing malignant melanoma [7, 9].
Clinical Presentation and Diagnosis
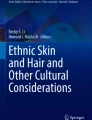
Small and medium-sized congenital nevi usually are oval or round, flat, pale tan to light brown macules or papules. Others are well-circumscribed lesions with mottled freckling. With time they become elevated, and coarse dark brown hairs may or not become prominent. Giant nevi frequently lie in the distribution of a dermatome and vary in size. Furthermore, they may cover limbs or extensive areas of trunk (Fig. 60.2). Their color ranges from dark brown to black and over 95% have a hairy component consisting of large coarse terminal hairs [1]. It is common to also observe a verrucous or papillomatous surface and an irregular margin. Almost invariably satellite nevi appear at the periphery of the lesion, and numerous other pigmented nevi coexist elsewhere on the body. Giant hairy nevi, particularly those on the scalp and neck, may be associated with leptomeningeal melanocytosis and neurologic disorders such as epilepsy or other focal neurologic abnormalities. Those that overlie the vertebral column may be associated with spina bifida or meningomyelocele [1].

Giant melanocytic nevi in arm and hand
Characteristically dermoscopy demonstrates a target network, focal thickening of network lines, target globules, skin furrow hypopigmentation, focal hypopigmentation, hair follicles, perifollicular hypopigmentation, vessels, and target vessels.
Halo Nevus
Concepts and Clinical Presentation
Halo nevus (Sutton’s nevus or leukoderma acquisitum centrifugum) consists of a single or multiple pigmented skin lesion centrally placed surrounded by a 1- to 5-mm halo of depigmentation (Fig. 60.3). This common disorder occurs between 3 and 45 years of age, usually with onset in late adolescence [1]. Compound and intradermal nevi are the most frequently associated melanocytic lesions. However, it may also occur with blue nevi, neuromas, neurofibromas, melanomas, metastatic lesions, seborrheic keratoses, angiomas, molluscum contagiosum, warts, basal cell carcinoma, and congenital nevi. The cause appears to be related to an immunologic destruction of melanocytes and nevus cells. About 30% of patients with halo nevi have a tendency to vitiligo. It may occur on almost any cutaneous surface and is usually asymptomatic. The natural course tends to a spontaneous resolution and disappearance of the central lesion. Later, complete resolution leads to repigmentation of the site [1].

Halo nevi
Diagnosis
Dermoscopy reveals in the center of these lesions usually a regular pigmented network, dots and globules, an amorphous area, or a pseudonetwork pattern when lesions are located on the face. During involution, these structures disappear. The histologic examination reveals reduction or absence of melanin and dense inflammatory infiltrate around the central lesion.
Therapeutic Approach
The prognosis for benign lesions is excellent, but attention must be directed to the rare cases in which a malignant melanoma or metastatic lesions of this tumor may be the affected lesion [1]. The correct management consists in the clinical and the dermatoscopic observation of central lesion. With benign characteristics (color, regularity, shape, development) and its permanence over the consultations, the lesion may be observed until it has resolved. Lesions with unusual appearance and evolution require surgical excision of the central tumor and its surrounding halo [1].
Nevus Spilus
Concepts and Clinical Presentation
Nevus spilus (speckled lentiginous nevus, zosteriform lentiginous nevus) is a solitary, flat, brown patch dotted by smaller dark brown to blackish brown freckle-like areas of pigmentation ranging from 1 to 6 mm of diameter (Fig. 60.4). These dots vary from junctional and compound nevi to Spitz and blue nevi. Nevus spilus may vary from 1 to 20 cm in diameter and appear on any area of the face, trunk, or extremities without relation to sun exposure. Larger lesions may be unilateral or segmental, or follow Blaschko lines affecting substantial parts of the skin (a limb, trunk). It is a common disorder, usually presenting at birth, although it may appear at any age and persists indefinitely. Males and females are equally affected. Nevus spilus should be considered with the same potential for neoplastic change as any other pigmented nevus.

Nevus spilus
Diagnosis
The dermoscopy presents a thin and bright reticular background and outbreaks with pigmented network and aggregated globules.
Therapeutic Approach
There are reports about dysplastic transformation or melanomas appearing from these lesions. For this reason, periodic clinical and photographic observation is recommended. In addition, biopsy and surgical excision is necessary for lesions with typical dysplasia or a clearly documented onset [10].
Becker’s Nevus
Concepts
Becker’s nevus (pigmented hairy nevus or nevus spilus tardus) may begin in childhood or shortly after puberty. It is six times more common in males than in females and may occur in all races [11]. The pathogenesis is unclear, but the clinical features seen in individuals with this disorder suggest a localized increase in androgen sensitivity. Furthermore, a familial occurrence seen in some patients demonstrates a genetic influence [12]. The association with other abnormalities (such as unilateral breast, areolar hypoplasia, pectus carinatum, spina bifida) suggests an organoid nevus, as a part of the spectrum of epidermal nevi and the epidermal nevus syndrome [13]. There are no nevus cells and no increases in the number of melanocytes; therefore, malignant transformation does not occur.
Clinical Presentation and Diagnosis
Becker’s nevus is a relatively frequent and asymptomatic disorder. Usually it begins as a grayish brown pigmentation, unilateral on the chest, back, or upper arm, that spreads in an irregular format until it reaches an area 10–15 cm in diameter (Fig. 60.5), often surrounded by islands of blotchy pigmentation. It has been reported on other areas of the trunk, face, neck wrist, buttocks, and shins. After 1–2 years coarse hairs appear in the region. The hairy area does not necessarily coincide with the pigmented area. The hyperpigmentation and hypertrichosis tend to persist for life. Acneiform lesions have been described in association with Becker’s nevus.

Becker’s nevus on the back
Histopathologic features reveal epidermal thickening, elongation of the rete ridges, and hyperpigmentation of the basal layer. Network, focal hypopigmentation, skin furrow hypopigmentation, hair follicles, perifollicular hypopigmentation, and vessels are the main dermoscopic features. Differential diagnosis includes congenital melanocytic nevus, plexiform neurofibroma, and smooth muscle hamartoma.
Therapeutic Approach
The treatment of this disorder is purely cosmetic (electrolysis, depilation, camouflage), and therapy with lasers have also been described (Q-switched, Nd:YAG) [14].
Freckles
Concepts, Clinical Presentation, and Diagnosis
Freckles (ephelides) are red or light brown circumscribed macules, round, oval, or irregular, usually less than 5 mm in diameter. These lesions appear in early childhood, generally between 2 and 4 years of age, especially on sun-exposed areas of the skin (face, shoulders, upper back), and tend to fade during the winter and in adult life (Fig. 60.6) [1]. It appears to be inherited as an autosomal dominant trait linked with a tendency to fair skin and red or reddish-brown hair. There is seasonal variation in their appearance. They become darker and more confluent during the summer and are smaller and lighter during the winter [1]. The sun increases the melanogenesis and the transport of melanosomes to keratinocytes. Freckles do not have tendency to malignant transformation.

Freckles
Histopathologic features include increased melanin pigmentation of the basal layer without an increase in the number of melanocytes, which are more arborized and reactive to dopa than adjacent skin and also contain more melanosomes [1].
Therapeutic Approach
The treatment is based on avoidance of sun exposure and covering makeup. Sunscreens permit a more uniform tan whereby freckling is less pronounced. Peeling, cryotherapy, and hydroquinone use may be partially effective. Laser therapy also is effective.
Lentigines
Lentigines are seen in all races and equally in both sexes. They are small, tan, dark brown or black, flat, oval, or circular lesions. They usually begin in childhood and may increase in number during adult life. They vary from 1 to 5 mm in diameter and may occur on any cutaneous surface or, occasionally, on the mucous membrane or conjunctiva of the eyes. The pigmentation is uniform and darker than that seen in ephelides, and the color is unaffected by sun exposure [1]. They may occur as a single lesion or be multiple. Generalized or multiple lentigines can be an isolated phenomenon with no disease involved, present at birth or later in childhood or adult life. However, lentigines may be seen genetic diseases with other multiple clinical manifestations, such as leopard syndrome, Peutz–Jeghers syndrome.
In mucous membranes lentigines often have nonhomogeneous irregular borders, with areas lacking pigmentation and varying in size and number. These lesions may grow slowly during months or years and also present with or without variations in pigmentation.
Solar Lentigines (Senile Lentigines, Liver Spots)
Concepts and Clinical Presentation
Solar lentigines are multiple light or dark brown macules related to solar explosion. They usually appear in the Caucasian population older than 60 years and are located on the forearms, face, chest, neck, and dorsal area of the hands (Fig. 60.7). However, they may also be observed in younger adults with heavy solar exposure. The shape of these lesions is well circumscribed or confluent, oval to round, varying from 3 mm to 2 cm in diameter. They may slowly disappear with sun protection. Solar lentigines are an independent risk factor for the development of melanoma.

Solar lentigines
Diagnosis
For the evaluation of these lesions it may be necessary to use Wood’s lamp, dermoscopy, and histopathologic examination. Differential diagnosis includes junctional and compound melanocytic nevi, ephelides, actinic keratosis, pigmented actinic keratosis, seborrheic keratosis, hemangioma, cutaneous hemorrhage, and cutaneous melanoma.
Dermoscopy demonstrates a faint pigmented network, fingerprint structures, or uniform pigmentation.
Histopathologic features include an increase in the number of melanocytes just above the basal layer, and an increase of melanization of the keratinocytes of the basal layer. The etiology is unknown but seems to be related to genetic modifications of the neural crest.
Therapeutic Approach
Treatment other than for cosmetic purposes is ordinarily not indicated. For senile lentigines, it is important to monitor for melanoma or nonmelanoma cutaneous cancer. Clarifying agents are not effective, although cryotherapy and laser surgery may help. Prevention with sun protection is necessary [1, 6].
Café-au-Lait Spots
Concepts, Clinical Presentation, and Diagnosis
Café-au-lait spots are large flat lesions, round or oval, of light brown to dark brown pigmentation, found in 10–20% of normal individuals. They may occur anywhere on the skin and are frequently present at birth. In addition, they may be unique or multiple, often increasing in number and size with age. They vary from 1.5 cm or less to 15–20 cm in diameter (Fig. 60.8). The average size varies from 2 to 5 cm in adults. These macules may be a sign of neurofibromatosis and may be associated with other neurocutaneous disease, for example McCune–Albright syndrome. There is no risk of malignancy. Multiple lesions are rare in the normal population and should alert the physician to the possibility of an associated disease [1].

Café-au-lait spot on the back
Café-au-lait spots occur in 90% of patients with neurofibromatosis. Characteristically, six or more lesions greater than 1.5 cm in diameter may be observed in this disease. Smaller spots in the axilla, called axillary freckling, may also serve as a valuable diagnostic sign of neurofibromatosis (Crowe’s sign). In addition there is an increased incidence of café-au-lait spots in patients with tuberous sclerosis, epidermal nevus syndrome, Bloom’s syndrome, Sylver’s syndrome, basal cell nevus syndrome, Gaucher’s disease, ataxia-telangiectasia, and Turner’s syndrome [6].
Histopathologic examination reveals an increase in pigment in the basal layer of the epidermis. Ultrastructural examination may reveal giant pigmented granules in the keratinocytes and melanocytes, particularly in those of individuals with neurofibromatosis [1]. The number of melanocytes per unit area in patients with neurofibromatosis may be increased, decreased, or equal to that in normal-appearing surrounding skin [15]. Differential diagnosis includes nevus spilus, Becker’s melanosis, mastocytoma, postinflammatory hyperpigmentation, acquired melanocytic nevus, congenital nevus, and lentigines.
Therapeutic Approach
Treatment is unnecessary [1]. The results with hydroquinone and laser therapy are poor with a high risk of hyperpigmentation. Camouflage can help for cosmetic appearance.
Dermal Melanocytic Lesions
Mongolian Spots
Concepts, Clinical Presentation, and Diagnosis
Mongolian spots are flat dark brown to gray or blue-black large macular lesions, poorly circumscribed and reaching more than 20 cm. They may present as a single or multiple lesions, usually located over the lumbosacral area, buttocks, lower limbs, and shoulders of normal infants (Fig. 60.9). It may be seen in all races, especially in blacks, Asians, Indians, Hispanics, and less frequently in Caucasians (9.8%) [1]. The spots develop in utero, present at birth, in both sexes, and often fade during the first 1 or 2 years of life [1]. Occasionally they persists into adulthood, although these lesions usually disappear by 7–13 years of age [16].

Mongolian spot
The color seen is a result of the presence of melanocytes located deep in the dermis, probably as a result of an arrest during their embryonic migration from neural crest to the epidermis where they suffer cellular death. The blue color depends on the Tyndall effect (a phenomenon whereby light passing through skin is scattered as it strikes particles of melanin). Colors of shorter wavelengths (blue, indigo, and violet) are scattered to the side and backward to the skin surface, thus creating the blue-black or slate-gray discoloration [1].
Clinical morphology aids the differential diagnosis with nevus of Ota and nevus de Ito, maculous blue nevus, trauma, and hemangiomas. When in doubt, the diagnosis may be confirmed by histopathologic examination of lesions. Histopathology shows the presence of collections of elongated, slender, spindle-shaped, dopa-positive melanocytes that run in parallel to the skin surface, deep within the dermis or around the cutaneous appendages.
Therapeutic Approach
Treatment is unnecessary. Cosmetic camouflage and laser therapy may help [1, 6].
Nevus of Ota
Concepts, Clinical Presentation, and Diagnosis
Nevus of Ota (nevus fuscoceruleus ophthalmomaxillaris) represents a bluish gray discoloration of the skin of the face, usually unilateral. Size and shape may vary (round, oval, serrated) and the lesion is located on the skin supplied by the first and second divisions of the trigeminal nerve, especially the periorbital region, the forehead, nose, malar area, and temple (Fig. 60.10). In 5–15% of patients nevus of Ota may be bilateral, and in many cases the lips, palate, pharynx, eardrum, and nasal mucosa are involved. About two-thirds of patients have a patchy bluish discoloration of the sclera of the ipsilateral eye, occasionally also affecting the conjunctiva, cornea, retina, iris, and optic nerve. It may grow with time and generally persists throughout life (although some have been observed to fade over the course of years). Malignant transformation and sensorineural deafness are rare [1].

Nevus of Ota
Approximately 50% of lesions are congenital; the remainder appear during the second decade (puberty) or are associated with pregnancy. Most commonly seen in Asians and blacks, it has been described also in Caucasians. It is more commonly seen in females (80% occur in females) [1].
The characteristic color is due to the production of melanin from dendritic and elongated melanocytes located in dermis, especially in the upper-third portion, scattered among the collagen bundles.
Considering the colors, shapes, and histopathologic features, the nevus of Ito (nevus fuscoceruleus acromiodeltoideus), differs from nevus of Ota by its location. It tends to involve the shoulder, supraclavicular areas, sides of the neck, and the upper arm, scapular, and deltoid regions. It may occur alone or be seen in conjunction with the nevus of Ota.
Mongolian spots, blue nevus, facial melasma, nevus spilus, and vascular malformations are part of differential diagnosis.
Therapeutic Approach
Monitoring of glaucoma and ocular melanoma by the ophthalmologist is important. Cosmetic camouflage is necessary in many cases. Successful treatment has been obtained with laser ablation by Q-switched ruby, alexandrite, and Nd:YAG lasers [17, 20].
Blue Nevi
Concepts, Clinical Presentation, and Diagnosis
Blue nevi (blue nevi of Jadassohn–Tièche) usually are acquired in childhood and adolescence, although 25% appear in adult life. They are benign tumors constituted by dermal melanocytes. These lesions represent hamartomas that result from the arrested embryonal migration of melanocytes limited to the dermal–epidermal junction. Their color is the result of the Tyndall phenomenon. Blue nevi may be divided in two groups: common and cellular.
Common blue nevi are small, round or oval, dark blue or bluish black, smooth-surfaced and sharply circumscribed lesions (Fig. 60.11). In addition, they may be a slightly elevated dome-shaped nodule or plaque ranging from 2 to 10 mm in diameter. Usually isolated, they may occur on any part of the body. Areas of predilection include the buttocks, dorsal aspect of the hands and feet, scalp, and extensor surfaces of the forearms. Blue nevi usually remain unchanged and persist throughout life. Malignant degeneration of this type is rare. Dermoscopy of common blue nevi is characterized for its grayish blue or blackened blue homogeneous pigmentation [1].

Blue nevi in arm
Histopathologic examination reveals compactly arranged and elongated spindle-shaped, flattened, or fusiform melanocytes grouped in irregular bundles, mainly in the middle and lower third of the dermis. These cells have long dendritic processes, with their long axes parallel to the epidermis. Occasionally the melanocytes may extend to subcutaneous layer or epidermis. The amount of collagen is usually increased, giving a fibrous appearance [6].
Cellular blue nevi are less common and larger than common blue nevi, generally measuring more than 1 cm in diameter. They present as blue or grayish blue, smooth-surfaced nodules or plaques occasionally with an irregular surface. Cellular blue nevi appear in a relatively high incidence over the buttocks, sacrococcygeal areas, and dorsal aspect of hands and feet, although common blue nevi are five times more common. There is a low risk of malignant transformation, which should be suspected if the following features are observed: sudden increase in size with multinodular appearance, asymmetry, infiltrative changes, and ulceration. They are locally aggressive, more common on the scalp, and in about 5% may present with the risk of producing regional lymph node metastases. Except for the local involvement, patients may be asymptomatic for many years after the primary tumor excision [1].
Histopathology reveals nodular islands composed of densely packed, large, rounded, or spindle-shaped cells with variously shaped nuclei and abundant pale cytoplasm. Round islands of these melanocytes are often seen in the subcutaneous layer and may appear atypical with nuclear pleomorphism.
Traumatic tattoos, vascular lesions, primary melanoma and its metastasis, atypical nevi, dermatofibroma, pigmented basal cell carcinoma, apocrine hidrocystoma, nevi of Ota, hamartomas, and spindle cell nevus are part of the differential diagnosis of blue nevi.
Therapeutic Approach
The treatment for lesions of less than 1 cm diameter is conservative. Larger lesions with atypical characteristics, a multinodular or patch aspect, asymmetry, or undergoing any transformation should be considered for histopathologic examination. Many authors consider the treatment of choice for both types of blue nevus to be conservative surgical excision with careful histologic examination. Patients who have cellular blue nevi should be examined for the presence of regional lymphadenopathy [1].
Pigmented Lesions Important in the Differential Diagnosis of Melanoma (See Also Chap. 14)
Spitz Nevus
Concepts, Clinical Presentation, and Diagnosis
Spitz nevus (spindle cell nevus, spindle and epithelioid nevus) is a benign lesion of melanocytic origin that can occur anywhere on the cutaneous surface, more often on the face, usually the cheek of children and adolescents. It is believed that about 1% of lesions surgically removed from children exhibited histologic characteristics of Spitz nevus, in any age group and in both sexes. These lesions have certain histologic features that may resemble malignant melanoma and may be a cause of concern to physicians and pathologists [18]. No etiologic factors have been identified, but eruptive cases have been identified in immunosuppressed patients and pregnancy.
Clinically the lesions present as a smooth-surfaced, hairless, dome-shaped papule or nodule with a distinctive reddish brown color, usually single or less often multiple. Spitz nevi may vary in size from a few millimeters to several centimeters, usually ranging from 0.6 to 1 cm in diameter (Fig. 60.12). In some lesions, particularly those on the extremities, the reddish color is replaced by a mottled brown to tan or black appearance, often with a verrucous surface and an irregular margin [1]. Multiple or disseminated cases may be seen with hundreds of lesions of sudden onset, on any part of the body, with the exception of palms, soles, and mucous membranes. These cases tend to be polymorphic, more often in adults, with a possibility of spontaneous regression and no reported cases of malign transformation [1].

Spitz nevus
Atypical cases have one or more characteristics that differ from conventional lesions, such as larger size, asymmetry, ulceration, pagetoid dissemination, or high density of melanocytes in dermis.
The histologic pattern of this disorder appears to be a variant of the compound nevus. The nevus cells are pleomorphic and generally consist of spindle-shaped and, less frequently, polygon-shaped epithelioid cells. Multinucleated giant cells and mitotic figures complete the histopathologic features. This benign tumor can be differentiated from malignant melanoma by the presence of spindle and giant cells, and absence or sparseness of melanin, edema, and telangiectasia of the stroma and increased maturation of the tumor cells in the deeper aspect of the dermis. Important characteristics that aid the diagnosis are recognition that the cells are larger than those of common melanocytic nevi and the coalescent eosinophilic globules resembling colloid bodies (Kamino bodies), which are present in the basal layer above the tips of dermal papillae [1, 19, 20].
The differential diagnosis includes intradermal nevi, pyogenic granulomas, juvenile xanthogranulomas, hemangiomas, adnexal tumors, dermatofibromas, mastocytomas, and malignant melanomas.
Therapeutic Approach
There is controversy regarding the management of these lesions. Some authors take a conservative approach, because the histopathologic appearance of incompletely removed lesions or biopsied lesions that leave a slight residual cellular or vascular component may be misinterpreted as malignant melanoma. Total conservative surgical excision is frequently recommended. In addition, other authors recommend removal with at least 1 cm of margin for atypical lesions and a periodic evaluation every 6 or 12 months.
Reed Tumor
Concepts, Clinical Presentation, and Diagnosis
Reed tumor represents a pigmented form of Spitz nevus. They are less common than Spitz nevi and are seen especially in women of a mean age of 25 years. These lesions present with a mottled brown to tan or black appearance and are uniform in color, often with a verrucous surface and irregular margin (this lesion may easily be confused with a malignant melanoma). In addition, Reed tumors may be flat or slightly elevated in shape, usually measuring an average of 4 mm (variation at 1.5–10 mm), particularly on the extremities. Dermoscopy often demonstrates a dark central area without structures, with globules or pseudopodia on the periphery, symmetrically arranged (Fig. 60.13). Variations in this pattern are seen in atypical cases [1, 6].

Reed tumor
The differential diagnosis includes melanoma, atypical nevus, blue nevus, angiokeratoma, and pigmented basal cell carcinoma.
The principal histologic characteristics are ribbons of thin and uniform fusiform cells closely organized with granular melanin and streaky tissue slits. The nuclear appearance is homogeneous with subdued chromatin. The histopathologic examination is essential for the correct diagnosis [1, 6].
Therapeutic Approach
The natural evolution is unknown. The knowledge about the association of atypical variants with melanoma is evidence of this rare transformation. The recommended treatment is total surgical excision with free margins to avoid recurrence. The pathologic characteristics of Reed tumor are extremely difficult to distinguish from melanoma. When atypical characteristics are seen, surgical excision is recommended with margins between 5 and 10 mm and medical monitoring for 6 or 12 months [1, 6].
Recurrent Nevus
Concepts and Clinical Presentation
A recurrent or a persistent nevus is the development of a melanocytic lesion where a previous benign nevus was removed [21]. Many times it may clinically, dermoscopically, and histologically resemble melanoma, for which reason it has been called “pseudomelanoma.” However, many authors find this term confusing and misleading, since recurrent nevi are benign and should not be mistaken for recurrent melanomas.
Recurrent nevi occur after incomplete removal of a melanocytic nevus. It may be observed after shave biopsies, electrocoagulation, or laser therapy [21]. The occurrence of this phenomenon can be explained by the reminiscent melanocytes in the adnexal structures, which migrate into the regenerating epithelium [22, 23]. During the healing process and scar formation, these melanocytes may be stimulated to proliferate [21].
Clinically, recurrent nevi are characterized by dark brown to black pigment in the scar, often exhibiting bizarre forms [21, 24]. Lesions may also display asymmetry (Fig. 60.14) [21, 24]. Various reports have stated that when recurrence of pigmentation is confined to the scar, this is a sign of benignity, such as recurrent nevi. Usually pigmentation of recurrent nevi develops for a limited period and stabilizes, sometimes even fading over time [25].

Recurrent nevus
Recurrent nevi occur more frequently in females under the age of 40 years and in lesions excised on the back, followed by the abdomen and extremities [22, 26]. Usually the pigmentation recurs within 6 months after the initial procedure [22, 27]. The majority of recurrent nevi may be observed after removal of ordinary nevi, followed by dysplastic nevus [22, 26]. Additional studies have shown that in 23% of cases of recurrent nevi the primary lesion appeared to be completely removed in the histopathologic report [22] and that only 75% of recurrent nevi had previous positive margins [26].
The most important differential diagnosis with recurrent nevi is recurrent melanoma (Tables 60.1 and 60.2) [25]. With the objective of studying the diagnostic differences between these lesions, a multicenter study was conducted in 2014 [28]. The authors found that patients with recurrent melanoma had a longer time interval between the procedures (median 25 months), while recurrent nevi occurred more quickly (median 8 months) [28]. Also, to help differentiation between both entities, the study defined dermoscopic characteristics for recurrent nevi and recurrent melanomas. Recurrent nevi were characterized by radial lines, symmetry, and a centrifugal growth pattern. Meanwhile, recurrent melanomas showed eccentric pigmentation at the periphery, a chaotic and noncontinuous growth pattern, and pigmentation beyond the scar’s edge. In addition, it was found that recurrent melanomas may display a circular pattern; however, most lesions included in this subgroup were on the face, a possible confounder [28]. Also, authors found that the presence of globules and heterogeneous pigmentation were the strongest dermoscopic findings related to recurrent nevi, followed by irregular network and absence of streaks [28].
Another differential diagnosis to recurrent nevi is reactive pigmentation. This entity tends to extend perpendicular to the main axis of the scar, and shows a regular pigmented network and thin continuous streaks [29].
Three zones may be seen in histology: intraepidermal alterations that can be mistaken for melanoma, as a junctional melanocytic component with varying degrees of pigmentation; fibrotic scar tissue; and below this, the residual intradermal component of the melanocytic lesion may be seen [21]. It is possible to observe a histologic overlap with primary melanoma in some cases, especially when a retiform epidermis and atypical features are found, such as a confluent growth pattern, pagetoid spread, and cytologic spread [22].
Immunohistochemical analysis may be useful to help differentiate atypical recurrent nevi and melanoma. In recurrent nevi, labeling for gp100 (with HMB-45) is strong only in the junctional portion, while in melanomas it is found to be strong in both the junctional and deep dermal components [31]. Furthermore, tyrosinase and Ki-67 demonstrate a maturation pattern in recurrent nevi, whereby the strongest labeling is seen in the junctional component, with a progressive reduction throughout the dermis. The Ki-67 junctional proliferation rate is also found to be less than 5%. By contrast, melanoma expresses tyrosinase throughout the whole lesion and the proliferation rate is much higher [30].
Diagnosis
To confirm the exact diagnosis of a recurrent nevus and exclude the possibility of recurrent melanoma, it is recommended to review the original histopathologic slides [21]. The importance of analyzing the first original sections lies in the fact that in only 67% of cases is it possible to correctly predict the original melanocytic lesion [26].
Therapeutic Approach
In cases where there is no previous histopathologic diagnosis, excision and histopathologic examination are mandatory to rule out melanoma. With the confirmation of a benign nevus, no further treatment is necessary.
Whenever melanoma is suspected or the diagnosis is unclear, the lesion should be completely excised [21]. Partial biopsies may be problematic when trying to differentiate recurrent nevi from atypical melanocytic proliferations and melanoma. Cases in which biopsies were thought to represent recurrent nevi but the re-excised lesion showed unequivocal melanoma have been described [22].
Atypical Nevus
Concepts
Atypical nevi, also known as Clark nevi, are benign melanocytic lesions that may share clinical and dermoscopic features with melanoma [31]. To date, the correct terminology between atypical and dysplastic nevus has been controversial. Often the term “atypical nevus” is clinically used to describe potentially suspicious lesions, which could present with histologic dysplasia. However, there is not always a clinical and histologic correlation [32, 33]. Therefore, many authors encourage the use of the term “atypical nevi” in the clinical setting, while “dysplastic nevi” is used as a histologic description [21, 34].
In 1992, an expert panel organized by the NIH Consensus Development Conference proposed abandoning the term “dysplastic nevus” and reinforced the terms “atypical nevus” [35]. This approach was justified based on two common errors: viewing different grading steps of dysplasia as a progression toward melanoma or stating that dysplastic nevus would be a “premalignant lesion” [32]. Many have even advocated the term “Clark nevus” to honor its first descriptor, as referred below, and to reaffirm the idea that it is simply a nevus variant [32]. In addition, many also use the term “nevus with architectural disorder” [32].
The first description regarding atypical nevi and melanoma was introduced by Clark and coworkers in 1978, termed the B-K mole syndrome [36]. The letters B and K stood for the initials of the two affected families [36]. Later, Lynch et al. characterized the familiar atypical multiple mole melanoma syndrome (FAMMM), referring to patients with a similar phenotypic nevus in a melanoma-prone family [37]. In addition, Elder et al. [38] described the “dysplastic nevus syndrome” with familiar and sporadic variants. Later on, Rigel et al. [39] created a melanoma risk classification for patients with dysplastic nevus syndrome, according to their personal and family history of melanoma. Thus, both groups showed that there is a broad melanoma risk spectrum regarding this syndrome, ranging from isolated cases of individuals with only atypical moles to the description of FAMMM syndrome [40].
The exact prevalence of dysplastic nevus is unknown, because the majority of studies do not include histologic confirmation. Regarding the clinical classification, the estimated frequency of atypical nevi is 2–10% of the population [21, 41].
Diagnosis
Atypical nevi usually appear during puberty, although they may develop throughout life [32]. Often atypical nevi are located in intermittently sun-exposed areas, such as the trunk and extremities. However, they may also appear in sun protected areas [31].
Many clinical criteria for atypical nevi overlap with those of early melanomas [21]. Tucker et al. clinically defined atypical nevus characteristics: variable pigmentation, irregular or asymmetric outline, indistinct borders, diameter over 5 mm, and a macular component [42].
Analyzing dermoscopic aspects, Hoffman-Wellenhof et al. identified six patterns, including reticular, globular, homogeneous, reticuloglobular, reticular-homogeneous, and globular-homogeneous (Fig. 60.15). Additionally the distribution of pigmentation was classified into six groups: central hyperpigmentation or hypopigmentation, eccentric peripheral hyperpigmentation or hypopigmentation, and multifocal hyperpigmentation or hypopigmentation. Similarly to common nevi, the authors found that most individuals had one predominant type of atypical nevi, also known as the signature nevi. Moreover, it was observed that eccentric peripheral hyperpigmentation is a rare (7.5%) finding in atypical nevi and should be evaluated to rule out melanoma [43].

Dermoscopy of atypical nevus
Atypical nevi may be observed as isolated lesions or also can occur in the “atypical or dysplastic mole syndrome,” which presents a broad clinical spectrum. Patients may have atypical/dysplastic nevus with no personal or family history of melanoma, while others may present with FAMMM syndrome [31]. According to the NIH Consensus statement published in 1992, the diagnosis of FAMMM or dysplastic nevus syndrome requires: occurrence of melanoma in one or more first or second degree relatives; presence of a large quantity of nevi (>50), some of which are clinically atypical; and nevi with distinct histologic features [35]. Compared with the general population, FAMMM carriers have a 150-fold greater risk of developing melanoma.
Histologic criteria for classification of dysplastic nevus may be divided into architectural and cellular [21]. Regarding architectural aspects, atypical nevus may display irregular nests at the junctional zone, bridging (horizontal anastomosis) between these nests, and the “shoulder phenomenon,” which occurs when junctional nests extend beyond the dermal component [21]. Furthermore, lamellar or concentric fibroplasia (a dense extracellular matrix around the epidermal ridges) may be observed, as well as initial migration of single cell elements or nests through the epidermis [21]. At the cellular level, atypical melanocytes, nuclear polymorphism, and shift of the nucleus/plasma ratio may be seen [21].
In an attempt to standardize the histologic classification of dysplastic nevus, the World Health Organization enumerated major and minor criteria [44]. For establishment of the diagnosis it is necessary to have both major criteria and at least two minor criteria [44]. The major criterion is basilar proliferation of atypical melanocytes, which must extend at least three rete ridges beyond the dermal component and organization of this proliferation in a lentiginous or epithelioid-cell pattern. The minor criteria include the presence of lamellar fibrosis or concentric eosinophilic fibrosis, neovascularization, an inflammatory response, and the fusion of rete ridges [44].
There is controversy over whether dysplastic nevi may be melanoma precursors, as it is known that most do not progress to melanoma [21, 34]. Tsao et al. estimated the individual risk of a nevus (including a dysplastic nevus) transforming to melanoma is 1 in 10,000 during a lifetime [45]. In addition, only 20–30% of melanomas arise from nevi [46]. Of these nevus-derived melanomas, it appears that the incidence between common and dysplastic nevus is similar [47].
However, it is well established that atypical nevus is a phenotypic risk marker for melanoma [32]. The presence of atypical nevus, regardless of the total number of moles, increases the melanoma risk ten-fold compared with their absence [41].
Therapeutic Approach
Prophylactic excision of atypical nevi is not indicated, since there is lack of evidence that the procedure reduces melanoma risk [48, 49, 50]. Also, unnecessary excisions increase costs and morbidity. Atypical lesions should only be removed when there is doubt regarding its differential diagnosis with melanoma [34, 49]. As in common nevi, atypical nevi may be removed by several techniques such as elliptical resection, shaving, or cauterization. Whenever possible, full excision should be attempted, so that the whole lesion can be assessed histologically. Therefore, a narrow excisional biopsy with 1- to 3-mm margins beyond the clinically visible pigmentation is recommended, as well as a depth sufficient to avoid transection [34]. It is known that dysplastic nevus may demonstrate heterogeneous histopathology and that melanoma may be missed through a sampling error [34, 51]. When these techniques are not possible, it is acceptable to carry out incisional punch biopsy or shaving of a more suspicious dermoscopic area [34].
The necessity of re-excision of dysplastic nevus is very controversial and there are no strong and formal recommendations. Some physicians decide to re-excise to prevent recurrence and the pseudomelanoma phenomenon. However, greater consensus exists regarding re-excision of severely dysplastic nevus, independently of margins, because of the difficulty of distinguishing it from melanoma [49]. In 2014, a panel of specialists summarized the results of several studies and established management recommendations for atypical nevus/dysplastic nevus [52, 53]. This report, authors stated that: (1) mildly and moderately dysplastic nevus with clear margins do not need to be re-excised; (2) mildly dysplastic nevus with positive margins and without clinical recurrence may be observed; (3) moderately dysplastic nevus with positive margins and without clinical recurrence possibly may be observed, although there is a lack of more formal data to verify this recommendation; (4) in cases with severe dysplasia and positive margins, re-excision is recommended with a 2–5-mm clinical margin [52, 53].
The follow-up of patients with atypical nevus includes clinical and dermoscopic evaluation every 3–6 months, which can be spaced to semiannually or annually if lesions remain stable [54]. Patients who are at higher risk, such as those with multiple atypical lesions and personal or family history of melanoma, benefit from total body photography and digital dermoscopy [31, 54]. In addition, patients should be advised to perform self-examinations periodically and to use regular sun protection. In patients with dysplastic nevus syndrome or FAMMM, some consensus indicates annual eye examination, as there could be a greater risk of developing ocular melanoma.
References
Hurwitz S. Cutaneous tumors in childhood. In: Hurwitz S (Org.). Clinical pediatric dermatology: a textbook of skin disorders of childhood and adolescence. Philadelphia: W.B. Saunders Company; 1993. p. 198–241.
Walton RG, Jacobs AH, Cox AJ. Pigmented lesions in newborn infants. Br J Dermatol. 1976;95:389–96.
Mishima Y. Macromolecular changes in pigmentary disorders. Arch Dermatol. 1965;91:519–57.
Masson P. My conception of cellular nevi. Cancer. 1951;4:9–38.
Braun RP, Rabinovitz HS, Oliviero M, Kopf AW, Saurat JH. Dermoscopy of pigmented skin lesions. J Am Acad Dermatol. 2005;52:109–21.
Barnhill RL, Rabinovitz H. Neoplasias Melanocíticas Benignas. In: Bolognia JL, Jorizzo JL, Rapini RP (Org.). Dermatologia. São Paulo: Elsevier; 2011. p. 1713–40.
Rhodes AR, Sober AJ, Day CL. The malignant potential of small congenital nevocellular nevi: Na estimate based on histologic study of 234 primary cutaneous melanomas. J Am Acad Dermatol. 1982;6:230–41.
Illig L, Weidner F, Hundeiker M, et al. Congenital nevi <10 cm as precursors to melanoma. Arch Dermatol. 1985;121:1274–81.
Hurwitz S. Pigmented nevi: semin. Dermatology. 1988;7:17–25.
Rhodes AR, Mihm MC Jr. Origin of cutaneous melanoma in a congenital dysplastic nevus spilus. Arch Dermatol. 1990;126:500–5.
Cohen PR. Becker’s nevus. Am Fam Physician. 1988;37:221–6.
Fretzin DF, Whitney D. Familial Becker’s nevus. J Am Acad Dermatol. 1985;12:589–90.
Glinick SE, Alper JC, Bogaars H, et al. Becker’s melanosis: associated abnormalities. J Am Acad Dermatol. 1980;9:509–14.
Tse Y, Levine VJ, McClain SA, Ashinoff R. The removal of cutaneous pigmented lesions with the Q-switched ruby laser and the Q-switched Nd:YAG laser: a comparative study. J Dermatol Surg Oncol. 1994;20:795–800.
Jimbow K, Szabo G, Fitzpatrick TB. Ultrastructure of giant pigment granules (macromelanosomes) in cutaneous pigmented macules of neurofibromatosis. J Invest Dermatol. 1973;61:300–9.
Cole HN Jr, Hubler WR, Lund HZ. Persistent, aberrant Mongolian spots. Arch Dermatol Syph. 1950;61:244–60.
Chan HH, Ying SY, Ho HS, et al. An in vivo trial comparing the clinical efficacy and complications of Q-switched 755 nm alexandrite and Q-switched 1064 nm Nd:YAG lasers in treatment of nevus of Ota. Dermatol Surg. 2000;26:919–22.
Spitz S. Melanomas of childhood. Am J Pathol. 1948;24:591–602.
Arbuckle S, Weedon D. Eosinophilic globules in the Spitz nevus. J Am Acad Dermatol. 1982;7:324–7.
Paniago-Pereira C, Maize JC, Ackerman AB. Nevus of large spindle and/or epithelioid cells (Spitz’s nevus). Arch Dermatol. 1978;114:1811–23.
Hauschild A, Egberts F, Garbe C, Bauer J, Grabbe S, Hamm H, et al. Melanocytic nevi. J Dtsch Dermatol Ges. 2011;9(9):723–34.
King R, Hayzen BA, Page RN, Googe PB, Zeagler D, Mihm MC Jr. Recurrent nevus phenomenon: a clinicopathologic study of 357 cases and histologic comparison with melanoma with regression. Mod Pathol. 2009;22:611–7.
Fox JC, Reed JA, Shea CR. The recurrent nevus phenomenon: a history of challenge, controversy, and discovery. Arch Pathol Lab Med. 2011;135:842–6.
Tschandl P. Recurrent nevi: report of three cases with dermatoscopic-dermatopathologic correlation. Dermatol Pract Concepts. 2013;3:29–32.
Kelly JW, Shen S, Pan Y, Dowling J, McLean CA. Postexcisional melanocytic regrowth extending beyond the initial scar: a novel clinical sign of melanoma. Br J Dermatol. 2014;170:961–4.
Sommer LL, Barcia SM, Clarke LE, Helm KF. Persistent melanocytic nevi: a review and analysis of 205 cases. J Cutan Pathol. 2011;38:503–7.
Dummer R, Kempf W, Burg G. Pseudomelanoma after laser therapy. Dermatology. 1998;197:71–3.
Blum A, Hofmann-Wellenhof R, Marghoob AA, Argenziano G, Cabo H, Carrera C, et al. Recurrent melanocytic nevi and melanomas in dermoscopy: results of a multicenter study of the International Dermoscopy Society. JAMA Dermatol. 2014;150:138–45.
Botella-Estrada R, Nagore E, Sopena J, Cremades A, Alfaro A, Sanmartín O, et al. Clinical, dermoscopy and histologic correlation study of melanotic pigmentations in excision scars of melanocytic tumours. Br J Dermatol. 2006;154:478–84.
Hoang MP, Prieto VG, Burchette JL, Shea CR. Recurrent melanocytic nevus: a histologic and immunohistochemical evaluation. J Cutan Pathol. 2001;28:400–6.
Bolognia JL, Schaffer JV, Duncan KO, Ko CJ. Neoplasms of the skin. In: Bolognia JL, Schaffer JV, Duncan KO, Ko CJ, editors. Dermatology essentials. EUA: Elsevier; 2014. p. 892–928.
Duffy K, Grossman D. The dysplastic nevus: from historical perspective to management in the modern era: part I. J Am Acad Dermatol. 2012;67:1.e1–16.
Antonio JR, Soubhia RM, D’Avila SC, Caldas AC, Trídico LA, Alves FT. Correlation between dermoscopic and histopathologic diagnoses of atypical nevi in a dermatology outpatient clinic of the Medical School of São José do Rio Preto, SP, Brazil. An Bras Dermatol. 2013;88:199–203.
Kim CC, Swetter SM, Curiel-Lewandrowski C, Grichnik JM, Grossman D, Halpern AC, et al. Addressing the knowledge gap in clinical recommendations for management and complete excision of clinically atypical nevi/dysplastic nevi: pigmented lesion subcommittee consensus statement. JAMA Dermatol. 2015;151:212–8.
NIH Consensus Development Conference. Diagnosis and treatment of early melanoma. Consens Statement. 1992;10:1–25.
Clark WHJ, Reimer RR, Greene M, Ainsworth AM, Mastrangelo MJ. Origin of familial malignant melanomas from heritable melanocytic lesions: “The B-K mole syndrome”. Arch Dermatol. 1978;114:732–8.
Lynch HT, Fusaro RM, Pester J, Lynch JF. Familial atypical multiple mole melanoma (FAMMM) syndrome: genetic heterogeneity and malignant melanoma. Br J Cancer. 1980;42:58–70.
Elder DE, Goldman LI, Goldman SC, Greene MH, Clark WH Jr. Dysplastic nevus syndrome: a phenotypic association of sporadic cutaneous melanoma. Cancer. 1980;46:1787–94.
Rigel DS, Rivers JK, Friedman RJ, Kopf AW. Risk gradient for malignant melanoma in individuals with dysplastic naevi. Lancet. 1988;1:352–3.
Reimer RR, Clark WH Jr, Greene MH, Ainsworth AM, Fraumeni JF Jr. Precursor lesions in familial melanoma. A new genetic preneoplastic syndrome. JAMA. 1978;239:744–6.
Gandini S, Sera F, Cattaruzza MS, Pasquini P, Abeni D, Boyle P, et al. Meta-analysis of risk factors for cutaneous melanoma: I. Eur J Cancer. 2005;41:28–44.
Tucker MA, Halpern A, Holly EA, Hartge P, Elder DE, Sagebiel RW, et al. Clinically recognized dysplastic nevi. A central risk factor for cutaneous melanoma. JAMA. 1997;277:1439–44.
Hofmann-Wellenhof R, Blum A, Wolf IH, Piccolo D, Kerl H, Garbe C, et al. Dermoscopic classification of atypical melanocytic nevi (Clark nevi). Arch Dermatol. 2001;137:1575–80.
Clemente C, Cochran AJ, Elder DE, Levene A, MacKie RM, Mihm MC, et al. Histopathologic diagnosis of dysplastic nevi: concordance among pathologists convened by the World Health Organization Melanoma Programme. Hum Pathol. 1991;22:313–9.
Tsao H, Bevona C, Goggins W, Quinn T. The transformation rate of moles (melanocytic nevi) into cutaneous melanoma: a population-based estimate. Arch Dermatol. 2003;139:282–8.
Lin WM, Luo S, Muzikansky A, Lobo AZ, Tanabe KK, Sober AJ, et al. Outcome of patients with de novo versus nevus-associated melanoma. J Am Acad Dermatol. 2015;72:54–8.
Fuller SR, Bowen GM, Tanner B, Florell SR, Grossman D. Digital dermoscopic monitoring of atypical nevi in patients at risk for melanoma. Dermatol Surg. 2007;33:1198–206.
Arumi-Uria M, McNutt NS, Finnerty B. Grading of atypia in nevi: correlation with melanoma risk. Mod Pathol. 2003;16:764–71.
Duffy K, Grossman D. The dysplastic nevus: from historical perspective to management in the modern era: part II. J Am Acad Dermatol. 2012;67:19.e1–12.
Halpern AC, Guerry D 4th, Elder DE, Trock B, Synnestvedt M, Humphreys T. Natural history of dysplastic nevi. J Am Acad Dermatol. 1993;29:51–7.
Barr RJ, Linden KG, Rubinstein G, Cantos KA. Analysis of heterogeneity of atypia within melanocytic nevi. Arch Dermatol. 2003;139:289–92.
Strazzula L, Vedak P, Hoang MP, Sober A, Tsao H, Kroshinsky D. The utility of re-excising mildly and moderately dysplastic nevi: a retrospective analysis. J Am Acad Dermatol. 2014;71:1071–6.
Hocker TL, Alikhan A, Comfere NI, Peters MS. Favorable long-term outcomes in patients with histologically dysplastic nevi that approach a specimen border. J Am Acad Dermatol. 2013;68:545–51.
Silva JH, Sá BC, Avila AL, Landman G, Duprat Neto JP. Atypical mole syndrome and dysplastic nevi: identification of populations at risk for developing melanoma – review article. Clinics (Sao Paulo). 2011;66:493–9.
Suggested Literature
Farber MJ, Heilman ER, Friedman RJ. Dysplastic nevi. Dermatol Clin. 2012;30:389–404.
Kittler H, Tschandl P. Dysplastic nevus: why this term should be abandoned in dermatoscopy. Dermatol Clin. 2013;31:579–88.
Marghoob AA. Recurrent (persistent) nevi. In: Marghoob AA, Malvehy J, Braun RP, editors. Atlas of dermoscopy. London: Informa Healthcare; 2012. p. 198–202.
Nestle FO, Halpern AC. Melanoma. In: Bolognia JL, Jorizzo JL, Rapini RP (Org.). Dermatology. EUA: Elsevier; 2008. p. 1745–70.
Rosendahl CO, Grant-Kels JM, Que SK. Dysplastic nevus: fact and fiction. J Am Acad Dermatol. 2015;73:507–12.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Glossary
- Cryotherapy
-
A technique that uses an extremely cold liquid or instrument to freeze and destroy abnormal skin cells that require removal.
- Electrolysis
-
Electrochemical process whereby current is passed between two electrodes through an ionized solution (electrolyte) to deposit positive ions (anions) on the negative electrode (cathode) and negative ions (cations) on the positive electrode (anode). It is used for removing unwanted hair by destroying the hair root.
- Hydroquinone
-
An aromatic organic compound that is a type of phenol, having the chemical formula C6H4(OH)2. It is prescribed to reduce pigmentation of the skin in certain conditions whereby an excess of melanin causes hyperpigmentation.
- HMB-45
-
A monoclonal antibody that reacts against an antigen present in melanocytic tumors such as melanomas. The use of immunohistochemistry with melanocytic markers such as HMB-45 and Melan A, increases the detection rate of micrometastases.
- Ki-67
-
The Ki-67 protein (also known as MKI67) is a cellular marker for proliferation. It is strictly associated with cell proliferation.
- Leptomeningeal melanocytosis
-
The excessive deposit of melanin by increasing the number of melanocytes, usually seen as a signal in the convexities of subarachnoid spaces, or brain parenchyma such as cerebellum, temporal lobes, pons, and medulla on noncontrast images.
- Melanocytic
-
A type of lesion that contains nevus cells (a type of melanocyte).
- Peeling
-
Peeling skin, called desquamation in medical terms, can be caused by different conditions. Very often, skin peels following chemical, thermal, or sunburn, with the latter being the most common cause.
- Pseudopodia
-
Cytoplasmic structures found in some eukaryotes. Pseudopods are one of the three locomotion modes of unicellular organisms (together with flagella and cilia). Pseudopods can also capture prey by phagocytosis.
- Tyrosinase
-
An oxidase that is the rate-limiting enzyme for controlling the production of melanin.
Rights and permissions
Copyright information
© 2018 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Mariante, J.C.S., Escobar, G.F. (2018). Pigmented Lesions. In: Bonamigo, R., Dornelles, S. (eds) Dermatology in Public Health Environments. Springer, Cham. https://doi.org/10.1007/978-3-319-33919-1_60
Download citation
DOI: https://doi.org/10.1007/978-3-319-33919-1_60
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-33917-7
Online ISBN: 978-3-319-33919-1
eBook Packages: MedicineMedicine (R0)