
Abstract
Arid regions, the source of most airborne mineral dusts, comprise a third of the Earth’s land surface, where some two billion people are exposed daily to the fine particles raised by wind. Crossing political borders and travelling on air currents around the world, these particles not only affect the health of local communities, but also put many other populations extant at risk for cardiovascular and respiratory illnesses and a host of other health problems. Risks of exposure are affected by climatic conditions and their local and regional weather characteristics. And today, because of advancements in science and technology we are at the threshold of significantly reducing these health problems. Examples of meningitis, asthma and Valley fever are used to illustrate how risks may be lowered through a Dust-Health Early Warning System. A little more than a half-century of dedicated measurements of particulate air quality and of environmental science enhanced by Earth-orbiting satellites reveal the truth of airborne dust extent, and much of its variability in time and space. These truths have been essential in advancing numerical, dynamical models of the atmosphere that mimic and predict weather systems that loft the airborne dusts that medical sciences and epidemiology are proving harmful. This union of scientific disciplines and services makes possible today a means to improve public health around the world through a Global Dust-Health Early Warning System.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Aerosols
- Particulates
- Airborne dust
- Fungi
- Mineral dust
- Haboob
- Dust storm
- Dust source
- Cardiovascular
- Respiratory illness
- Valley fever
- Cocci
- Coccidioidomycosis
- Asthma
- Human health
- Health risks
1 A Global Dust-Health Early Warning System (D-HEWS)—The Motive
In late February 2015, a dust storm covering the Arabian Peninsula lasted several days. Child asthma emergency admissions to medical centers in Dubai jumped more than 20 % and asthma related hospital admissions increased more than 25 % in Abu Dhabi, United Arab Emirates (UAE 2015). While the Arabian Peninsula storm was underway, Korean television was alerting the Seoul population of an Asian dust storm bringing health-threatening dust into their area (Arirang 2015). Neither storms such as this nor their health consequences are unexpected. The World Health Organization (WHO) previously alerted all nations of the connection between cardiovascular hospital admissions and mortality to windblown desert dust (WHO 2006, 2013). In Geneva, just a few blocks away from the WHO, Terradellas et al. (2015) raised the human health problem again at the World Meteorological Organization (WMO).
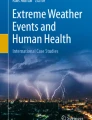
In the Sonoran desert of North America a dust storm of frightening proportions roared through the U.S. city of Phoenix, Arizona on 5 July 2011 (Fig. 1). It was an American haboob, a storm seen rarely in America except for the arid southwest. Produced from thunderstorms that advanced north from Tucson with downdrafts of 110 km/h pummeling the dry, hot desert floor, outflowing winds gusted to 80 km/h raising a cloud of dirt, sand and dust 1800 m high travelling more than 250 km through city, suburbs, farms and ranches along a 160 km front, 18 km deep (National Weather Service 2011). Mike Olbinski, the Phoenix photographer who took the picture in Fig. 1, says that when the dust overtook him, where he had quickly sought the safety of his truck, visibility dropped to zero (personal communication 2015). It was the first and largest of six such storms that occurred that year in Phoenix (Sprigg et al. 2014). On average, one to three haboob-like storms occur in the region each year according to Raman and Arellano (2013).

The Phoenix, Arizona haboob of 5 July 2011 around 7 PM local time looking southwest. See also the time lapse movie (https://vimeo.com/26045314). Photo and movie courtesy of Mike Olbinski, Phoenix, Arizona
Airborne mineral dusts range in size, from sand, a little larger than the width of a 70 µm human hair, to smaller, easily inhalable particles of PM10 and PM2.5. The latter refer to particulate matter of aerodynamic diameter 10 µm and less, and 2.5 µm and less. One micrometer (µm), or micron, is one millionth of a meter. These smaller particles maneuver past the fine hairs in one’s nose, into the lung. The finer, PM2.5 particles penetrate deep into the lung, and ultrafine particles even enter the blood stream.
Backed by a growing number of studies, arid land mineral dust emissions are shown to contribute to both cardiovascular and respiratory illnesses. Gupta et al. (2012) show that asthma patients experienced significant reduced pulmonary function when exposed to mineral dusts (PM10) that were collected from Rajasthan, the desert state of India. Meng and Lu (2007) statistically analyze respiratory and cardiovascular hospitalizations in Minqin, China, finding that Asia dust events increased both health problems, even reflecting the seasonal characteristics of disease surveillance. Giannadaki et al. (2014) assess global mortality rates from long-term exposure to airborne mineral dusts. More studies include Styer et al. (1995), Ostro et al. (1999, 2000), Lipsett et al. (2006), Cheng et al. (2008), and Goudie (2014). Whether in Kuwait (Thalib and Al-Taiar 2012), Lanzhou (Yan et al. 2012), Seoul (Hong et al. 2010), Sydney (Merrifield et al. 2013), Taipei (Chan and Ng 2011) or El Paso (Grineski et al. 2011), piece-by-piece the harm exacted by windblown dust is being documented.
Yet, more concerns of blowing dust emerge, including eye infections, meningitis, and Valley fever, or coccidioidomycosis: Laniado-Laborin (2007), Sandstrom and Forsberg (2008) and Morman and Plumlee (2013). Stafoggia et al. (2015) are convincing when they link mortality and hospital admissions in Southern Europe with invading Saharan dust. Goudie (2014) chronicles an extensive list of health problems associated with windblown desert dust. And, the U.S. National Research Council (2010) reviewed a Department of Defense effort to understand the health implications of airborne particulates from arid surroundings.
While concerns of public health agencies run the gamut of health complications from windblown dusts, three are elaborated in the following paragraphs: meningitis in Africa, asthma around the world, and Valley fever, or coccidioidomycosis, in the Americas. Addressing these will demonstrate the Conceptual Framework for the global early warning system: global monitoring of dust sources and airborne plumes; forecasts on hemispheric, regional and local geographical scales; and particulate air quality outlooks on climate space and time scales.
1.1 Meningitis
Africa’s Meningitis Belt stretches across the sub-Sahara (Sahel) afflicting many of the least developed countries of the world. The timing of major meningitis outbreaks and dust storms from the Sahara appear highly correlated, and Noinaj et al. (2012) hypothesize that Neisseria bacteria, responsible for meningitis, need iron-laden dust to grow and become virulent. Hence, simulating historical events of windblown dust helps to understand whatever role mineral dust may play in meningitis outbreaks across Africa (Pérez et al. 2014; Thomson et al. 2006, 2009; Molesworth et al. 2003). Forecasting near-term Saharan dust storms may lead to reductions in the severity of meningitis outbreaks when the connections between airborne dust and illness are well established and appropriate warning systems are in effect.
Today, the logistics of field research are helped by these forecasts. International organizations including the World Meteorological Organization (WMO), the World Health Organization (WHO) and the Group on Earth Observations (GEO) support research with many African countries in the “Meningitis Environmental Risk Information Technologies” project (MERIT 2012), where the WMO Sand and Dust Storm Warning Advisory and Assessment System (SDS-WAS) has provided observations, forecasts and simulations of airborne dust and dust storms to assess risks and attribution, cause and effect.
Yaka et al. (2008) and Sultan et al. (2005), examining climate time scales, show that wind is associated with meningitis outbreaks. Sultan even suggests that an “early warning index” for meningitis outbreaks could be developed from wind climate variability. It follows, too, that dust emissions will track climate conditions, as soil is anchored by dampening effects of precipitation and by moisture-invigorated plant roots; fresh foliage is an efficient trap for wind-driven sand and dust. Anticipating Africa’s climate may inform agencies of future efforts required to face the risks of meningitis.
A long-term drought across the Sahel that began in the early 1970s was a factor behind calls in the U.S. and elsewhere to increase climate research. The Sahel drought and overgrazing led to drying of Lake Chad and, quite possibly, to observed increases in dust, and whatever hitchhikes with it, transported across the Atlantic Ocean. Caribbean and Western Atlantic dust concentrations correlate with rainfall deficits in North Africa (Prospero and Lamb 2003). Iron- and clay-rich soils found in the Caribbean came from Africa. Prospero and Mayol-Bracero (2013) and Prospero et al. (2014) estimate that every year more than 700 million tons of Africa’s dust reach the Americas. In the Pacific basin, Schmidt (2014) and Shinn et al. (2000) find that nutrient-laden dust in Hawaiian rainforests is transported from Asian deserts.
1.2 Asthma
Exposure to desert dust is shown to increase risk of asthma hospitalization for children in Toyama, Japan (Kanatani et al. 2010). In Korea, Yoo et al. (2008, 1) report “… significantly higher frequency of respiratory symptoms” during Asian dust events. Yet, other studies have not found the connection, as in investigation of child asthma and airborne desert dust in Riyadh, Saudi Arabia (Alangari et al. 2015) and in Fukuoka City, Japan (Ueda et al. 2010). Watanabe et al. (2015a) found that Asia dust storms reduced pulmonary function in children, with the degree of impact differing with each dust event. Yet, in a companion study of adults with asthma (Watanabe et al. 2015b), pulmonary function scores were not significantly affected by Asia dust, but storms with larger, inhalable sand particles made lower respiratory tract symptoms worse.
On the other side of the world, under the influence of Africa dust outbreaks, Reyes et al. (2014) found conclusively that Saharan dust transported to Madrid, Spain, increased respiratory-caused hospital admissions. The Caribbean Allergy and Respiratory Association found that asthma has increased 17-fold in Barbados and Trinidad between 1973 and the turn of the Century (Shinn et al. 2000; Prospero and Lamb 2003; Prospero and Mayol-Bracero 2013). And, Molinie (2015) relates Africa dust to pediatric asthma on Guadeloupe. In a conflicting study, the Barbados Public Health Laboratory (Blades 2015) found no relationship between asthma and the 50-year record of Saharan dust measured at Ragged Point on the eastern edge of Barbados (Prospero et al. 2014). A general review of the literature shows that the epidemiology of desert dust and asthma is variable, often conflicting and inconclusive. This is at least partly due to what Wijesinghe et al. (2009, p. 1045) conclude as “… inherently difficult to interpret (trends in asthma mortality) because of the many factors that may change in different countries over time.” Asthma in Trinidad has been linked to both Africa dust (Gyan et al. 2003) and climatic conditions (Ivey et al. 2003).
Africa dust makes up about half the airborne particulates in South Florida’s air during the summer (Prospero and Lamb 2003; Prospero and Mayol-Bracero 2013). And, Saharan dust does not necessarily stop at Florida and the Caribbean. Further west, local sources of airborne dust are implicated in pediatric asthma and acute bronchitis in El Paso, Texas (Grineski et al. 2011), and Morain et al. (2007, 2009, 2010) engaged several state health agencies (and elementary school nurses) to test the efficacy of dust alerts in reducing respiratory, particularly asthma, risk.
1.3 Valley Fever
Exact locations of Coccidioides (C. immitis and C. posadasii) fungi are poorly known. They thrive in the generally hot, alternately damp and dry soils of the New World. When viable and inhaled, they cause Valley fever (coccidioidomycosis or cocci). Humans as well as their pet dogs and cats are at risk (Graupmann-Kuzma et al. 2008). This Valley fever, getting its name from San Joaquin Valley, California, not to be confused with Africa’s Rift Valley Fever, is believed endemic only in the Americas, generally from California south and east along the U.S./Mexico border, well into Mexico and Central and South America (Hector and Laniado-Laborin 2005; Barker et al. 2012). Yet, as we have seen, dust (and we must assume viable C. immitis and C. posadasii) is carried over considerable distance. Coccidioides fragments are 3–5 μm in size (Galgiani 2013) and would be included along with other dust particles in PM10. Yin and Sprigg (2010) show that significant amounts of dust cross the border into Texas from Mexico during typical dust events, with dust sources in the U.S. also affecting Mexico’s air quality. For Valley fever spores, a question remains as to how long in the free atmosphere Coccidioides fungi can stay viable. Pappagianis and Einstein (1978) attributed more than 379 new cases of Valley fever in California to a single 1977 dust storm. Windblown cocci spores from a landslide triggered during the 1994 Northridge, California earthquake caused 203 Valley fever cases in Ventura County, California (Schneider et al. 1997). Litvintseva et al. (2014) found human infection of Valley fever and local C. immitis spores in soils further north, well outside the known endemic regions for cocci, in Washington State. While spores may be carried to these regions beyond known endemic regions in ways other than severe weather, organism survival is, indeed, possible over long distances. For example, Prospero et al. (2005) captured viable, Saharan-sourced fungi and bacteria in the Caribbean.
Nguyen et al. (2013) review the state-of-the-science of Valley fever. Most cases are slight and unreported. For thirty to forty percent of cases that are documented, symptoms often mimic pneumonia. Common symptoms include coughing, fever, skin rash, feeling tired and difficulty breathing (Galgiani et al. 2005). Among the U.S. States, Arizona records the greatest number of cases. In 2004 about half of the 6000 cases reported nationwide occurred there (Laniado-Laborin 2007). The fact that cocci was not a reportable disease until 1997, and changes in laboratory tests in 2009 and reporting in 2013, have made construction of a long history of cocci impossible. For example, the 2009 change resulted in cocci numbers more than doubling the next year to 11,888 cases (Tsang et al. 2010; ADHS 2012). Treatment for the infection includes antifungal medication. Concerning vaccines, Galgiani (2008) gave a rather pessimistic prognosis that a vaccine to prevent coccidioidomycosis among infants in endemic regions and immigrants of any age would not be cost-effective.
Costs for cocci treatment are not trivial: 2007 Arizona Hospital Discharge Data show 1735 hospital visits for the disease, which translates to about $86 million. Galgiani et al. (2005) and Tsang et al. (2010) have analyzed cost and occurrence statistics for Valley fever in Arizona. Hector et al. (2011) report extensively on statistics for both Arizona and California. In neighboring Kern County, California, the CDC (1994) estimated $45 million for hospital stays and outpatient care between 1991 and 1993. Huang et al. (2015) figure 161 deaths from valley fever occurred on average every year between 1990 and 2008 in the United States. About 30 deaths are attributed to cocci in Arizona each year (Galgiani et al. 2005; Tsang et al. 2010). According to Flaherman and Rutherford (2007) an average of 70 deaths occurred annually in California between 1997 and 2008.
Yet, it appeared to this author that people were generally unaware of Valley fever, what caused it, and how risks of catching it might be lowered. The value of an early warning system will depend on a community’s understanding of the risks if warnings are ignored. Hearing from people who have contracted cocci might reveal clues about populations at risk, and how an early warning system might lower that risk.
1.3.1 Interviews with Valley Fever Sufferers
To gain a better understanding of the real impact of Valley fever, this author asked three individuals from Arizona neighborhoods who were under active surveillance or treatment for Valley fever if they would discuss their experiences for readers of this chapter. Two agreed, Mrs. K and Mr. H. Their accounts follow. The third, the youngest and most seriously affected, declined. One clear message from both interviews is that an early warning system must include public education about the disease, mainly because it is not widely publicized and often is misdiagnosed.
-
Mrs. K, In Her Own Words, June 22, 2015
I now live in Ohio, but early on a Wednesday morning in 2007 I lived in Southern Arizona and awoke with a bad headache and feeling very tired. Taking aspirin I struggled through that day and night. But Thursday morning the headache had worsened and now was accompanied by a terrible pain in my foot. I was listless and had developed a cough. I had no energy to get out of bed. My husband stayed home from work to tend to me. By Friday I had developed a fever and, along with the headache and joint pain, tired and short of breath, a rash appeared on my legs. We went to an Urgent Care where I was prescribed ‘Benedril,’ and sent home. The diagnosis: allergic reaction to an unknown factor.
Benedril was no help. The rash travelled up my legs, all the way to my neck. My husband took me to the hospital emergency room, for I was in no condition to drive. The triage nurse, seeing the rash on my stomach, gasped and said I had ‘cocci,’ which I learned later was Valley fever. The attending emergency room physician thought differently, agreeing with the allergic reaction diagnosed earlier at Urgent Care. I was given steroids through an IV and treated as ‘outpatient.’ The weekend went agonizingly slowly and painfully. My listlessness, shortness of breath, joint pain, cough and rash worsened.
On Monday I returned to the emergency room where a blood test for cocci returned negative and a chest X-ray revealed a small spot on my lung. Diagnosis: viral pneumonia. The next couple of days I heard nothing from the hospital as to what really might be wrong with me. I did not believe that viral pneumonia was responsible for all these symptoms! I was referred to a pulmonary specialist, and another blood test for cocci, which again came back negative. Someone, I no longer remember who, said I might have lung cancer!
Finally, after nearly two weeks of seeing so many doctors I lost count, a third blood test returned positive for Valley fever. Two weeks of watching the disease advance. At least now we knew the problem and it could be treated, as it should, with an anti-fungal medication, fluconazole. I took the antifungal pill for three months. My hair fell out. My pulmonary symptoms continued intermittently and other symptoms became significantly less severe. None of the previously prescribed treatments had helped at all.
Along the way through this ordeal I developed fibromyalgia in my legs, which, according to experts, is often associated with Valley fever. This was a new, very painful, experience. Cocci, it seems, wreaks havoc with one’s neural system.
For two and a half years after catching Valley fever I periodically developed lesions and the same rash on my stomach, the lingering consequences of Valley fever.
When asked whether she knew when she might have been exposed to the cocci fungus, Mrs. K said that it may have happened perhaps a week or more prior to that Wednesday she awoke with such stress. She had been in her back yard when a strong wind suddenly picked up dirt and dust from all around her. Before she could take cover, the dust enveloped her. She talked also about the family dog, Lady (an alias), who developed Valley fever at the same time, coughing, tired and walking with difficulty. Treated with similar antifungal medication over many months Lady recovered. Clearly, Mrs. K’s life had been severely changed by Valley fever and would never return to the quality before that Wednesday in 2007 when she first realized she was so ill.
Recollections of Mr. H
Sometimes the case for Valley fever is not as clear. Take, for example, Mr. H (Personal communication, May 18–28, 2015). In 2002, just before moving to the American Southwest, Mr. H had a regular health exam in New Jersey, including a chest X-ray that had revealed no problem. In 2003, just months after arriving in his new home in the Sonoran desert, he “experienced a rash on my arms and legs, and flu like symptoms, including headache, joint pain and a general feeling of fatigue over a ten to fourteen day period.” He does not recall having a fever or feeling nauseous. Since the time between infection and emergence of symptoms may be as long as four weeks (Galgiani 2012) he may not even recall when or where he was exposed to the cocci mold spore. He did not seek medical treatment. Being a newcomer to the region he had heard nothing about Valley fever or its symptoms.
He is a smoker and his Arizona internist ordered a chest X-ray in his 2004 annual physical. “Results suggested lung abnormalities, and comparison to the 2002 films evidenced a pronounced difference. Examination by a pulmonary specialist and a full C-T scan preceded a lung biopsy in January 2005. With seven nodules identified clearly by the C-T, the presumptive ingoing position was that I had lung cancer. They were all benign.”
“The biopsy was not the closing chapter in my book,” says Mr. H. “Although characterized as ‘damage or abnormality consistent with Valley fever exposure,’ further examination and blood tests did not provide confirmation. The exact cause of my lung nodules is indeterminate. I have an annual lung scan, results of which are compared to all prior records to ascertain if the nodules have changed in size or shape. I have been ‘stable’ since 2005.”
So, is Mr. H “stable” from a case of cocci … or something else? He has definitely suffered from something that negatively impacted his breathing and lung function. One fact is clear. Newcomers to cocci endemic regions are usually unaware of the disease, the symptoms or cause. Sometimes this applies to attending clinicians as well. An early warning system that includes public alerts, first of climatic pre-conditions for Valley fever and then, forecasted dust storms, will educate visitors and all new residents, physicians and clinicians included, of the dangers and ways to lower risks. As of right now however, no such system exists. Yet, as we shall see in the following pages, one could be operational today by making use of current technology.
1.3.2 Acquired Insights for a Valley Fever Early Warning System
A 2012 NASA-sponsored workshop and consequent study (Sprigg et al. 2012, 2014) makes several recommendations for reducing risk of contracting valley fever. Many of these risks may be lowered through increased cocci surveillance, stabilization of reporting methods, availability of satellite-based remote sensing and advances in dust storm modeling and prediction. New optimism about low cost, effective means of detecting C. immitis and C. posadasii in the soil (Sheff et al. 2010; Litvintseva et al. 2014; Hasan et al. 2014) opens the way to better define the geographical regions where cocci risks are higher, and where education, storm warnings and mitigation efforts may be most valuable. Too, C. immitis and C. posadasii thrive only in rather narrow climatic ranges (Kolivras and Comrie 2003a, b; Zender and Talamantes 2005; Comrie 2012), which informs us where potential changes in endemic areas may occur under conditions of climate variability and change. Enhanced cocci surveillance along with routine airborne dust forecasting will improve disease epidemiology and risk avoidance.
2 This Chapter’s Focus on Airborne Dust and Human Health
There are, of course, other health effects of wind blown dust, one or two steps removed from this chapter’s focus. They would include risks to aviation and highway safety, loss of arable soil and risks to food supplies, and to changes in fresh water storage and availability because dust accelerates melt of mountain snow and ice. Only aspects related to inhalation of airborne dust (and whatever hitchhikes with it) are addressed here.
In a world community of environmental and health scientists, health practitioners and service providers, we are far behind following through on the problem of airborne dirt from nature’s back yard. Common wisdom says that inhalation of particulates of any kind is unhealthy, but the focus of research, engineering and service has rested on man-made particles, principally those emissions from industry, energy and transportation. Outdoor natural environmental conditions are difficult to deconstruct. The problem has appeared intractable, as we shall see in 2.1. In addition to the anthropogenic source pollutants, spores, bacteria, viruses, pollens and other organic particles are carried along with mineral dust (Prospero et al. 2005; Smith et al. 2011). They complicate the epidemiologists’ world (Watanabe et al. 2011). So, to help those epidemiologists, the mechanisms for cause and effect, from inhalation of dust to negative health outcome, are under medical science scrutiny as well: Ghio et al. (2014), for example, show that human respiratory epithelial cells respond biologically to desert mineral dust, an effect further confirmed in respiratory tract injuries in mice following dust inhalation. And Ichinose et al. (2008) show that mice, exposed intratracheally to mineral dust, particularly silicon dioxide (SiO2), react with allergic inflammation in the lung—SiO2 is common in Earth’s crust, common in Arizona deserts, and commonly associated with sandstone and silica sand throughout the world.
2.1 The Dust-Health Challenge
Today, with negative health implications better understood, what can be done to stop emissions or avoid breathing this dust from a third of the Earth’s land surface? These questions are rather intimidating. At first blush it appears the answer is “nothing,” because such huge scales are involved. Recall that Prospero et al. (2014) estimate more than 700 million tons of Africa’s dust are transported annually across the Atlantic to the Caribbean and Central and South America—about half of the world’s annual airborne desert dust. We think of most of the other half also coming from such vast, uncontrollable sources as the Taklimakan, Gobi, Atacama, Simpson and Mohave deserts. These questions, and the usual hesitations that follow, often justify low priority for this research. Nonetheless, after the last decade or two of investigation into these dust sources, development of observation tools and networks, and atmospheric models that mimic pick-up, entrainment and dispersion of dust, the answers are right before us. The once parallel lines of airborne-dust-focused health and environmental sciences may now be aimed to intersect in a global dust-health early warning system. With it, comes a wealth of information for the epidemiology, diagnosis and prevention of all airborne particulate-based illnesses around the world.
-
Dust storms, their three dimensional plumes and downwind dust concentrations can be predicted, an opportunity to avoid harmful exposure
-
Dust storms and their downwind concentrations can be simulated, an opportunity for epidemiological studies of health consequences when looking into the past … or into the future under changing environmental conditions
-
Satellite-based instruments identify, measure and follow dust plumes around the world, a means to warn of approaching trans-continental, global dust movement
-
Surface-based remote sensing, a valuable complement to satellite instruments, identify and measure dust plume characteristics, a means to verify model forecasts and health consequences of exposure
-
Atmospheric models calculate the back-trajectories of known hazardous plumes to identify their origins, an opportunity to control emissions
-
Since dust emissions, even from the major deserts, are characteristically “point” sources, a few particularly hazardous ones may be controlled
-
Global, regional and local infrastructures are available to warn of oncoming windblown dust, including weather services, broadcast media, and social networks paced by smartphone technology
-
Global, regional and local health infrastructures are in place to respond to alerts and warnings, including the World Health Organization, the International Federation of Red Cross and Red Crescent Societies (IFRC 2013, 2014a, b), the Pan-America Health Organization, the Caribbean Public Health Agency, and public health service offices around the world.
3 Dust-Health Early Warning System—The Means
The underpinning for a Dust Health Early Warning System is available: in the medical, health, biological, and environmental sciences that currently demonstrate why airborne dust is a health hazard and how health risks may be reduced; in the current remote sensing and in situ environmental monitoring technology that reveal the truth of exposure; in the current skill of model forecasts and simulations; and in the infrastructure of current weather, health and information services that international, national and local missions provide. While nonexistent today, a D-HEWS could be assembled quickly from these components to serve global public health and medical communities.
3.1 Atmospheric Dust Modeling
Contemporary airborne dust forecast models can identify the time and place when blowing dust, or dirt, will cause air quality standards to be violated or will be a problem because of its content.
Zavisa Janjic (personal communication, Janjic 2013), in a lecture after receiving the prestigious International Meteorological Organization Prize for 2012, stated “… 10 km resolution medium range global forecasts and high resolution climate studies (are) possible with the NMMB (Nonhydrostatic Multiscale Model on B Grid).” This aim and thrust of research is another cause for optimism. We may relatively soon be able to go beyond the future-climate scenario-building of the Intergovernmental Panel on Climate Change (IPCC) and anticipate, in higher time and space resolution, local and regional dust-related health problems in future climates, not just for current climate conditions, as we do today. Current capabilities based on the Nickovic et al. (2001) dust regional model, DREAM, replicate all significant processes of dust mobilization, entrainment, dispersion and downwind wet and dry deposition (Nickovic 2002). In a forecast and simulation system in the U.S. Southwest that depends on state-of-the-science weather forecast models, such as the NMMB (Janjic and Gall 2012), and remote sensing technology and computer power, DREAM has demonstrated 24 to 36-h warnings of respirable dust concentrations on fine grid scales of under 4 km spatial resolution (Sprigg et al. 2014). This includes one remarkable forecast of the American haboob (Fig. 1) that struck the U.S. city of Phoenix on 5 July 2011 (Vukovic et al. 2014). Epidemiologists, public health experts and dust modelers have participated in tests of dust model systems for application in public health (Morain et al. 2007, 2009, 2010; Sprigg et al. 2014). The field of study has progressed such that within the framework of the World Meteorological Organization (WMO) Sand and Dust Storm Warning Advisory and Assessment System (SDS-WAS), dust models are now being compared with each other, to see which model structures and their internal components and treatments prove best under different circumstances and conditions (Huneeus et al. 2015).
Recall the potential health risks of very fine (SiO2) Silica dust (Ichinose et al. 2008) mentioned in Sect. 2. The digitized global database of soil classification is improving (Nickovic et al. 2012) and, when used in model boundary conditions for dust forecasts or simulations, adds a critical parameter for estimating health risk. Harris and Roffers (2012) show how existing geologic and soils data can be used to estimate risk potential for Valley fever. While Fisher et al. (2000, 2012) describe optimum soil environment conditions for Coccidioides (C. immitis and C. posadasii), the soil-dwelling spores responsible for Valley fever (coccidioidomycosis, or cocci), Sprigg et al. (2014) demonstrate how this information can be used in forecast models to assess downwind valley fever risks. As a first-order estimate of cocci high-risk areas, following techniques described, for example, in Steinberg and Steinberg (2015), these and other spatially mapped data locate high-risk, current hot spots for potential cocci spores, which would then form the model boundary condition for Coccidioides-laden dust emissions.
3.1.1 Model Forecast and Simulation Verification
Model objective verification is essential for the credibility of every operational forecasting system. Well-defined and conducted verification helps in several ways: An informed user needs to understand the quality of the product; verification guides model development and forecast improvement strategies; and the statistics of verification allow comparison of models with other systems and different forecast methodologies. The latter is of much practical value when selecting the most appropriate forecast system for a given application; the “best” performer in one season or region of the world may not be the best in another season or region. Typically, one wants to know forecast scores, bias (mean error), mean absolute error, root mean square error, and correlation coefficient of surface dust concentration (PM10 and PM2.5) and aerosol optical depth (AOD).
Verification of a dust forecast is challenging since surface observations of dust concentrations or low visibilities are not always located where the dust is occurring. Satellite observations over land also face problems such as high (and similar) reflectance for both dust aloft and soil below. The two vantage points for dust observations, space-based and surface-based, or in situ, are discussed next.
3.2 Satellite-Based Remote Sensing
Remote sensing from space-based platforms can identify and monitor dust sources and identify and track dust plumes as they drift around the world. Prospero et al. (2002) used satellite technology to identify preferential sources of dust. Morain et al. (2007, 2009) and Sprigg et al. (2008) applied NASA’s Moderate Resolution Imaging Spectroradiometer (MODIS), which sees every part of the earth every one to two days, to monitor dust sources in the NASA projects, PHAiRS (Public Health Applications in Remote Sensing) and ENPHASYS (ENvironmental Public Health Application SYStems). The Short-term Prediction Research and Transition (SPoRT) Center at NASA Marshall Space Flight Center uses a MODIS Normalized Difference Vegetation Index (NDVI) to produce a high-resolution, real-time, daily map of areas covered (and not) by vegetation. It has been shown to improve model surface characteristics (Case et al. 2014).
However, when dust becomes airborne over the land from which it originates it is hard to see. Technology improved quickly (Walker et al. 2009; Ginoux et al. 2010) from earlier attempts (Mahler et al. 2006) in the American southwest desert to distinguish airborne dust from the sand and dust of the same colour as the surface below. These new data and analysis methods help identify “point” emission sources from sites that appear to prefer releasing soil to the wind, while areas surrounding them are less apt to do so. Certain of these preferential point sources may be small enough to control.
Aiming to develop satellite tools for public health, Estes et al. (2009) use space-based remote sensing to identify dust storms. Prasad et al. (2010) used satellite observations to study implications of Sahara dust transported into the Nile Delta. Researchers all over the world are using satellite sensors to detect and distinguish airborne smoke, anthropogenic aerosols, dust and other airborne particles. For example, with critical use of satellite observations, El-Askary et al. (2003, 2009) and Fetouh et al. (2013) shed light on the complex nature of windblown dust and anthropogenic pollution over Egypt and the Nile delta region.
Remote sensing technology continues to offer new tools for researchers as well as practitioners to see further, faster and more completely than ever before. Details of particle composition and distribution with altitude are now possible, for example, from instruments that depict a virtual slice or cross-section of the atmosphere as the satellite flies overhead. The CALIPSO (Cloud-Aerosol Lidar and Infrared Pathfinder Satellite Observation) satellite, a French–American collaboration, provides such atmospheric profiles (Winker et al. 2004; McGill et al. 2007). Although it is relatively rare to catch a short-term event like an haboob, El-Askary was lucky! A CALIPSO flyby collected data which he analyzed for the date and time of the American haboob as it struck Phoenix on 5 July 2011 (Vukovic et al. 2014).
Satellites provide remotely sensed data from a maze of acronymned instruments useful in detecting and monitoring airborne dust, including the aforementioned MODIS twin sensors aboard NASA’s Terra and Aqua satellites, the Visible Infrared Imaging Radiometer Suite (VIIRS) aboard the Suomi NPP (National Polar-orbiting Partnership) satellite operated by the National Oceanic and Atmospheric Administration (NOAA), the Multi-angle Imaging Spectro-radiometer (MISR) instrument on Terra, the Ozone Monitoring Instrument (OMI) on the NASA Aura satellite, the Cloud-Aerosol Lidar with Orthogonal Polarization (CALIOP) sensor on CALIPSO.
Detecting bare soil, potential dust emission sites, is but one part of the solution to monitoring dust sources. When the ground is wet, sand and dust are not likely to become airborne. Dust forecasts depend on knowing when this may happen. While some numerical dust forecast systems (e.g. Nickovic et al. 2001) include damping of sources in the model forecast scheme, it is best to have verification, and perhaps even some reliance, on an observation. So, precipitation over potential dust emitting sources is important. Rainfall is measured from space in a collaboration of aerospace agencies from Japan, India, Europe and the U.S. One result is the Global Precipitation Measurement (GPM) Core Observatory satellite operated jointly by JAXA (Japan Aerospace eXploration Agency) and NASA. If you are still counting acronyms, here are three more: the GPM Imager (GMI), which maps precipitation across the land surface, the Dual-Frequency Precipitation Radar (DPR), which detects the intensity of snow and rain at Earth’s surface, and NASA’s Soil Moisture Active Passive (SMAP) mission, which maps soil moisture and whether the surface is frozen or thawed.
Technically sophisticated resources are globally available to forecast dust emissions and plumes. Most, if not all, dust researchers and forecasters take advantage of them, for example Liu et al. (2011) and Wang et al. (2011) for dust events over China and environs, and El-Askary et al. (2006) and Prasad and Singh (2007) who consider both space-based (MODIS) and surface-based (AERONET) remote sensing for insight on dust storm impacts over India. AERONET is discussed in following sections.
3.3 Surface-Based Remote Sensing and in Situ Observations
While space-based instruments, looking down, provide essential global coverage of Earth’s environmental dust conditions, similar technologies, looking up, anchored on the surface, are critical as well. Weather radar and instruments that measure meteorological conditions from points around the world are operated by national weather services linked to global data networks coordinated through the WMO. They are invaluable in verifying weather and dust model forecasts. The WHO monitors air quality to assess risks to human health; data are provided from national networks that serve various purposes, including epidemiology and development and enforcement of air quality standards.
3.3.1 Upward Looking Remote Sensing
A number of short-term, even multi-year research projects use upward-looking remote sensing instruments such as ceilometers (used to measure cloud heights and aerosol concentration), hand held sun-photometers (instruments for measuring direct Solar radiance) and Lidars (Light Detection And Ranging) to measure vertical column characteristics of dust and other aerosols. Data from many of these projects are not immediately available and are generally unannounced and unknown until completion of the project and publication of the results. A Dust-Health Early Warning System cannot depend on these disparate projects for routine model forecast verification. On the other hand, governments have established surface-based remote sensing networks that are dependable, tested, and data-rich, with data easily accessed and widely used.
The Aerosol Robotic Network (AERONET) is a federation of cooperative observing sites around the world using sun-photometers, direct-beam solar measurements that provide daytime AOD (Aerosol Optical Depth) measurements on average every 15-min (Holben et al. 1998, 2001; Dubovik et al. 2000). Established by NASA and the Centre National de la Recherche Scientifique (CNRS), AERONET provides information on the optical, physical and radiative properties of dust and other aerosols in the atmosphere. The network is used extensively today as a complement to AOD measurements from space and in airborne dust model verification (WMO 2015). With approximately 400 sites in 50 countries on all seven continents, it is the world’s largest ground-based network of sensors for aerosols.
The NASA Micro-Pulse Lidar Network (MPLNET) federated network of NASA and partners around the world measures aerosol (including dust) vertical structure continuously, day and night (Campbell et al. 2012). Lidar technology illuminates a target (e.g., a cloud of dust particles) with a laser, measures the distance to it, and analyzes the reflected light. Most MPLNET sites are co-located with AERONET sites. The networks provide vertical profiles of dust (and other aerosol) properties such as optical depth and particle size distribution (Campbell et al. 2010). MPLNET data are used to calibrate space-based lidars such as CALIOP/CALIPSO and to validate and help interpret measurements from NASA satellite sensors such as MISR (Misra et al. 2012). There were 17 active MPLNET sites reported in 2000 (Welton et al. 2001).
The European Lidar Network (EARLINET) provides ground-based information on the vertical distribution of aerosols over Europe. This included 27 stations in 16 countries in 2013 (Pappalardo et al. 2014; Binietoglou et al. 2015). The network was initially a research project established in 2000 to build a multi-year, statistically significant, database of a three dimensional, temporal distribution of aerosols on a continental scale.
3.3.2 In Situ Dust Measurements and Monitoring
Near surface observations of dust concentrations reveal the quality of the air we breathe. How well these observations contribute to health surveillance, epidemiology and dust modelling depends upon their length of record, their continuity, and the extent to which they are part of a coordinated network with high standards of measurement. Dust forecasts and simulations are compared with these observations for quantitative assessment of model skill. However, particulate air quality networks vary across the globe. To address this issue, the United Nations Environment Programme, with the WHO, World Bank, WMO and other international partners are part of a Global Platform on Air Quality and Health, now in the process of developing tools and information for monitoring and assessing air quality and health consequences around the world (WHO 2008; UNEP 2015). For the purpose of this chapter’s discussion, air quality networks of the United States, and the way in which the State of Arizona apply them, may serve as a model for the Dust-Health Early Warning System.
The U.S. Example of the Arizona Department of Environmental Quality (ADEQ) operates a network of ambient air quality instruments in order to meet Federal and State air quality requirements. The network exists, fundamentally, to answer the question: is Arizona in compliance with the National Ambient Air Quality Standards (Federal Register 2013) to protect public health and the environment? ADEQ’s six PM2.5 and fifteen PM10 monitoring sites include both filter-based samplers and continuous monitors located across the state. Filtered samples are analyzed for particle metal and chemical composition. The data from them become part of the US Environmental Protection Agency’s Air Quality database (AIRNow, http://www2.epa.gov/aqs#_). Individual counties in Arizona also maintain measurement sites that become part of the State and Federal cooperative network. All conform to data management and quality assurance according to national standards.
These data become part of the Center for Disease Control and Prevention (CDC) Environmental Public Health Tracking Network (Meyer et al. 2006; Charleston et al. 2008). Not all U.S. States participate directly in the EPHTN. Arizona does not, for example. Sprigg et al. (2012, 2014) make a case for expanding the CDC network, at least to all western states, where epidemiological studies of windblown dust health impacts are starved for a longer and a more geographically dense record of PM measurements and disease surveillance.
The EPHTN aims for the ongoing assembly, integration, analysis, interpretation, and dissemination of environmental hazard, human exposure and health surveillance data (Meyer et al. 2006; Charleston et al. 2008). The CDC funds 26 state and local health departments to develop local tracking networks that contribute to the national network. English and Balmes (2004) and Wilhelm et al. (2008) give the example of California.
The ADEQ partners with more PM networks, increasing data access for all: the Chemical Speciation Network (CSN), the National Air Toxics Trends Stations (NATTS), and the Interagency Monitoring of Protected Visual Environments (IMPROVE). The NATTS network is nationwide. The CSN is designed to determine trends in concentration of selected ions, metals, carbon species, and organic compounds in the PM2.5 samples. The CSN has about 200 sites nationwide. In 2002 there were 160 sites associated with IMPROVE, most located in the west (UC Davis 2002). The whole is, indeed, other than the sum of the parts.
Furthermore, it is common to cast a broad net for more data on particulate air quality. One example comes from the ADEQ Urban Haze Network, with high-resolution cameras, transmissometers and nephelometers that monitor visibility (ADEQ, Visibility Index Oversight Committee 2003). Vukovic et al. (2014) used Doppler RADAR images to define the three-dimensions of an American haboob. The RADAR’s radio waves bounced off the dust particles to reveal a picture of the storm that verified the model forecast.
4 Global Partners in Public Health Applications: Dust-Health Early Warning System—The Opportunity
Epidemiology, medical science and clinical evidence confirm that airborne dust is a health risk. Science and engineering have developed the tools to avoid much of that risk. And, the infrastructure to apply these tools for a healthier world is embedded in the missions of international, national, and local agencies and nongovernmental organizations.
4.1 A Conceptual Framework
The globally successful (Famine Early Warning System) begun in 1985 by the U.S. Agency for International Development, is a model for risk reduction and avoidance (Brown 2008). Research based analyses over an international federation of partners, delivers early warnings of environmental hazards and risks to agriculture and food production. A D-HEWS (Dust-Health Early Warning System) for health services can begin where dust forecast and simulation models are quasi-operational today and where they can be implemented with the earliest and greatest gain. A case in point: the African Sahel and wherever the dust and sand from the Sahara may travel, including to neighbors around the Mediterranean and the distant Caribbean and Americas. On the other side of the world, Asian dust events are a consequence as far eastward as the U.S., and routinely affect nearby Japan, Korea and Taiwan.
4.1.1 Global Dust Movement
The WMO Sand and Dust Storm Warning Advisory and Assessment System (WMO 2015) is operational today with forecasts and simulations of dust plumes on the hemispheric scale, generally depicting the 3-D presence of dust, in varying degrees of optical depth (AOD) or particle concentration, around 50 km spatial resolution. The global networks of observation systems, both satellite- and surface-based, monitor dust sources and plumes in real-time, and provide real-world data for model verification.
4.1.2 Regional and Local Dust Exposure
The synoptic scale forecast of near surface PM2.5 or PM10 concentrations is ready for validation in routine health and safety service operations (Sprigg et al. 2014). These forecasts, covering, for example, the entire SW United States, have spatial resolutions less than 4 km, fine enough to resolve thunderstorm dynamics and haboob-forming processes (Vukovic et al. 2014). Forecast skills will continue to improve from scientific advances, perhaps, for example, by Janjic’s 10 km global forecast model, by an expansion of the lidar system MPLNET, or by faster computers.
Rudiments of the synoptic scale warning system have been tested through the NASA sponsored projects mentioned earlier in Sect. 3.2, PHAiRS and ENPHASYS. Both focused on dust storm emissions of particulates (PM2.5 and PM10), their public health and safety consequences in the Southwest United States, how such conditions and their downwind plume concentrations may be predicted, and how to communicate results and find community solutions engaging science, service and the public (Morain et al. 2007, 2009; Sprigg et al. 2008, 2012).
4.1.3 Transdisciplinary Information Exchange (TIE)
The D-HEWS is an opportunity to “go global” with an international version of the CDC’s National Public Health Tracking Network (www.cdc.gov/nceh/tracking and www.ephtracking.cdc.gov). The NPHTN attracts the necessary talent in scientists, data managers and practitioners because it addresses a problem that everyone recognizes is important, each participant takes an essential role in a consensus plan, and accomplishments are documented and clear. The TIE for D-HEWS, adapted from the NPHTN structure, is envisioned a catalyst for assembling and distributing information on the sources and makeup of airborne dust, the observed and modeled airborne dust concentrations, and a clearinghouse for the scientific literature documenting potential human health risks.
4.2 Implementation
The WMO Sand and Dust Storm Warning Advisory and Assessment System (SDS-WAS), launched in 2007, responding to a request from more than forty countries to help address the health and safety issues surrounding windblown desert dust. From the system’s implementation plan (WMO 2015), its purpose is to “… develop, refine and provide a basis for distributing to the global community products that are useful in reducing the adverse impacts of SDS and to assess impacts of the SDS process on society and nature.” The WMO confidence in following through is undoubtedly based on many factors, including much improved, worldwide extent of environmental observations and dust measurements, advanced weather models, and the growing number of researchers attacking the problem.
A significant increase in airborne dust-related research publications (Stout et al. 2009), from 150 publications per year to 250 per year, roughly corresponds to greater access to in situ particulate air quality monitoring in the mid-1960s. The number of publications increased steadily to more than 500 per year in 1990, to approximately 900 per year in 1995. By 2012 the number jumped to some 7000 per year, as found in a Google Scholar search (WMO 2015) for “atmospheric dust Sahara” alone! Airborne dust forecast and simulation research from this author’s team (e.g., Mahler et al. 2006; Yin and Sprigg 2010; Sprigg et al. 2008, 2012, 2014; Vukovic et al. 2014) and that of his contemporaries (e.g., Park and In 2003; Zhou et al. 2008; Grell and Baklanov 2011; Knippertz and Todd 2011; Pérez et al. 2006; Pérez García-Pando et al. 2014; Huang et al. 2015) has been stimulated in the 21st century by greater availability of in situ and space-based observations, computing power and advances in weather forecast modeling (e.g. Tanaka and Chiba 2005; Janjic et al. 2001, 2010; Janjic and Gall 2012; Adachi et al. 2013; Müller and Janjic 2015).
The goals and mission for the SDS-WAS welcome a D-HEWS: (a) delivery of information and technology along with local capability in their use, (b) receipt of information on local dust characteristics and health consequences, and (c) assessment of priorities for research and services. Its mission: enhance WMO Members’ ability to deliver timely, quality sand and dust storm forecasts, observations, information and knowledge to users through an international partnership of research and operational communities (WMO 2015). In 2008, two SDS-WAS regional centres were established in China and Spain. A third node of cooperation that will complete global coverage for the System is under consideration for Pan America. Countries participating now in SDS-WAS number more than fifty (WMO 2015).
The WMO has integrated the SDS-WAS into other global, international infrastructure to add resources and greater assurance of long-term operational stability. The WMO World Weather Research Programme and the Global Atmosphere Watch coordinate the System jointly. In 2014, the World Health Organization (WHO) and the WMO formed a joint office to improve application of research, observations and knowledge of weather and climate in matters of global environmental health. Thus, the mechanism exists for WMO and WHO collaboration in SDS-WAS to understand airborne dust contributions to air quality and human health for today and for future climates. From this collaboration, further ties to public health communities are virtually assured and include the International Federation of Red Cross and Red Crescent Societies the regional Pan-America Health Organization and the Caribbean Public Health Agency, and national and local public health service offices around the world. The charter of the International Federation of Red Cross and Red Crescent Societies (IFRC 2014a) is particularly apt, with a mission to build local capacity within high-risk and vulnerable communities (IFRC 2013) and support national societies to develop the “processes, systems and teams” for acting locally and linking globally (IFRC 2014b).
5 Conclusions: Best Practices in Technology Transfer, Capacity Building, Training and Education
Meiyan et al. (2015, p. 1) state intentions, or best practices, quite nicely for early warning weather systems in general:
Increased media coverage and a perception of an acceleration in the occurrence of disasters has led to a public outcry for better information that will permit individuals to act in time to save their lives, property and livelihoods from damage. Thus, over the last 50 years, governments and the public have shifted from wanting to know what the weather will be to wanting to know what the weather will do (to socio-economic systems). Both want to mitigate and reduce disaster risks.
Dust forecasts through the WMO SDS-WAS will, of course, help in real-time risk avoidance. And model simulations of past dust conditions add to the air quality period of record, to building the capacity for epidemiological studies and to a deeper understanding of weather related health issues. Satellite pictures and forecast displays are important for education and raising public awareness of potential risks. Mobile apps and other public media allow rapid transfer of information to and from the public, researchers and forecast operations. Information and technology transfer, training for product production and use, and measures for assessing progress in “capacity building” would be done through “cooperation projects” that have the big picture in mind, integrated within the SDS-WAS, and leveraging health NGOs, local and regional resources, the WHO, PAHO and other intergovernmental agencies. And, research will keep feeding the system with new ideas and improvements.
All the necessary resources to launch a global, coordinated Dust-Health Early Warning System are available. Organizing them into an operational, federated system will require participation of the agencies and institutions that fund and manage them—and a plan. The quickest path to launch is through the agencies and organizations with a global mandate, but all who are integral to the system should be present, at least figuratively, from the beginning. So, local, regional and international health and environmental services will participate, as will medical, health and environmental sciences, without prejudice for either top-down or bottom-up guidance.
References
Adachi Y, Yukimoto S, Deushi M, Obata A, Nakano H, Tanaka TY, Hosaka M, Sakami T, Yoshimura H, Hirabara M, Shindo E, Tsujino H, Mizuta R, Yabu S, Koshiro T, Ose T, Kitoh A (2013) Basic performance of a new earth system model of the Meteorological Research Institute (MRI-ESM1). Pap Meteor Geophys 64:1–19. doi:10.2467/mripapers.64.1
ADEQ Visibility Index Oversight Committee (2003) Final report: recommendation for a Phoenix area visibility index. ADEQ. Phoenix, AZ, 5 Mar 2003
ADHS (2012) Arizona Valley Fever Report, 2007–2011. Arizona Department of Health Services, Phoenix, AZ
Alangari AA, Riaz M, Mahjoub MO, Malhis N, Al-Tamimi S, Al-Modaihsh A (2015) The effect of sand storms on acute asthma in Riyadh, Saudi Arabia; Ann Thorac Med 10(1):29–33. doi:10.4103/1817-1737.146857
Arirang (2015) http://www.arirang.co.kr/News/News_View.asp?nseq=176248
Barker BM, Tabor JA, Shubitz LF, Perrill R, Orbach MJ (2012) Detection and phylogenetic analysis of Coccidioides posadasii in Arizona soil samples. Fungal Ecol 5:163–176
Binietoglou I, Basart S, Alados-Arboledas L, Amiridis V, Argyrouli A, Baars H, Baldasano JM, Balis D, Belegante L, Bravo-Aranda JA, Burlizzi P, Carrasco V, Chaikovsky A, Comerón A, D’Amico G, Filioglou M, Granados-Muñoz MJ, Guerrero-Rascado JL, Ilic L, Kokkalis P, Maurizi A, Mona L, Monti F, Muñoz-Porcar C, Nicolae D, Papayannis A, Pappalardo G, Pejanovic G, Pereira SN, Perrone MR, Pietruczuk A, Posyniak M, Rocadenbosch F, Rodríguez-Gómez A, Sicard M, Siomos N, Szkop A, Terradellas E, Tsekeri A, Vukovic A, Wandinger U, Wagner J (2015) A methodology for investigating dust model performance using synergistic EARLINET/AERONET dust concentration retrievals. Atmos Meas Tech 8(3577–3600):2015
Blades E (2015) Personal communication
Brown ME (2008) Famine early warning systems and remote sensing data. Springer, Heidelberg. ISBN 978-3-540-75367-4 (Print) 978-3-540-75369-8 (Online)
Campbell JR, Reid JS, Westphal DL, Zhang J, Hyer EJ, Welton EJ (2010) CALIOP aerosol subset processing for global aerosol transport model data assimilation. J Sel Topics Appl Earth Obs Rem Sens 3:203–214
Campbell JR, Tackett JL, Reid JS, Zhang J, Curtis CA, Hyer EJ, Sessions WR, Westphal DL, Prospero JM, Welton EJ, Omar AH, Vaughan MA, Winker DM (2012) Evaluating nighttime CALIOP 0.532 μm aerosol optical depth and extinction coefficient retrievals. Atmos Meas Tech 5:2143–2160. doi:10.5194/amt-5-2143-2012
Case JL, LaFontaine FJ, Bell JR, Jedlovec GJ, Kumar SV, Peters-Lidard CD (2014) A real-time MODIS vegetation product for land surface and numerical weather prediction models. IEEE Trans Geosci Remote Sens 52(3):1772–1786
CDC (1994) Coccidioidomycosis—California, 1991–1993. MMWR 43(23):421–423
Chan CC, Ng HC (2011) A case-crossover analysis of Asian dust storms and mortality in the downwind areas using 14-year data in Taipei. Sci Total Environ 410–411:47–52
Charleston AE, Wall PA, Kassinger C, Edwards PO (2008) Implementing the environmental public health tracking network: accomplishments, challenges, and directions. J Public Health Manage Pract 14(6):507–514
Cheng MF, Ho SC, Chiu HF, Wu TN, Chen PS, Yang CY, Yang CY (2008) Consequences of exposure to Asian dust storm events on daily pneumonia hospital admissions in Taipei, Taiwan. J Toxicol Environ Health—Part A—Curr Issues 71(19):1295–1299. doi:10.1080/15287390802114808
Comrie AC (2012) Climate and coccidioidomycosis; valley fever and airborne dust forecasts and simulation workshop, 12 Jan 2012. In: Sprigg et al (ed) Airborne dust models: a tool in environmental health tracking; final report, CDC and the NASA program in applied sciences for health and air quality, CDC, Atlanta, GA, p 180
Dubovik O, Smirnov A, Holben BN, King MD, Kaufman YJ, Eck TF, Slutsker I (2000) Accuracy assessments of aerosol optical properties retrieved from AERONET sun and sky-radiance measurements. J Geophys Res Atmos 105:9791–9806
El-Askary H, Sarkar S, El-Ghazawi TA (2003) Multisensor approach to dust storm monitoring over the Nile delta. IEEE Trans Geosci Remote Sens 41:2386–2391
El-Askary H, Gautam R, Singh RP, Kafatos M (2006) Dust storms detection over the Indo-Gangetic basin using multi sensor data. Adv Space Res 37:728–733
El-Askary H, Farouk R, Ichoku C, Kafatos M (2009) Transport of dust and anthropogenic aerosols across Alexandria, Egypt. Ann Geophys 27:2869–2879. doi:10.5194/angeo-27-2869-2009
English P, Balmes J (2004) California’s new environmental health tracking programs. San Francisco Med 99(4):32–35
Estes SM, Haynes JA, Sprigg WA, Morain SA, Budge A (2009) Using NASA satellite remote sensing to identify dust and sand storms that aggravate respiratory diseases. American Thoracic Society 2009 International Conference, 15–20 May 2009, San Diego, California; 04/2009
Federal Register (2013) National ambient air quality standards for particulate matter. Final rule. National Archives and Records Administration, Federal Register, vol 78(10), pp 3086–3287
Fetouh YA, Askary HE, Allali M, Sprigg WA, Kafatos M (2013) Annual patterns of atmospheric pollutions and episodes over Cairo Egypt. Adv Met 2013, Article ID 984853, 11pp
Fisher F, Bultman MW, Pappagianis D (2000) Operational guidelines for geological fieldwork in areas endemic for coccidioidomycosis (Valley Fever). U.S. Geological Survey Open-File Report. U.S. Department of the Interior, Washington, DC, USA, pp 1–16
Fisher F, Bultman MW, Gettings ME, Johnson SM, Pappagianis D, Ampel NM (2012) A habitat overview. Valley fever and airborne dust forecasts and simulation workshop, 12 Jan 2012. In: Sprigg et al (ed) Airborne dust models: a tool in environmental health tracking; final report, the US Centers for Disease Control and Prevention and the National Aeronautics and Space Administration’s program in Applied Sciences for Health and Air Quality, CDC, Atlanta, GA, p 180
Flaherman VJ, Rutherford RGW (2007) Estimating severe coccidioidomycosis in California. Emerg Infect Dis 13(7):1087–1090
Galgiani JN (2008) Vaccines to prevent systemic mycoses: holy grails meet translational realities. J Infect Dis 197:938–940
Galgiani JN (2012) Recent dust storms and the risk of valley fever. Maricopa County Medical Society, Round-up, pp 16–18
Galgiani JN (2013) personal communication
Galgiani JN, Ampel NM, Blair JE, Catanzaro A, Johnson RH, Stevens DA, Williams PL (2005) Coccidioidomycosis. Clin Infect Dis 41(9):1217–1223
Ghio AJ, Kummarapurugu ST, Tong H, Soukup JM, Dailey LA, Boykin E, Gilmour MI., Ingram P, Roggli VL, Goldstein HL, Reynolds RL (2014) Biological effects of desert dust in respiratory epithelial cells and a murine model. Inhalation Toxicol 26(5):299–309. doi:10.3109/08958378.2014.888109
Giannadaki D, Pozzer A, Lelieveld J (2014) Modeled global effects of airborne desert dust on air quality and premature mortality. Atmos Chem Phys 14:957–968. doi:10.5194/acp-14-957-2014
Ginoux P, Garbuzov D, Hsu NC (2010) Identification of anthropogenic and natural dust sources using moderate resolution imaging spectroradiometer (MODIS) Deep Blue level 2 data. J Geophys Res 115(D05204):2010. doi:10.1029/2009JD012398
Goudie AS (2014) Desert dust and human health disorders. Environ Int 63:101–113. doi:10.1016/j.envint.2013.10.011 Epub 2013 Nov 26
Graupmann-Kuzma A, Valentine BA, Shubitz LF, Dial SM, Watrous B, Tornquist SJ (2008) Coccidioidomycosis in dogs and cats: a review. J Am Anim Hosp Assoc 44(5):226–235. doi:10.5326/0440226
Grell G, Baklanov A (2011) Coupled modeling for forecasting weather and air quality. Atmos Environ 45(38):6845–6851. doi:10.1016/j.atmosenv.2011.01.017
Grineski SE, Staniswalis JG, Bulathsinhala P, Peng Y, Gill TE (2011) Hospital admissions for asthma and acute bronchitis in El Paso, Texas: do age, sex, and insurance status modify the effects of dust and low wind events? Environ Res 111(8):1148–1155. doi: 10.1016/j.envres.2011.06.007. Epub 2011 Jul 23
Guputa P, Singh S, Kumar S, Choudhary M, Singh V (2012) Effect of dust aerosol in patients with asthma. J Asthma 2012(49):134–138
Gyan K, Henry W, Lacaille S, Laloo A, Lamsee C, Banks E, McKay S, Antoine RM, Monteil MA (2003) African dust clouds are associated with increased paediatric asthma Accident and Emergency admissions on the Caribbean island of Trinidad. ERA-International-Health (Lancet-based website for international research)
Harris WJ, Roffers PD (2012) Assessing erosion potential and Coccidioides immitis probability using existing geologic and soils data. In: Digital mapping techniques, 2010, workshop proceedings, USGS open-file report, 2012–1171
Hasan NA, Young BA, Minard-Smith AT, Saeed K, Li H, Heizer EM, McMillan NJ, Isom R, Abdullah AS, Bornman DM, Faith SA, Choi SY, Dickens ML, Cebula TA, Colwell RR (2014) Microbial community profiling of human saliva using shotgun metagenomic sequencing. PLoS ONE 9(5):e97699. doi:10.1371/journal.pone.0097699
Hector RF, Laniado-Laborin R (2002) Coccidioidomycosis—a fungal disease of the Americas. 10.1371/journal.pmed.0020002.g001
Hector RF, Rutherford GW, Tsang CA, Erhart LM, McCotter O, Anderson SM, Komatsu K, Tabnak F, Vugia DJ, Ying Y, Galgiani JN (2011) Public health impact of coccidioidomycosis in California and Arizona. Int J Environ Res Public Health 8(4):1150–1173
Holben BN, Eck TF, Slutsker I, Tanré D, Buis JP, Setzer A, Vermote E, Reagan JA, Kaufman YJ, Nakajima T, Lavenu F, Jankowiak I, Smirnov A (1998) AERONET—a federated instrument network and data archive for aerosol characterization. Remote Sens Environ 66(1–16):1998
Holben BN, Tanré D, Smirnov A, Eck TF, Slutsker I, Abuhassan N, Newcomb WW, Schafer JS, Chatenet B, Lavenu F, Kaufman YJ, Vande Castle J, Setzer A, Markham B, Clark D, Frouin R, Halthore R, Karneli A, O’Neill NT, Pietras C, Pinker RT, Voss K, Zibordi G (2001) An emerging ground based aerosol climatology: aerosol optical depth from AERONET. J Geophys Res 106(1206712097):2001
Hong Y-C, Pan X-C, Kim S-Y, Park K, Park E-J, Jin X, Yi S-M, Kim Y-H, Park C-H, Song S, Kim H (2010) Asian Dust Storm and pulmonary function of school children in Seoul. Sci Total Environ 408(4):754–759. doi:10.1016/j.scitotenv.2009.11.015
Huang M, Tong D, Lee P, Pan L, Tang Y, Stajner I, Pierce RB, McQueen J, Wang J (2015) Toward enhanced capability for detecting and predicting dust events in the western United States: the Arizona case study. acp-2015-526
Huneeus N, Basart S, Fiedler S, Morcrette JJ, Benedetti A, Mulcahy J, Terradellas E, Perez CGP, Pejanovic G, Nickovic S, Arsenovic P, Schulz M, Cuevas E, Baldasano JM, Pey J, Remy S, Cvetkovic B (2015) Forecasting the North African dust outbreaks towards Europe in April 2011: a model intercomparison. Atmos Chem Phys 15(19):26661–26710. doi:10.5194/acpd-15-26661-2015
Ichinose T, Yoshida S, Sadakane K, Takano H, Yanagisawa R, Inoue K, Nishikawa M, Mori I, Kawazato H, Yasuda A (2008) Effects of Asian sand dust, Arizona sand dust, amorphous silica and aluminum oxide on allergic inflammation in the murine lung. Inhalation Toxicol 2008(20):685–694
IFRC (2013) Annual report. http://www.ifrc.org/en/publications-and-reports/annual-report-2013/
IFRC (2014a) Disaster risk reduction makes development sustainable, IFRC, UNDP, UNICEF, Oxfam, GFDRR, UNISDR, 8 Apr 2014
IFRC (2014b) Setting up a national disaster preparedness and response mechanism; IFRC, 1 Oct 2014, 64 pp; ePub file, 125 MB
Ivey M, Simeon D, Monteil MA (2003) Climate variables are associated with seasonal acute asthma admissions to accident and emergency room facilities in Trinidad, West Indies. Clin Exp Allergy 33(11):1526–1530
Janjic Z (2013) PowerPoint presentation on nonhydrostatic multi-scale model (NMMB). NOAA/NWS/NCEP/EMC, College Park, MD; unpublished, personal communication
Janjic Z, Gall RL (2012) Scientific documentation of the NCEP nonhydrostatic multiscale model on the B grid (NMMB). Part 1 Dynamics. NCAR technical note NCAR/TN- 489+STR. doi:10.5065/D6WH2MZX
Janjic ZI, Gerrity JP Jr, Nickovic S (2001) An alternative approach to nonhydrostatic modeling. Mon Weather Rev 129:1164–1178
Janjic Z, Gall R, Pyle ME (2010) Scientific Documentation for the NMM Solver. NCAR Technical Note NCAR/TN-477+STR, 54 pp
Kanatani KT, Ito I, Al-Delaimy WK, Adachi Y, Mathews WC, Ramsdell JW (2010) Desert dust exposure is associated with increased risk of asthma hospitalization in children. Am J Respir Crit Care Med 182(12):1475–1481. Published online 2010 Jul 23. doi:10.1164/rccm.201002-0296OC
Knippertz P, Todd MC (2011) Mineral dust aerosols over the Sahara: meteorological controls on emission and transport and implications for modeling. Rev Geophys 50(RG1007):2012. doi:10.1029/2011RG000362
Kolivras KN, Comrie AC (2003a) Modeling valley fever (coccidioidomycosis) incidence on the basis of climate conditions. Int J Biometeorol 47(2):87–101
Kolivras KN, Comrie AC (2003b) Modeling valley fever (coccidioidomycosis) incidence on the basis of climate conditions. Int J Biometeorol 47(2):87–101
Laniado-Laborin R (2007) Expanding understanding of epidemiology of coccidioidomycosis in the Western hemisphere. Ann NY Acad Sci 1111:19–34
Lipsett MJ, Tsai FC, Roger L, Woo M, Ostro BD (2006) Coarse particles and heart rate variability among older adults with coronary artery disease in the Coachella Valley, California. Environ Health Perspect 114(8):1215–1220
Litvintseva AP, Marsden-Haug N, Hurst S, Hill H, Gade L, Driebe EM, Ralston C, Roe C, Barker BM, Goldoft M, Keim P, Wohrle R, Thompson GR III, Engelthaler DM, Brandt ME, Chiller T (2014) Valley fever: finding new places for an old disease: Coccidioides immitis found in Washington state soil associated with recent human infection. Clin Inf Dis. doi:10.1093/cid/ciu681
Liu J, Zheng Y, Li Z, Flynn C, Welton EJ, Cribb M (2011) Transport, vertical structure and radiative properties of dust events in southeast China determined from ground and space sensors. Atmos Environ 45(6469–6480):2011
Mahler A-B, Thome K, Yin D, Sprigg WA (2006) Dust transport model validation using satellite- and ground-based methods in the southwestern United States. SPIE 6299. ISBN 9780819463784
McGill MJ, Vaughan MA, Trepte CR, Hart WD, Hlavka DL, Winker DM, Kuehn R (2007) Airborne validation of spatial properties measured by the CALIPSO lidar. J Geophys Res 112:D20201. doi:10.1029/2007JD008768
Meiyan J, Lianchun S, Tong J, Di Z, Jianqing Z (2015) China’s implementation of impact and risk-based early warning. WMO Bull 64(2):9–12. http://www.wmo.int/bulletin/en/content/chinas-risk-based-early-warning
Meng ZQ, Lu B (2007) Dust events as a risk factor for daily hospitalization for respiratory and cardiovascular diseases in Minqin, China. Atmos Environ 41:7048–7058
MERIT (2012) 6th MERIT technical meeting report, Nov 2012. Health and Climate Foundation, Geneva, Switzerland, 43 pp. Available from: http://merit.hc-foundation.org/eventpage.html
Merrifield A, Schindeler S, Jalaludin B, Smith W (2013) Health effects of the September 2009 dust storm in Sydney, Australia: did emergency department visits and hospital admissions increase? Environ Health 12:32. doi:10.1186/1476-069X-12-32
Meyer P, WatkinsT, Qualters J (2006) National Environmental Public Health Tracking Network. EM. 22–24 Sept 2006
Misra A, Tripathi SN, Kaul DS, Welton EJ (2012) Study of MPLNET-derived aerosol climatology over Kanpur, India, and validation of CALIPSO Level 2 Version 3 backscatter and extinction products. J Atmos Oceanic Technol 29:1285–1294
Molesworth AM, Cuevas LE, Connor SJ, Morse AP, Thomson MC (2003) Environmental risk and meningitis epidemics in Africa. Emerg Infect Dis 9:1287–1293
Molinie J (2015) The relationship between pediatric asthma on Guadeloupe and PM2.5 and PM10 associated with African dust. In: Symposium on airborne dust, climate change, and human health, Miami, Florida; 19–21 May 2015
Morain SA, Sprigg WA, Benedict K, Budge A, Budge T, Hudspeth W, Barbaris B, Yin D, Shaw P (2007) Public health applications in remote sensing: verification and validation report. NASA Cooperative agreement NNS04AA19A
Morain SA, Sprigg WA, Benedict K, Budge A, Budge T, Hudspeth W, Sanchez G, Barbaris B, Catrall C, Chandy B, Mahler AB, Shaw P, Thome K, Nickovic S, Yin D, Holland D, Spear J, Simpson G, Zelicoff A (2009) Public health applications in remote sensing: final benchmark report. NASA Coorperative agreement NNS04AA19A
Morain SA, Budge AM, Sprigg WA (2010) Modeling atmospheric dust for respiratory health alerts. American Meteorological Society, Atlanta, GA. Manuscript J 17.4, p 7
Morman SA, Plumlee GS (2013) The role of airborne mineral dusts in human disease. Aeolian Res 9:203–212
Müller DM, Janjic ZI (2015) Verification of the new nonhydrostatic multiscale model on B grid (NMMB): a view on global predictability of surface parameters. Weather Forecast 30(3):150128094517003. doi:10.1175/WAF-D-14-00049.1
National Research Council (NRC) (2010) Review of the Department of Defense Enhanced Particulate Matter Surveillance. National Academies Press. ISBN:978-0-309-15413-0
National Weather Service (2011) http://www.wrh.noaa.gov/psr/pns/2011/July/DustStorm.php
Nguyen C, Barker BM, Hoover S, Nix D, Ampel NM, Frelinger JA, Orbach MJ, Galgiani JN (2013) Recent advances in our understanding of the environmental, epidemiological, immunological, and clinical dimensions of coccidioidomycosis. Clin Microbiol Rev 26(3):505. doi:10.1128/CMR.00005-13
Nickovic S (2002) Dust aerosol modeling: step toward integrated environmental forecasting (invited paper). Eos Trans AGU 83(47), Fall Meet Suppl, Abstract A71E-04
Nickovic S, Kallos G, Papadopoulos A, Kakaliagou O (2001) A model for prediction of desert dust cycle in the atmosphere. J Geophys Res 106:18113–18129
Nickovic S, Vukovic A, Vujadinovic M, Djurdjevic V, Pejanovic G (2012) Technical note: high-resolution mineralogical database of dust-productive soils for atmospheric dust modeling. Atmos Chem Phys 12:845–855. doi:10.5194/acp-12-845-2012
Noinaj N, Easley NC, Oke M, Mizuno N, Gumbart J, Boura E, Steere AN, Zak O, Aisen P, Tajkhorshid E, Evans RW, Gorringe AR, Mason AB, Steven AC, Buchanan SK (2012) Structural basis for iron piracy by pathogenic Neisseria. Nature 483:53–58. doi:10.1038/nature10823
Ostro BD, Hurley S, Lipsett MJ (1999) Air pollution and daily mortality in the Coachella Valley, California: a study of PM10 dominated by coarse particles. Environ Res 81:231–238
Ostro BD, Broadwin R, Lipsett MJ (2000) Coarse and fine particles and daily mortality in the Coachella Valley, California: a follow-up study. J Expo Anal Environ Epidemiol 10(5):412–419
Pappagianis D, Einstein H (1978) Tempest from Tehachapi takes toll or coccidioides conveyed aloft and afar. West J Med 1978(129):527–530
Pappalardo G, Amodeo A, Apituley A, Comeron A, Freudenthaler V, Linné H, Ansmann A, Bösenberg J, D’Amico G, Mattis I, Mona L, Wandinger U, Amiridis V, Alados-Arboledas L, Nicolae D, Wiegner M (2014) EARLINET: towards an advanced sustainable European aerosol lidar network. Atmos Meas Tech 7(2389–2409):2014
Park S-U, In H-J (2003) Parameterization of dust emission for the simulation of the yellow sand (Asian dust) event observed in March 2002 in Korea. J Geophy Res 108
Pérez García-Pando C, Stanton MC, Diggle PJ, Trzaska S, Miller RL, Perlwitz JP, Baldasano JM, Cuevas E, Ceccato P, Yaka P, Thomson MC (2014) Soil dust aerosols and wind as predictors of seasonal meningitis incidence in Niger. Environ Health Perspect 122:7. doi:10.1289/ehp.1306640
Pérez C, Nickovic S, Pejanovic G, Baldasano JM, Özsoy E (2006) Interactive dust-radiation modeling: a step to improve weather forecasts. J Geophys Res 111:D16206. doi:10.1029/2005JD006717
Prasad AK, Singh RP (2007) Changes in aerosol parameters during major dust storm events (2001–2005) over the Indo-Gangetic basin using AERONET and MODIS data. J Geophys Res 112:D09208. doi:10.1029/2006JD007778
Prasad AK, El-Askary H, Kafatos M (2010) Implications of high altitude desert dust transport from Western Sahara to Nile Delta during biomass burning season. Environ Pollut 158:3385–3391
Prospero JM, Lamb PJ (2003) African droughts and dust transport to the Caribbean: climate change implications. Science 302(5647):1024–1027. doi:10.1126/science.1089915
Prospero JM, Mayol-Bracero OL (2013) Understanding the transport and impact of African dust on the Caribbean Basin. Bull Am Meteorol Soc 94(9):1329–1337
Prospero JM, Ginoux P, Torres O, Nicholson SE, Gill TE (2002) Environmental characterization of global sources of atmospheric soil dust identified with the NIMBUS 7 Total Ozone Mapping Spectrometer (TOMS) absorbing aerosol product. Rev Geophys 40:1002. doi:10.1029/2000RG000095
Prospero JM, Blades E, Mathison G, Naidu R (2005) Interhemispheric transport of viable fungi and bacteria from Africa to the Caribbean with soil dust. Aerobiologia 21:1–19. doi:10.1007/s10453-004-5872-7
Prospero JM, Collard F-X, Molinié J, Jeannot A (2014) Characterizing the annual cycle of African dust transport to the Caribbean Basin and South America and its impact on the environment and air quality. Global Biogeochem Cycles 29:757–773. doi:10.1002/2013GB004802
Raman A, Arellano FA Jr (2013) Modeling and data analysis of 2011 Phoenix Dust Storm. 93rd AMS annual meeting, 5–10 Jan 2013, Austin, Texas
Reyes M, Diaz J, Tobias A, Montero JC, Linares C (2014) Impact of Saharan dust particles on hospital admissions in Madrid (Spain). Int J Environ Health Res 24(1):63–72. doi: 10.1080/09603123.2013.782604. Epub 2013 Apr 2
Sandstrom T, Forsberg B (2008) Desert Dust an unrecognized source of dangerous air pollution? Epidemiology 19:808–809
Schmidt LJ (2014) When the dust settles. http://earthobservatory.nasa.gov/Features/Dust/
Schneider E, Hajjeh RA, Speigel RA, Jibson RW, Harp EL, Marshall GA, Gunn RA, McNeil MM, Pinner RW, Baron RC, Burger RC, Hutwagner LC, Crump L, Kaufman SE, Reef GM, Feldman D, Pappagianis SB, Werner (1997) A coccidioidmycosis outbreak following the Northridge, California, Earthquake. J Am Med, Ass 277
Sheff K, York E, Driebe E, Barker B, Rounsley S, Waddell V, Beckstrom—Sternberg S, Keim P, Engelthaler D (2010) Development of a rapid, cost—effective TaqMan real—time PCR assay for identification and differentiation of Coccidioides immitis and Coccidioides posadasii. Med Mycol 48:466–469
Shinn EA, Smith GW, Prospero JM, Betzer P, Hayes ML, Garrison V, Barber RT (2000) African dust and the demise of Caribbean coral reefs. Geophys Res Lett 27(19):3029–3032
Smith DJ, Griffin DW, McPeters RD, Ward PD, Schuerger AC (2011) Microbial survival in the stratosphere and implications for global dispersal. Aerobiologia 27:319–332
Sprigg WA, Barbaris B, Morain S, Budge A, Hudspeth W, Pejanovic G (2008) Public health applications in remote sensing. http://spie.org/x33688.xml?ArticleID=33688
Sprigg WA, Galgiani JN, Nickovic S, Pejanovic G, Vujadinovic M, Vukovic A, Prasad A, Petkovic S, El-Askary H, Gaddi R, Janjic Z, Pappagianis D, Sarafoglou N, Kafatos M, Bruck M, Ferng M-J (2012) Airborne dust models: a tool in environmental health tracking. Final report, the U.S. Centers for Disease Control and Prevention and the National Aeronautics and Space Administration’s program in Applied Sciences for Health and Air Quality; CDC, Atlanta, GA, 180 pp
Sprigg WA, Nickovic S, Galgiani J, Pejanovic G, Petkovic S, Vujadinovic M, Vukovic A, Dacic M, DiBiase S, Prasad A, El-Askary H (2014) Regional dust storm modeling for health services: the case of valley fever. J Aeolian Res. doi:10.1016/j.aeolia.2014.03.001
Stafoggia M, Zauli-Sajani S, Pey J, Samoli E, Alessandrini E, Basagaña X, Cernigliaro A, Chiusolo M, Demaria M, Díaz J, Faustini A, Katsouyanni K, Kelessis AG, Linares C, Marchesi S, Medina S, Pandolfi P, Pérez N, Querol X, Randi G, Ranzi A, Tobias A, Forastiere F, MED-PARTICLES Study Group (2015) Desert dust outbreaks in Southern Europe: contribution to daily PM10 concentrations and short-term associations with mortality and hospital admissions. Environ Health Perspect. doi:10.1289/ehp.1409164
Steinberg SL, Steinberg SJ (2015) GI research methods: incorporating spatial perspectives. Esri Press, Redlands, CA. ISBN 978-1-58948-378-1
Stout JE, Warren A, Gill TE (2009) Publication trends in aeolian research: an analysis of the bibliography of Aeolian Research. Geomorphology 105(2009):6–17. doi:10.1016/j.geomorph.2008.02.015
Styer P, McMillan N, Gao F, Davis J, Sacks J (1995) Effect of outdoor airborne particulate matter on daily death counts. Environ Health Perspect 103:490–497
Sultan B, Labadi K, Guegan JF, Janicot S (2005) Climate drives the meningitis epidemics onset in West Africa. Plos Med 2:43–49
Tanaka TY, Chiba M (2005) Global simulation of dust aerosol with a chemical transport model, MASINGAR. J Meteorol Soc JPN 83A:255–278
Terradellas E, Nickovic S, Zhang XY (2015) Airborne dust: a hazard to human health, environment and society. WMO Bull 64(2):42–46
Thalib L, Al-Taiar A (2012) Dust storms and the risk of asthma admissions to hospitals in Kuwait. Sci Total Environ 433:347–351
Thomson MC, Molesworth AM, Djingarey MH, Yameogo KR, Belanger F, Cuevas LE (2006) Potential of environmental models to predict meningitis epidemics in Africa. Trop Med Int Health 11:781–788
Thomson MC, Jeanne I, Djingarey M (2009) Dust and epidemic meningitis in the Sahel: a public health and operational research perspective. IOP Conf Ser: Earth Environ Sci 7:4
Tsang CA, Anderson SM, Imholte SB, Erhart LM, Chen S, Park BJ, Christ C, Komatsu KK, Chiller T, Sunenshine RH (2010) Enhanced surveillance of coccidioidomycosis, Arizona, USA, 2007–2008. Emerg Infect Dis 16(11). www.cdc.gov/eid
UAE (2015) http://www.thenational.ae/uae/asthma-cases-up-by-25-as-dust-blows-across-the-uae
UC Davis (2002) Annual report, aerosol collection and compositional analysis for improve; NPS Contract C2350990001; http://vista.cira.colostate.edu/improve/Publications/AnnulReport_UCD/CY02ANN.pdf
Ueda K, Nitta H, Odajima H (2010) The effects of weather, air pollutants, and Asian dust on hospitalization for asthma in Fukuoka. Environ Health Prev Med 15:350–357
UNEP (2015) Air quality monitoring system. Division of Early Warning and Assessment. UNEP, Nairobi, Kenya
Vukovic A, Vujadinovic M, Pejanovic G, Andric J, Kumjian MR, Djurdjevic V, Dacic M, Prasad AK, El-Askary HM, Paris BC, Petkovic S, Nickovic S, Sprigg WA (2014) Numerical simulation of “an American haboob”. Atmos Chem Phys 14:3211–3230. doi:10.5194/acp-14-3211-2014
Walker AL, Liu M, Miller SD, Richardson KA, Westphal DL (2009) Development of a dust source database for mesoscale forecasting in southwest Asia. J Geophys Res 114:D18207. doi:10.1029/2008JD011541
Wang S-H, Tsay S-C, Lin N-H, Hsu NC, Bell SW, Li C, Ji Q, Jeong M-J, Hansell RA, Welton EJ, Holben BN, Sheu G-R, Chu Y-C, Chang S-C, Liu J-J, Chiang W-L (2011) First detailed observations of long-range transported dust over the northern South China Sea. Atmos Environ 45(4804–4808):2011
Watanabe M, Igishi T, Burioka N, Yamasaki A, Kurai J, Takeuchi H, Sako T, Yoshida A, Yoneda K, Fukuoka Y, Nakamoto M, Hasegawa Y, Chikumi H, Matsumoto S, Minato S, Horasaki K, Shimizu E (2011) Pollen augments the influence of desert dust on symptoms of adult asthma patients. Allergol Int 60:517–524
Watanabe M, Noma H, Kurai J, Sano H, Saito R, Abe S, Kimura Y, Aiba S, Oshimura M, Yamasaki A, Shimizu E (2015a) Decreased pulmonary function in school children in Western Japan after exposures to Asian desert dusts and its association with interleukin-8. Biomed Res Int 2015:583293. doi:10.1155/2015/583293 Epub 2015 Apr 28
Watanabe M, Noma H, Kurai J, Shimizu A, Sano H, Kato K, Mikami M, Ueda Y, Tatsukawa T, Ohga H, Yamasaki A, Igishi T, Kitano H, Shimizu E (2015b) Association of sand dust particles with pulmonary function and respiratory symptoms in adult patients with asthma in Western Japan using light detection and ranging: a panel study. Int J Environ Res Public Health 12(10):13038–13052. doi:10.3390/ijerph121013038
Welton EJ, Campbell JR, Spinhirne JD, Scott VS III (2001) Global monitoring of clouds and aerosols using a network of micropulse lidar systems. In: Singh UN (ed) Lidar Remote Sensing for Industry and Environment Monitoring. International Society for Optical Engineering (SPIE proceedings, vol 4153), pp 151–158. doi:10.1117/12.417040
WHO (2006) WHO air quality guidelines global update 2005, Bonn, Germany, World Health Organization, ISBN 92-890-2192-6. WHO Regional Office for Europe, Copenhagen Ø, Denmark
WHO (2008) Part 1: Guidance document on characterizing and communicating uncertainty in exposure assessment, harmonization project document no. 6. Published under joint sponsorship of the World Health Organization, the International Labour Organization and the United Nations Environment Programme. WHO Press, World Health Organization, Geneva, Switzerland
WHO (2013) Review of evidence on health aspects of air pollution—REVIHAAP project, technical report. WHO Regional Office for Europe, Copenhagen Ø, Denmark, 309 pp
Wijesinghe M, Weatherall M, Perrin K, Crane J, Beasley R (2009) International trends in asthma mortality rates in the 5- to 34-year age group: a call for closer surveillance. CHEST 2009 135:1045–1049. doi:10.1378/chest.08-2082
Wilhelm M, Meng Y, Rull R, English P, Balmes J, Ritz B (2008). Environmental public health tracking of childhood asthma using California health interview survey, Traffic and Outdoor Air Pollution Data. Environ Health Perspect. doi:10.1289/ehp.10945
Winker DM, Hunt WH, Hostetler CA (2004) Status and performance of the CALIOP lidar. Proc SPIE Int Soc Opt Eng 5575:8–15
WMO (2015) Sand and dust storm warning advisory and assessment system (SDS-WAS). Science and implementation plan: 2015–2020. WMO Research Department, Atmo. Res. Environ. Br., 30 pp
Yaka P, Sultan B, Broutin H, Janicot S, Philippon S, Fourquet N (2008) Relationships between climate and year-to-year variability in meningitis outbreaks: a case study in Burkina Faso and Niger. Int J Health Geographics 7:13. doi:3410.1186/1476-072x-7-34
Yan T, An XQ, Sun ZB, Qing H, Yu W (2012) Association between dust weather and number of admissions for patients with respiratory diseases in spring in Lanzhou. Sci Total Environ 423:8–11. doi:10.1016/j.scitotenv.2012.01.064
Yin D, Sprigg WA (2010) Modeling airborne mineral dust: A Mexico—United States trans-boundary perspective. In: Halvorson W, Schwalbe C, van Riper C III (eds) Southwestern desert resources. University of Arizona Press, Tucson, AZ, pp 303–317
YooY, Choung JT, Yu J, Kim do K, Koh YY (2008) Acute effects of Asian dust events on respiratory symptoms and peak expiratory flow in children with mild asthma. J Korean Med Sci 23(1):66–71. doi:10.3346/jkms.2008.23.1.66
Zender CS, Talamantes J (2005) Climate controls on valley fever incidence in Kern County, California. Int J Biometeorol 50(3):174–182 Epub 2005 Oct 26
Zhou CH, Gong SL, Zhang XY, Wang YQ, Niu T, Liu HL, Zhao TL, Yang YQ, Hou Q (2008) Development and evaluation of an operational SDS forecasting system for East Asia: CUACE/Dust. Atmos Chem Phys 8:787–798
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Sprigg, W.A. (2016). Dust Storms, Human Health and a Global Early Warning System. In: Steinberg, S., Sprigg, W. (eds) Extreme Weather, Health, and Communities. Extreme Weather and Society. Springer, Cham. https://doi.org/10.1007/978-3-319-30626-1_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-30626-1_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-30624-7
Online ISBN: 978-3-319-30626-1
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)