
Abstract
Patient presenting following the incidental detection of a 9 mm nodule at the pancreatic tail. 68Ga-DOTA-NOC PET/CT documented a focal area of uptake (red arrow) in the nodule confirming its neuroendocrine nature
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Patient presenting following the incidental detection of a 9 mm nodule at the pancreatic tail. 68Ga-DOTA-NOC PET/CT documented a focal area of uptake (red arrow) in the nodule confirming its neuroendocrine nature
68Ga-DOTA-peptide PET/CT imaging is accurate for the characterisation of even very small well differentiated neuroendocrine lesions.

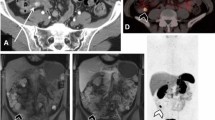
68Ga-DOTA-NOC PET/CT images of a patient studied for staging of a NEN of the pancreatic tail. PET/CT confirmed the primary lesion (white arrow) and multiple secondary lesions (nodes, liver, bone; red arrows). Pathology on surgical sample documented a G1 disease
PET/CT provides accurate staging (T,N,M) of well differentiated NEN.

68Ga-DOTA-NOC PET/CT images showing multiple areas of tracer pathological uptake in the left breast (red arrow) of a patient with multifocal breast NEN
Neuroendocrine differentiation in other solid tumours may occur. 68Ga-DOTA-NOC PET/CT may provide data on SSTR expression.

68Ga-DOTA-NOC PET/CT images showing multiple focal areas of tracer pathological uptake (red arrows) in a patient with paraganglioma
68Ga-DOTA-NOC is accurate to study patients with paraganglioma, providing data on somatostatin receptor expression and on disease localization in the whole body.

History:
2007: breast carcinoma (surgery + chemo-/radiotherapy).
August 2010: surgical resection of ileum NEN (G2) followed by 68Ga-DOTA-NOC PET/CT (30/09/2010), negative.
The patient was followed up by CT (every 3 months in the first year and once a year afterwards). 2012: at 2 years after primary surgery, CT documented disease relapse at liver level, and 68Ga-DOTA-NOC PET/CT (24/09/2012) showed a focal pathological area at the fifth segment (SUVmax = 9, red arrow). The patient was addressed to surgical resection of the single liver lesion
68Ga-DOTA-NOC PET/CT is accurate for the detection of relapse.

History (same patient as previous image):
2007: breast carcinoma (surgery + chemo-/radiotherapy).
2010: surgical resection of ileum NEN (G2) followed by 68Ga-DOTA-NOC PET/CT (30/09/2010): negative.
2012: relapse at liver level. Surgical resection of the single liver lesion.
2015: After 5 years of the ileal NEN primary tumour resection, a follow-up 68Ga-DOTA-NOC PET/CT showed a multifocal relapse (red arrows) undetected by CT
NEN patients may relapse a long time after primary surgery. 68Ga-DOTA-NOC PET/CT can identify relapse undetected by CT.

History: patient with HCC, incidental CT-detection (images not shown) of a hypervascularised duodenal nodule of suspicious NE nature. 68Ga-DOTA-NOC PET/CT showed a focal area of tracer uptake of unclear anatomical localization (red arrow)

History: patient with HCC, incidental CT-detection (images not shown) of a hypervascularised duodenal nodule of suspicious NE nature.
68Ga-DOTA-NOC PET/CT showed a focal area of tracer uptake of unclear anatomical localisation (a, standard 60 min acquisition). Delayed images (b) showed a clear projection on the duodenum. Arrows indicate sites of disease
68Ga-DOTA-peptide PET/CT delayed imaging may be useful for better localisation of equivocal imaging findings at standard acquisition time.

68Ga-DOTA-NOC PET/CT of a patient studied for follow-up of an ileal NET showing a diffuse uptake at the head of the pancreas on one occasion (a; February 2009) that disappeared at the subsequent follow-up scan (b; June 2009)
Diffuse non-pathologic 68Ga-DOTA-peptides uptake at the pancreatic head may be encountered and may be transient in the same patient.

68Ga-DOTA-NOC MIP and transaxial images of a patient presenting with dyspepsia. CT showed the presence of a solid hypervascularised nodule (14 × 15 mm) at the head of the pancreas. 68Ga-DOTA-NOC PET/CT showed that the nodule presented an elevated expression of somatostatin receptors. Arrows indicate sites of disease
Although the head of the pancreas can present a faint diffuse non-pathologic uptake, in the presence of a nodule with increased uptake of the 68Ga-DOTA-peptide, the presence of disease should be suspected.

Patient with unknown primary tumour (neuroendocrine tumour assessed on pathology of an excised liver lesion). 68Ga-DOTA-NOC PET/CT documented an area of focal tracer uptake at ileal level suggestive for primary tumour site
68Ga-DOTA-peptides imaging can be useful to detect the unknown primary tumour site in patients with documented neuroendocrine secondary lesions.

Patient presenting with neuroendocrine liver lesions (G2) but unknown primary site. 68Ga-DOTA-NOC PET/CT showed only faint uptake at bone level (posterior arch of C2, images not shown), while liver lesions were negative (a). On low-dose CT images, a lung nodule was detected (b). On the basis of these findings, an 18F-FDG PET/CT scan was performed (see next panel). Arrows indicate sites of disease
In patients with NEN presenting lesions without significant somatostatin receptor expression, 18F-FDG PET/CT should be considered as additional examination.

Patient presenting with neuroendocrine liver lesions (G2) but unknown primary site (same patient as previous panel). 18F-FDG PET/CT was performed to evaluate the 68Ga-DOTA-NOC/negative lesions (a). 18F-FDG (b) documented a hypermetabolic lung nodule (compatible with the primary site; red arrow) and metastatic lesions (liver, bone)
In patients with NEN secondary lesions and unknown primary, 18F-FDG PET/CT may provide valuable information on primary site in cases with undifferentiated tumours.

Patient presenting with neuroendocrine liver lesions (G2) but unknown primary site (same patient as previous panel). 68Ga-DOTA-NOC (a) and 18F-FDG transaxial images (b) comparison. 18F-FDG PET/CT-detected multiple pathological and focal areas of uptake at the right lung (primary) and at liver and bone level
Although generally well differentiated, undifferentiated NET may be encountered, are clinically more aggressive and generally show preferential 18F-FDG uptake.

18F-FDG (a) and 68Ga-DOTA-NOC (b) PET/CT images of a patient with pancreatic (tail) NET with multiple secondary lesions (nodes, liver, lung, peritoneal carcinomatosis) showing some lesions with a cold core area employing both tracers
A cold central lesion area may be encountered in both 68Ga-DOTA-NOC and 18F-FDG PET/CT images, especially in large lesions representing necrosis (in case of concordant findings). It must also be mentioned that in some cases a lesion with a peripheral rim and a cold core at 68Ga-DOTA-NOC PET/CT may present with 18F-FDG uptake only in the 68Ga-DOTA-peptide-negative area; in this case disease differentiation should be suspected.

18F-FDG PET/CT images of a patient with a lung NET (ki67 = 70 %) showing multiple areas of tracer pathologic uptake
Although most NEN are well differentiated, aggressive forms showing FDG avidity are encountered. High-grade tumours show preferential FDG uptake.

68Ga-DOTA-NOC images of a patient with pancreatic metastatic NEN and liver metastasis studied before (a; February 2013) and after PRRT (b; September 2013). PRRT induced a reduction in lesions number, size, and uptake (SUVmax before PRRT = 37, SUVmax after PRRT = 13)
68Ga-DOTA-peptides uptake correlates with SSTR expression and is useful to select candidate patients for PRRT. 68Ga-DOTA-peptides PET/CT is also useful to guide further treatment planning after PRRT.

68Ga-DOTA-NOC PET/CT images of a patient studied before (a, c) and after (b, d) PRRT showing disease progression
Although ideally a metabolic tracer should be employed to assess disease after therapy, correlating with SSTR expression, 68Ga-DOTA-peptides may be useful to guide further treatment planning.

18F-DOPA images of a patient with a clinically suspected pheochromocytoma, showing intense and focal uptake at right adrenal level
18F-DOPA is accurate for the detection of pheochromocytoma lesions (on the contrary 68Ga-DOTA-peptides have shown suboptimal sensitivity due to the generally low/variable expression of somatostatin receptors)

Patient presenting with abrupt onset of otherwise unexplained hypertension and a CT-detected abdominal mass. 18F-FDG confirmed the presence of a voluminous adrenal lesion presenting an increased and heterogeneous uptake (SUVmax = 20), suggestive for a highly aggressive pheochromocytoma lesion
Although pheochromocytoma may be well differentiated, aggressive undifferentiated forms can be encountered and show a preferential 18F-FDG uptake.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Ambrosini, V., Fanti, S. (2016). Neuroendocrine Tumours Pictorial Atlas. In: Ambrosini, V., Fanti, S. (eds) PET/CT in Neuroendocrine Tumors. Clinicians’ Guides to Radionuclide Hybrid Imaging(). Springer, Cham. https://doi.org/10.1007/978-3-319-29203-8_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-29203-8_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-29202-1
Online ISBN: 978-3-319-29203-8
eBook Packages: MedicineMedicine (R0)