
Abstract
This chapter includes definitions and diagnosis of early pregnancy complications (including spontaneous abortion, early pregnancy failure, threatened or incomplete abortion, septic abortion, and molar pregnancy). Management of these conditions is discussed, with particular emphasis on septic abortion—a potentially life-threatening condition that requires expedient surgical management.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Spontaneous abortion
- Threatened abortion
- Complete abortion
- Incomplete abortion
- Early pregnancy failure
- Molar pregnancy
- Septic abortion
Definitions
Spontaneous Abortion
Also known as a miscarriage , or early pregnancy loss, it occurs in pregnancies less than 20 weeks of gestational age. Up to 20 % of clinically recognized pregnancies will end in miscarriage [1]. Approximately 50 % of spontaneous pregnancy losses are due to chromosomal abnormalities [2]. Risk factors for spontaneous abortion include, but are not limited to, maternal age greater than 35 years, antiphospholipid antibody syndrome, congenital uterine anomalies, uncontrolled diabetes or thyroid disease, low body mass index, obesity, smoking, and prior miscarriages [3–6]. In women with three or more prior miscarriages, the risk of miscarriage is greater than 40 % [7].
Early Pregnancy Failure
The failure of a pregnancy to continue to develop normally. This term is often used interchangeably with the term “missed abortion,” which technically means a pregnancy that has been demised and retained for weeks [8]. Given the early and accurate diagnosis of most pregnancy failures, the term “missed abortion” seldom applies anymore. Most early pregnancy criteria are diagnosed by ultrasound findings; see the “Diagnosis” section below.
Threatened Abortion
Vaginal bleeding , often light to moderate and without passage of tissue, in a pregnancy prior to 20 weeks of gestation, in a patient with a closed cervix.
Inevitable Abortion
Bleeding and cramping in pregnancy prior to 20 weeks of gestation without passage of any products of conception, with an open cervix.
Incomplete Abortion
Some but not all products of conception have passed spontaneously, but retained products—usually fragments of the placenta—remain.
Complete Abortion
The patient has completely passed all products of conception without any interventions; the cervix is closed.
Septic Abortion
An infection of the upper genital tract following any type of abortion [9]. Patients may present with pain, fever, vaginal discharge or bleeding, and uterine tenderness on physical examination. Broad-spectrum antibiotic coverage and expeditious surgical evacuation are crucial, as patients can quickly become severely septic [10].
Molar Pregnancy
Nonviable pregnancies occurring in less than 0.1 % of gestations, resulting from abnormal fertilization [11]. Also called hydatidiform moles, molar pregnancies are classified as complete (with no fetal parts) or partial (with fetal parts) [12, 13]. Approximately 20 % of molar pregnancies are complicated by persistent trophoblastic tissue; most cases are nonmetastatic proliferations, though invasive moles and metastases can develop [14, 15]. The risk for persistent trophoblastic disease after a molar pregnancy is significantly higher following a complete molar pregnancy (20 %) as compared to partial molar pregnancy (5 %); risk factors also include age greater than 40 years, an enlarged uterus, presence of theca lutein cysts, and elevated serum beta-human chorionic gonadotropin (hCG) (over 50,000 milli-international units per milliliter, mIU/mL) [15–17].
When You Get the Call
Ask for a full set of vital signs, and request a pelvic ultrasound if one has not already been performed, if the patient is sufficiently stable.
When You Arrive
Review the patient’s vital signs in detail to assess for evidence of septic physiology or anemia, including tachycardia and hypotension. For immediate management of sepsis , please see Chap. 1, Acute Pelvic Pain, and, for hemorrhage, see Chap. 2, Vaginal Hemorrhage. If possible, review the medical record to verify whether an intrauterine pregnancy has been confirmed in this patient prior to her presentation.
History
Ask the patient for the date of her last menstrual period and whether she has had any bleeding or complications during this pregnancy prior to her current presentation. Review whether an intrauterine pregnancy had been confirmed prior to her presentation. Ask the patient to describe the onset and severity of her symptoms; if she is bleeding, inquire how often she is changing her pads. A patient report of soaking two maxi pads per hour for 2 h is a rough estimate of excessive bleeding. Ask about associated symptoms, including fever. If the patient had already been diagnosed with a spontaneous abortion prior to her current presentation, review when and how the diagnosis was made and whether she received any treatment or interventions.
Review the patient’s obstetrical history in detail, including prior deliveries, ectopic pregnancies, or miscarriages. The patient’s medical history should be reviewed, including hypertension and asthma (both of which limit the use of some uterotonic medications), bleeding diathesis and use of anticoagulant medications, as well as her surgical history.
Physical Examination
An abdominal examination should be performed to assess the patient’s tenderness, noting the presence of peritoneal signs, including rebound (pain with abdominal pressure is quickly withdrawn) or involuntary guarding. While women having a miscarriage may have uterine cramping, acute abdominal tenderness may indicate another process, such as infection or blood in the peritoneal cavity.
A speculum exam should be performed to assess the amount of vaginal bleeding; wall suction, available in most emergency room examination areas, may be helpful in patients with copious bleeding. Any products of conception visualized at the cervical os should be removed with a ring forceps and sent to pathology for confirmation. Of note, if the tissue cannot be easily extracted, abort efforts to remove it; this tissue could represent a cervical implantation or abnormally adherent placental tissue, and extraction could lead to severe hemorrhage. A bimanual exam should be performed to assess whether the cervix is open (indicating spontaneous or inevitable abortion).
Diagnosis
The diagnosis of a spontaneous abortion is made using a combination of the patient’s history, physical examination, and imaging. All pregnant patients with vaginal bleeding and pain should have a blood type, antibody screen, and complete blood count checked; in patients known or suspected to be in the first trimester, a serum hCG should also be obtained.
Transvaginal ultrasound is crucial to the assessment of patients with possible spontaneous abortion. The diagnosis of a spontaneous abortion should begin with confirmation of an intrauterine pregnancy, either by an earlier ultrasound this pregnancy or during a patient’s current presentation, by visualization of a yolk sac or fetal pole on imaging [18]. Without either of these, the patient has a pregnancy of unknown location. Please see Chap. 3, Pregnancy of Unknown Location and Ectopic Pregnancy, Fig. 3.1, for a flowchart of the diagnosis of patients with positive serum hCG and pain and/or bleeding.

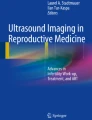
Complete hydatidiform mole. Grayscale (a) and power Doppler (b) sonographic images demonstrate cystic spaces within the endometrial cavity with increased vascularity (arrowheads). No fetus or gestational sac is seen (Reprinted from Shanbhogue et al. [12], with permission from Elsevier)
Absence of a Confirmed Intrauterine Pregnancy
Patients with spontaneous abortions and ectopic pregnancies may present similarly with bleeding and pain. A patient with a positive pregnancy test without documentation of an intrauterine pregnancy, particularly those presenting with bleeding and/or pain, should be considered at risk of an ectopic pregnancy. In hemodynamically stable patients, a repeat hCG is checked in 2 days to establish the hCG trajectory. Please refer to Chap. 3, Pregnancy of Unknown Location and Ectopic Pregnancy, for a discussion of hCG trends and diagnosing pregnancy location. Of note, the proposed hCG trends for differentiating intrauterine, ectopic and failing pregnancies are guidelines only, and deviations are often observed; hCG trends should be correlated with the patient’s clinical findings.
Septic Abortion
A septic abortion is diagnosed in any pregnant patient at less than 20 weeks of gestational age, with a fever over 38 °C (100.4 °F) not attributable to any source other than intrauterine contents. Patients may also have abdominal pain, particularly fundal tenderness. Of note, in patients undergoing medical management of an early pregnancy failure, fevers in the first 24 h may be related to administration of prostaglandin analogs such as misoprostol, but infection must be ruled out regardless [19].
Diagnostic criteria of sepsis are shown in Table 8.1 [20, 21]. In patients with fever or otherwise concerning for infection, a complete blood count should be obtained to assess for leukocytosis and bandemia, which are indicative of infection. In patients with temperatures over 101 °F, blood and urine cultures should be obtained. In patients with signs of sepsis, electrolytes, creatinine, liver function tests, a blood type and antibody screen, coagulation studies (prothrombin time (PT), activated partial thromboplastin time (aPTT) and fibrinogen), and a lactate level should be ordered. Consider an arterial blood gas if the patient is in distress. Nucleic acid amplification testing (NAAT) of a cervical swab for Neisseria gonorrhoeae and Chlamydia trachomatis can also be helpful. A pelvic ultrasound can help clarify whether a patient has any possible retained intrauterine products of conception, which require evacuation if septic abortion is suspected.
Hemorrhage
Recognition of severe hemorrhage is crucial, and resuscitation should begin alongside diagnosis. Diagnostic criteria of hemorrhagic shock are shown in Table 8.2 [22]. Patients with hemorrhage must have a complete blood count, blood type and antibody screen, coagulation studies and a fibrinogen level ordered. Coagulation factors and fibrinogen may become abnormal due to excessive blood loss.
Early Pregnancy Failure
Early pregnancy failure can be diagnosed according to strict ultrasonographic guidelines. Ultrasound criteria of early pregnancy failure include (1) gestational sac at least 25 millimeters (mm) in diameter without an embryo (also called an anembryonic pregnancy), (2) an embryo with a crown rump length of 7 mm or more without fetal heart activity, (3) no fetal heart activity 11 days or more after an ultrasound showing a gestational sac with a yolk sac, and (4) no fetal heart activity 14 days or more after an ultrasound showing a gestational sac without a yolk sac [23].
Threatened Abortion
In patients presenting with a threatened abortion and ultrasound evidence of an intrauterine pregnancy, certain ultrasound findings can increase a clinician’s concern for impending spontaneous abortion. A slow fetal heart rate in the first trimester confers an increased risk of spontaneous abortion. A fetal heart rate of less than 100 beats per minute up to 6.2 weeks of gestation and a fetal heart rate below 120 beats per minute from 6.3 to 7 weeks of gestation are associated with an increased risk of demise [24]. Subchorionic hematoma, which appears as a hypoechoic area behind the gestational sac, is associated with double the risk of spontaneous abortion; subchorionic hematomas are also associated with an increased risk of preterm premature rupture of membranes, placental abruption, and stillbirth [25].
Incomplete and Complete Abortion
The diagnosis of an incomplete or complete abortion is reserved for patients with a confirmed intrauterine pregnancy; otherwise, the patient technically has a pregnancy of unknown location. The differentiation between incomplete and complete abortion can be challenging. Patients who have undergone complete abortion usually report cramping and heavy bleeding with passage of tissue, followed by vast improvement or resolution of their vaginal bleeding by the time of assessment.
The use of ultrasound to differentiate complete from incomplete abortion, by assessing for retained products of conception, is controversial, as ultrasounds have a false-positive rate of 34 % for retained products of conception, and Doppler flow may be present in the endometrial linings of patients who do not ultimately have retained products of conception [26, 27]. The endometrial lining may not be significantly thicker in patients with incomplete versus complete abortions, though the presence of hyperechoic material in the endometrial lining is suggestive of retained products of conception [28].
Given the limitations of ultrasound, management should be guided by the patient’s symptoms. Patients with prolonged and heavy bleeding are more likely to have retained products of conception; no strict guidelines exist, but bleeding that soaks two or more maxi pads per hour or that lasts more than 3 weeks may be indicative of retained products of conception. Abdominal pain is not correlated with retained products of conception [28].
Molar Pregnancy
Molar pregnancy commonly presents with vaginal bleeding and elevated hCG [14]. As diagnosis is increasingly made in the first trimester, more extreme symptoms of enlarged uterine size, hyperthyroidism, hyperemesis, and respiratory distress are less common [16].
In patients with the diagnosis of molar pregnancy suggested by imaging or clinical presentation, a complete blood count, blood type and antibody screen, clotting studies, liver and renal function testing, and chest radiograph should be obtained [15]. Less than 50 % of molar pregnancies are detected by ultrasound prior to evacuation, and the remainder is only diagnosed by pathologic analysis of uterine contents following uterine evacuation for a presumed early pregnancy failure or incomplete abortion [30]. Rates of detection by ultrasound are higher for complete molar pregnancies than partial molar pregnancies [30]. The classic ultrasound appearance of a complete mole is the “cluster of grapes” or “snowstorm” finding (Fig. 8.1) [12]. By ultrasound, a partial mole may have less cystic degeneration of the placenta, and a gestational sac or embryo may be visible (Fig. 8.2) [12].

Partial hydatidiform mole. Grayscale sonographic images of the uterus demonstrate cystic changes within the placenta (arrowhead in a) and an abnormal nonviable fetus (arrows in a and b) (Reprinted from Shanbhogue et al. [12], with permission from Elsevier)
Management
All pregnant patients with vaginal bleeding and rhesus (Rh)-negative blood type should receive Rho(D) immune globulin to avoid isoimmunization.
Any patient without a confirmed intrauterine pregnancy should be assessed and closely followed for a possible ectopic pregnancy. Please see Chap. 3, Pregnancy of Unknown Location and Ectopic Pregnancy, for more information.
Antibiotic prophylaxis is generally recommended for patients requiring dilation and curettage in early pregnancy. Many antibiotics protocols exist, largely extrapolated from the surgical abortion literature, and there is insufficient evidence to support one over another. Ideally, antibiotic prophylaxis should be initiated preoperatively and used in the shortest possible course. Options for antibiotic prophylaxis include: (1) doxycycline 200 mg PO or IV preoperatively, or (2) azithromycin 1 g PO or IV and metronidazole 500 mg PO or IV preoperatively [29, 31, 32].
Hemorrhage
Particularly in patients with hemodynamic changes or estimated blood loss of 500 mL or more, resuscitation efforts should begin immediately with crystalloid and packed red blood cells as necessary, in parallel with operative planning. Please see Chap. 13, Preparing for Urgent or Emergent Surgery, for further information on resuscitation and blood products.
Patients with clinically significant hemorrhage , particularly unstable vital signs, should be managed with urgent dilation and curettage. Uterotonics can be administered to limit blood loss, shown in Table 8.3 [33–37]. Furthermore, while preparing to proceed to the operating room, uterine tamponade can be established by gently introducing a Foley catheter or Bakri® balloon (Cook Medical, Bloomington, IN) into the uterus using a ring forceps [34, 38, 39]. A 30 mL Foley catheter can be inflated with up to 60 mL of normal saline, while a Bakri balloon can hold 500 mL, which is often too large for the uterine cavity following a first trimester spontaneous abortion [40]. Uterine tamponade can also be applied postoperatively in patients with persistent bleeding. If tamponade is curative, the balloon can stay in place for 12–24 h, with or without uterotonics and antibiotics [40].
If bleeding continues despite dilation and curettage and uterine tamponade, patients may require additional interventions, including uterine artery embolization (UAE), laparoscopy, laparotomy, or rarely hysterectomy. UAE, performed by interventional radiology, has been used with great success to treat postabortion complications including atony and abnormal placentation [42]. UAE involves the cannulation of the femoral artery followed by catheter-guided delivery of embolic particles to the uterine arteries. UAE is a relatively low-risk and well-tolerated procedure, though it can result in significant cramping and fevers; complications include groin puncture site infection or hematoma, contrast allergy, arterial trauma, or accidental embolization of nontarget vessels [41]. If interventional radiology is not available, surgical intervention may rarely be required, including hypogastric artery ligation and/or hysterectomy [43, 44].
Please see Chap. 2, Vaginal Hemorrhage, for more information on the diagnosis and management of vaginal hemorrhage.
Septic Abortion
In pregnant patients with signs of sepsis and the history, physical exam, labs and imaging reveal no source of infection other than the uterus, resuscitation must begin quickly while mobilizing resources to proceed to the operating room for uterine evacuation. Please refer to Chap. 1, Acute Pelvic Pain, for more information on the management of sepsis. If a patient is septic and hemodynamically unstable, with the uterus being the most likely source of infection, patients may rarely have to go to the operating room for evacuation and potentially other exploratory procedures following an abbreviated assessment and without imaging. Delayed uterine evacuation places patients at risk of worsening sepsis and death [45]. Patients may require further surgery , including hysterectomy, for failure to respond to antibiotics, abscess, or necrotizing pelvic infections. Please see Chap. 16, Complications of Minimally Invasive Gynecologic Surgery, for more information on necrotizing infections.
The patient should receive crystalloid resuscitation , with goals of a central venous pressure of 8–12 mmHg; mean arterial pressure of at least 65 mm of mercury (Hg); urine output of greater than 0.5 mL/kg/h; normalized lactate level; and hemoglobin level of 7–9 g per deciliter (dL) [21]. Repeat a lactate and any other lab values as indicated (such as CBC and coagulation studies in a patient with DIC) during resuscitation to assess progress.
Intravenous broad-spectrum antibiotics should be started within an hour of presentation. A common regimen is ampicillin (2–3 g IV every 6 h), clindamycin (900 mg IV every 8 h), and gentamicin (2 mg/kg IV one time, followed by 1.5 mg/kg IV every 8 h). Another option is ampicillin-sulbactam, 3 g IV every 6 h [46]. Tissue obtained from any uterine evacuation should be sent for culture to direct antibiotic selection.
In patients who present with fever after complete abortion or prior surgical evacuation, with neither significant symptoms (vaginal hemorrhage or pain) nor pelvic ultrasound findings concerning for retained products of conception, treatment for mild endometritis can be initiated. Options include amoxicillin-clavulanic acid (875 mg PO every 12 h) alone or amoxicillin (500 mg PO every 8 h) plus metronidazole (500 mg PO every 8 h) [47]. Clindamycin can also be given orally (600 mg every 6 h), and gentamicin can be given intramuscularly (4.5 g every 24 h), which is less convenient but feasible if no other options are available. Of note, chlamydia and gonorrhea are not addressed by this regimen, and testing for these bacteria should be sent [48].
Molar Pregnancy
Patients with molar pregnancies require surgical evacuation by uterine curettage; hysterectomy is an alternative for patients who are done with childbearing [15]. In patients who undergo uterine curettage, contraception is vital to prevent a new pregnancy during the post-procedural monitoring period.
Following uterine evacuation or hysterectomy, serial serum hCG measurements are vital to monitoring for persistent trophoblastic disease. Serum hCG levels should be obtained each week until levels are negative for 3 weeks, followed by monthly testing for 6 months [14]. An abnormal hCG trend requiring further assessment is defined as a plateau—four sequential hCG levels within 10 % of one another—an increase of 10 % or more of three sequential values, or detectable serum hCG more than 6 months after evacuation [49].
Complete Abortion
In patients with prior confirmed intrauterine pregnancies and without signs of infection following their complete abortions, no further management is commonly necessary. Patients with suspected complete abortions without documentation of intrauterine pregnancies should be carefully counseled and followed for pregnancies of unknown location. Please see Chap. 3, Pregnancy of Unknown Location and Ectopic Pregnancy, for more information. Patients should be counseled that they may have bleeding for several weeks following a complete abortion and to follow up with their continuity providers.
Incomplete Abortion and Early Pregnancy Failure
Patients with a retained failed early pregnancy or an incomplete abortion, and without evidence of infection or hemorrhage may elect for expectant, medical, or surgical management. The relative success rates of these options are shown in Table 8.4 [50, 51]. The rate of infection is low (2–3 %) and similar among all three methods. The rate of unplanned hospital admission and dilation and curettage is higher in patients pursuing expectant or medical management.
Expectant Management
Expectant management can be considered in women without signs of infection at less than 14 weeks of gestational age [52]. Expectant management can be attempted for 4 weeks, after which intervention is generally recommended. Failed expectant management is suspected in patients who do not report heavy menses; ultrasound may provide additional supporting evidence (particularly if an intrauterine gestational sac is still identified). Patients who successfully pass a failed pregnancy should be counseled that light bleeding may persist for over 2 weeks; bleeding is a few days shorter in duration in patients electing for medical or surgical interventions [53].
Medical Management
Medical management is performed with misoprostol, a prostaglandin analog, which leads to uterine contractions that expel the gestational tissue. Medical management of an incomplete abortion or early pregnancy failure without hospital admission is generally recommended in women at less than 10 weeks of gestational age, largely extrapolated from the elective abortion literature [54]. Contraindications include high clinical suspicion for ectopic pregnancy, current use of an intrauterine device (IUD), long-term corticosteroid use, adrenal insufficiency, coagulopathy or anticoagulant therapy, significant anemia (usually defined as a hemoglobin of less than 9.5 or 10 g/dL), misoprostol allergy, and inability to follow up [55]. Patients should be counseled that misoprostol leads to painful cramping and heavy vaginal bleeding and can also result in nausea and vomiting, diarrhea, and headache [56]. Misoprostol can be associated with fevers of greater than 38 °C (100.4 °F) in 40 % of women without other signs of infection, particularly in the first 24 h, though patients should be assessed for infection regardless [19].
Several misoprostol regimens are used; the World Health Organization recommends misoprostol 800 μg vaginally or 600 μg sublingually for missed abortions and 600 μg orally for incomplete abortions [56, 57–59]. Patients should be counseled to call their providers if significant vaginal bleeding and passage of tissue have not occurred in 24–48 h. The addition of mifepristone confers no advantage in the medical management of early pregnancy failure [60].
Surgical Management
For patients with signs of infection or clinically significant hemorrhage, or who prefer surgical management, dilation and curettage is performed. Suction curettage is preferable to sharp curettage [61]. Antibiotic prophylaxis is recommended for patients undergoing dilation and curettage for spontaneous abortion, though there is insufficient evidence to recommend any one of the proposed regimens. Prophylaxis should be initiated preoperatively and used in the shortest possible course. Options include: (1) doxycycline 200 mg PO or IV preoperatively or (2) azithromycin 1 g PO or IV and metronidazole 500 mg PO or IV preoperatively [29, 31, 32].
Follow-Up
Following any type of spontaneous abortion, patients should be counseled to observe pelvic rest—meaning no intercourse, douching, or use of tampons—for 2 weeks, in order to avoid infection. Patients should be counseled to follow up with their continuity providers within 2–4 weeks, to monitor their postabortion symptoms, and to discuss contraception and future pregnancy planning. No clear guidelines exist regarding a recommended interval to attempting conception. The common advice to wait 3 months before attempting conception may be excessive, as recent research does not show an increase in adverse outcomes in patients conceiving within 3 months of a spontaneous loss [62].
References
Everett C. Incidence and outcome of bleeding before the 20th week of pregnancy: prospective study from general practice. BMJ. 1997;315:32–4.
Eiben B, Bartels I, Bähr-Porsch S, Borgmann S, Gatz G, Gellert G, et al. Cytogenetic analysis of 750 spontaneous abortions with the direct-preparation method of chorionic villi and its implications for studying genetic causes of pregnancy wastage. Am J Hum Genet. 1990;47:656–63.
Feodor Nilsson S, Andersen P, Strandberg-Larsen K, Nybo Andersen AM. Risk factors for miscarriage from a prevention perspective: a nationwide follow-up study. BJOG. 2014;121:1375–85.
Maconochie N, Doyle P, Prior S, Simmons R. Risk factors for first trimester miscarriage–results from a UK-population-based case–control study. BJOG. 2007;114:170–86.
Cramer DW, Wise LA. The epidemiology of recurrent pregnancy loss. Semin Reprod Med. 2000;18:331–9.
Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98:1103–11.
Regan L, Braude PR, Trembath PL. Influence of past reproductive performance on risk of spontaneous abortion. BMJ. 1989;299:541–5.
Hoffman BL, Schorge JO, Schaffer JI, Halvorson LM, Bradshaw KD, Cunningham F, et al. Chapter 6. First-trimester abortion. In: Hoffman BL, Schorge JO, Schaffer JI, Halvorson LM, Bradshaw KD, Cunningham F, Calver LE, editors. Williams gynecology. 2nd ed. New York: McGraw-Hill; 2012. http://accessmedicine.mhmedical.com.ezp-prod1.hul.harvard.edu/content.aspx?bookid=399&Sectionid=41722294. Accessed 1 Sep 2015.
Lapinsky SE. Obstetric infections. Crit Care Clin. 2013;29:509–20.
Stubblefield PG, Grimes DA. Septic abortion. N Engl J Med. 1994;331:310–4.
Semer DA, Macfee MS. Gestational trophoblastic disease: epidemiology. Semin Oncol. 1995;22:109–12.
Shanbhogue AK, Lalwani N, Menias CO. Gestational trophoblastic disease. Radiol Clin North Am. 2013;51:1023–34.
Berkowitz RS, Goldstein DP. Chorionic tumors. N Engl J Med. 1996;335:1740–8.
Berkowitz RS, Goldstein DP. Clinical practice. Molar pregnancy. N Engl J Med. 2009;360:1639–45.
Soper JT, Mutch DG, Schink JC, American College of Obstetricians and Gynecologists. Diagnosis and treatment of gestational trophoblastic disease: ACOG Practice Bulletin No. 53. Gynecol Oncol. 2004;93:575–85.
Morrow CP. Postmolar trophoblastic disease: diagnosis, management, and prognosis. Clin Obstet Gynecol. 1984;27:211–20.
Niemann I, Petersen LK, Hansen ES, Sunde L. Predictors of low risk of persistent trophoblastic disease in molar pregnancies. Obstet Gynecol. 2006;107:1006–11.
Barnhart KT. Clinical practice. Ectopic pregnancy. N Engl J Med. 2009;361:379–87.
von Hertzen H, Piaggio G, Wojdyla D, Nguyen TM, Marions L, Okoev G, et al. Comparison of vaginal and sublingual misoprostol for second trimester abortion: randomized controlled equivalence trial. Hum Reprod. 2009;24:106–12.
Fischerova D. Urgent care in gynaecology: resuscitation and management of sepsis and acute blood loss. Best Pract Res Clin Obstet Gynaecol. 2009;23:679–90.
Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637.
Committee on Trauma. Advanced trauma life support 1 student manual. 8th ed. Chicago: American College of Surgeons; 2008.
Doubilet PM, Benson CB, Bourne T, Blaivas M; Society of Radiologists in Ultrasound Multispecialty Panel on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369:1443–51.
Doubilet PM, Benson CB. Embryonic heart rate in the early first trimester: what rate is normal? J Ultrasound Med. 1995;14:431–4.
Tuuli MG, Norman SM, Odibo AO, Macones GA, Cahill AG. Perinatal outcomes in women with subchorionic hematoma: a systematic review and meta-analysis. Obstet Gynecol. 2011;117:1205–12.
Sadan O, Golan A, Girtler O, Lurie S, Debby A, Sagiv R, et al. Role of sonography in the diagnosis of retained products of conception. J Ultrasound Med. 2004;23:371–4.
Achiron R, Goldenberg M, Lipitz S, Mashiach S. Transvaginal duplex Doppler ultrasonography in bleeding patients suspected of having residual trophoblastic tissue. Obstet Gynecol. 1993;81:507–11.
Abbasi S, Jamal A, Eslamian L, Marsousi V. Role of clinical and ultrasound findings in the diagnosis of retained products of conception. Ultrasound Obstet Gynecol. 2008;32:704–7.
American College of Obstetricians and Gynecologists. ACOG practice bulletin No. 104: antibiotic prophylaxis for gynecologic procedures. Obstet Gynecol. 2009;113:1180–9.
Fowler DJ, Lindsay I, Seckl MJ, Sebire NJ. Routine pre-evacuation ultrasound diagnosis of hydatidiform mole: experience of more than 1000 cases from a regional referral center. Ultrasound Obstet Gynecol. 2006;27:56–60.
Achilles SL, Reeves MF, Society of Family Planning. Prevention of infection after induced abortion. Contraception. 2011;83:295–309.
Royal College of Obstetricians and Gynaecologists. The care of women requesting induced abortion: summary. Evidence-based clinical guideline number 7. London: RCOG Press; 2011. https://www.rcog.org.uk/globalassets/documents/guidelines/abortion_guideline_summary.pdf. Accessed 22 Sept 2015.
O'Connell K, Jones H, Simon M, Saporta V, Paul M, Lichtenberg E. First-trimester surgical abortion practices: a survey of National Abortion Federation members. Contraception. 2009;79:385–92.
American College of Obstetricians and Gynecologists. ACOG Practice Bulletin: postpartum hemorrhage. Obstet Gynecol. 2006;108:1039–47.
Nygaard IH, Valbø A, Heide HC, Kresovic M. Is oxytocin given during surgical termination of first trimester pregnancy useful? A randomized controlled trial. Acta Obstet Gynecol Scand. 2011;90:174–8.
Meckstroth K, Whitaker A, Bertisch S, Goldberg A, Darney P. Misoprostol administered by epithelial routes: drug absorption and uterine response. Obstet Gynecol. 2006;108:582–90.
Cunningham F, Leveno KJ, Bloom SL, Spong CY, Dashe JS, Hoffman BL, et al. Obstetrical hemorrhage. In: Cunningham F, Leveno KJ, Bloom SL, Spong CY, Dashe JS, Hoffman BL, Casey BM, Sheffield JS, editors. Williams obstetrics. 24th ed. New York: McGraw-Hill; 2013. http://accessmedicine.mhmedical.com.ezp-prod1.hul.harvard.edu/content.aspx?bookid=1057&Sectionid=59789185. Accessed 10 June 2015.
Kauff ND, Chelmow D, Kawada CY. Intractable bleeding managed with Foley catheter tamponade after dilation and evacuation. Am J Obstet Gynecol. 1995;173:957–8.
Olamijulo J, Doufekas K. Intrauterine balloon tamponade for uncontrollable bleeding during first trimester surgical termination of pregnancy. J Obstet Gynaecol. 2007;27:440–1.
Kerns J, Steinauer J. Management of postabortion hemorrhage: release date November 2012 SFP Guideline #20131. Contraception. 2013;87:331–42.
Katz MD, Sugay SB, Walker DK, Palmer SL, Marx MV. Beyond hemostasis: spectrum of gynecologic and obstetric indications for transcatheter embolization. Radiographics. 2012;32:1713–31.
Steinauer JE, Diedrich JT, Wilson MW, Darney PD, Vargas JE, Drey EA. Uterine artery embolization in postabortion hemorrhage. Obstet Gynecol. 2008;111:881–9.
Grimes DA, Flock ML, Schulz KF, Cates Jr W. Hysterectomy as treatment for complications of legal abortion. Obstet Gynecol. 1984;63:457–62.
Boynukalin FK, Boyar H, Gormus H, Aral AI, Boyar N. Bilateral hypogastric artery ligation in emergency setting for intractable postpartum hemorrhage: a secondary care center experience. Clin Exp Obstet Gynecol. 2013;40:85–8.
Wolman I, Gordon D, Yaron Y, Kupferminc M, Lessing JB, Jaffa AJ. Transvaginal sonohysterography for the evaluation and treatment of retained products of conception. Gynecol Obstet Invest. 2000;50:73–6.
Stiglich N, Alston M, Vanswam S. Optimizing treatment of intra-amniotic infection and early-onset postpartum endometritis: advantages of single-agent therapy. Perm J. 2011;15:26–30.
Meaney-Delman D, Bartlett LA, Gravett MG, Jamieson DJ. Oral and intramuscular treatment options for early postpartum endometritis in low-resource settings: a systematic review. Obstet Gynecol. 2015;125:789–800.
2015 STD Treatment Guidelines. Centers for Disease Control and Prevention website. http://www.cdc.gov/std/tg2015/2015-poster-press.pdf. Updated 4 June 2015. Accessed 10 June 2015.
Kohorn EI. The new FIGO 2000 staging and risk factor scoring system for gestational trophoblastic disease: description and critical assessment. Int J Gynecol Cancer. 2001;11:73–7.
Luise C, Jermy K, May C, Costello G, Collins WP, Bourne TH. Outcome of expectant management of spontaneous first trimester miscarriage: observational study. BMJ. 2002;324:873–5.
Zhang J, Gilles JM, Barnhart K, Creinin MD, Westhoff C, Frederick MM, National Institute of Child Health Human Development (NICHD) Management of Early Pregnancy Failure Trial. A comparison of medical management with misoprostol and surgical management for early pregnancy failure. N Engl J Med. 2005;353:761–9.
Nanda K, Lopez LM, Grimes DA, Peloggia A, Nanda G. Expectant care versus surgical treatment for miscarriage. Cochrane Database Syst Rev. 2012;3:CD003518.
Wieringa-de Waard M, Vos J, Bonsel G, Bindels P, Ankum W. Management of miscarriage: a randomized controlled trial of expectant management versus surgical evacuation. Hum Reprod. 2002;17:2445–50.
Winikoff B, Dzuba IG, Chong E, Goldberg AB, Lichtenberg ES, Ball C, et al. Extending outpatient medical abortion services through 70 days of gestational age. Obstet Gynecol. 2012;120:1070–6.
American College of Obstetricians and Gynecologists. Practice bulletin no. 143: medical management of first-trimester abortion. Obstet Gynecol. 2014;123:676–92.
American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 427: Misoprostol for postabortion care. Obstet Gynecol. 2009;113:465–8.
Blum J, Winikoff B, Gemzell-Danielsson K, Ho PC, Schiavon R, Weeks A. Treatment of incomplete abortion and miscarriage with misoprostol. Int J Gynaecol Obstet. 2007;99:S186–9.
Gemzell-Danielsson K, Ho PC, Gómez Ponce de León R, Weeks A, Winikoff B. Misoprostol to treat missed abortion in the first trimester. Int J Gynaecol Obstet. 2007;99:S182–5.
Neilson JP, Gyte GM, Hickey M, Vazquez JC, Dou L. Medical treatments for incomplete miscarriage. Cochrane Database Syst Rev. 2013;3:CD007223.
Stockheim D, Machtinger R, Wiser A, Dulitzky M, Soriano D, Goldenberg M, et al. A randomized prospective study of misoprostol or mifepristone followed by misoprostol when needed for the treatment of women with early pregnancy failure. Fertil Steril. 2006;86:956–60.
Verkuyl DA, Crowther CA. Suction v. conventional curettage in incomplete abortion. A randomised controlled trial. S Afr Med J. 1993;83:13–5.
Wong LF, Schliep KC, Silver RM, Mumford SL, Perkins NJ, YE A, et al. The effect of a very short interpregnancy interval and pregnancy outcomes following a previous pregnancy loss. Am J Obstet Gynecol. 2015;212:e1–11.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Brady, P.C., Pocius, K.D. (2016). Spontaneous Abortions. In: Handbook of Consult and Inpatient Gynecology. Springer, Cham. https://doi.org/10.1007/978-3-319-27724-0_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-27724-0_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-27722-6
Online ISBN: 978-3-319-27724-0
eBook Packages: MedicineMedicine (R0)