
Abstract
Long-term anticoagulation is often considered to be a relative contraindication to shunt surgery for patients with normal pressure hydrocephalus (NPH). While the overall risk of bleeding associated with shunt placement is low, the risk of bleeding in the elderly is increased, particularly with regard to immediate intracerebral hemorrhage or delayed subdural hematoma (SDH) during or after CSF shunting. Furthermore, NPH patients receiving antithrombotic therapy are at a significantly increased risk of hemorrhagic complication compared to patients who are not on antithrombotic therapy. Given the advanced age, gait impairment, and dementia associated with NPH, the bleeding and thrombotic risk may be even higher in NPH than the general population receiving antithrombotic therapy. Therefore, consultation with a hematologist and/or cardiologist is warranted in order to determine which patients can safely suspend antithrombotic therapy prior to surgery versus those who require bridging. Preoperatively, antiplatelet therapy should be stopped at least 7–14 days prior to surgery, whereas warfarin therapy should be stopped at least 5–7 days prior to surgery and/or bridged with a short-acting anticoagulant, in general. Operative considerations that can reduce the risk of hemorrhagic complication include incision of the pia mater prior to ventricular catheter insertion, potential use of intraoperative imaging guidance, and placement of an adjustable and gravity-assisted shunt valve to lower the risk of overdrainage. In the outpatient setting, gradual lowering of the pressure setting should be performed over time until a balance is reached between maximum symptomatic improvement and the onset of symptoms suggestive of low intracranial pressure (e.g., orthostatic headache and dizziness). Postoperatively, the time to resumption of antithrombotic therapy depends on the patients’ individual risk of thrombosis and bleeding as well as radiographic evaluation for intracranial hemorrhage. In summary, patients on long-term antithrombotic therapy can be safely and effectively evaluated and treated for NPH, with the use of appropriate perioperative and postoperative management.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- CSF shunting
- Antithrombotic therapy
- Intracerebral hemorrhage
- Subdural hematoma
- Normal pressure hydrocephalus
Introduction
Normal pressure hydrocephalus (NPH) is a common and treatable neurological disorder that often results in progressive gait impairment, urinary incontinence, and dementia in the context of ventricular enlargement with normal cerebrospinal fluid (CSF) opening pressure on lumbar puncture and absence of papilledema [1, 2]. NPH may be idiopathic or secondary to traumatic brain injury, subarachnoid hemorrhage, tumor, infection, or surgical complication [3]. While secondary NPH can occur at any age, idiopathic NPH (iNPH) typically affects individuals in their 60s and 70s [4]. Epidemiological data regarding NPH remains limited; however, based on studies from Scandinavia and Japan, the estimated incidence of NPH ranges from 5.5 to 120/100,000 persons per year, in patients above 70 years of age [5, 6]. According to five community-based studies, the overall prevalence of iNPH ranges from 0.12 % to 2.9 %, with a prevalence as high as 5.9 % in patients above 80 years of age [7].
CSF diversion is warranted in the majority of patients with symptomatic NPH and results in clinical improvement in up to 80–90 % of individuals [2]. As such, CSF shunting is the most commonly employed treatment for the long-term management of NPH. However, like all surgical interventions, CSF shunting carries a risk of both intraoperative and postoperative complications. Immediate complications include parenchymal injury and/or intracranial hemorrhage during catheter placement, and delayed complications include shunt obstruction, infection, subdural hygroma or hematoma, and shunt migration [8, 9]. Complications from hematologic causes can be particularly devastating in this group, given the aforementioned potential surgical complications and intrinsic or extrinsic patient-specific factors that can increase risk. iNPH typically occurs in the elderly and common cardiovascular comorbidities associated with thrombosis in this age group are prevalent, including: atrial fibrillation, valvular disease, ischemic heart disease, and deep venous thrombosis (DVT) . Likewise, Krauss et al. reported a significant association between NPH and diabetes mellitus (P < 0.015), as well as cardiac (P < 0.001), cerebral arteriosclerotic (P = 0.007), and other arteriosclerotic diseases (P = 0.001) [10]. Similarly, Eide and Pripp found a significantly increased prevalence of diabetes mellitus and cardiovascular diseases, such as arterial hypertension (males), angina pectoris (females and males), and cardiac infarction (males) in iNPH patients compared to healthy controls [11]. Patients with these cardiovascular diseases are commonly prescribed antithrombotic therapy (i.e., anticoagulant and/or antiplatelet) to reduce the risk of stroke. Moreover, long-term daily use of aspirin or anticoagulants is recommended for diabetic patients unless otherwise contraindicated, due to an increased risk of developing arterial disease (e.g., coronary artery, cerebrovascular and peripheral arterial disease) [12]. As such, many NPH patients presenting for shunt placement may have a history of long-term antithrombotic therapy.
Long-term anticoagulation is often considered to be a relative contraindication to shunt surgery for patients with NPH given serious concerns regarding the increased risk of anticoagulant-associated bleeding in the elderly, particularly with regard to immediate intracranial hemorrhage (ICH) or delayed subdural hematoma (SDH) during or after CSF shunting [13]. Furthermore, elderly patients often have additional concomitant physical and medical issues necessitating the use of multiple medications, such as antiplatelet drugs, that increase the interactions and risks associated with anticoagulant therapy. According to the National Center for Health Statistics’ Health, United States, 2013 report, 47.5 % of adults aged 65 and over were taking at least five or more drugs simultaneously between 2007 and 2010. Therefore, a careful assessment of the overall risk-benefit ratio associated with CSF shunting in anticoagulated NPH patients must be employed. While few studies have objectively explored the outcomes after shunt placement in anticoagulated NPH patients, the results of our previous study demonstrated that patients on long-term anticoagulant therapy using warfarin can be safely and effectively evaluated and treated for NPH [3].
In this chapter, we discuss the risks associated with CSF shunting in anticoagulated NPH patients, and review the evidence on management strategies to reduce the risk of hematologic morbidity related to CSF diversion in these patients.
Common Anticoagulants Encountered in the NPH Population
Diseases associated with thrombosis are more common in the elderly population, including those with NPH. Appropriate antithrombotic therapy effectively reduces morbidity and mortality due to stroke and thromboembolism, and is therefore warranted for many elderly patients. According to the National Center for Health Statistics’ Health, United States, 2013 report, 18.1 % of adults 65 years and older were using one or more anticoagulant and/or antiplatelet medication between 2007 and 2010, increased from 9.1 % between 1999 and 2002. Commonly used antithrombotic agents in this age group include: warfarin, heparin, direct factor Xa inhibitors (e.g., Rivaroxaban), direct thrombin inhibitors (e.g., Dabigatran), aspirin, and clopidogrel. Each agent has unique applications and risks that must be individually considered when encountering an anticoagulated NPH patient who presents for CSF shunting. However, an individual discussion surrounding the unique aspects of particular antithrombotic therapies is beyond the scope of this chapter, and consultation with a hematologist and/or cardiologist is encouraged prior to shunt placement.
Diagnostic Protocol for Patients on Anticoagulants
The efficacy of CSF shunting in patients with suspected NPH varies widely in the literature, with rates of clinical improvement ranging from 24 % to greater than 96 %; however, in appropriately selected patients, shunt insertion can result in significant improvement in the majority of patients with NPH, with low iatrogenic morbidity and mortality [14]. As such, several imaging techniques and invasive procedures, ranging from CSF drainage, to continuous intracranial pressure monitoring, to hydrodynamic study methods, can be utilized to improve diagnostic evaluation and predict response to CSF shunting [15]. Despite their utility, invasive diagnostic procedures carry a low, but important, risk of hemorrhagic complications, particularly in patients receiving antithrombotic therapy [16–18].
Gait impairment is the most common and often is the presenting symptom in patients with NPH [19]. The Timed Up and Go (TUG) and Tinetti Performance Oriented Mobility Assessment are often utilized to reliably and accurately measure functional outcomes related to gait [20]. In addition to monitoring gait outcomes after shunting, these assessments are valuable tools that can be used to assess falling risk in anticoagulated NPH patients, potentially predicting the risk of traumatic intracranial hemorrhage. More robust studies evaluating the ability of these noninvasive tests to predict the risk of a fall-related intracranial hemorrhage could be useful in stratifying patients that would benefit from increased prophylactic measures, irrespective of their NPH status.
Lumbar drainage , whether through a large volume tap or continuous drainage, can be used to determine whether a patient is likely to respond to CSF shunting. This modality is one of the preferred diagnostic interventions of choice used to assist surgeons in the evaluation of the risk-benefit ratio associated with shunt placement in NPH patients. However, it is important to note that in patients on concomitant anticoagulation therapy, anticoagulant-associated bleeding can occur due to lumbar puncture itself. While rare, hemorrhagic complications including epidural, subdural, and subarachnoid hemorrhage are serious potential side effects of lumbar puncture [21, 22]. For example, in 2004, Samdani et al. reported a case of a 34-year-old man, with a history of daily aspirin use for back pain, who experienced a subdural hematoma after diagnostic lumbar puncture [23]. Likewise, Paal et al. reported a case of spinal subarachnoid hemorrhage caused by diagnostic lumbar puncture in a 51-year-old patient on a daily combined regimen of aspirin and clopidogrel [24]. In 2005, Burger et al. performed a meta-analysis of randomized controlled trials regarding the discontinuation of aspirin prior to diagnostic or therapeutic interventions and, based on the evidence, concluded that aspirin should only be discontinued in cases where its continued use would be associated with a higher risk of mortality than the increased risk of vascular accident without it [25]. Likewise, the risk for hemorrhage after lumbar puncture is increased in patients using anticoagulants such warfarin, low molecular weight heparins, and direct factor Xa and thrombin inhibitors [18].
Intracranial pressure (ICP) monitoring may also be employed during the evaluation and treatment of NPH. In 2010, Eide et al. reported that improvement after surgery can be anticipated in 90 % of iNPH patients with abnormal ICP pulsatility, compared to 10 % of patients with normal ICP pulsatility, highlighting the utility of this invasive procedure in the diagnosis of NPH [26]. While the authors reported a low complication rate related to ICP monitoring, with no reports of hemorrhagic complication [26], other studies have reported low, but significant rates of intracranial hemorrhage associated with ICP monitoring via the gold standard procedure of external ventricular drain (EVD) placement . The rate of hemorrhagic complication associated with EVDs ranges from 0 % to 15 %, with two (0.6 %) deaths occurring in Karkala et al.’s study of the safety and accuracy of bedside EVD placement [17]. Of note, the rate of hemorrhage associated with EVD placement estimated in these studies is likely higher than in the general NPH population given the fact that the majority of patients had an EVD placed for emergent circumstances, such as subarachnoid hemorrhage, intracranial hemorrhage, and intraventricular hemorrhage in Karkala et al.’s study, while diagnostic EVD placement for NPH is generally an elective procedure. Therefore, complete reversal of anticoagulation in patients on antithrombotic therapy in these studies may not have been possible. Although the factors of this study do not match the NPH population, given the increased risk of bleeding in anticoagulated NPH patients, careful evaluation for evidence of potential hemorrhagic complication should be performed in patients who undergo diagnostic ICP monitoring.
Preoperative Anticoagulation Management Strategy: Complication Avoidance and Preoperative Considerations
Studies regarding perioperative management of anticoagulation in neurosurgical patients remain limited [27], particularly regarding shunt placement for NPH. Currently, there is no consensus on the most appropriate perioperative anticoagulation regimen in elective and emergent intracranial shunt surgery. As a result, surgeons often base their perioperative anticoagulation management strategy upon anecdotal observations and personal professional experiences [28]. To complicate matters further, the majority of neurosurgical procedures are considered to be high risk for perioperative bleeding and thrombosis [29–31]. For example, Hamilton et al. reported postoperative DVTs in >25 % of non-anticoagulated patients who underwent craniotomies [32]. Furthermore, temporary cessation of long-term anticoagulation exposes patients to an increased risk of thrombotic complications [30, 33, 34]. Conversely, continuation or early postoperative resumption of therapeutic anticoagulation increases the risk of postoperative hemorrhagic complications [28, 30, 34–37]. Several factors associated with a patients’ risk of thrombotic and bleeding complications include: the primary indication for long-term anticoagulation, type and duration of anticoagulant therapy, the patients’ baseline bleeding and thrombotic risks, urgency of surgery, duration of perioperative anticoagulant cessation, and whether partial or complete reversal of anticoagulation is achieved [31, 38–40]. Therefore, a meticulous balance between the opposing thrombotic and bleeding risks is crucial for safe and effective management of patients who undergo shunt placement for the management of NPH.
Given the unique considerations above, we recommend perioperative consultation with a hematologist and/or cardiologist in anticoagulated NPH patients undergoing shunt surgery. Due to the high risk of bleeding associated with intracranial procedures [29, 30, 41, 42], the majority of anticoagulated NPH patients require temporary interruption of therapy prior to shunt surgery. While long-term cessation of antithrombotic therapy is associated with a substantially increased risk of thrombotic complication in patients who require antithrombotic therapy, temporary cessation of therapy can be generally considered safe.
For patients on warfarin, Goodwin et al. proposed a perioperative anticoagulation management strategy, in which anticoagulation should be stopped at least 5–7 days before invasive diagnostic procedures or surgery to allow adequate time for their INR to normalize (Fig. 28.1) [3]. In patients whose INR remains above 1.5, oral phytonadione (vitamin K) may be used the day prior to surgery to reach normal levels. In patients considered too high risk for thromboembolism with complete cessation of anticoagulant therapy, bridging to intravenous (IV) unfractionated heparin (UFH), or therapeutic doses of subcutaneous (SQ) low molecular weight heparin (LMWH) can be utilized. Patients who may not be amenable to cessation of anticoagulation include those with a mechanical heart valve, history of atrial fibrillation, or recent venothromboembolism (<6 months). Bridging should be performed 36–48 h after the last dose of warfarin. The appropriate dose of anticoagulant used for bridging is dependent on the patient’s individual risk of thrombosis and bleeding, weight, and renal function. In an effort to reduce the risk of perioperative bleeding, bridging therapy should be stopped at least 24 h prior to surgery in patients receiving SQ LMWH, or 4–6 h prior to surgery if the patient is receiving IV UFH. The decision to bridge anticoagulation in patients who are determined to be at a moderate- to low-risk level for thromboembolism can be left to the discretion of the surgical and/or hematology/cardiology team. Furthermore, patients considered to be at a very low risk for thromboembolism , such as patients with bileaflet aortic valve prosthesis without atrial fibrillation or other risk factors for stroke, CHADS2 score of 0–2 without a history of prior stroke or transient ischemic attack or >12 months since their last and no other thromboembolic risk factors [42], should not be bridged prior to surgery [31]. Patient-specific factors such as medication adherence, comprehension, and ability to comply with the management plan should also be considered when deciding to bridge AC prior to surgery, particularly in NPH patients with significant dementia.

A proposed algorithm for perioperative management of NPH patients on warfarin therapy. Abbreviations: NPH normal pressure hydrocephalus, UFH unfractionated heparin, LMWH low molecular weight heparin. *Bridging therapy refers to stopping warfarin and transitioning to intravenous UFH or subcutaneous LMWH. **AC is stopped at least 24 h prior to surgery in patients receiving LMWH, or 4–6 h if UFH is used
In our practice, we suspend the use of aspirin and other antiplatelet agents at least 7–14 days prior to surgery in order to reduce the risk of hemorrhagic complications. This time frame is recommended based on the fact that many antiplatelet agents, such as aspirin, are irreversible inhibitors and platelet formation takes at least 5–7 days to replenish the available pool for clotting. Birkeland et al. also recommended the same timeline for cessation of antiplatelet therapy in their analysis of 35 patients receiving aspirin therapy in their study regarding the risk of subdural hematoma associated with shunt placement in patients with NPH (Fig. 28.2) [43].

A proposed algorithm for perioperative management of NPH patients on aspirin therapy. Adapted from Birkeland P, Lauritsen J, Poulsen FR. Aspirin is associated with an increased risk of subdural hematoma in normalFig. 28.2 (continued) pressure hydrocephalus patients following shunt implantation. J Neurosurg. 2015;123:423–6. Abbreviations: NPH normal pressure hydrocephalus, HCT head computed tomography, r/o rule out
The above approach should only be considered as a guideline for anticoagulated NPH patients, and is not a substitute for clinician judgment regarding perioperative anticoagulation in this challenging patient population. Likewise, newer antithrombotic therapies may require different perioperative management; therefore, consultation with a hematologist and/or cardiologist is encouraged. In all NPH patients receiving antithrombotic therapy, the INR, aPTT, and/or bleeding time should be measured in order to confirm that they are within the normal range prior to surgery. Placement of an IVC filter prior to shunt surgery can also be considered in patients at a particularly high risk for thromboembolism.
Surgical Considerations and Potential Intraoperative Complications
Aside from the general risks associated with performing a craniotomy or burr hole in an anticoagulated NPH patient, unique risks associated with shunt placement should also be considered. For example, incision of the pia mater prior to insertion of the shunt catheter is essential to avoid a subdural hematoma caused by unintentional stretching and tearing of the bridging veins from pushing the brain away from the overlying dura with catheter insertion. Image guidance may also improve the accuracy of ventricular shunt catheter placement, and avoid parenchymal injury and hemorrhagic complication due to multiple passes particularly in the hands of less experienced surgeons who do not commonly perform the procedure [44, 45]. In addition, an adjustable shunt valve with an anti-siphon device should be utilized to allow gradual adjustment of the pressure setting in order to lower the risk of subdural hygroma or hematoma postoperatively [46], particularly in anticoagulated NPH patients. In their randomized prospective study of 96 patients with NPH, Boon et al. found an increased risk of subdural effusions in patients receiving a low pressure shunt system (71 %) compared to a medium pressure system (34 %) [47]. However, a recent randomized controlled trial in iNPH patients found that gradual lowering of an adjustable shunt valve setting to a mean of 7 cm H2O resulted in a similar rate of shunt complications and overdrainage, when compared to a fixed valve setting of 13 cm H2O [48]. Of note, the use of perioperative antithrombotic therapy was similar between groups; though, anticoagulant medication was discontinued at least 1 week prior to shunt surgery in all patients in their study.
Postoperative Anticoagulation Management Strategy —Complication Avoidance and Postoperative Consideration
A head CT (HCT) should be performed within 24 h after shunt placement in anticoagulated NPH patients to assess for early, postoperative hemorrhagic complications (Figs. 28.3 and 28.4). If there is no radiographic or clinical evidence of hemorrhage, antithrombotic therapy can be restarted within an appropriate time frame as deemed by the management team. However, if a clinical or radiographic bleed is identified, antithrombotic therapy should be held until serial imaging shows resolution (in low-risk patients) or stability (in high-risk patients) of the hemorrhage. Also, the patient should be carefully evaluated for evidence of thrombotic complications secondary to temporary cessation of antithrombotic therapy.

Non-contrast axial head CT depicting preoperative (a), post-hemorrhage (b), and post-resolution (c) images in an 80-year-old male on long-term coumadin therapy prior to shunt placement for NPH. (On postoperative day 1, the patient experienced a large intraventricular hemorrhage bilaterally, involving the occipital horns and a small intraparenchymal hemorrhage around the catheter. The hemorrhage completely resolved 2 months postoperatively)

Non-contrast axial head CT depicting preoperative (a), post-hemorrhage (b), and last follow-up (c) images in an 85-year-old male on high-dose (325 mg daily) aspirin therapy prior to shunt placement for NPH. (On postoperative day 5, the patient experienced a large intraparenchymal hemorrhage along the course of the right posterior parietal approach ventricular shunt catheter extending into the right lateral ventricle. The hemorrhage continued to gradually evolve, with extension into the intraventricular system, until the patient’s death 1 month postoperatively)
Long-acting warfarin therapy may be subsequently restarted 24–48 h postoperatively if the postoperative CT is negative, or as soon as it is considered safe by the multidisciplinary team. Of note, in our previous study, warfarin therapy was restarted 3–5 days after surgery or at the time of discharge [3]; however, based on recent evidence, the American College of Chest Physicians (ACCP) guidelines recommends earlier resumption of warfarin after surgery [42]. However, in their 2013 New England Journal of Medicine review, Baron et al. deemed all neurosurgical procedures as high risk of hemorrhagic complication [31]. The authors also stated that due to the fact that resumption of warfarin therapy takes several days to achieve full anticoagulation, it can typically be restarted the evening of postoperative day 1, “unless there is a substantial risk of delayed bleeding or unless reoperation is anticipated” [31]. Due to the higher risk of significant morbidity and mortality associated with intracranial hemorrhage, and need for emergent surgical intervention if substantial bleeding is encountered, further studies are needed to substantiate this recommendation and to determine whether restarting warfarin 24 h postoperatively is safe after neurosurgical procedures and in the NPH population. Furthermore, caution should be taken in this particular population due to their increased gait instability and higher fall risk. Importantly, it may take >48 h after resumption of warfarin to reach a partial response (INR >1.5). In patients taking LMWH or UFH, anticoagulation can be resumed 24–72 h postoperatively, or after adequate hemostasis has been achieved. Based on the 2012 ACCP guidelines, antiplatelet therapy may be resumed 24–48 h after surgery [40]; however, based on the increased risk described above, most neurosurgeons prefer to wait at least 7 days for the resumption of aspirin therapy or 1–2 months for clopidogrel.
After restarting antithrombotic therapy , additional cranial imaging can be obtained after one to two doses of the medication to determine if a hemorrhagic event has occurred. If bleeding is identified, serial imaging should be performed until the bleed is stable to assess for progression/regression, as mentioned above. Surgical versus medical management with blood products is determined based on the extent and location of the bleed ± neurologic symptomatology. If no evidence of bleeding is observed, anticoagulant therapy can be continued. Additional imaging should be obtained if there is new onset of neurologic deficits or worsening of symptoms (i.e., headache). Imaging may also be obtained if anticoagulation becomes supratherapeutic and the patient is at substantial risk for hemorrhage that would necessitate immediate and complete interruption of therapy versus gradual dosing adjustment.
In the outpatient setting, gradual lowering of the pressure setting should be performed over time until maximum symptomatic improvement is achieved, without the onset of low pressure symptomatology [3].
Postoperative Complications
The most serious, and deadly, complication associated with antithrombotic therapy is intracranial hemorrhage, most commonly via ICH [49]. According to McGovern et al.’s study, symptomatic ICH was observed in 1.5 % of NPH patients who received a ventriculoperitoneal shunt; however, the effect of antithrombotic therapy was not assessed [50]. Importantly, however, the initial volume and duration of expansion is greater in anticoagulant-associated ICH compared to spontaneous ICH, with a corresponding mortality rate greater than 50 % [51]. Furthermore, warfarin therapy doubles the risk of fatal intracranial hemorrhage, with ICH causing approximately 90 % of permanent morbidity and mortality in patients with bleeding associated with anticoagulation [52, 53]. Likewise, the risk of ICH is increased with the use of aspirin therapy by approximately 40 % [49]. Combined use of warfarin and aspirin likely further increases the risk of hemorrhage than either therapy alone [54], and approximately 20 % of elderly adults are on a combined regimen of anticoagulant-antiplatelet therapy [55]. While newer anticoagulants are associated with a lower risk of intracranial hemorrhage compared to warfarin, as demonstrated by the RE-LY (i.e., dabigatran) [56], ROCKET-AF (i.e., rivaroxaban) [57], and ARISTOTLE (i.e., apixaban) trials [58], caution must be performed due to the lack of available reversal agents for these newer agents.
Common, delayed, postoperative complications after shunt surgery include shunt obstruction, infection, subdural hygroma or hematoma, and shunt migration [8, 9]. Surgical overdrainage of CSF via ventricular shunting, particularly in the upright position, increases the risk of subdural hygroma or hematoma. Overdrainage adversely affects surgical and postoperative clinical outcomes for NPH and, to a lesser degree, generic measures of health-related quality of life [59]. Subdural hematoma occurs after 2–17 % of shunt surgeries for the treatment of NPH [3, 43]. Khan et al. reported eight (5 %) cases of SDH requiring surgical evacuation after shunt placement in patients with iNPH; however, the effect of antithrombotic therapy was not assessed [60]. In their systematic review of the outcome after shunt surgery for iNPH, Toma et al. reported a 6.3 % (range 2–47 %) rate of subdural hematoma (SDH) or hygroma and an ICH or stroke rate of 0.4 % (range 0–18 %) [61]. The effect of antithrombotic therapy was not determined in these cases. Epidural hematoma after CSF shunting is much less common, and almost always develops within the first few hours after surgery; on the other hand, SDH may be either acute or delayed [62]. Similarly, anticoagulation-associated subarachnoid hemorrhage is rare, with Mattle et al. reporting only seven out of 76 cases (9.2 %) of intracranial hemorrhage over a 6-year period [63].
In our previous study of 15 anticoagulated NPH patients who underwent shunt surgery, two (13 %) patients experienced symptomatic, postoperative bleeding complications [3]. One patient, with comorbid cirrhotic hepatitis C, who received bridging therapy with IV UFH, experienced an SDH 13 days after shunt surgery. Subsequently, anticoagulation was stopped immediately until the INR and aPTT normalized, and the shunt was removed 2 days after cessation of anticoagulant therapy . Another patient developed a large abdominal subcutaneous hematoma 5 days after shunt surgery, and required surgical evacuation.
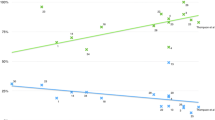
In a recent assessment of the risk of subdural hematoma (SDH) in 80 patients who underwent shunt surgery for NPH, 35 of whom were taking aspirin and 13 who were on combined anticoagulant-antiplatelet therapy, 11 (14 %) cases of symptomatic SDH occurred. All cases of SDH after shunt surgery arose in patients receiving aspirin or clopidogrel, with a hazard ratio of 12.8 (95 % CI 3.1–53) associated with aspirin use (Fig. 28.5). The authors concluded that clopidogrel may pose an even greater risk of postoperative subdural hematoma after shunt surgery [43]. In this study, the authors hypothesized that shunting in NPH patients increases the risk for the brain to collapse, resulting in increased susceptibility to SDH, particularly in patients receiving antiplatelet therapy (e.g., aspirin and/or clopidogrel). Mahaney et al. reported a slightly lower, but significant, rate of postoperative hemorrhage associated with shunt placement in patients on dual antiplatelet therapy with 325 mg acetylsalicylic acid daily and 75 mg clopidogrel daily (P = 0.0075), with a total of four (10.8 %) cases of intracranial hemorrhage associated with dual antiplatelet therapy [64]. Of note, dual antiplatelet therapy was not stopped prior to shunt placement in any of the patients in their study [64].

Kaplan-Meier plot of event-free survival in patients on aspirin therapy. Courtesy of Birkeland P, Lauritsen J, Poulsen FR. Aspirin is associated with an increased risk of subdural hematoma in normal-pressure hydrocephalus patients following shunt implantation. J Neurosurg. 2015;123:423–6
Conclusions
Ultimately, patients on long-term antithrombotic therapy can be safely and effectively evaluated and treated for NPH, with the use of appropriate perioperative and postoperative management. While the overall risk of bleeding associated with shunt placement is low, NPH patients receiving antithrombotic therapy are at a significantly increased risk of hemorrhagic complication compared to patients who are not on antithrombotic therapy. Given the advanced age, gait impairment, and dementia associated with NPH, the bleeding and thrombotic risk may be even higher in NPH than the general population receiving antithrombotic therapy. Therefore, consultation with a hematologist and/or cardiologist is warranted in order to determine which patients can safely suspend antithrombotic therapy prior to surgery versus those who require bridging. Operative considerations that can reduce the risk of hemorrhagic complication include incision of the pia mater prior to ventricular catheter insertion, potential use of intraoperative imaging guidance, and placement of and adjustable and gravity-assisted shunt valve to lower the risk of overdrainage. In the outpatient setting, gradual lowering of the pressure setting should be performed over time until a balance is reached between maximum symptomatic improvement and the onset of symptoms suggestive of low intracranial pressure (e.g., orthostatic headache and dizziness). Postoperatively, the time to resumption of antithrombotic therapy depends on the patients’ individual risk of thrombosis and bleeding as well as radiographic evaluation for intracranial hemorrhage.
References
Adams RD, Fisher CM, Hakim S, Ojemann RG, Sweet WH. Symptomatic occult hydrocephalus with “normal” cerebrospinal-fluid pressure. A treatable syndrome. N Engl J Med. 1965;273:117–26.
Hakim S, Adams RD. The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure. Observations on cerebrospinal fluid hydrodynamics. J Neurol Sci. 1965;2(4):307–27.
Goodwin CR, Kharkar S, Wang P, Pujari S, Rigamonti D, Williams MA. Evaluation and treatment of patients with suspected normal pressure hydrocephalus on long-term warfarin anticoagulation therapy. Neurosurgery. 2007;60(3):497–501. discussion 502.
Black PM, Ojemann RG, Tzouras A. CSF shunts for dementia, incontinence, and gait disturbance. Clin Neurosurg. 1985;32:632–51.
Iseki C, Takahashi Y, Wada M, Kawanami T, Adachi M, Kato T. Incidence of idiopathic normal pressure hydrocephalus (iNPH): a 10-year follow-up study of a rural community in Japan. J Neurol Sci. 2014; 339(1–2):108–12.
Brean A, Eide PK. Prevalence of probable idiopathic normal pressure hydrocephalus in a Norwegian population. Acta Neurol Scand. 2008;118(1):48–53.
Jaraj D, Rabiei K, Marlow T, Jensen C, Skoog I, Wikkelsø C. Prevalence of idiopathic normal-pressure hydrocephalus. Neurology. 2014;82(16):1449–54.
Aoki N. Lumboperitoneal shunt: clinical applications, complications, and comparison with ventriculoperitoneal shunt. Neurosurgery. 1990;26(6):998–1003. discussion 1003–4.
Samuelson S, Long DM, Chou SN. Subdural hematoma as a complication of shunting procedures for normal pressure hydrocephalus. J Neurosurg. 1972;37(5):548–51.
Krauss JK, Regel JP, Vach W, Droste DW, Borremans JJ, Mergner T. Vascular risk factors and arteriosclerotic disease in idiopathic normal-pressure hydrocephalus of the elderly. Stroke. 1996;27(1):24–9.
Eide PK, Pripp AH. Increased prevalence of cardiovascular disease in idiopathic normal pressure hydrocephalus patients compared to a population-based cohort from the HUNT3 survey. Fluids Barriers CNS. 2014;11:19.
Hager KK, Loprinzi P, Stone D. Implementing diabetes care guidelines in long term care. J Am Med Dir Assoc. 2013;14(11):851.e7–15.
Bergsneider M, Black PM, Klinge P, Marmarou A, Relkin N. Surgical management of idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005;57(3 Suppl):S29–39. discussion ii–v.
Poca MA, Mataró M, Del Mar Matarín M, Arikan F, Junqué C, Sahuquillo J. Is the placement of shunts in patients with idiopathic normal-pressure hydrocephalus worth the risk? Results of a study based on continuous monitoring of intracranial pressure. J Neurosurg. 2004;100(5):855–66.
Pfisterer WK, Aboul-Enein F, Gebhart E, Graf M, Aichholzer M, Mühlbauer M. Continuous intraventricular pressure monitoring for diagnosis of normal-pressure hydrocephalus. Acta Neurochir (Wien). 2007;149(10):983–90. discussion 990.
Koskinen LO, Grayson D, Olivecrona M. The complications and the position of the Codman MicroSensor™ ICP device: an analysis of 549 patients and 650 sensors. Acta Neurochir (Wien). 2013;155(11):2141–8. discussion 2148.
Kakarla UK, Kim LJ, Chang SW, Theodore N, Spetzler RF. Safety and accuracy of bedside external ventricular drain placement. Neurosurgery. 2008;63(1 Suppl 1):ONS162–6; discussion ONS166–7.
Pitkänen M, Fürster J. Complications caused by lumbar puncture. Duodecim. 2014;130(18):1834–42.
Fisher CM. Hydrocephalus as a cause of disturbances of gait in the elderly. Neurology. 1982;32(12): 1358–63.
Feick D, Sickmond J, Liu L, et al. Sensitivity and predictive value of occupational and physical therapy assessments in the functional evaluation of patients with suspected normal pressure hydrocephalus. J Rehabil Med. 2008;40(9):715–20.
Vos PE, de Boer WA, Wurzer JA, van Gijn J. Subdural hematoma after lumbar puncture: two case reports and review of the literature. Clin Neurol Neurosurg. 1991;93(2):127–32.
Hillemacher T, Bleich S, Wiltfang J, Weber M, Kornhuber J, Frieling H. Should aspirin be discontinued for diagnostic lumbar puncture? J Am Geriatr Soc. 2006;54(1):181–2.
Samdani A, Garonzik IM, Zahos P. Subdural hematoma after diagnostic lumbar puncture. Am J Emerg Med. 2004;22(4):316–7.
Paal P, Putz G, Gruber E, Le GT, Lemberger P. Subarachnoid hemorrhage after lumbar puncture in a patient receiving aspirin and clopidogrel. Anesth Analg. 2006;102(2):644–5.
Berger JS, Roncaglioni MC, Avanzini F, Pangrazzi I, Tognoni G, Brown DL. Aspirin for the primary prevention of cardiovascular events in women and men: a sex-specific meta-analysis of randomized controlled trials. JAMA. 2006;295(3):306–13.
Eide PK, Sorteberg W. Diagnostic intracranial pressure monitoring and surgical management in idiopathic normal pressure hydrocephalus: a 6-year review of 214 patients. Neurosurgery. 2010;66(1): 80–91.
Scheller C, Rachinger J, Strauss C, Alfieri A, Prell J, Koman G. Therapeutic anticoagulation after craniotomies: is the risk for secondary hemorrhage overestimated? J Neurol Surg A Cent Eur Neurosurg. 2014;75(1):2–6.
Rachinger JC, Koman G, Scheller C, Prell J, Rampp S, Strauss C. Practice in the perioperative prevention of deep vein thrombosis in German neurosurgical departments: is there a trend towards homogenization? Cent Eur Neurosurg. 2011;72(3):115–9.
Zakaryan A. Perioperative management of neurosurgical patients receiving chronic anticoagulation therapy. Front Pharmacol. 2014;5:64.
Thachil J, Gatt A, Martlew V. Management of surgical patients receiving anticoagulation and antiplatelet agents. Br J Surg. 2008;95(12):1437–48.
Baron TH, Kamath PS, McBane RD. Management of antithrombotic therapy in patients undergoing invasive procedures. N Engl J Med. 2013;368(22): 2113–24.
Hamilton MG, Hull RD, Pineo GF. Venous thromboembolism in neurosurgery and neurology patients: a review. Neurosurgery. 1994;34(2):280–96. discussion 296.
Schanbacher CF, Bennett RG. Postoperative stroke after stopping warfarin for cutaneous surgery. Dermatol Surg. 2000;26(8):785–9.
Lecompte TP. Antithrombotic agents and invasive procedures—hematologist point of view. Thromb Res. 2012;130 Suppl 1:S61–2.
Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med. 1997;336(21):1506–11.
Laohaprasit V, Mayberg MR. Risks of anticoagulation therapy after experimental corticectomy in the rat. Neurosurgery. 1993;32(4):625–8. discussion 628–9.
Schaible KL, Smith LJ, Fessler RG, Rachlin JR, Brown FD, Mullan S. Evaluation of the risks of anticoagulation therapy following experimental craniotomy in the rat. J Neurosurg. 1985;63(6):959–62.
Grant PJ, Brotman DJ, Jaffer AK. Perioperative anticoagulant management. Anesthesiol Clin. 2009;27(4): 761–77.
Douketis JD. Perioperative anticoagulation management in patients who are receiving oral anticoagulant therapy: a practical guide for clinicians. Thromb Res. 2002;108(1):3–13.
Gleason LJ, Friedman SM. Preoperative management of anticoagulation and antiplatelet agents. Clin Geriatr Med. 2014;30(2):219–27.
Lazio BE, Simard JM. Anticoagulation in neurosurgical patients. Neurosurgery. 1999;45(4):838–47. discussion 847–8.
Douketis JD, Spyropoulos AC, Spencer FA, et al. Perioperative management of antithrombotic therapy: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e326S–50.
Birkeland P, Lauritsen J, Poulsen FR. Aspirin is associated with an increased risk of subdural hematoma in normal-pressure hydrocephalus patients following shunt implantation. J Neurosurg. 2015;123:423–6.
Kim YB, Lee JW, Lee KS, Lee KC. Image-guided placement of ventricular shunt catheter. J Clin Neurosci. 2006;13(1):50–4.
Jakola AS, Reinertsen I, Selbekk T, et al. Three-dimensional ultrasound-guided placement of ventricular catheters. World Neurosurg. 2014;82(3–4):536.e5–9.
Freimann FB, Vajkoczy P, Sprung C. Patients benefit from low-pressure settings enabled by gravitational valves in normal pressure hydrocephalus. Clin Neurol Neurosurg. 2013;115(10):1982–6.
Boon AJ, Tans JT, Delwel EJ, et al. Dutch Normal-Pressure Hydrocephalus Study: randomized comparison of low- and medium-pressure shunts. J Neurosurg. 1998;88(3):490–5.
Sæhle T, Farahmand D, Eide PK, Tisell M, Wikkelsö C. A randomized controlled dual-center trial on shunt complications in idiopathic normal-pressure hydrocephalus treated with gradually reduced or “fixed” pressure valve settings. J Neurosurg. 2014;121(5): 1257–63.
Connolly BJ, Pearce LA, Kurth T, Kase CS, Hart RG. Aspirin therapy and risk of subdural hematoma: meta-analysis of randomized clinical trials. J Stroke Cerebrovasc Dis. 2013;22(4):444–8.
McGovern RA, Kelly KM, Chan AK, Morrissey NJ, McKhann GM. Should ventriculoatrial shunting be the procedure of choice for normal-pressure hydrocephalus? J Neurosurg. 2014;120(6):1458–64.
El Ahmadieh TY, Aoun SG, Daou MR, et al. New-generation oral anticoagulants for the prevention of stroke: implications for neurosurgery. J Clin Neurosci. 2013;20(10):1350–6.
Fang MC, Go AS, Chang Y, et al. Death and disability from warfarin-associated intracranial and extracranial hemorrhages. Am J Med. 2007;120(8):700–5.
Rosand J, Eckman MH, Knudsen KA, Singer DE, Greenberg SM. The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med. 2004;164(8):880–4.
Hart RG, Benavente O, Pearce LA. Increased risk of intracranial hemorrhage when aspirin is combined with warfarin: a meta-analysis and hypothesis. Cerebrovasc Dis. 1999;9(4):215–7.
Shireman TI, Howard PA, Kresowik TF, Ellerbeck EF. Combined anticoagulant-antiplatelet use and major bleeding events in elderly atrial fibrillation patients. Stroke. 2004;35(10):2362–7.
Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139–51.
Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883–91.
Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981–92.
Meier U, Stengel D, Müller C, et al. Predictors of subsequent overdrainage and clinical outcomes after ventriculoperitoneal shunting for idiopathic normal pressure hydrocephalus. Neurosurgery. 2013;73(6):1054–60.
Khan QU, Wharen RE, Grewal SS, et al. Overdrainage shunt complications in idiopathic normal-pressure hydrocephalus and lumbar puncture opening pressure. J Neurosurg. 2013;119(6):1498–502.
Toma AK, Papadopoulos MC, Stapleton S, Kitchen ND, Watkins LD. Systematic review of the outcome of shunt surgery in idiopathic normal-pressure hydrocephalus. Acta Neurochir (Wien). 2013;155(10): 1977–80.
Driesen W, Elies W. Epidural and subdural haematomas as a complication of internal drainage of cerebrospinal fluid in hydrocephalus. Acta Neurochir (Wien). 1974;30(1–2):85–93.
Mattle H, Kohler S, Huber P, Rohner M, Steinsiepe KF. Anticoagulation-related intracranial extracerebral haemorrhage. J Neurol Neurosurg Psychiatry. 1989;52(7):829–37.
Mahaney KB, Chalouhi N, Viljoen S, et al. Risk of hemorrhagic complication associated with ventriculoperitoneal shunt placement in aneurysmal subarachnoid hemorrhage patients on dual antiplatelet therapy. J Neurosurg. 2013;119(4):937–42.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Sankey, E.W., Goodwin, C.R., Jusue-Torres, I., Rigamonti, D. (2016). Is It Safe to Shunt Anticoagulated NPH Patients?. In: Loftus, C. (eds) Anticoagulation and Hemostasis in Neurosurgery. Springer, Cham. https://doi.org/10.1007/978-3-319-27327-3_28
Download citation
DOI: https://doi.org/10.1007/978-3-319-27327-3_28
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-27325-9
Online ISBN: 978-3-319-27327-3
eBook Packages: MedicineMedicine (R0)