
Abstract
In some men, semen passes into the bladder instead of out through the urethra; this is known as retrograde ejaculation. Retrograde ejaculation occurs if the nerves and muscles that control ejaculation are damaged, or removed, or if the prostate is enlarged. Increasing the pH of the urine prior to ejaculation may preserve the viability of the sperm.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
1 Introduction
In some men, semen passes into the bladder instead of ejecting out through the urethra; this is known as retrograde ejaculation [1]. Retrograde ejaculation occurs if the nerves and muscles that control ejaculation are damaged, or removed, or if the prostate is enlarged. Increasing the pH of the urine prior to ejaculation may preserve the viability of the sperm [1–3].
2 Patient Instructions
Patients are instructed to urinate without completely emptying the bladder. The patient should then collect his ejaculate into a sterile collection container. After collecting the semen sample (Fig. 13.1), the patient then urinates into a separate sterile container containing ~9 mL of warm (37 °C) sperm wash media (HTF) prepared just prior to the patient’s appointment (Fig. 13.2).

Urine sample collection container containing 9 mL HTF [Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2015. All Rights Reserved]

Semensample collection container [Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2015. All Rights Reserved]
Note: The tops of the collection containers should be marked with the words “semen” and “urine” to make it clear to the patient which container is for what specimen.
3 Equipment/Reagents
-
A.
Sperm wash media—modified HTF with 5 % human serum albumin
-
B.
Centrifuge
-
C.
Incubator
-
D.
Computer-assisted semen analyzer (Hamilton Thorne)
-
E.
Sterile 15 mL centrifuge tubes with caps
-
F.
Sterile graduated serological pipettes (2 and 10 mL)
-
G.
Sterile disposable Pasteur pipettes
-
H.
Eppendorf pipette tips (5 μL)
-
I.
Disposable 20 μm sperm counting chambers
-
J.
Sterile collection containers
4 Quality Control
Weekly Precision: A donor specimen should be obtained and run through the CASA. A manual count and motility reading should also be performed in conjunction with the CASA analysis.
Criteria: All manual results should be within a 20 % difference of the CASA values.
Response: If results are not within the defined percentage difference, the semen analysis must be repeated. If it is still out of range, inform the Supervisor or Director.
5 Procedure
Note: Sterile technique should be used throughout the procedure.
-
A.
Warm ~12 mL of HTF media to 37 °C in an incubator.
-
B.
When the patient arrives, transfer ~9 mL of the warm HTF media into a sterile collection container (labeled with the patient’s name, MRN, and “urine” to aid the patient) and give to the patient for collection of his urine sample. Label another container with “semen” and give to the patient for his semen sample.
-
C.
Provide patient with proper collection instructions (see Sect. 2, above).
-
D.
Complete the necessary paperwork making sure to record the patient’s name, MRN, ordering physician, time of collection, and length of abstinence.
-
E.
After the patient collects the specimens, place the semen sample in the incubator. While the semen is incubating, measure the volume of the urine/HTF mixture (Fig. 13.3) then transfer the specimen into sterile 15 mL conical tubes (Fig. 13.4) using a 10 mL serological pipette. Centrifuge at 1600 RPM for 10 min (Fig. 13.5).
Fig. 13.3 
Urine/HTF sample [Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2015. All Rights Reserved]
Fig. 13.4 
Urine/HTF sample evenly distributed into 15 mL conical vials [Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2015. All Rights Reserved]
Fig. 13.5 
First centrifugation of urine /HTF specimen; subsequent separation of urine/HTF from sperm pellet and removal of supernatant [Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2015. All Rights Reserved]
Note: Record the urine/HTF volume on the patient worksheet along with the volume of the HTF added to the collection container prior to sample collection; note that the specimen type, “urine,” on the worksheet.
-
F.
Discard the supernatant from each tube into a waste container being careful not to disturb the pellet, or cloudy portion, at the bottom of the tube(s).
-
G.
Remove the supernatant and resuspend in 1.0–2.0 mL of HTF (Fig. 13.6). Note and record the sample volume on the patient report form then proceed to analyze the sample per the “Routine Semen Analysis” protocol and in accordance with Sect. 6 below.
Fig. 13.6 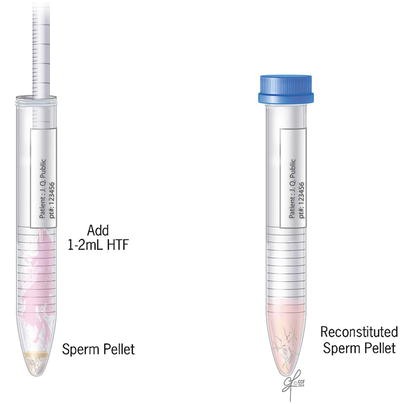
Addition of 1–2 mL of HTF and resuspension of sperm pellet [Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2015. All Rights Reserved]
Note: On the report form, note the total volume of the reconstituted sample, the HTF volume added, and that the specimen was spun and reconstituted. Use this reconstituted volume for the calculations.
-
H.
Take the semen sample from the incubator and analyze per the “Routine Semen Analysis” protocol.
-
I.
After checking the results to ensure accuracy, enter results into Sunquest and print the final report. Review the final report to check for errors and correct if necessary.




6 Procedural Notes
Cytospin slides should only be made in cases where no sperm is seen in the semen sample; cytospin slides should not be made for urine specimens.
References
WHO laboratory manual for the examination and processing of human semen. 5th ed.; 2010, published in Switzerland.
Tepper G, Rabbani R, Yousefzadeh M, Prince D. Quantitative assessment of retrograde ejaculation using semen analysis, comparison with a standardized qualitative questionnaire, and investigating the impact of rhBMP-2. Spine (Phila Pa 1976). 2013;38(10):841–5.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Cleveland Clinic
Cleveland Clinic

Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Agarwal, A., Gupta, S., Sharma, R. (2016). Procedure for Retrograde Ejaculate. In: Agarwal, A., Gupta, S., Sharma, R. (eds) Andrological Evaluation of Male Infertility. Springer, Cham. https://doi.org/10.1007/978-3-319-26797-5_13
Download citation
DOI: https://doi.org/10.1007/978-3-319-26797-5_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-26795-1
Online ISBN: 978-3-319-26797-5
eBook Packages: MedicineMedicine (R0)