
Abstract
Suicide shows a very strong association with affective illnesses, yet not all mood disorder patients commit suicide; therefore analysing affective pathology for those characteristics which differentiate suicidal and non-suicidal patients would be a key step in understanding the pathology of suicidal behaviour. One such phenomenon associated with affective illnesses and suicidal behaviour as well is affective temperaments. While the different affective temperamental types (depressive, anxious, irritable, cyclothymic, and hyperthymic) have all been shown to have some pattern of association with suicidal behaviour, results most consistently point to a key role for cyclothymic temperament for increasing the risk of suicide and suicide attempts via multiple mechanisms and not only in case of mood disorders but also in other psychiatric illnesses and in healthy samples. Hyperthymic temperament, on the other hand, seems to have a protective effect. Although the biological substrate of the association between affective temperaments and suicidality is not well understood, one possible factor may be the presence of the 5-HTTLPR s allele, which is associated with affective temperaments carrying a depressive component and also violent suicidal behaviour. Understanding the role of affective temperaments in the development of suicidal behaviour may bring us closer not only to understanding the etiopathology of suicide and may provide us with important new research models but may also mean new targets for screening and intervention.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Suicidal behaviour, a complex multicausal human phenomenon aimed at self-destruction, is the most tragic event of our human life, deleterious not only for its victim but also causing serious distress among relatives and friends as well as among treating doctors, at least in cases when the victim was in contact with medical care. Because suicide is a rare event in the community, its precise prediction in individual cases is very difficult. However, suicidal behaviour (completed suicide and suicide attempt) is quite frequent among psychiatric patients who contact different levels of healthcare some weeks or months before their death (Luoma et al. 2002). Untreated unipolar or bipolar major depressive episode is the main clinical substrate of completed suicide, accounting for 56–87 % of the cases (Rihmer 2007; Hawton and van Heeringen 2009). What is most important in this respect is that suicidal behaviour in mood disorder patients is a state- and severity-dependent phenomenon and that suicidality decreases/vanishes after the clinical recovery (Rihmer 2007; Rihmer and Gonda 2013). This underscores the importance of early recognition and appropriate acute and long-term treatment/care of patients with mood disorder in preventing suicidal behaviour. However, as the majority of depressed patients never complete suicide and about half of them never attempt it, special clinical (agitated/mixed depression, insomnia, hopelessness, etc.), psychological (premorbid personality, coping style, etc.), and psychosocial risk factors (early and current adverse life events, permanent stressors, etc.) also play a significant contributory role (Rihmer 2007; Hawton and van Heeringen 2009). Suicide risk factors are additive in their nature and a constellation of these factors may help identify those patients who are at an especially high risk for suicide.
2 Personality Features and Suicidal Behaviour
As for psychological characteristics, it is well known for many decades that suicidality is also associated with certain personality features, such as aggressive/impulsive traits, hopelessness, and pessimism, and the risk increases if these traits are present in combination (Mann et al. 1999; Oquendo et al. 2004; MacKinnon et al. 2005). Impulsivity, a characteristic trait in bipolar patients, was associated with nonlethal suicide attempts in general samples, and in case of affective patients, it is also associated with severe suicide attempts and completed suicide (Swann et al. 2005). Impulsivity distinguishes suicidal and non-suicidal affective inpatients and controls and in bipolar patients suicidal intent correlated with impulsivity even when controlling for aggression. Impulsivity increases suicide risk when combined with depression, and even modest manic symptoms during bipolar depressive episodes are associated with a greater level of impulsivity and higher rates of suicide attempts (Swann et al. 2005). Several studies have shown that suicidal behaviour was also associated with aggressive traits in the case of major depression and bipolar disorder (Mann et al. 1999; Grunebaum et al. 2006; Hawton and van Heeringen 2009). Bipolar patients with a family history of suicidal behaviour and exposed to childhood physical and/or sexual abuse are at greater risk for suicide attempts (Carballo et al. 2008) and impulsivity seems to be the link between childhood abuse and suicidal behaviour (Braquehais et al. 2010). In a study on bipolar patients, harm avoidance and persistence as measured by Cloninger’s TCI were significantly related to prior suicide attempts (Engstrom et al. 2004). Hostility was also found to be a suicide attempt risk factor, while optimistic personality features and many reasons for living an important protective factor in bipolar disorder (Chaudhury et al. 2007).
3 Affective Temperaments and Suicidal Behaviour
However, only in the last decade did it become evident that affective temperaments, known to be subclinical manifestations and precursors of major mood disorders (Akiskal et al. 2003; Kochman et al. 2005; Pompili et al. 2008), are also predisposing (risk) factors for suicidal behaviour. Classically, temperament carries the temporally stable biological “core” of personality and plays a role in establishing an individual’s activity levels, rhythms, moods, and related cognitions as well as their variability, while personality, a broader phenotype, refers also to acquired characterologic determinants and interpersonal operations (Akiskal et al. 1983; Bouchard 1994). The concept that different kinds of temperament are constitutionally based types of behaviour can be traced back to the ancient humoral theory of Hippocrates (Akiskal 1996). About 100 years ago, Kraepelin described four basic affective dispositions (depressive, manic, cyclothymic, and irritable) which he believed were subclinical forms and many times precursors of major affective disorders and had their roots in adolescence. He also described that these four basic affective dispositions could be frequently found in blood relatives of manic-depressive patients (Kraepelin 1915). The modern concept of affective temperaments, as operationalized in research originally conducted at the University of Tennessee, Memphis, USA, by Akiskal and his co-workers (Akiskal and Mallya 1987; Akiskal et al. 1977) was based primarily on the works of Kraepelin (1915) and Kretschmer (1936) and was derived from both theoretical considerations and clinical observations yielding five affective temperaments (depressive, cyclothymic, hyperthymic, irritable, and anxious). This concept was turned into an instrument called as TEMPS-A (Temperament Evaluation of the Memphis, Pisa, Paris, and San Diego Autoquestionnaire version) for assessing depressive, cyclothymic, hyperthymic irritable, and anxious temperaments. This autoquestionnaire version requiring just simple “yes” or “no” answers contains 110 items (109 for males) (Akiskal et al. 2005a, b).
While the role of temperamental factors in suicidal behaviour has been known for decades (Maser et al. 2002), recent studies on this field have shown a strong relationship between specific affective temperament types and suicidal behaviour. Compared to bipolar II patients without cyclothymic temperament (n = 120), bipolar II patients with such temperament (n = 74) reported significantly more frequent lifetime suicide attempts (38 % vs 49 %) and experienced more current hospitalization for suicidal risk (50 % vs 61 %) (Akiskal et al. 2003). Other studies have also shown that bipolar I, bipolar II, and unipolar major depressive disorder patients with a cyclothymic temperament have a significantly higher rate of prior suicide attempts and lifetime/current suicidal ideation than noncyclothymic patients (Young et al. 1995).
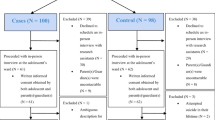
Recent studies have found that in contrast to hyperthymic temperament which seems to be a protective factor against suicidal behaviour (Vazquez et al. 2010; Pompili et al. 2008, 2012; Rihmer et al. 2009a), cyclothymic, irritable, depressive, and anxious affective temperaments were significantly overrepresented in suicide attempters or in mood disorder inpatients with high current suicide risk (Rihmer et al. 2009a; Pompili et al. 2008, 2012). Pompili et al. (2008) investigated the affective temperament profile of 150 consecutively hospitalized psychiatric patients; 80 % of them have had unipolar, bipolar I, or bipolar II major depressive episode and 41 % have had current suicidal risk at admission. They found that the 62 suicidal patients scored significantly higher on depressive, cyclothymic, irritable, and anxious and significantly lower on hyperthymic subscales of the TEMPS-A than the 88 patients with no suicidal risk. Using the same instrument, we also compared the affective temperament types of 150 consecutively investigated nonviolent suicide attempters (106 females) and 302 age-, sex-, and education-matched controls. Compared to controls, both female and male suicide attempters scored significantly higher in the four of the five affective temperaments, containing more or less of a depressive component (depressive, cyclothymic irritable, and anxious), while no significant difference was found for the hyperthymic temperament. Consequently, the dominant forms of depressive, cyclothymic, irritable, and anxious temperaments were significantly more common and hyperthymic temperament was (nonsignificantly) less frequent among the attempters (Rihmer et al. 2009a). Our recent study on 346 adult inpatients with major mood disorders, 81 % of patients with prevailing cyclothymic-depressive-anxious temperament had mild to severe suicidal risk on the M.I.N.I. versus only 42 % of those with a prevailing hyperthymic temperament. Sixty-four percent of patients with cyclothymic-depressive-anxious temperament had high suicide risk according to the Beck Hopelessness Scale versus only 13 % of patients with hyperthymic temperament (Pompili et al. 2012). The findings of these three studies (Pompili et al. 2008, 2012; Rihmer et al. 2009a) support the strong relationship between depression and suicidal behaviour even on temperamental level and suggest a possible protective role of hyperthymic temperament at least in the case of suicide attempts or mood disorder patients with current suicidality. The significantly higher cyclothymic and irritable scores among suicide attempters with childhood abuse also (Rihmer et al. 2009b) show the modifying role of early adverse events on the personality development in general and on the affective temperament in particular. The significantly higher cyclothymic and irritable scores among suicide attempters with childhood abuse also show the modifying role of early adverse events on the personality development in general and on the affective temperament in particular.
In addition, cyclothymic temperament significantly predicted future bipolar transformation and suicide attempts in adult (Goto et al. 2011) and juvenile depressives (Kochman et al. 2005). In a large-scale French study, it has also been found that cyclothymic temperament was one of the eight risk factors (such as young age at onset, depressive or mixed polarity of first episode, stressful life events, etc.) statistically significantly associated with lifetime suicide attempts in patients with bipolar I disorder (Azorin et al. 2009).
Affective temperaments seem to be related to suicidal behaviour also in non-clinical samples. Investigating the affective temperamental profile, as measured by TEMPS-A, among 1381 college students in Austria it has been found that lifetime suicidal ideation was associated with the depressive, cyclothymic, and anxious temperament in both sexes and the irritable temperament in males and no relationship was found regarding hyperthymic temperament (Skala et al. 2012). In a sample of public school students (N = 1713, aged between 12 and 20 years) in Portugal, the history of prior self-harm was associated, in both genders, with a significant deviation on depressive, cyclothymic, and irritable dimensions of the TEMPS-A, and again, hyperthymic temperament was unrelated to self-harm (Guerreiro et al. 2013). However, marked affective temperaments that can be detected in about 15–20 % of the general population (Rihmer et al. 2010; Gonda et al. 2011b) become suicide risk factors only during major depressive episode as persons with marked affective temperament have a much higher chance to develop major mood episodes and particularly the combination of cyclothymic or irritable personality traits and major depressive episode results in a mixed depressive episode that carries very high suicide risk (Rihmer 2007; Rihmer et al. 2010). Suicide attempters with cyclothymic and irritable affective temperaments report significantly more frequently childhood physical and/or sexual abuse (Rihmer et al. 2009b) suggesting that besides impulsivity (Braquehais et al. 2010), cyclothymic or irritable temperaments are further mediating variables between these early negative life events and adult suicidal behaviour (Rihmer et al. 2009b).
4 How Can a Specific Affective Temperament Predispose for Suicidal Behaviour?
Currently, we have limited understanding concerning what mediates the how effects of these affective temperament on suicidal behaviour. Cyclothymic temperament may influence suicide risk on multiple levels, from determining emotional reactivity in stressful situations at the level of the personality, through determining illness and illness course characteristics, to influencing within-episode dynamics. Cyclothymic temperament is associated with rapid mood fluctuations, mood reactivity, and emotional instability contributing to extreme distress. Furthermore, cyclothymic temperament makes adapting to environmental changes and adversities difficult. Combined with other traits, cyclothymic temperament also contributes to a darker and more risk-taking impulsive side of hypomania, and this, as well as the instability associated with this affective temperament, increases the risk of encountering stressful life events and comorbid conditions which play a role in triggering mood episodes and suicide. The temperamental reactivity embodied in cyclothymia also seems to be a stable trait constituting a basis for rapid shifts between inhibition and disinhibition providing the drive and energy for the suicidal act (Pompili et al. 2012). The relationship between affective temperaments and suicidal behaviour is, however, more complex than the simple additive effect of depressive personality components and current major depressive episode, as cyclothymic temperament seems to be also a contributor to suicidality in patients with other diagnosis than major depression, The presence of cyclothymic temperament increases suicide risk not only in affective disorders but in other illnesses as well, such as obsessive-compulsive disorder (Hantouche et al. 2003). The central role of cyclothymic oscillations of mood, thinking, and behaviour in the evolution of suicidal process has been shown by studies reporting that history of rapid mood switching was associated with increased likelihood of prior suicidal ideation or attempt (MacKinnon et al. 2005), and variability of suicidal ideation was a significantly better predictor of prior suicide attempts than duration and intensity of ideation (Witte et al. 2005).
Hyperthymic temperament, on the other hand, may be protective through being associated with lower levels of hopelessness, as well as high energy, lifelong drive, ambition, and such social-interpersonal skills which enables more effective coping with inner and outer events and make the individual less vulnerable to mood changes contributing to more effective defence against impulses toward suicide (Pompili et al. 2008; Vazquez et al. 2010). It should be also noted that recently a strong relationship has been found between psychological resilience and hyperthymic temperament both in depressive and healthy individuals (Kesebir et al. 2013).
Furthermore, the biological substrate of the association between affective temperaments and suicidality may be carried by the presence of the “s” or short allele of the 5-HTTLPR polymorphism of the serotonin transporter gene, known to be associated with suicidal behaviour (Gonda et al. 2011b) and affective temperaments as well (Gonda et al. 2006). Even more interestingly, the s allele is also associated with other endophenotypes related to suicidal behaviour, such as aggressiveness (Gonda et al. 2011a) or neuroticism (Gonda et al. 2009); therefore this genetic polymorphism seems to convey some kind of general vulnerability, which, depending on complex gene x gene and longitudinal and cross-sectional gene x environment interactions, may be expressed in various forms predisposing to suicidal behaviour, including the marked manifestation of affective temperaments (Gonda et al. 2011a). Affective temperaments, especially the frequency of their presentation in dominant form, show a characteristic geographical distribution, which also shows and excitingly parallel pattern to the distribution of the score of cultural indexes described by Hofstede, which in turn has been related to prevalence of affective illness (Gonda et al. 2011c). Hofstede’s individualism-collectivism score was also found to show a parallel geographical distribution to the 5-HTTLPR s allele (Chiao and Blizinsky 2010). These above factors already outline a complex and delicate network of important and yet unidentified and undetected etiological factors in the background of suicidal behaviour, determining its biological as well as psychosocial factors. However, affective temperaments seem to play a central role in this multilevel network, mediating the effects of a possible genetic background and psychosocial determinants of suicidal behaviour both on the individual and possibly on a higher and more complex social level.
References
Akiskal HS (1996) The temperamental foundations of affective disorders. In: Mundt C, Freeman HL (eds) Interpersonal factors in the origin and course of affective disorders, Interpersonal Factors in the Origin and Course of Affective Disorders. Gaskell, London, pp 3–30
Akiskal HS, Mallya G (1987) Criteria for the “soft” bipolar spectrum: treatment implications. Psychopharmacol Bull 23(1):68–73
Akiskal HS, Djenderedjian AM, Rosenthal RH, Khani MK (1977) Cyclothymic disorder: validating criteria for inclusion in the bipolar affective group. Am J Psychiatry 134(11):1227–1233
Akiskal HS, Hirschfeld RM, Yerevanian BI (1983) The relationship of personality to affective disorders. Arch Gen Psychiatry 40(7):801–810
Akiskal HS, Hantouche EG, Allilaire JF (2003) Bipolar II with and without cyclothymic temperament: “dark” and “sunny” expressions of soft bipolarity. J Affect Disord 73(1–2):49–57
Akiskal HS, Akiskal K, Allilaire JF, Azorin JM, Bourgeois ML, Sechter D, Fraud JP, Chatenet-Duchene L, Lancrenon S, Perugi G, Hantouche EG (2005a) Validating affective temperaments in their subaffective and socially positive attributes: psychometric, clinical and familial data from a French national study. J Affect Disord 85(1–2):29–36. doi:10.1016/j.jad.2003.12.009
Akiskal HS, Akiskal KK, Haykal RF, Manning JS, Connor PD (2005b) TEMPS-A: progress towards validation of a self-rated clinical version of the temperament evaluation of the Memphis, Pisa, Paris, and San Diego autoquestionnaire. J Affect Disord 85(1–2):3–16. doi:10.1016/j.jad.2004.12.001
Azorin JM, Kaladjian A, Adida M, Hantouche E, Hameg A, Lancrenon S, Akiskal HS (2009) Risk factors associated with lifetime suicide attempts in bipolar I patients: findings from a French National Cohort. Compr Psychiatry 50(2):115–120. doi:10.1016/j.comppsych.2008.07.004
Bouchard TJ Jr (1994) Genes, environment, and personality. Science 264(5166):1700–1701
Braquehais MD, Oquendo MA, Baca-Garcia E, Sher L (2010) Is impulsivity a link between childhood abuse and suicide? Compr Psychiatry 51(2):121–129. doi:10.1016/j.comppsych.2009.05.003
Carballo JJ, Harkavy-Friedman J, Burke AK, Sher L, Baca-Garcia E, Sullivan GM, Grunebaum MF, Parsey RV, Mann JJ, Oquendo MA (2008) Family history of suicidal behavior and early traumatic experiences: additive effect on suicidality and course of bipolar illness? J Affect Disord 109(1–2):57–63. doi:10.1016/j.jad.2007.12.225
Chaudhury SR, Grunebaum MF, Galfalvy HC, Burke AK, Sher L, Parsey RV, Everett B, Mann JJ, Oquendo MA (2007) Does first episode polarity predict risk for suicide attempt in bipolar disorder? J Affect Disord 104(1–3):245–250. doi:10.1016/j.jad.2007.02.022
Chiao JY, Blizinsky KD (2010) Culture-gene coevolution of individualism-collectivism and the serotonin transporter gene. Proc Biol Sci/Roy Soc 277(1681):529–537. doi:10.1098/rspb.2009.1650
Engstrom C, Brandstrom S, Sigvardsson S, Cloninger CR, Nylander PO (2004) Bipolar disorder. III: harm avoidance a risk factor for suicide attempts. Bipolar Disord 6(2):130–138
Gonda X, Rihmer Z, Zsombok T, Bagdy G, Akiskal KK, Akiskal HS (2006) The 5HTTLPR polymorphism of the serotonin transporter gene is associated with affective temperaments as measured by TEMPS-A. J Affect Disord 91(2–3):125–131. doi:10.1016/j.jad.2005.12.048
Gonda X, Fountoulakis KN, Juhasz G, Rihmer Z, Lazary J, Laszik A, Akiskal HS, Bagdy G (2009) Association of the s allele of the 5-HTTLPR with neuroticism-related traits and temperaments in a psychiatrically healthy population. Eur Arch Psychiatry Clin Neurosci 259(2):106–113. doi:10.1007/s00406-008-0842-7
Gonda X, Fountoulakis KN, Csukly G, Bagdy G, Pap D, Molnar E, Laszik A, Lazary J, Sarosi A, Faludi G, Sasvari-Szekely M, Szekely A, Rihmer Z (2011a) Interaction of 5-HTTLPR genotype and unipolar major depression in the emergence of aggressive/hostile traits. J Affect Disord 132(3):432–437. doi:10.1016/j.jad.2011.03.029
Gonda X, Fountoulakis KN, Harro J, Pompili M, Akiskal HS, Bagdy G, Rihmer Z (2011b) The possible contributory role of the S allele of 5-HTTLPR in the emergence of suicidality. J Psychopharmacol 25(7):857–866. doi:10.1177/0269881110376693
Gonda X, Vazquez GH, Akiskal KK, Akiskal HS (2011c) From putative genes to temperament and culture: cultural characteristics of the distribution of dominant affective temperaments in national studies. J Affect Disord 131(1–3):45–51. doi:10.1016/j.jad.2010.12.003
Goto S, Terao T, Hoaki N, Wang Y (2011) Cyclothymic and hyperthymic temperaments may predict bipolarity in major depressive disorder: a supportive evidence for bipolar II1/2 and IV. J Affect Disord 129(1–3):34–38. doi:10.1016/j.jad.2010.07.016
Grunebaum MF, Ramsay SR, Galfalvy HC, Ellis SP, Burke AK, Sher L, Printz DJ, Kahn DA, Mann JJ, Oquendo MA (2006) Correlates of suicide attempt history in bipolar disorder: a stress-diathesis perspective. Bipolar Disord 8(5 Pt 2):551–557. doi:10.1111/j.1399-5618.2006.00304.x
Guerreiro DF, Sampaio D, Rihmer Z, Gonda X, Figueira ML (2013) Affective temperaments and self-harm in adolescents: a cross-sectional study from a community sample. J Affect Disord 151(3):891–898. doi:10.1016/j.jad.2013.07.034
Hantouche EG, Angst J, Demonfaucon C, Perugi G, Lancrenon S, Akiskal HS (2003) Cyclothymic OCD: a distinct form? J Affect Disord 75(1):1–10
Hawton K, van Heeringen K (2009) Suicide. Lancet 373(9672):1372–1381. doi:10.1016/S0140-6736(09)60372-X
Kesebir S, Gundogar D, Kucuksubasi Y, Tatlidil Yaylaci E (2013) The relation between affective temperament and resilience in depression: a controlled study. J Affect Disord 148(2–3):352–356. doi:10.1016/j.jad.2012.12.023
Kochman FJ, Hantouche EG, Ferrari P, Lancrenon S, Bayart D, Akiskal HS (2005) Cyclothymic temperament as a prospective predictor of bipolarity and suicidality in children and adolescents with major depressive disorder. J Affect Disord 85(1–2):181–189. doi:10.1016/j.jad.2003.09.009
Kraepelin E (1915) Psychiatrie. Ein Lehrbuch für Studierende und Arzte. J.A. Barth, Leipzig
Kretschmer E (1936) Psychique und Character. Kegan, Paul, Trench, Trubner and Co. Ltd, London
Luoma JB, Martin CE, Pearson JL (2002) Contact with mental health and primary care providers before suicide: a review of the evidence. Am J Psychiatry 159(6):909–916
MacKinnon DF, Potash JB, McMahon FJ, Simpson SG, Depaulo JR Jr, Zandi PP, National Institutes of Mental Health Bipolar Disorder Genetics I (2005) Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord 7(5):441–448. doi:10.1111/j.1399-5618.2005.00236.x
Mann JJ, Waternaux C, Haas GL, Malone KM (1999) Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry 156(2):181–189
Maser JD, Akiskal HS, Schettler P, Scheftner W, Mueller T, Endicott J, Solomon D, Clayton P (2002) Can temperament identify affectively ill patients who engage in lethal or near-lethal suicidal behavior? A 14-year prospective study. Suicide Life Threat Behav 32(1):10–32
Oquendo MA, Galfalvy H, Russo S, Ellis SP, Grunebaum MF, Burke A, Mann JJ (2004) Prospective study of clinical predictors of suicidal acts after a major depressive episode in patients with major depressive disorder or bipolar disorder. Am J Psychiatry 161(8):1433–1441. doi:10.1176/appi.ajp.161.8.1433
Pompili M, Rihmer Z, Akiskal HS, Innamorati M, Iliceto P, Akiskal KK, Lester D, Narciso V, Ferracuti S, Tatarelli R, De Pisa E, Girardi P (2008) Temperament and personality dimensions in suicidal and nonsuicidal psychiatric inpatients. Psychopathology 41(5):313–321. doi:10.1159/000146069
Pompili M, Innamorati M, Rihmer Z, Gonda X, Serafini G, Akiskal H, Amore M, Niolu C, Sher L, Tatarelli R, Perugi G, Girardi P (2012) Cyclothymic-depressive-anxious temperament pattern is related to suicide risk in 346 patients with major mood disorders. J Affect Disord 136(3):405–411. doi:10.1016/j.jad.2011.11.011
Rihmer Z (2007) Suicide risk in mood disorders. Curr Opin Psychiatry 20(1):17–22. doi:10.1097/YCO.0b013e3280106868
Rihmer Z, Gonda X (2013) Pharmacological prevention of suicide in patients with major mood disorders. Neurosci Biobehav Rev 37(10 Pt 1):2398–2403. doi:10.1016/j.neubiorev.2012.09.009
Rihmer A, Rozsa S, Rihmer Z, Gonda X, Akiskal KK, Akiskal HS (2009a) Affective temperaments, as measured by TEMPS-A, among nonviolent suicide attempters. J Affect Disord 116(1–2):18–22. doi:10.1016/j.jad.2008.10.024
Rihmer A, Szilagyi S, Rozsa S, Gonda X, Faludi G, Rihmer Z (2009b) A gyermekkori abúzusok szerepe a felnőttkori szuicid magatartás kialakulásában. Neuropsychopharmacologia Hungarica: a Magyar Pszichofarmakologiai Egyesulet lapja. Off J Hung Assoc Psychopharmacology 11:237–246
Rihmer Z, Akiskal KK, Rihmer A, Akiskal HS (2010) Current research on affective temperaments. Curr Opin Psychiatry 23(1):12–18. doi:10.1097/YCO.0b013e32833299d4
Skala K, Kapusta ND, Schlaff G, Unseld M, Erfurth A, Lesch OM, Walter H, Akiskal KK, Akiskal HS (2012) Suicidal ideation and temperament: an investigation among college students. J Affect Disord 141(2–3):399–405. doi:10.1016/j.jad.2012.03.010
Swann AC, Dougherty DM, Pazzaglia PJ, Pham M, Steinberg JL, Moeller FG (2005) Increased impulsivity associated with severity of suicide attempt history in patients with bipolar disorder. Am J Psychiatry 162(9):1680–1687. doi:10.1176/appi.ajp.162.9.1680
Vazquez GH, Gonda X, Zaratiegui R, Lorenzo LS, Akiskal K, Akiskal HS (2010) Hyperthymic temperament may protect against suicidal ideation. J Affect Disord 127(1–3):38–42. doi:10.1016/j.jad.2010.04.015
Witte TK, Fitzpatrick KK, Joiner TE Jr, Schmidt NB (2005) Variability in suicidal ideation: a better predictor of suicide attempts than intensity or duration of ideation? J Affect Disord 88(2):131–136. doi:10.1016/j.jad.2005.05.019
Young LT, Cooke RG, Robb JC, Joffe RT (1995) Double bipolar disorder: a separate entity. Depression 2:223–225
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Rihmer, Z., Gonda, X. (2016). Temperament in Suicidal Behaviour. In: Courtet, P. (eds) Understanding Suicide. Springer, Cham. https://doi.org/10.1007/978-3-319-26282-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-26282-6_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-26280-2
Online ISBN: 978-3-319-26282-6
eBook Packages: MedicineMedicine (R0)