
Abstract
We discuss five softwares commonly used for preoperative planning for high tibial osteotomy, namely MedWeb, TraumaCad, MediCad, Sectra and Photoshop. Each software has their own specialty and specification based on surgeon requirements. Detail of methods for each software is discussed. This paper aims to highlights the strength and weaknesses of the softwares. Our comparison shows that the selection of method to be used depends on the needs of the surgeon. The different software suitability discussed are axis used, users’ control capability, automatic wedge selection, CORA’s point, tibial slope, automatic measurement, and visualize correction. The results obtained from the comparative analysis are expected to aid in development innovative software for preoperative osteotomy planning, based on the strengths of each software discussed.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
- Software
- Preoperative planning
- Tibial slope
- Center of rotation of angulation (CORA)
- Mechanical axis
- Image dimension
- Visualize correction
1 Introduction
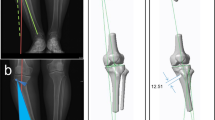
Osteotomy is an operation performed by orthopaedic surgeon to correct bone deformity. It happens when the human long bones are bent toward (valgus) or away(varus) from the midline of the human body. The bones that are commonly operated upon to are tibia, femur abd humerus (Fig. 1) The goal of an osteotomy is to realign the mechanical axis of the affected limb by shifting the eccentric loading forces back to its mechanical axis alignment. Shifting the loading forces to its normal mechanical axis is an important factor in determining the long-term outcome for patients’ satisfaction and relief [1]. This paper will only focuses on osteotomy of tibia, known as high tibial osteotomy or HTO.

Femur, tibia and humerus location
2 High Tibial Osteotomy
High tibial osteotomy (HTO) is one of the most reliable methods for the correction of proximal tibial deformity [2, 3]. This method has been used by surgeons all around the world in resolving tibia deformity where the tibia is sloping closer or away from the vertical plane of the human body. The deformity may occurs during childhood such as idiopathic tibia vara or due to malalignment following fracture malunion.
Manual pre-operative planning for HTO requires the surgeons to have a ruler, scissor, goniometer and the radiograph. As technology advances, many hospitals have changed their radiographic film to digital format. Hence, there is a need for software to handle the digital format.
Preoperative planning with computer aided process for HTO is an area where the technical design and development of human-computer interaction is a critical success factor. Careful preoperative planning for proximal tibial osteotomy is essential if the desired correction of alignment with long term satisfactory outcome is to be achieve [4, 5]. The existence of software that has a user-friendly interface and easy to meet surgeon’s specific requirements will facilitate a quicker and more efficient preoperative planning.
3 Methods of Study
This study is based on previous literature acquired by researchers. Researchers decided to discuss further five softwares with namely MedWeb, TraumaCad, MediCad, Photoshop and Sectra. Detailed features were selected based on the needs of preoperative planning of high tibial osteotomy’s routine such as the preparing of 2 and/or 3 dimension image, providing the mechanical or anatomical axis, how far users have control capability, selecting wedge, presenting CORA’s point on the image, displaying degree angle tibial slope, calculating for femoral-tibia is automatic, visualizing correction and either they providing computer navigation or not. Details will discuss further in different topics.
4 Computer Aided for Preoperative Planning Osteotomy
Since radiographic film has been digitized, preoperative planning with computer aided for this was created for the purpose of replacing manual methods and speed up the work procedures with more efficient results. Some of the strengths and issues of this study will be discussed.
4.1 TraumaCad
Austin Radiological Association in Israel introduced TraumaCad. This software is used for preoperative planning in various areas of orthopedic surgery, such as joint replacement, treatment of fractures, limb deformities in a population of children and adults, spine surgery, foot and ankle [6]. Patient management in pediatric orthopedic surgery depends on the radiographs interpretation and anatomical frame size measurement, angle, and index as an important adjunct to clinical examination. This software has a template of variable measurement tool to measure the correction osteotomy. The template is capable in measuring the length of the patient’s leg, the exact point of center of rotation of angulation (CORA), and also visualizes correction [7]. Figure 2(a) shows the interface of TraumaCad software.

(a-e) Software interface as discussed.
This software is capable of reading three-dimensional medical images [8], loaded for the purpose of scaling and magnification of the image automatically [9], and is the standard approach with two sizes of deformity correction template for osteotomy [6]. Tests were made by [6] on 57 patients using first size, it produces an accuracy of 87 % while the testing on 65 patients using second size produces an accuracy of 96 %.
Whereas according to the study of [9], the median error expansion in two size groups is 1.14 % when calculated automatically. The median size of a single error is 5.98 %. Relationship between actual and forecast growth is stronger in the double marker with a very good relationship (r = 0.91). Reference [10] in their study stated that TraumaCad was useful in preoperative hip template where it successfully predicts the components of the prosthesis within ±1 size in most waist studied. However, it should not be used as an absolute measurement for the size of the prosthesis to be used. This software is usually provided together with computer navigation to enhance the process in intra-operative.
4.2 MediCad
References [11, 13] were using the MediCad which was introduced by Hectec GmbH, Niederviehbach, German for the computer-aided analysis. This software has features to analyze alignment, joint orientation and long legs. It can also display the preoperative dimension automatically including related data [14]. MediCad provide corrective recommendations based on the line selection. Figure 2(b) shows a MediCad software. MediCad also has the measurement template, which is able to read two-dimensional and three-dimensional medical image for osteotomy correction. This software is also provided together with computer navigation to enhance the process in intra-operative.
4.3 Sectra
Sectra is the software, which was introduced by Sectra in Northern Ireland. This software is used to signify, simulate correction and creates a wedge angle for osteotomy correction. It provides five-point guides that will be used to determine the length of the foot (two-step), marking the resection line at the desired tibia (two steps), and simulate the selection of the wedge on the tibia (the fifth step). However, researcher found that there was no CORA point displayed to guide the surgeon. Display of the software is shown in Fig. 2(c). Sectra also has specific guidelines for completing the preoperative planning process.
4.4 MedWeb
This software allows the user to measure the total length of the patient’s leg on digital X-rays and shows the degree of the slope angle of the tibia, however the software does not allow determination of point of wedge center of rotation and angulation (CORA) and planning appropriate selection is made [15]. Figure 2(d) shows the interface of MedWeb.
4.5 Adobe Photoshop
Reference [12] discusses the advantages of using Adobe Photoshop 9, a professional graphics editing software for preoperative osteotomy. The study reported is that the software is able to create digital storage for preoperative planning, does require some line drawings and angle, easy to copy for the purpose of a few times planning but easy to compare between the process of preoperative planning and intraoperative decision, as well as it has the ability to display digital plan on the computer in the operating room. Nonetheless, researchers have found it quite difficult to record the angle correction automatically in which the required information must be entered manually in the image. Figure 2(e) shows the preoperative planning using Adobe Photoshop by [12].
5 Software Comparisons
See Table 1.
6 Discussion
The use of computed tomography (CT) for three dimension (3D) image is capable of producing clear and detailed images, but it will expose the patient to ionizing radiation at a relatively high dose [16], which is less suitable for children. Magnetic resonance imaging (MRI), which is said to produce similar quality images with CT, and has another advantage that is free of radiation, which is much safer for patients [17]. Nonetheless, the sedative should be given to the child in order for him to remain static until the completion of the imaging process. This is due to the range of time for as session is within an hour [18]. To that end, the researchers propose to use X-ray images using a two-dimensional (2D), offering advantages such as lower exposure dose per frame and a wider dynamic range [19].
Many established softwares are provided with axis to comfort users in planning process. However, it is not a big problems to expert users in determining the axes manually. Provision of software templates are very helpful in preoperative planning. Coupled with the convenience of auto-flexi, it really helps the surgeon to plan fast, precise, effective and more productive.
An Open or closed wedge osteotomies are the most commonly practiced. CORA is important in determining the angle of correction for tibial slope. While auto-visualise for corrective osteotomy is useful in helping surgeons in explaining to their patients on what happening before, during and after surgery. All these functions give advantages to the surgeon before performing the surgical correction. Computer navigation is a device which provided together with dedicated preoperative planning software, such as TraumaCad and MediCad. However, with the high cost compared to the number of patients per year, most hospitals in development countries cannot affort to buy this software.
The bones of each individual is unique and different from each other depending on gender, population, age, and body mass index (BMI) [20–23]. Reference [24] state that there is no way to be accurate and reliable in preoperative control towards the correction angle, the tibia slope, and the changes produced by osteotomy rotation. The tibia slope is not static and will constantly change from birth until a bone reach its maturity. This slope is also strongly influenced by differential among dominant or not of each person [25].
7 Conclusion
The study focuses in brief, five common softwares used for preoperative planning of an osteotomy. The comparison made was to study the different specification applied to implement preoperative planning for an osteotomy. The strength for the software will guide us to develop a better method, while the weaknesses will be avoided and overcome. Our future research will concentrate on the selection of the best method based on the preoperative planning for high tibial osteotomy.
References
Franco, V., Cerullo, G., Cipolla, M., Gianni, E., Puddu, G.: Open wedge high tibial osteotomy. Tech. Knee Surg. 11(2), 68–77 (2012)
Lorenz, S., Morgenstern, M., Imhoff, A.B.: Development of an image-free navigation tool for high tibial osteotomy. Oper. Tech. Orthop. 17(1), 58–65 (2007)
Picardo, N.E., Khan, W., Johnstone, D.: Computer-assisted navigation in high tibial osteotomy: a systematic review of the literature. Open Orthop. J. 6, 305–312 (2012)
De Mauro, A., Mazars, J., Manco, L., Mataj, T., Fernandez, A.H., Cortes, C., De Paolis, L.T.: Intraoperative navigation system for image guided surgery. In: 2012 Sixth International Conference on Complex, Intelligent, Software Intensive Systems, pp. 486–490 (2012)
Brown, G.A., Amendola, A.: Radiographic evaluation and preoperative planning for high tibial osteotomies. Oper. Tech. Sports Med. 20(1), 93–102 (2012)
Steinberg E.L., Segev, E.: Pre-operative planning using the TraumaCad software system. US Radiol pp. 87–91 (2010)
Voyant Health: Voyant Health, A Brainlab Company (2013). http://www.voyanthealth.com/news_press.jsp
Pilson, H.T., Reddix, R.N., Jr., Mutty, C.E., Webb, L.X.: The long lost art of preoperative planning—resurrected?. Orthop. 31(12), December 2008
Baxter, J.A., Barlow, T., Karthikeyan, S., Mayo, D.J., King, R.J.: The accuracy of automatic calibration of digital pelvic radiographs using two different scale markers: a comparative study. Hip Int. 22(1), 82–89 (2012)
Salisbury, H., Jain, N.P.M., Knowles, D.: Pre-operative templating of elective total hip replacement using TraumaCad software. J. Bone Jt. Surg. Br. 94(10) (2012). bjjprocs.boneandjoint.org.uk
Gebhard, F., Krettek, C., Hüfner, T., Grützner, P.A., Stöckle, U., Imhoff, A.B., Lorenz, S., Ljungqvist, J., Keppler, P., Messmer, P., Kahler, D.: Reliability of computer-assisted surgery as an intraoperative ruler in navigated high tibial osteotomy. Arch. Orthop. Trauma Surg. 131(3), 297–302 (2011)
Shiha, A., Krettek, C., Hankemeier, S., Liodakis, E., Kenawey, M.: The use of a professional graphics editing program for the preoperative planning in deformity correction surgery: a technical note. Injury 41(6), 660–664 (2010)
Heijens, E., Kornherr, P., Meister, C.: The role of navigation in high tibial osteotomy: a study of 50 patients. Orthopedics 32(10 Suppl), 40–43 (2009)
Hectec: MediCad, the orthopedic solution (2013). http://www.hectec.de/content/index.php/us/
Abdul Rashid, A.H.: Permasalahan Perancangan Prabedah Osteotomi PPUKM (2013)
Viceconti, M., Lattanzi, R., Antonietti, B., Paderni, S., Olmi, R., Sudanese, A., Toni, A.: CT-based surgical planning software improves the accuracy of total hip replacement pre-operative planning. Med. Eng. Phys. 25(5), 371–377 (2003)
Utzschneider, S., Goettinger, M., Weber, P., Horng, A., Glaser, C., Jansson, V., Müller, P.E.: Development and validation of a new method for the radiologic measurement of the tibial slope. Knee Surg. Sports Traumatol. Arthrosc. 19(10), 1643–1648 (2011)
Abd Hamid, H.: Pengimejan Perubatan bagi Keperluan Perancangan Pembetulan Osteotomi, Kuala Lumpur (2013)
Dance, D. R.: Digital X-ray imaging. In: Molecular Imaging: Computer Reconstruction and Practice (2008)
Lee, D.-H., Nha, K.-W., Park, S.-J., Han, S.-B.: Preoperative and postoperative comparisons of navigation and radiologic limb alignment measurements after high tibial osteotomy. Arthroscopy 28(12), 1842–1850 (2012)
Masrouha, K.Z., Sraj, S., Lakkis, S., Saghieh, S.: High tibial osteotomy in young adults with constitutional tibia vara. Knee Surg. Sport Traumatol. Arthrosc. 19(1), 89–93 (2011)
Olin M.D., Vail, T.P.: High tibial osteotomy : will new techniques provide better results? pp. 8–12 (2001)
Tang, Y., Zhu, Y., Chiu, K.: Axial alignment of the lower extremity in Chinese adults. J. Bone Jt. Surg. Am. 82, 1603–1608 (2000)
Menetrey, J., Duthon, V., Fritschy, D.: Computer-assisted open-wedge high tibial osteotomy. Oper. Tech. Orthop. 18(3), 210–214 (2008)
Hohmann, E., Bryant, A.: Closing or opening wedge high tibial osteotomy: watch out for the slope. Oper. Tech. Orthop. 17, 38–45 (2007)
Acknowledgment
This research project was conducted in collaboration with Associate Prof Dr. Abdul Halim Abdul Rashid from the Department of Orthopedic and Traumatology, Medical Centre of University Kebangsaan Malaysia. This research was also funded by the University Grants UKM-GUP-2015-004.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this paper
Cite this paper
Awang, N., Sulaiman, R., Shapi’i, A., Rashid, A.H.A., Amran, M.F.M., Osman, S. (2015). A Comparative Study of Computer Aided System Preoperative Planning for High Tibial Osteotomy. In: Badioze Zaman, H., et al. Advances in Visual Informatics. IVIC 2015. Lecture Notes in Computer Science(), vol 9429. Springer, Cham. https://doi.org/10.1007/978-3-319-25939-0_17
Download citation
DOI: https://doi.org/10.1007/978-3-319-25939-0_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-25938-3
Online ISBN: 978-3-319-25939-0
eBook Packages: Computer ScienceComputer Science (R0)