
Abstract
The approach to interventional airway management must be consistent and disciplined. This chapter will describe one method to assess the airway and potentially predict which ones could be difficult and require additional interventions to secure and protect. In addition, assessments for difficult bag mask ventilation, laryngoscopy, extraglottic devices, and surgical interventions will be discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Assessment of the Airway
Assessment of respiratory distress and subsequent need to control the airway in the ICU setting is a very common occurrence. The distinction between ventilation and oxygenation must be assessed and are both managed differently. The focus of this chapter will be on the assessment and management of the airway.
The failure to identify and recognize a difficult airway is the single most common cause of a failed airway. A failed airway may be defined as:
-
Failure to maintain saturations (>90 % SpO2).
-
Three failed intubation attempts.
There are four dimensions of predicting difficult airway management [1]—they include:
-
Predicting difficult BVM ventilation (MOANS).
-
M = Mask seal (any difficulty with obtaining a mask seal).
-
O = Obesity (redundant posterior pharyngeal tissue).
-
A = Age > 55 (loss of muscular tone).
-
N = No teeth.
-
S = Snores/stiff lungs (COPD, pneumothorax, etc.).
-
-
Predicting difficult intubation (LEMONS).
-
L = Look externally (evaluate for trauma, landmarks).
-
E = Evaluate 3–3–2.
-
Three of patients’ fingers between incisors (access).
-
Three fingers between tip of chin and chin–neck junction (compression space for tongue).
-
Two fingers between chin–neck junction and top of laryngeal cartilage (location of airway).
-
-
M = Mallampati score (1–4) (see Fig. 6.1).
Fig. 6.1 
Mallampati score . North Seattle University [Internet]. Seattle. Cited April 24, 2015. Retrieved from public domain images at: http://facweb.northseattle.edu/cduren/North%20Seattle%20AT%20Program%202011-2012%20CJ%20Duren-Instructor/ATEC%20002%20Anesthesia%20Related%20Anatomy%20and%20Physiology/Week%203/Additional%20Week%203%20Lesson%20Resources/Mallampati%20Score-Mallampati%20Classification%20Picture.png
-
O = Obstruction
-
N = Neck mobility (limited—i.e., C-collar in place).
-
S = Saturations (keep above 90 %).
-
-
Predicting difficult extraglottic devices (RODS).
-
R = Restricted mouth opening (<3 cm).
-
O = Obstruction at larynx.
-
D = Disrupted/distorted anatomy.
-
S = Snores/stiff lungs.
-
-
Predicting difficult surgical airway (SMART).
-
S = Surgeries (previous).
-
M = Mass.
-
A = Access difficulties (obesity).
-
R = Radiation (previous or current).
-
T = Tumor.
-

Since 1956, clinicians have been searching for the perfect way to predict airway management difficulty. Studies have looked at various airway geometry indicators, anatomical predictors, and imaging studies. There is no one “fool proof” method.
2 Pharmacology Decision Points
There are multiple pharmacologic decision points when the decision has been made to perform endotracheal intubation. These include pretreatment medications, sedation medications, paralytic agents, and finally longer-acting sedatives and possible longer-acting paralytic agents.
3 Pretreatment Medications
The decision to use these medications is generally made by the person directing the intubation process. If being supervised for this procedure, check with the clinician responsible for the procedure and verify if they choose to use one of these medications.
The mnemonic LOAD may be used when considering pretreatment medications:
-
Lidocaine is often used when brain injury is a possibility. Dose, 1.5 mg/kg IVP (at least 3 min before the intubation procedure).
-
Opioid may be considered if time permits. Morphine, 5–10 mg IVP on an adult-sized patient, or fentanyl, 0.5–1 mcg/kg IV (given slowly over 1–2 min), may be omitted if patient is hypotensive (SBP < 90) or dependent upon sympathetic drive for hemodynamics.
-
Atropine may be needed if the patient develops non-hypoxemic bradycardia; dose, 0.5–1.0 mg IV; may be repeated if needed.
-
Defasciculating dose of a noncompeting neuromuscular paralytic.
4 Sedation/Induction Medications
Common induction medications used for rapid sequence intubation (RSI) include:
-
Etomidate—0.3 mg/kg IV, best hemodynamic profile, short acting.
-
Versed—0.1 mg/kg IV.
-
Ativan—5–10 mg IV on an adult-sized patient, longer acting.
-
Ketamine—1.5 mg/kg IV, used in patients with asthma.
-
Propofol—1.5 mg/kg IV, monitor for hypotension.
5 Paralytics
Paralytics come in two varieties:
-
Depolarizing (succinylcholine).
-
Non-depolarizing (rocuronium and vecuronium are examples).
6 Depolarizing Muscle Paralytics
Succinylcholine is actually two-acetylcholine molecules linked together. It has a rapid onset (30–60 s) and relatively short half-life (3–5 min). It is metabolized by the enzyme acetylcholinesterase. There are some populations that have an acetylcholinesterase deficiency. In those cases, the effects of succinylcholine may last longer. The primary advantage of using succinylcholine is that if you are unable to get the patient intubated, with its short half-life, the medication will be metabolized, and the patient should resume spontaneous respirations within 3–5 min.
The dose of succinylcholine is 1.5 mg/kg. The dose is never reduced. It has no effect on hemodynamics.
There are some contraindications to using succinylcholine. They include:
-
History of malignant hyperthermia.
-
Burns >5 days—until healed.
-
Crush injury to large muscle mass >5 days.
-
Spinal cord injury/stroke with hemi- or paraplegia >5 days to 6 months.
-
Neuromuscular disease.
-
History of hyperkalemia/dialysis patients.
7 Non-Depolarizing Paralytics
There are many choices. Two will be covered here. Rocuronium is the paralytic of choice when succinylcholine is contraindicated. It has an onset of 60 s and a half-life of 30–45 min. It is given at a dose of 1.0 mg/kg IV push after the administration of an appropriate induction agent has been administered.
The second non-depolarizing agent that may be given is vecuronium. It has an onset of 3 min and a half-life of 60–75 min. The intubation dose of vecuronium is 0.15 mg/kg IV push after the administration of an appropriate induction agent has been administered.
8 The RSI Procedure
The RSI procedure has been described as the seven “Ps” [2]. They are:
-
Preparation.
-
Monitors (ECG, SpO2, EtCO2, BP), IV access, equipment, suction.
-
-
Preoxygenation.
-
3 min of 100 % FiO2 (or 8 vital capacity breaths).
-
-
Pretreatment.
-
Lidocaine (if suspected head injury or asthma)—3 min before intubation to be effective.
-
Opioid (fentanyl for CV disease or head injury).
-
Atropine (ready for non-hypoxemic bradycardia).
-
Defasciculating dose of paralytic.
-
-
Paralysis—induction agent and muscular paralytic given rapid IV push.
-
Remember—if no opioid was given, the induction agent and muscular paralytic have no effect on pain sensation.
-
-
Protection and positioning.
-
Sniffing position and cricoid pressure.
-
-
Placement of airway.
-
Confirm endotracheal tube placement with EtCO2, SpO2, breath sounds bilaterally, no sounds over epigastrium; secure the endotracheal tube.
-
-
Post-intubation management.
-
Additional longer-acting sedation and muscular paralysis if needed; consider pain medication, hemodynamic and oxygenation monitoring, and appropriate ventilator settings.
-
9 Indications for Intubation
-
Poor anticipated clinical course.
-
Glasgow Coma Scale of 8 or less.
-
Failure to maintain adequate oxygenation and/or ventilation.
10 Contraindications for Intubation
-
Patient able to maintain airway patency, ventilation, and oxygenation.
11 Complications
-
Hypotension.
-
Failed recognition of an esophageal intubation.
-
Damage to airway structures during attempt.
-
Damage to teeth.
12 Intubation Equipment
-
Oxygen, suction, oropharyngeal or nasopharyngeal airways (Figs. 6.2 and 6.3).
Fig. 6.2 
Oropharyngeal airway
Fig. 6.3 
Nasopharyngeal airway
-
Monitoring equipment (ECG, SpO2, B/P, respiratory rate, ETCO2).
-
Bag valve mask and/or non-rebreather oxygen mask.
-
Endotracheal tubes.
-
For most adult patients, consider sizes 7.0, 7.5, and 8.0.
-
-
Endotracheal tube stylet.
-
Laryngoscope handle (contact versus fiber optic) Fig. 6.4.
Fig. 6.4 
Fiber optic on the left and contact on the right (note green band) (no green band)
-
Laryngoscope blade.
-
10 ml syringe (for ET tube cuff).
-
Commercial ET tube holder or ET tape.
-
Color metric capnometer or qualitative end-tidal CO2 monitor.
-
Gum elastic bougie.





13 Procedure
-
1.
Assure patient is connected to appropriate monitors and adequate IV access is achieved. Assemble equipment and suction.
-
2.
If the patient is breathing at an adequate rate and volume, assure appropriate preoxygenation by utilizing a non-rebreather mask for at least 3 min (Fig. 6.7). If the patient is not breathing at an adequate rate or volume (minute ventilation), assist ventilations with a BVM device after placing an oropharyngeal or nasopharyngeal airway and applying cricoid pressure to reduce the incidence of gastric insufflation (Fig. 6.8). Preoxygenate with 100 % oxygen for a minimum of 3 min or 8 vital capacity breaths (Figs. 6.9 and 6.10).
Fig. 6.7 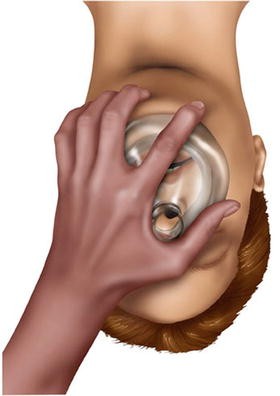
Assure good mask seal
Fig. 6.8 
Thumb and Index finger form the letter C; other three fingers form the letter E
Fig. 6.9 
Assure good seal - two hand technique
Fig. 6.10 
Jaw-thrust and mask seal
-
3.
If the intubator chooses to use a pre-intubation medication such as lidocaine, opioid, atropine, or a defasciculating dose of a neuromuscular blocker, now is the time to administer these medications.
-
4.
The selection and dosage of the sedative and neuromuscular blocker should be made at this point. Remember, for hemodynamic instability (SBP < 90 mmHg), the sedative should be half-dosed. The neuromuscular blocker is never given at a reduced dose. Rapid sequence induction or intubation is given its name because the sedative is given rapid IV push followed immediately by the neuromuscular blocker IV push. Check for muscle flaccidity.
-
5.
Insert the blade of choice and sweep the tongue from right to left.
-
(a)
If the Macintosh (curved) blade is used, the tip of the blade is placed at the base of the tongue (Fig. 6.11), and the mandible is displaced anteriorly until the epiglottis is raised to easily visualize the vocal cords.
Fig. 6.11 
Macintosh blade at base of tongue
-
b.
If the Miller (straight) blade is used, the tip of the blade is placed under the epiglottis (Fig. 6.12) and is used to elevate the epiglottis to visualize the cords.
Fig. 6.12 
Miller blade lifting the epiglottis
-
(a)
-
6.
The endotracheal tube, with stylet in place and not extending beyond the tip of the ETT, is placed in the trachea under direct visualization. The ETT is placed at a depth of approximately three times the size of the ETT. For example, if placing an 8.0 ETT, it should be inserted to a depth of 24 cm at the teeth or lips. The stylet is removed, the cuff inflated, and confirmation assured by one of the following methods: ETCO2 capnography, colorimetric capnography, auscultation of bilateral breath sounds and no sounds over the epigastrium with bag-assisted ventilations, or condensation in the ETT. Wave form qualitative capnography is considered the “gold standard” for proof of correct placement.
-
7.
Once correct placement is confirmed, the ETT should be secured with a commercial ETT tube holder or ETT tape. A post-intubation chest X-ray should be ordered to confirm correct depth of the ETT.






14 Summary
Only after a comprehensive airway assessment has been completed and the provider has determined the risks and benefits of RSI should the procedure be performed. It is just as important to recognize which patient to proceed with the RSI procedure as to whom not to. Airway management is very similar to the game of Chess—the provider must be thinking three and four steps ahead. If this fails, what is plan B and plan C? In many cases, it is wise for the provider to already have prepared the equipment that will be needed in the event of failing to secure the airway for those patients that have been deemed difficult. This is often referred to as a “double setup.”
Failure to recognize an esophageal intubation in a timely fashion can be fatal. When in doubt regarding airway placement, nothing beats direct laryngoscopy to assure correct tube placement. In the following chapter, we will discuss rescue airway devices and their use.
References
Walls R, Murphy M. The difficult and failed airway. In: Walls R, Murphy R, editors. Manual of emergency airway management. Philadelphia: Wolters Kluwer Lippincott Williams & Wilkins; 2012. p. 9–21.
Walls R. Rapid sequence intubation. In: Walls R, Murphy R, editors. Manual of emergency airway management. Philadelphia: Wolters Kluwer Lippincott Williams & Wilkins; 2012. p. 221–32.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Taylor, D.A., Heffner, A., Sing, R.F. (2016). Airway Management in the ICU. In: Taylor, D., Sherry, S., Sing, R. (eds) Interventional Critical Care. Springer, Cham. https://doi.org/10.1007/978-3-319-25286-5_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-25286-5_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-25284-1
Online ISBN: 978-3-319-25286-5
eBook Packages: MedicineMedicine (R0)