
Abstract
Pectus Carinatum (PC) or protrusion deformity of the chest wall accounts for 5 % of all chest wall deformities affecting 1 in 2500 live births (Ravitch, Congenital deformities of the chest wall and their operative correction. WB Saunders, Philadelphia, 1977). It is also know as pigeon chest. It can be unilateral, bilateral or mixed and there is predominance in males (Robicsek, Chest Surg Clin N Am 10(2):357–76, 2000).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
Pectus carinatum (PC) or protrusion deformity of the chest wall accounts for 5 % of all chest wall deformities affecting 1 in 2500 live births [1]. It can be unilateral, bilateral or mixed and there is predominance in males with a ration 4:1 [2]. However in some areas PC is almost equally or more frequent than PE [3, 4]. PC has not attributed the same interested as PE and the majority of the clinicians and thoracic surgeons are still unaware of surgical or conservative management options available. Since PC is rarely noticed at birth it is believed to be acquired rather than congenital. In most of cases it is perceived by the age of 10, is accentuated at puberty and reaches its peak at the ages of 16 and 18 respectively in female and male [3]. On the other hand a congenital association can be established by the following: presence at birth [4]; association with Marfan syndrome, congenital heart disease and hand agenesis [5]; observation in monozygotic twins [6, 7]; occurrence in more than two members in the same family. An association with reflux and mitral stenosis or prolapse has also been reported [8]. Another theory includes exaggerated growth of the cartilages [9, 10]. In PC an anterior growth can pull the sternum. Depending the location of the protrusion PC can be classified into the two following types:
-
Inferior PC or chondrogladiolar (chicken breast or pigeon breast): It is the most frequent type and characterize by a prominent sternum mainly in its mid and lower portion. In almost all cases is associated with lower bilateral costal depression. It is more often symmetric (Figs. 5.1, 5.2, and 5.3).
Figs. 5.1, 5.2, and 5.3 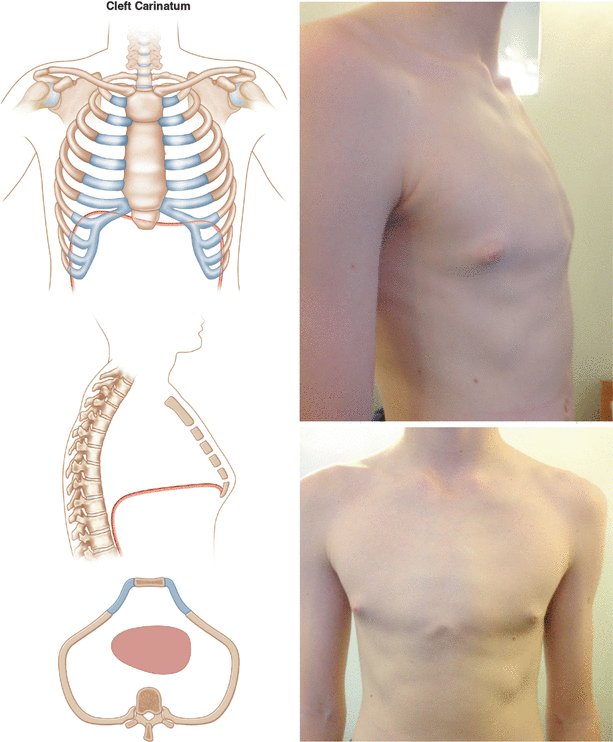
Inferior PC or chondrogladiolar (chicken breast or pigeon breast): It is the most frequent type and characterize by a prominent sternum mainly in its mid and lower portion. In almost all cases is associated with lower bilateral costal depression. It is more often symmetric
-
Superior PC or chondromanubrium (pouter pigeon or Currarino & Silverman syndrome): It consists of upper protrusion of the sternal notch that is proximal to midsternum and lower pseudo depression. It is subdivided to upper PC with midsternum depression and without midsternuml depression [11].

Clinically the deformity presents a typical progressive growth and can be accompanied by cardiovascular and respiratory symptoms similar to PE. These usually include palpitations, dyspnoea, wheezing with exertion and reduced exercise tolerance. Usually the cardiac and pulmonary function are less implicated than in PE but psychological effects of PC can be severe and responsible for low self esteem [12] leading to the necessity of a surgical correction.
References
Nuss D, Croitoru DP, Kelly RE. Congenital chest wall deformities. In: Ashcraft KW, Holcomb III GW, Murphy JP, editors. Pediatric surgery. 4th ed. Philadelphia: Elsevier Saunders; 2005. p. 245–63.
Shamberger RC, Welch KJ. Surgical correction of pectus carinatum. J Pediatr Surg. 1987;22:48–53.
Acastello E. Patologias de la pared toracica en pediatria. Buenos Aires: Editorial El Ateneo; 2006.
Martinez-Ferro M, Fraire C, Bernard S. Dynamic compression system for the correction of pectus carinatum. Semin Pediatr Surg. 2008;17(3):194–200.
Lodi R, Bondioli A, Curti L, Bruni GC, Palmieri B. Surgical correction of the pectus excavatum and carinatum in the adult. Report of an unusual case of combination of the straight back and pectus excavatum. Minerva Chir. 1975;30(3):131–8.
Currarino G, Silverman FN. Premature obliteration of sternal suture and pigeon-breast deformity. Radiology. 1958;70(4):532–40.
Lam CR, Taber RE. Surgical treatment of pectus carinatum. Arch Surg. 1971;103(2):191–4.
Chidambaram B, Mehta AV. Currarino-Silverman syndrome (pectus carinatum type 2 deformity) and mitral valve disease. Chest. 1992;102(3):780–2.
Lester CW. Pigeon breast (pectus carinatum) and other protrusion deformities of the chest of developmental origin. Ann Surg. 1953;137(4):482–9.
Ravitch MM. Congenital deformities of the chest wall and their operative correction. Philadelphia: WB Saunders; 1977.
Robicsek F. Surgical treatment of pectus carinatum. Chest Surg Clin N Am. 2000;10(2):357–76.
Fonkalsrud EW, Anselmo DM. Less extensive techniques for repair of pectus carinatum: the undertreated chest deformity. J Am Coll Surg. 2004;198(6):898–905.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Kolvekar, S.K., Panagiotopoulos, N. (2016). Pectus Carinatum. In: Kolvekar, S., Pilegaard, H. (eds) Chest Wall Deformities and Corrective Procedures. Springer, Cham. https://doi.org/10.1007/978-3-319-23968-2_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-23968-2_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23966-8
Online ISBN: 978-3-319-23968-2
eBook Packages: MedicineMedicine (R0)