
Abstract
The skin is home to a wide variety of unique epithelial, mesenchymal, and hematopoietic neoplasms as well as a frequent site of involvement with systemic neoplasia. This chapter focuses on those entities that arise primarily in the skin, with distinction made between the often different biologic behavior of cutaneous neoplasms and their systemic counterparts, where applicable. The chapter concludes with a detailed examination of immunodermatology in the modern era with a focus on immunobullous and connective tissue diseases.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
Cutaneous Neoplasms and Developmental Anomalies
Epithelial Neoplasms and Developmental Anomalies
Cystic Lesions: Neoplastic or Developmental
Epidermoid Cyst (Infundibular Cyst )
Clinical
-
♦
Dome-shaped lesions with central punctum; multiple lesions may be associated with Gardner syndrome
Microscopic
-
♦
Dermal cyst with/without an epidermal connection lined by stratified squamous epithelium with a granular layer; cyst contains laminated keratin debris
Comedonal Cyst
Microscopic
-
♦
Similar to the epidermoid cyst but characterized by follicular plugging and hyperkeratosis; may be more superficial and typically has a larger epidermal ostia or punctum
Milia
Clinical
-
♦
Small white-yellow papules which may occur sporadically or in association with blistering diseases (epidermolysis bullosa, porphyria cutanea tarda, pemphigoid, etc.) which disrupt or occlude the eccrine ducts or hair follicles
Microscopic
-
♦
A small epidermoid-like cyst located in the superficial dermis
Steatocystoma (Fig. 18.1)

Steatocystoma (A, B).
Clinical
-
♦
May occur in a solitary form (simplex) or as multiple lesions inherited in an autosomal dominant fashion (multiplex)
Microscopic
-
♦
An irregular, collapsed, intradermal cyst lined by a stratified squamous epithelium with an irregular, corrugated internal cuticle. Sebaceous glands are usually evident in the duct walls, and the cyst contains proteinaceous debris but no keratin
Dermoid Cyst
Clinical
-
♦
An embryonic closure defect that typically involves the skin lateral to the eye, the scalp, the neck, or near the mastoid process. Usually detected early in life
Microscopic
-
♦
A unilocular dermal or subcutaneous cyst lined by stratified squamous epithelium and having hair follicles, glands, and, sometimes, smooth muscle in the cyst wall
Cysts Associated with Branchial Cleft Deformities
Clinical
-
♦
Cystic lesions may be formed in and around the ear in association with branchial cleft deformities. These differ from the branchial cleft cyst of the neck by their location and their microscopic characteristics
Microscopic
-
♦
May be similar to an epidermoid cyst except for their tendency to collapse and assume a multiloculated appearance. Other forms, in addition to the above, have adnexal structures and even cartilage within their walls
Branchial Cleft Cyst
Clinical
-
♦
A developmental anomaly presenting as a cyst in the lateral aspect of the neck
Microscopic
-
♦
A lymphoepithelial cyst characterized by a stratified squamous or a pseudostratified ciliated lining with a dense lymphocytic infiltrate with germinal centers in the wall
Eruptive Vellus Hair Cyst
Clinical
-
♦
Small flesh-colored papules in children and young adults
Microscopic
-
♦
An epidermoid-like cyst that contains numerous, small vellus hairs
Pigmented Terminal Hair Cyst
Microscopic
-
♦
An epidermoid-like cyst containing numerous pigmented, terminal hairs
Trichilemmal (Pilar) Cyst
Clinical
-
♦
Dome-shaped papules/nodules found predominantly on the scalp; may be single or multiple
Microscopic
-
♦
A dermal or subcutaneous cyst lined by an eosinophilic stratified squamous epithelium that lacks a granular layer. The cyst contents are composed of solid, nonlaminated keratin
Proliferating Trichilemmal Cyst/Tumor (Fig. 18.2)

Proliferating trichilemmal cyst/tumor (A, B).
Clinical
-
♦
Multinodular scalp lesion more common in females
Microscopic
-
♦
Well-defined, multilobular tumor with trichilemmal keratinization; dense fibrous tissue surrounds the individual lobules; cystic areas may be inconspicuous
-
♦
Malignant forms occur but are rare
-
♦
More marked infiltration, cytologic atypia, and mitotic activity characterize the malignant variants
Bronchogenic Cyst
Clinical
-
♦
A developmental cyst usually found near the precordium early in life
Microscopic
-
♦
This cystic lesion attempts to recapitulate the bronchi with a cyst lined by respiratory epithelium and a cyst wall with smooth muscle, glands, and/or cartilage
Thyroglossal Duct Cyst
Clinical
-
♦
A developmental cyst found in the midline of the neck, near the hyoid bone
Microscopic
-
♦
The cyst may be lined by cuboidal, columnar, or stratified squamous epithelium
-
♦
The cyst wall contains thyroid follicles with or without skin appendages and lymphocytic inflammation
-
♦
Smooth muscle and cartilage are absent
Cutaneous Ciliated Cyst
Clinical
-
♦
Usually found on the lower extremities or buttocks of reproductive-aged women
Microscopic
-
♦
Ciliated, cuboidal, to columnar lined, multiloculated cyst surrounded by fibrous tissue
-
♦
No endometrial or fallopian tube-type stroma is evident within the cyst walls
Endometriosis and Endosalpingiosis
Clinical
-
♦
Blue-red cysts/nodules most commonly seen in the vulvar or periumbilical regions of reproductive-aged females
Microscopic
-
♦
Similar to the cutaneous ciliated cyst, except that the cyst wall contains endometrial/fallopian tube-type stroma with or without hemosiderin deposition
Hidrocystoma
Microscopic
-
♦
Unilocular or multilocular cysts lined by either apocrine or eccrine epithelium
-
Apocrine: decapitation secretion (apical snouts) and a myoepithelial layer; may have papillary projections
-
Eccrine: a two-layered cuboidal epithelium with no myoepithelial layer or decapitation secretion
-
Hybrid Cyst
Microscopic
-
♦
A cystic lesion combining the histologic features of more than one cyst type, usually trichilemmal and epidermoid cysts
Digital Mucous Cyst (Fig. 18.3)

Digital mucous cyst.
Clinical
-
♦
A fluctuant, sometimes tender, translucent nodule of the digits
Microscopic
-
♦
Dermal mucin deposited into a cyst-like space that may or may not also contain fibroblasts and collagen
-
♦
There is no true epidermal lining, and the cystic spaces may be multiloculated
Oral Mucocele
Clinical
-
♦
A translucent, blue nodule usually found on the lower lip
Microscopic
-
♦
A cystic space containing varying degrees of central mucin and lined by chronic inflammatory cells with numerous foamy histiocytes
-
♦
There is no true epithelial lining
Epidermal Tumors and Proliferations
Actinic Keratosis (Senile, Solar)
Clinical
-
♦
White-yellow, erythematous, and scaly patches or plaques on sun-damaged skin; some may be pigmented
Microscopic
-
♦
While a variety of histologic types exist, all have in common epidermal dysplasia, which may also involve the hair follicles
-
♦
Hyperplastic, atrophic, acantholytic, epidermolytic, lichenoid, pigmented, bowenoid, and clear cell categories exist and reflect additional alterations to the dysplastic epidermis (e.g., lichenoid variant = actinic keratosis with a band-like lymphocytic inflammatory infiltrate; bowenoid variant = actinic keratosis with full-thickness dysplasia = carcinoma in situ)
Benign Lichenoid Keratosis (Fig. 18.4) (Lichen Planus-Like Keratosis)

Benign lichenoid keratosis.
Clinical
-
♦
Solitary papule or plaque found primarily on the trunk or upper extremities
Microscopic
-
♦
Very similar to lichen planus with a dense band-like lymphocytic infiltrate at the dermal–epidermal interface with basilar vacuolar degeneration and cytoid bodies
-
♦
In contrast to lichen planus, eosinophils and parakeratosis may be seen
-
♦
In contrast to a lichenoid actinic keratosis, there is no keratinocyte dysplasia
Seborrheic Keratosis
Clinical
-
♦
Brown, elevated, and sharply demarcated lesions which occur most commonly on the face, trunk, and upper extremities
-
♦
These benign tumors often have a “stuck-on” appearance and are more common in middle-aged and older adults
-
♦
The sudden appearance of numerous seborrheic keratosis in association with visceral malignancy is referred to as the Leser–Trelat sign
Microscopic
-
♦
An epidermal proliferation of bland basaloid and polygonal keratinocytes associated with prominent keratin cyst formation
-
♦
The lesion is sharply delineated at its base and appears to grow up from the epidermis
-
♦
Irritated forms demonstrate more endophytic growth and form numerous squamous eddies
-
♦
Acanthotic, adenoid, clonal, pigmented, and hyperkeratotic variants exist
Inverted Follicular Keratosis (Fig. 18.5)

Inverted follicular keratosis.
Microscopic
-
♦
An endophytic epidermal growth with numerous squamous eddies which, like seborrheic keratosis, is sharply delineated but is centered on the hair follicles
-
♦
Note: This entity is considered a variant of seborrheic keratosis by some experts and a viral-induced lesion by others
Warty Dyskeratoma (Fig. 18.6)

Warty dyskeratoma.
Clinical
-
♦
A benign, solitary, umbilicated nodule or papule on sun-exposed skin
Microscopic
-
♦
A hair follicle-centered, endophytic squamous proliferation which is sharply delineated
-
♦
The base of the lesion typically reveals elongated trabeculae with varying degrees of dyskeratosis that underlies broad areas of acantholytic dyskeratosis located immediately below a keratin-filled, central crater
Linear Epidermal Nevus
Clinical
-
♦
Localized and systemic forms exist and are characterized by a linear arrangement of closely set papillomatous papules
-
♦
The systemic form may be associated with other defects, including skeletal and central nervous system abnormalities
Microscopic
-
♦
Both variants demonstrate epidermal papillomatosis, acanthosis, and hyperkeratosis
-
♦
Many histologic variants exist, but, importantly, the presence of epidermolytic hyperkeratosis may be associated with systemic involvement
Nevus Comedonicus
Clinical
-
♦
Comedo-like papules with a central keratin plug usually in a linear arrangement on the palms, soles, or other sites
Microscopic
-
♦
Deep epidermal invaginations with laminated keratin similar to a comedo
-
♦
Epidermolytic hyperkeratosis may be evident
White Sponge Nevus
Clinical
-
♦
Extensive, white patches and plaques involving mucosal sites (chiefly oral but also vaginal, rectal, and esophageal) which are evident early in life and are inherited in an autosomal dominant pattern
Microscopic
-
♦
There is acanthosis and pallor of the mucosal lining due to prominent cytoplasmic clearing (intracellular edema) of the suprabasilar keratinocytes
-
♦
Similar changes are seen in leukoedema and pachyonychia congenita
Leukoedema
Clinical
-
♦
Patchy white plaques and patches of the oral mucosa with an adult onset
-
♦
These lesions remit and recur and are not inherited
Microscopic
-
♦
Similar to white sponge nevus from which it differs by clinical grounds
Geographic Tongue (Lingua Geographica )
Clinical
-
♦
Irregular, erythematous patches with white borders on the tongue
Microscopic
-
♦
The erythematous areas show loss of the normal granular and horny layers, while the white areas demonstrate acanthosis with neutrophilic inflammation
Clear Cell Acanthoma (Fig. 18.7)

C lear cell acanthoma (A, B).
Clinical
-
♦
Solitary, slowly growing nodules or plaques with an oozing surface
-
♦
These lesions are most common on the lower extremities
Microscopic
-
♦
A platelike epidermal thickening by a proliferation of clear, heavily glycogenated keratinocytes
-
♦
The tumors are sharply demarcated from the adjacent epidermis (eyeliner sign) and, characteristically, have neutrophils scattered throughout the proliferation, an important feature in separating this entity from other tumors with a platelike growth pattern
Large Cell Acanthoma
Clinical
-
♦
Erythematous patches on sun-exposed skin
Microscopic
-
♦
A sharply defined epidermal proliferation of enlarged, pale keratinocytes with mild dysplasia
-
♦
Comment: these lesions are aneuploid and are best considered to be a variant of actinic keratosis
Squamous Cell Carcinoma In Situ (Bowen Disease )
Clinical
-
♦
Erythematous, irregular, scaly patches, and plaques that may involve any skin surface as well as the mucous membranes
-
♦
Bowen disease of the penis is often referred to as erythroplasia of Queyrat
-
♦
Sun exposure, arsenic, and other chemicals are associated with an increased risk of development of Bowen disease
-
♦
Approximately 5% of these lesions develop an invasive component
Microscopic
-
♦
Epidermal acanthosis associated with full-thickness epidermal dysplasia, which may involve the adnexa
-
♦
A dense lichenoid inflammatory infiltrate may also be present
-
♦
Intraepidermal spread (Borst–Jadassohn phenomena) may be prominent and should be differentiated from melanoma and Paget disease
Bowenoid Papulosis
Clinical
-
♦
Red-brown papules or plaques on the external genitalia and perineum of young adults
-
♦
Lesions are frequently multiple, and there is a strong association with human papillomavirus (HPV) types 16 and 18 with other types occurring less frequently
-
♦
Unlike Bowen disease, these lesions may regress and are less likely to give rise to an invasive carcinoma
Microscopic
-
♦
Fairly discrete areas of epidermal acanthosis associated with varying degrees of epidermal dysplasia, koilocytosis, hypergranulosis, and parakeratosis
-
♦
In situ carcinoma may be present
Squamous Cell Carcinoma (Fig. 18.8)

S quamous cell carcinoma.
Clinical
-
♦
Indurated, hyperkeratotic nodules which may show ulceration or verruciform changes
-
♦
Currently, squamous cell carcinoma is the second most common cutaneous malignancy
-
♦
The incidence is increasing
-
♦
While most are related to sun exposure, other risk factors include fair complexion, chronic inflammation, immunosuppression, burns, HPV infection, and chemical exposure (e.g., arsenic)
-
♦
The overall rate of metastases is approximately 5% but is >10% at mucosal sites and the ear
Microscopic
-
♦
Atypical nests of epidermoid cells invasive into the dermis and, usually, with overlying epidermal dysplasia
-
♦
Differentiation varies from poorly differentiated (minimal keratin production, marked nuclear pleomorphism, high mitotic rate) to well differentiated (abundant keratin pearl formation, minimal cytologic atypia, and few mitoses)
-
♦
The presence of keratin production, intercellular desmosomes (“spines”), and overlying epidermal dysplasia are useful features in separating this tumor from other entities
-
♦
Variants include clear cell, spindle cell, acantholytic, and verrucous tumors
Verrucous Carcinoma
Clinical
-
♦
A variant of squamous cell carcinoma that typically appears as a large hyperkeratotic nodule
-
♦
All cutaneous surfaces may be involved but plantar, oral (oral florid papillomatosis), and anogenital lesions are particularly common
-
♦
These tumors frequently recur but have little metastatic potential
Microscopic
-
♦
An endophytic and exophytic growth of well-differentiated squamous epithelium with extensive keratinization
-
♦
The deep component shows a broad, pushing front at its advancing edge
-
♦
If any significant nuclear dysplasia is present, a diagnosis of squamous cell carcinoma should be made
Keratoacanthoma
Clinical
-
♦
A rapidly growing, umbilicated nodule with a central keratin plug
-
♦
Multiple lesions may be present
-
♦
Typically, these tumors regress over the course of a few months, but they may recur
-
♦
These tumors are considered to be a variant of squamous cell carcinoma by some experts
Microscopic
-
♦
A well-defined, sharply demarcated, crateriform squamous proliferation with a central keratin plug
-
♦
The squamous epithelium frequently has a glassy appearance and lacks significant cytologic atypia
-
♦
A lichenoid inflammatory infiltrate may be present
-
♦
The presence of cytologic atypia, infiltrative borders, or atypical mitoses warrants a diagnosis of a squamous cell carcinoma
Pilar and Pilosebaceous-Derived Tumors
Dilated Pore of Winer
Clinical
-
♦
Flesh-colored papule or cyst with a central keratotic plug found chiefly on the head and neck
Microscopic
-
♦
A cone-shaped dilatation of the follicular infundibulum with a central keratin plug
-
♦
The wall of the pore is proliferative with fingerlike projections extending into the adjacent dermis
-
♦
No secondary hair follicles are evident within the cyst wall
Pilar Sheath Acanthoma
Clinical
-
♦
Small nodule with a central keratin-filled pore on the upper lip
Microscopic
-
♦
Similar in architecture to the dilated pore but with a more proliferative wall
-
♦
The epithelium of the wall is paler than that of the dilated pore and may have some degree of peripheral palisading, suggesting abortive hair follicle development
-
♦
No well-developed secondary hair follicles with hair formation are evident
Trichofolliculoma (Fig. 18.9)

Trichofolliculoma.
Clinical
-
♦
Solitary, flesh-colored nodules with a central pore from which numerous white hairs emerge
Microscopic
-
♦
Similar to the dilated pore, a central, elongated, and dilated infundibulum is present
-
♦
Numerous secondary hair follicles radiate peripherally from the central cavity that is filled with laminated keratin and numerous hairs
-
♦
If sebaceous glands are evident within the secondary follicles, then a diagnosis of a sebaceous trichofolliculoma is appropriate
Tumor of the Follicular Infundibulum (Fig. 18.10)

Tumor of the follicular infundibulum.
Clinical
-
♦
Small, hyperkeratotic papules or plaques on the head and neck
Microscopic
-
♦
A platelike expansion of the epidermis by interanastomosing and interweaving trabeculae of glycogenated squamous epithelium within the superficial dermis
-
♦
The trabeculae show multiple attachments to the epidermis and to the hair follicles
-
♦
The trabeculae may show some peripheral palisading but lack mucin deposition or stromal retraction
-
♦
Elastic fibers are often condensed at the base of the lesion
Differential Diagnosis
-
♦
Fibroepithelioma of Pinkus and eccrine syringofibroadenoma
-
♦
Fibroepithelioma of Pinkus has narrow trabeculae with more pronounced basaloid differentiation, while eccrine syringofibroadenoma shows scattered eccrine ducts within its trabeculae
Basaloid Follicular Hamartoma
Clinical
-
♦
Small, flesh-colored papules or plaques on the head and neck
-
♦
Solitary, multifocal, and inherited variants have been described
Microscopic
-
♦
Small, starfish- or octopus-like proliferations of basaloid cells within the dermis arranged as anastamosing trabeculae with peripheral palisading and surrounding fibrosis
Trichilemmoma (Fig. 18.11)

T richilemmoma.
Clinical
-
♦
Verrucous, hyperkeratotic papules usually found on the face
-
♦
Multiple trichilemmomas occur in the autosomal dominant disorder, Cowden disease
Microscopic
-
♦
A single lobule or, occasionally, a multilobular proliferation of round, clear (glycogen-rich) squamous cells giving a platelike thickening to the epidermis
-
♦
There is usually a follicular accentuation to the proliferation with the pale cells growing down preexisting follicular structures
-
♦
The lobules are surrounded by a PASD-positive basement membrane
-
♦
A desmoplastic variant exists which, in addition to typical trichilemmoma areas, has central trabeculae surrounded by a dense, hypocellular stroma
Trichoadenoma (Fig. 18.12)

Trichoadenoma.
Clinical
-
♦
Yellow to flesh-colored papule on the face
Microscopic
-
♦
Numerous keratin-filled cysts lined by a stratified squamous epithelium are evident within the dermis
-
♦
A granular layer is present (epidermoid keratinization), and the cysts have a surrounding fibrous stroma
-
♦
Solid trabeculae are rare
Trichoepithelioma
Clinical
-
♦
Small flesh-colored papules on the face of young- to middle-aged adults
-
♦
Solitary, desmoplastic, and multiple (autosomal dominant inheritance) variants exist
Microscopic
-
♦
An admixture of keratin-filled cysts and trabeculae of basaloid cells with peripheral palisading and a surrounding fibrous stroma
-
♦
Stromal retraction is not evident, and true hair bulb formation is rarely seen
Differential Diagnosis
-
♦
Keratotic basal cell carcinoma is different from trichoepithelioma by having stromal retraction, mucin deposition, individual cell necrosis, and numerous mitoses
-
♦
Microcystic adnexal carcinoma differs from desmoplastic trichoepithelioma by the presence of deeper infiltration with eccrine ducts lined by an eosinophilic cuticle. A layered appearance with cysts predominating superficially and trabeculae predominating at the deep aspect of the tumor are characteristic
Trichoblastoma
Clinical
-
♦
A controversial entity having histologic and clinical overlap with trichoepithelioma and basal cell carcinoma
Microscopic
-
♦
A proliferation of germinative basaloid cells arranged in nests, sheets, or trabeculae
-
♦
Conspicuous hair bulb differentiation is seen at the edge of the nests or sheets but also as single, primitive hair follicle-like structures surrounded by a dense fibrous sheath
-
♦
Stromal clefting and extensive mucin deposition are typically absent
Differential Diagnosis
-
♦
Basal cell carcinoma shows stromal clefting, mucin deposition, and single cell necrosis and lacks primitive hair bulb structures
-
♦
Trichoepithelioma has admixed keratin-filled cysts and has few to no primitive hair bulbs
Trichodiscoma
Clinical
-
♦
A hamartomatous proliferation of the hair disk which presents as multiple flesh-colored papules on the face and also elsewhere on the body
Microscopic
-
♦
A nodular mesenchymal proliferation surrounded by an epidermal collarette
-
♦
Centrally there are stellate fibroblasts embedded in collagen, reticulin, and elastic fibers with abundant mucin deposition
-
♦
Thin-walled vessels with prominent basement membranes are seen within the proliferation
Perifollicular Fibroma and Fibrofolliculoma
Clinical
-
♦
Both occur as solitary and, more often, multiple flesh-colored papules on the face or neck
Microscopic
-
♦
Perifollicular fibromas show a loose, concentric proliferation of fibrous tissue around normal hair follicles, while fibrofolliculomas show both a fibrous and a follicular proliferation centered on a dilated follicle
-
♦
The epithelial component of the latter consists of epithelial trabeculae that arise from the infundibulum and are surrounded by fibrous tissue
Pilomatricoma (Fig. 18.13) (Calcifying Epithelioma of Malherbe)

Pilomatricoma.
Clinical
-
♦
Deep-seated, frequently calcified nodules on the head, neck, and upper extremities of children and young adults
-
♦
These lesions may be solitary or multiple (autosomal dominant inheritance) or may be a marker of a systemic disease (Gardner syndrome)
Microscopic
-
♦
A cystic or multinodular tumor with a biphasic epithelial growth pattern consisting of eosinophilic, ghosts, or shadow cells centrally and basophilic, basaloid cells peripherally
-
♦
Granulomatous inflammation and calcification are frequent and may obscure the characteristic growth pattern
Basal Cell Carcinoma (Fig. 18.14)

Ba sal cell carcinoma.
Clinical
-
♦
Well-delineated, pearly, translucent, pink-tan papules or nodules with telangiectasia
-
♦
Superficial, nodular/ulcerative, pigmented, diffuse, morpheaform, and fibroepitheliomatous variants exist
-
♦
Most are found on sun-exposed skin of the elderly, but occasional cases are evident on non-sun-exposed skin
-
♦
Basal cell carcinoma is currently the most common cutaneous malignancy, and the incidence is increasing
-
♦
Risk of developing basal cell carcinomas is related to sun exposure and skin type
-
♦
Multiple tumors are seen in Bazex syndrome and basal cell carcinoma nevus syndrome (Gorlin syndrome), an autosomal dominant inherited disease also having odontogenic keratocysts, palmar-plantar pits, ectopic calcification, and skeletal abnormalities
-
♦
Basal cell carcinoma has little tendency to metastasize
Microscopic
-
♦
A proliferation of atypical basaloid cells in nests, trabeculae, and/or cysts within the dermis but often demonstrating multifocal epidermal attachment
-
♦
Peripheral palisading, stromal retraction, mucin deposition, single cell necrosis, and mitoses are characteristic and are useful in separating this tumor from other entities
-
♦
Nodulocystic, metatypical (keratotic), pigmented, adenoidal, infiltrating, superficial, and morpheaform histologic variants exist, with the latter two having an increased risk of recurrence
Fibroepithelioma of Pinkus (Fig. 18.15)

Fibroepithelioma of Pinkus.
Clinical
-
♦
Polypoid or plaque-like lesions on the thigh or trunk
-
♦
Considered as a premalignant lesion by many experts
Microscopic
-
♦
Interanastomosing epithelial strands with multiple points of attachment to the epidermis and surrounded by a fibrous stroma
-
♦
The trabeculae are thinner than the tumor of the follicular infundibulum, being two to three epithelial cells in thickness
Malignant Pilomatricoma
Clinical
-
♦
A rare tumor occurring as tumors or nodules on the face
Microscopic
-
♦
Similar to a benign pilomatricoma but showing areas with infiltration, mitoses, and nuclear pleomorphism
Nevus Sebaceous (Fig. 18.16)

Nevus sebaceous.
Clinical
-
♦
Single or multiple, yellow papules to plaques with or without verruciform features on the head and neck of infants, adolescents, and young adults
-
♦
A linear form exists
-
♦
Nevus sebaceous with cerebral abnormalities is referred to as the nevus sebaceous syndrome
-
♦
Basal cell carcinoma is the most common malignancy associated with nevus sebaceous, while syringocystadenoma papilliferum is the most common benign proliferation associated with this condition
Microscopic
-
♦
The epidermis frequently demonstrates papillomatosis or verruciform change
-
♦
Numerous immature or abortive hair follicles are situated within the superficial dermis with a reduction in the number of mature terminal hairs
-
♦
The sebaceous glands appear haphazardly distributed within the dermis and may appear atrophic, hyperplastic, or relatively normal in size
-
♦
Apocrine glands are a frequent finding in the deep dermis
Sebaceous Hyperplasia
Clinical
-
♦
Small yellow papules on the face and forehead of older adults
Microscopic
-
♦
Enlarged, hyperplastic sebaceous glands emptying into a central hair follicle often situated in the superficial dermis
Sebaceous Adenoma
Clinical
-
♦
Pink to yellow papules on the face and neck of older adults
-
♦
Multiple lesions are often associated with visceral malignancy (Muir–Torre syndrome)
Microscopic
-
♦
A multilobulated tumor often showing attachment to or emptying through the overlying epidermis
-
♦
The lobules are composed of basaloid cells peripherally and multivacuolated cells centrally
-
♦
By definition, the basaloid cells comprise less than 50% of cells of the individual lobules
-
♦
Infiltration, necrosis, and frequent mitoses are absent
Sebaceous Epithelioma
Clinical
-
♦
Similar to sebaceous adenoma
Microscopic
-
♦
A faintly lobular tumor similar to the sebaceous adenoma
-
♦
Basaloid cells comprise more than 50% of the cells in the individual lobules
-
♦
While occasional mitotic figures may be seen, abundant mitotic activity, infiltration, nuclear pleomorphism, or necrosis should lead to a consideration of sebaceous carcinoma or basal cell carcinoma with sebaceous differentiation
Sebaceous Carcinoma (Fig. 18.17)

Sebaceous carcinoma.
Clinical
-
♦
Ulcerated or nonulcerated nodules on the head and neck region of older adults
-
♦
The periocular region is a particularly common site where derivation from the meibomian gland occurs
-
♦
These tumors are associated with a high metastatic potential and increased mortality (~25%)
Microscopic
-
♦
These tumors may show irregular lobules or a diffuse infiltrating pattern
-
♦
Attachment to the overlying epidermis may be present, and pagetoid spread is common in the periocular variants
-
♦
These tumors show a spectrum of sebaceous differentiation varying from tumors composed predominantly of basaloid cells to tumors with numerous multivacuolated sebaceous cells
-
♦
Infiltration, necrosis, nuclear pleomorphism, nucleoli, and mitoses are usually readily evident
-
♦
Perineural and capillary–lymphatic space invasion may be seen
Immunophenotype
-
♦
Cytokeratin and EMA+; S-100 protein and CEA–
Eccrine-Derived Tumors and Proliferations
Syringoma-Like Proliferations Associated with Alopecia
Clinical
-
♦
No specific clinical findings are associated with this lesion which presents simply as alopecia of any etiology
Microscopic
-
♦
This is a relatively rare, apparently nonneoplastic proliferation of the eccrine ducts in response to alopecia
-
♦
The microscopic characteristic is that of the particular form of alopecia affecting the patient with the addition of a diffuse, haphazard proliferation of the eccrine ducts limited to the mid and upper dermis
-
♦
Ducts, trabeculae, comma, and tadpole-shaped forms may all be seen
-
♦
No nuclear pleomorphism or perineural invasion is evident, but mitotic figures may be seen
-
♦
This proliferation may be seen throughout the scalp in cases of severe alopecia
Differential Diagnosis
-
♦
Syringoma is usually a more localized and circumscribed eccrine proliferation and lacks the haphazard appearance of the above
-
♦
Microcystic adnexal carcinoma and eccrine syringoid carcinoma are more infiltrative lesions that typically involve the lower dermis and the subcutis and show frequent perineural invasion
Eccrine Syringofibroadenoma (Fig. 18.18)

Eccrine syringofibroadenoma.
Clinical
-
♦
Single or multiple papules or nodules with a wide age range and distribution
-
♦
The extremities are most commonly involved
Microscopic
-
♦
Interanastomosing cords and trabeculae of epithelial cells extending into the dermis with multiple points of attachment to the epidermis
-
♦
The cords are thin and surrounded by a fibrous stroma
-
♦
Scattered throughout the epithelial cords are areas of eccrine duct differentiation with prominent eosinophilic cuticles
Differential Diagnosis
-
♦
Tumor of the follicular infundibulum and fibroepithelioma of Pinkus lack eccrine differentiation
Syringoma (Fig. 18.19)

Syringoma.
Clinical
-
♦
Multiple flesh-colored or faintly yellow papules on the eyelids or upper face
-
♦
Other sites may also be involved, and linear and eruptive variants occur
-
♦
Clear cell variants may be associated with diabetes
Microscopic
-
♦
A fairly well-circumscribed but unencapsulated neoplasm involving the mid to upper dermis composed of eccrine-derived cords and ducts
-
♦
The cords may show characteristic tadpole-shaped forms
-
♦
Two or more cell layers with an internal eosinophilic cuticle and varying degrees of clear cell change line the ducts
-
♦
In general, the tumor does not infiltrate the deep dermis or subcutaneous fat, lacks mitotic activity and necrosis, and has no significant pleomorphism
Immunophenotype
-
♦
Eccrine-derived tumors typically stain positively for the cytokeratins, EMA, and CEA, which highlights the luminal aspect of the eccrine ducts
Differential Diagnosis
-
♦
Desmoplastic trichoepithelioma has numerous keratotic cysts and frequent calcification and lacks eccrine duct formation
-
♦
Microcystic adnexal carcinoma is much more infiltrative and typically involves the deep dermis and subcutaneous fat
Chondroid Syringoma (Benign Mixed Tumor, Fig. 18.20)

Chondroid syringoma.
Clinical
-
♦
A benign, slowly growing, typically solitary tumor nodule on the head and neck; other sites may be involved
Microscopic
-
♦
A well-circumscribed, biphasic tumor nodule located within the dermis and/or the subcutaneous fat
-
♦
Epithelial cords, trabeculae, and ducts are embedded in an abundant myxoid, fibromyxoid, or cartilaginous matrix
-
♦
The epithelial component lacks nuclear pleomorphism, infiltration, necrosis, and mitotic activity
-
♦
The ducts may show eccrine and/or apocrine differentiation
Differential Diagnosis
-
♦
Pleomorphic adenoma (benign mixed tumor of the salivary glands) should be differentiated from chondroid syringoma because of its tendency to recur and, possibly, malignant transformation
-
♦
As these tumors are similar histologically, location and the presence of adjacent normal salivary glands are the most reliable features used to separate these entities
Malignant Chondroid Syringoma
Clinical
-
♦
A rare, highly malignant tumor with a predilection for the distal extremities
-
♦
These tumors frequently recur and metastasize and are associated with increased mortality
Microscopic
-
♦
Malignant appearing, infiltrating epithelial cords, ducts, and sheets that overgrow the benign mesenchymal matrix
-
♦
Necrosis, mitoses, and nuclear pleomorphism are present
-
♦
An adjacent benign mixed tumor is not typically seen
Differential Diagnosis
-
♦
Carcinosarcoma shows a malignant mesenchymal component in addition to an epithelial malignancy
Papillary Eccrine Adenoma
Clinical
-
♦
A firm, pink to tan nodule on the distal extremities of adolescents and young adults with a female predominance
-
♦
Blacks are more commonly affected than Whites
Microscopic
-
♦
A fairly well-circumscribed but unencapsulated proliferation of eccrine ducts and duct-like structures within the dermis
-
♦
The ducts are lined by a multilayered cuboidal epithelium without apical snouts
-
♦
Micropapillary projections and transluminal bridging may be seen
-
♦
The tumor stroma is fibrotic and frequently hyalinized. Cribriform structures, necrosis, mitotic activity, and nuclear pleomorphism are absent
Differential Diagnosis
-
♦
Aggressive digital papillary adenoma/adenocarcinoma (see below)
Aggressive Digital Papillary Adenoma/Adenocarcinoma
Clinical
-
♦
Asymptomatic flesh-colored nodule on the digits of middle-aged adults
-
♦
The recurrence rate is approximately 50% for these tumors, and the overtly malignant lesions have a metastatic rate of approximately 25–40%
Microscopic
-
♦
Generally, an unencapsulated and poorly circumscribed proliferation of eccrine ducts, tubules, cysts, and nests within the dermis and/or subcutaneous fat
-
♦
The ducts and cystic structures are lined by a multilayered epithelium with abundant micro- and macropapillae
-
♦
Cribriform structures are frequently identified
-
♦
Varying degrees of nuclear pleomorphism, mitotic activity, and necrosis may be seen
-
♦
Tumor grade correlates with metastatic potential, but all forms may metastasize
-
♦
Note: all of these lesions are best classified as adenocarcinomas due to their propensity for recurrence
-
♦
A histologic grade should be given as a prognostic indicator for the risk of metastases
Differential Diagnosis
-
♦
Papillary eccrine adenoma does not show the infiltration, nuclear atypia, mitotic activity, or the cribriforming of the aggressive digital papillary adenocarcinoma
-
♦
Nodular hidradenoma (clear cell )
Hidradenoma, Solid-Cystic Hidradenoma, and Eccrine Acrospiroma (Fig. 18.21)

N odular hidradenoma (A, B).
Clinical
-
♦
Solid or cystic, intradermal nodule 05–2.0 cm in diameter
-
♦
These tumors are usually solitary but may be multiple
-
♦
The head, neck, and extremities are most commonly involved
-
♦
Predominates in young adults with a slight female predominance
Microscopic
-
♦
A well-circumscribed and often pseudoencapsulated tumor composed of a single lobule or, more often, multiple lobules of eosinophilic to clear cells in the dermis
-
♦
Cystic change may be prominent
-
♦
Tubular structures lined by cuboidal to columnar cells with an eosinophilic cuticle are evident in most tumors and are important in proper classification
-
♦
Foci of squamous and/or mucinous differentiation may be seen
-
♦
While this tumor is predominantly intradermal, occasional attachments may be seen to the overlying epidermis
-
♦
Necrosis, mitotic activity, and nuclear pleomorphism are absent or minimal in extent
Hidradenocarcinoma (Malignant Nodular Hidradenoma )
Clinical
-
♦
Similar distribution to their benign counterparts but occurs in older individuals (>50 years of age)
-
♦
Recurrence and metastatic rate is approximately 50%
Microscopic
-
♦
Like the hidradenoma, this tumor is composed of eosinophilic and/or clear cells forming lobules within the dermis
-
♦
The malignant variants, however, are asymmetrical, infiltrating, and mitotically active and demonstrate nuclear pleomorphism and/or necrosis
Differential Diagnosis
-
♦
Clear cell squamous cell carcinoma, clear cell renal cell carcinoma, clear cell melanoma, and trichilemmal carcinoma
-
♦
Look for tubular structures with an eosinophilic cuticle to confirm eccrine differentiation; CEA may be useful in that it highlights the luminal border of eccrine-derived structures
Hidroacanthoma Simplex (Intraepidermal Poroma )
Clinical
-
♦
A rare, benign variant of poroma typically involving the extremities of older individuals
Microscopic
-
♦
An intraepidermal proliferation (Borst–Jadassohn phenomenon) of round to faintly spindled cells with eosinophilic to faintly clear cytoplasm
-
♦
Intracytoplasmic glycogen is evident on PAS staining
-
♦
Rare eccrine ducts/tubules may be seen
-
♦
The individual cells are remarkably uniform and lack nuclear atypia
-
♦
The tumor cells are sharply demarcated from the squamous cells of the adjacent epidermis
Eccrine Poroma (Fig. 18.22)

Eccrine poroma.
Clinical
-
♦
A red to flesh-colored tumor found most frequently on the sole of the foot or hand, but other sites may be involved
-
♦
These tumors may reach many centimeters in diameter and may be pedunculated
-
♦
While the majority of these tumors are solitary, multiple lesions may be seen (eccrine poromatosis)
Microscopic
-
♦
This tumor is composed of numerous cords or trabeculae of small rounded tumor cells which rain down from the epidermis into the dermis in a fairly circumscribed manner
-
♦
The epidermal component is similar to hidroacanthoma simplex, while the dermal component often shows numerous well-formed lobules with frequently conspicuous duct formation
-
♦
Cystic change is typically less than that seen in hidradenoma, while the degree of epidermal involvement is significantly greater
-
♦
The tumor cells show intercellular bridges and should not be confused with squamous cells that are larger and more polygonal
-
♦
Poromatous lesions that are entirely limited to the dermis are often called dermal duct tumors
Porocarcinoma (Malignant Eccrine Poroma )
Clinical
-
♦
The malignant counterpart to the eccrine poroma affects similar sites but tends to occur in older individuals with a long history of progressive tumor growth
-
♦
The recurrence and metastatic rate approaches 25%
-
♦
Multiple cutaneous metastases are not uncommon
Microscopic
-
♦
Like their benign counterparts, epidermal, dermal, and mixed epidermal–dermal variants are seen
-
♦
The epidermal variants and the cutaneous metastases typically show frank pagetoidosis with scattered foci of ductal differentiation
-
♦
The mixed variants are by far the most common and have a similar architecture to their benign counterpart; however, these tumors are infiltrative and mitotically active and demonstrate nuclear pleomorphism and occasionally perineural and capillary–lymphatic invasion
Cylindroma and Malignant Cylindroma (Fig. 18.23)

Cylindroma.
Clinical
-
♦
Solitary or multiple, red to purple nodules on the head, neck, or scalp
-
♦
Multiple tumors (turban tumors) are inherited in an autosomal dominant fashion and may be associated with multiple trichoepitheliomas
Microscopic
-
♦
Multiple, dermal-based lobules are found in the dermis and have an interlocking or “jigsaw puzzle” appearance
-
♦
The individual lobules are surrounded by an eosinophilic basement membrane
-
♦
Two cell types are evident within the lobules: a lymphocyte-like population of cells with hyperchromatic nuclei which predominate at the periphery of the lobules and a population of larger cells with oval, vesicular nuclei which predominate centrally
-
♦
Hylanizing basement membrane-like material is also frequently evident within the lobules
-
♦
Malignant variants demonstrate nuclear pleomorphism, mitotic activity, loss of the surrounding basement membrane, and infiltration of adjacent tissue
-
♦
Malignant variants are rare and may arise in the background of multiple benign cylindromas
Eccrine Spiradenoma and Malignant Eccrine Spiradenoma (Fig. 18.24)

Eccrine spiradenoma (A, B).
Clinical
-
♦
Usually solitary, blue- to flesh-colored intradermal nodules on the ventral aspect of the body
-
♦
These tumors are frequently painful Rarely, multiple tumors may be seen in a linear or zosteriform distribution
Microscopic
-
♦
One or more basophilic tumor lobules are evident in the dermis and are usually encapsulated
-
♦
The lobules are composed of two cell types similar to the cylindroma: a small, lymphocyte-like population and a larger cell type with oval, vesicular nuclei
-
♦
Ductal differentiation may be conspicuous within the lobules, and pseudovascular spaces may give a hemangiomatous quality to the lesion
-
♦
The intervening stroma often demonstrates lymphangiectasia
-
♦
The rare malignant variants require an adjacent benign focus of typical microscopy for confident diagnosis
-
♦
The malignant variants are characterized by infiltration, mitoses, nuclear pleomorphism, necrosis, and lymphatic invasion
Eccrine Duct Carcinoma
Clinical
-
♦
A nodular and often ulcerated lesion of long-standing duration found most commonly on the head, neck, and extremities of older adults
-
♦
Approximately 50% metastasize to lymph nodes or visceral sites
Microscopic
-
♦
An infiltrating dermal tumor composed of strands, trabeculae, and tubules with varying degrees of lumen formation
-
♦
The histologic pattern is very similar to ductal carcinoma of the breast, which should always be excluded clinically
-
♦
There is at least some degree of nuclear pleomorphism, and nucleoli are frequently prominent
-
♦
Mitotic figures and necrosis may also be identified
Syringoid Eccrine Carcinoma (Eccrine Epithelioma )
Clinical
-
♦
Typically, a plaque or an ulcerated tumor of the scalp of middle-aged adults
-
♦
This tumor is locally aggressive with frequent recurrences, but metastases are rare
Microscopic
-
♦
A dermal-centered tumor showing extensive infiltration with the involvement of the subcutaneous fat
-
♦
This tumor is composed of infiltrating cords and trabeculae with faint lumen formation and a dense, hyalinizing stroma
-
♦
Unlike microcystic adnexal carcinoma, keratocysts are rarely present
-
♦
The individual cells often have basaloid features but lack peripheral retraction
-
♦
Nuclear pleomorphism is mild, and mitotic figures are scarce
-
♦
Perineural invasion is frequent
Microcystic Adnexal Carcinoma (Fig. 18.25)

Microcystic adnexal carcinoma (A, B).
Clinical
-
♦
A flesh-colored to yellow, slowly growing firm plaque or nodule involving the head, neck, or face of older adults
-
♦
Like syringoid eccrine carcinoma, this is a locally aggressive tumor with frequent recurrences but with no tendency to metastasize
Microscopic
-
♦
A dermal-centered tumor showing extensive infiltration of the deep dermis and subcutaneous tissues
-
♦
Keratocysts, trabeculae, and ductules are evident throughout the lesion, but keratocysts tend to predominate superficially while trabeculae predominate at the deeper aspect of the tumor
-
♦
The middle of the tumor shows an admixture of all forms, giving this tumor a triphasic or trilayered look from superficial to deep
-
♦
The individual epithelial units are frequently invested by a dense fibrous stroma, giving this tumor a sclerotic appearance
-
♦
Perineural invasion is common, while nuclear pleomorphism and mitotic activity are rare
Mucinous Eccrine Carcinoma
Clinical
-
♦
A flesh-colored to blue nodule on the head and neck region (particularly the eyelid) of older adults with a male predominance
Microscopic
-
♦
A dermal-based tumor showing islands of relatively bland epithelial cells floating in pools of mucin similar to colloid carcinoma of the breast
Adenoid Cystic Carcinoma
General
-
♦
A rare, primary cutaneous neoplasm showing a similar microscopic characteristic to its counterparts elsewhere but having a less aggressive course
Mucoepidermoid Carcinoma
General
-
♦
A rare primary tumor of the skin showing similar histologic features to its salivary gland counterpart
Apocrine-Derived Tumors and Proliferations
Apocrine Nevus
Clinical
-
♦
A rare lesion typically presenting as a papule in the axilla or on the scalp
Microscopic
-
♦
An increase in the number or size of mature-appearing apocrine glands
Syringocystadenoma Papilliferum (Fig. 18.26)

S yringocystadenoma papilliferum.
Clinical
-
♦
Typically a solitary, verrucous to papillary lesion on the scalp, face, or neck, but other sites may be involved
-
♦
In children, this tumor frequently arises within a nevus sebaceous
Microscopic
-
♦
A partially cystic, dermal-centered tumor showing overlying epidermal invagination
-
♦
The cystic space contains abundant papillary structures lined by a bilayered epithelium with apical snouts, consistent with apocrine differentiation
-
♦
The fibrovascular cores contain abundant plasma cells
Hidradenoma Papilliferum
Clinical
-
♦
Typically a solitary, asymptomatic nodule present in the genital region of females
-
♦
Similar lesions have been described within the ear, nipple, and eyelid
Microscopic
-
♦
A well-demarcated, dermal-based neoplasm showing no involvement of the overlying epidermis
-
♦
This tumor is also frequently cystic in areas and is characterized by numerous trabeculae, epithelial fronds, and papillary structures lined by a bilayered epithelium showing apocrine differentiation (apical snouts)
-
♦
The stroma is fibrovascular and lacks the plasma cells of syringocystadenoma papilliferum
-
♦
Occasional cases show a more pronounced fibrous stroma with a lobular architecture akin to fibroadenoma of the breast
-
♦
Rare cases show malignant transformation with high-grade nuclear features, frequent mitoses, necrosis, and infiltration
Tubular Apocrine Adenoma (Fig. 18.27)

Tubular apocrine adenoma.
Clinical
-
♦
A well-defined nodule occurring most commonly on the scalp of adults
Microscopic
-
♦
An unencapsulated but well-demarcated proliferation of numerous ducts/glands lined by a bilayered to multilayered epithelium showing apocrine differentiation
-
♦
Small papillary structures and occasional cribriforming may be seen and resemble proliferative lesions in the breast
-
♦
These lesions may show some degree of nuclear atypia and mitotic activity but generally are not considered as carcinomas unless obvious infiltration of surrounding tissues is seen
Apocrine Carcinoma
Clinical
-
♦
A rare primary tumor of the skin that typically presents as an erythematous nodule with or without ulceration in older adults
-
♦
A variety of sites may be affected including the scalp, eye, ear, and anogenital regions among others
-
♦
Recurrences and metastases may occur
Microscopic
-
♦
A variety of histologic appearances may be present including cystic, papillary, sheetlike, and ductal variants
-
♦
Infiltration of adjacent tissues is seen, and pagetoidosis may be evident
-
♦
Nuclear pleomorphism may be mild to marked, and varying degrees of mitotic activity and necrosis may be evident
-
♦
By definition, areas of apocrine differentiation should be identified, at least focally
Differential Diagnosis
-
♦
Apocrine carcinoma of the breast has similar histologic and immunophenotypic characteristics and should be excluded clinically
Neuroendocrine-Derived Tumors
Merkel Cell Carcinoma (Fig. 18.28)

Merkel cell carcinoma (A, B).
Clinical
-
♦
An aggressive neoplasm typically presenting as a slowly growing nodule on the sun-exposed skin (head and neck region) of older adults
-
♦
The recurrence and metastatic rate is approximately 40–50%
Microscopic
-
♦
A variety of histologic forms may be seen and include sheetlike, ribboned, nested, trabecular, and organoid variants
-
♦
Pseudorosettes may be prominent
-
♦
These tumors are typically dermal based but frequently involve the subcutis and may show an intraepidermal growth pattern
-
♦
Focal areas of squamous, eccrine, or sebaceous differentiation may be seen, and these tumors may arise in conjunction with another histologically distinct neoplasm
-
♦
The cytologic and immunophenotypic appearance is characteristic and common to all variants
-
♦
Cytologically, the tumor cells have very high nuclear/cytoplasmic ratios, indistinct cell borders, and hyperchromatic and finely granular nuclei with inconspicuous nucleoli and thin nuclear membranes
-
♦
Nuclear molding and mitoses are abundant
-
♦
Immunophenotypically, the tumor cells express low molecular weight cytokeratin (CAM 5.2) in a perinuclear dot-like pattern which may also be seen with neurofilament staining
-
♦
Cytokeratin 20 staining is generally positive, and these tumors express a variety of neuroendocrine markers including neuron-specific enolase, chromogranin, synaptophysin, and neurofilament but are generally negative for S-100 protein and vimentin
Differential Diagnosis
-
♦
Merkel cell carcinomas must be differentiated from a variety of other neuroendocrine tumors of either metastatic or primary origin
-
♦
Small cell neuroendocrine carcinomas from visceral sites metastatic to skin have an essentially identical histologic appearance but have recently been reported to be cytokeratin 20 negative
-
♦
Cutaneous neuroblastoma generally shows a filamentous background and/or focal ganglion cell differentiation and is typically cytokeratin negative (except for the olfactory variant)
-
♦
Primitive neuroectodermal tumors/extraosseous Ewing sarcomas are usually cytokeratin negative and typically express MIC- 2
Soft Tissue Neoplasms and Developmental Anomalies
Adipocyte-Derived Tumors and Proliferations
Lipoma
Clinical
-
♦
A sporadic or multifocal tumor of the middle aged to elderly typically involving the trunk and/or extremities
Microscopic
-
♦
A thin encapsulated proliferation of mature adipose tissue
-
♦
The adipose tissue may be accompanied by a wide variety of other types of mesenchymal-derived tissue: fibrous (fibrolipoma), bone (osteolipoma), cartilage (chondroid lipoma), bone marrow (myelolipoma), mucoid substances (myxoid lipoma), smooth muscle (myolipoma), and smooth muscle and vessels (angiomyolipoma)
Angiolipoma
Clinical
-
♦
A painful, subcutaneous nodule(s) involving the upper extremities of young adults
Microscopic
-
♦
Thin encapsulated proliferations of mature adipocytes and variably sized, thin-walled vessels
-
♦
Microthrombi are readily identified within the vessel lumina
-
♦
A cellular variant showing numerous small vessels with few adipocytes exists and must be differentiated from other vascular tumors that lack the proliferation of mature adipocytes
Spindle Cell Lipoma
Clinical
-
♦
A solitary, painless, subcutaneous nodule with a predilection for the base of the neck of middle-aged to older adults
Microscopic
-
♦
An encapsulated proliferation of mature adipocytes and bland, bipolar spindle cells embedded in a myxoid matrix with collagen fibers
-
♦
The spindle cells may predominate and typically show bland, uniform features
-
♦
Lipoblasts and the plexiform capillary network of myxoid liposarcoma are absent
-
♦
Occasional cases show bizarre, multinucleated cells and merge with pleomorphic lipoma
Pleomorphic Lipoma
Clinical
-
♦
Similar to spindle cell lipoma
Microscopic
-
♦
Similar to spindle cell lipoma with the addition of numerous, multinucleated (floret cells) cells with hyperchromatic, peripherally situated nuclei
Lipoblastoma and Lipoblastomatosi s
Clinical
-
♦
These are tumors of infants and young children and typically present as painless masses on the extremities in a localized (lipoblastoma) or diffuse (lipoblastomatosis) fashion
-
♦
The latter may recur with incomplete excision
Microscopic
-
♦
Multilobular proliferations of immature and mature adipocytes embedded in a myxoid matrix and separated by thin fibrous septae
-
♦
The adipocytes may show a wide spectrum of differentiation from spindle cells to multivacuolated lipoblasts to mature, univacuolated adipocytes
-
♦
These lesions tend to mature histologically with time
Lipofibromatous Hamartoma of Nerve
Clinical
-
♦
A tumorlike condition that presents as a mass of the wrist and/or forearm
-
♦
Typically, these patients are young children, but adult presentations also occur
-
♦
Sensory defects, paresthesias, pain, and macrodactyly may be prominent
-
♦
Due to the intimate association of this proliferation with nerves, surgical excision is contraindicated and may lead to permanent sensorimotor impairment
Microscopic
-
♦
A proliferation of benign fibroadipose tissue is evident in and around nerve fibers which show secondary degeneration, atrophy, and fibrosis
Lipomatosis
Clinical
-
♦
Multiple clinical forms exist including a diffuse variant typically involving the extremities or trunk of young children, a symmetrical variant (Madelung disease) involving the neck region of middle-aged adult males as well as visceral and pelvic variants
Microscopic
-
♦
All are unencapsulated proliferations of mature adipose tissue involving the subcutis, skeletal muscle, and, occasionally, other structures
Nevus Lipomatosus Superficialis
Clinical
-
♦
A hamartomatous proliferation typically presenting as multiple, polypoid papules or plaques on the buttocks, posterior trunk, or thigh of children to young adults
Microscopic
-
♦
Small lobules of mature adipocytes are evident in the superficial and mid dermis and may be associated with keratin plugs and loss of adnexal structures
Hibernoma
Clinical
-
♦
A slow-growing, asymptomatic mass of the chest or upper back of young to middle-aged adults
-
♦
Other sites may also be affected
Microscopic
-
♦
An encapsulated, multilobular tumor composed of an admixture of multivacuolated and univacuolated adipocytes and large cells with eosinophilic cytoplasm and distinct cell membranes
Liposarcoma
Clinical
-
♦
These are rare tumors of the skin that generally present as slowly growing subcutaneous masses in older adults
Microscopic
-
♦
The myriad of histologic types of liposarcoma are addressed in detail elsewhere
-
♦
Generally, the liposarcomas involving the skin are of the well-differentiated (atypical lipoma) or myxoid types
-
♦
The former have lipoma-like, sclerosing, and spindle cell variants which may recur but typically do not metastasize
Neural-Derived Tumors and Proliferations
Neurofibroma
Clinical
-
♦
Solitary and multiple forms exist
-
♦
The solitary variant is typically a soft, polypoid, flesh-colored tumor occurring in adults
-
♦
The multiple or diffuse variant has a strong association with neurofibromatosis type 1 and may show extensive, cosmetically deforming lesions with a bag-of-worms appearance and feel
-
♦
The diffuse variant is seen more frequently in childhood and adolescence
-
♦
The diffuse variant has definite malignant potential, while the sporadic variant lacks this characteristic
Microscopic
-
♦
A variety of histologic subtypes exist, but all are characterized by a proliferation of wavy, pointed spindle cells embedded in a variably collagenous to myxoid matrix
-
♦
These tumors are unencapsulated but are generally well circumscribed
-
♦
They do not infrequently incorporate dermal adnexal structures, but direct adnexal invasion is rare
-
♦
Plexiform, diffuse, myxoid, and pacinian variants exist
-
♦
The plexiform variant is thought to be diagnostic of neurofibromatosis, while the diffuse variant may also be associated with this disease at an increased rate
Special Studies
-
♦
Neurofibromas are derived from nerve and, as such, demonstrate positive staining for axonal markers such as neurofilament and silver impregnation techniques
-
♦
Similar to other neural-derived tumors, these lesions are also positive for S-100 protein, CD57, and neuron-specific enolase
Schwannoma (Neurilemmoma, Fig. 18.29)

Plexiform schwannoma.
Clinical
-
♦
A peripheral nerve sheath-derived tumor that generally presents as a solitary nodule/mass on the head, neck, or extremities of adults
-
♦
Rarely, multiple tumors may be evident (schwannomatosis), and at least some of these cases are associated with neurofibromatosis type 2
-
♦
In general, schwannomas have little, if any, malignant potential
Microscopic
-
♦
A well-circumscribed, encapsulated tumor within the subcutis or deeper tissues
-
♦
Occasionally, dermal involvement may be evident
-
♦
The tumor is composed of spindle cells with wavy, pointed nuclei embedded in a collagenous and highly vascular stroma
-
♦
Classically, cellular, Antoni A areas with palisading, Verocay bodies are admixed with paucicellular, myxoid, Antoni B areas
-
♦
Degenerative changes are frequent findings and include hyalinization, vascular thrombosis, dystrophic mineralization, and hemorrhage
-
♦
The ancient variants typically show some degree of nuclear pleomorphism and enlargement with a smudgy chromatin pattern
-
♦
Plexiform variants exist and typically present in childhood or adolescence
-
♦
These tumors are composed of multiple, cellular, Antoni A-like, encapsulated nodules that must be differentiated from plexiform neurofibroma and plexiform fibrohistiocytic tumor
-
♦
Cellular variants are moderately to markedly cellular and may have mitotic activity. Nuclear pleomorphism and necrosis, however, are absent. Melanotic variants also exist and must be differentiated from malignant melanoma
Special Studies
-
♦
Schwannomas are derived from the peripheral nerve sheath and, therefore, lack axonal differentiation; that is, they are neurofilament and silver staining negative
-
♦
Schwann cells are S-100 protein positive and are generally surrounded by type IV collagen-rich basement membrane
-
♦
Epithelial membrane antigen typically stains the capsule of schwann omas
Traumatic Neuroma
Clinical
-
♦
Reactive, nonneoplastic proliferations of nerve in response to injury
-
♦
Typically present as small, often painful, nodules at sites of previous injury
Microscopic
-
♦
A well-localized but unencapsulated, haphazard proliferation of nerve fibers associated with dermal fibrosis (scar)
Palisaded and Encapsulated Neuroma (Solitary Circumscribed Neuroma, Fig. 18.30)

Palisaded and encapsulated neuroma.
Clinical
-
♦
Solitary, flesh-colored papule on the face of middle-aged to older adults
Microscopic
-
♦
A nodular to multinodular, often dumbbell-shaped proliferation of spindle cells embedded in a collagenous matrix
-
♦
These lesions are well circumscribed but only partially encapsulated
-
♦
The superficial component generally lacks a true capsule and tends to resemble a neurofibroma, while the deep component is encapsulated and resembles a schwannoma
-
♦
The spindle cells demonstrate wavy, pointed nuclei and lack mitotic activity
-
♦
Contrary to its name, true nuclear palisading is rare in this lesion
-
♦
A nerve may be evident entering the base of the lesion
Special Studies
-
♦
Like neurofibroma, this lesion contains both axons and schwann cells and, hence, is S-100 protein and neurofilament positive
Granular Cell Tumor (Fig. 18.31)

Granular cell tumor.
Clinical
-
♦
Slowly growing, sometimes painful, flesh-colored nodules with a predilection for the tongue, trunk, and extremities of adults
-
♦
While usually solitary, multiple, and familial variants exist
Microscopic
-
♦
Irregular fascicles and/or sheets of large, round to polygonal cells with eosinophilic, granular cytoplasm
-
♦
Cell borders are indistinct giving this tumor a syncytial appearance
-
♦
Nuclei are generally round to ovoid, central, and monomorphic
-
♦
Nuclear pleomorphism, mitotic activity, necrosis, and large tumor size may be associated with the rare malignant variants
-
♦
Prominent pseudoepitheliomatous hyperplasia of the epidermis is often seen overlying this tumor and must not be mistaken for squamous cell carcinoma
Special Studies
-
♦
While the cell of origin remains to be clarified, most authorities support a schwann cell derivation for these tumors
-
♦
Accordingly, these tumors are usually, but not always, S-100 protein and neuron-specific enolase positive
Differential Diagnosis
-
♦
Secondary granular cell change is not an uncommon finding in other tumor types (dermatofibroma, neurofibroma, etc.) which should be excluded prior to making the diagnosis of granular cell tumor
-
♦
This tumor should also be differentiated from congenital epulis discussed below
Congenital Epulis
Clinical
-
♦
A polypoid gingival lesion in newborns that may spontaneously regress
Microscopic
-
♦
Similar to granular cell tumor, but these lesions are S-100 protein negative
Nerve Sheath Myxoma (NSM ) and Cellular Neurothekeoma (Fig. 18.32)

Neurothekeoma.
Clinical
-
♦
Soft, mobile, flesh-colored papules on the face or upper extremities of young adults
-
♦
These tumors may recur with incomplete excision
Microscopic
-
♦
NSM is a fascicular to lobular dermal tumor composed of spindle and stellate cells embedded in myxoid lobules which in turn are separated by fibrous septae
-
♦
Cellular neurothekeoma is composed of more uniform, epithelioid cells in nests and fascicles with minimal myxoid background material
-
♦
Mitotic activity and mild nuclear pleomorphism may be seen in both lesions
Special Studies
-
♦
NSM is typically S-100 protein+ and is likely derived from the peripheral nerve sheath
-
♦
Cellular neurothekeoma is S-100 protein− and its cell of origin is unclear
-
♦
The lack of S-100 protein positivity in the cellular variants allows these lesions to be readily distinguished from most melanocytic neoplasms
Perineurioma
Clinical
-
♦
A benign tumor of perineural origin that typically presents as a subcutaneous mass on the trunk and limbs of adults
Microscopic
-
♦
A well-circumscribed proliferation of bland spindle cells in fascicles with whorled and storiform areas
Special Studies
-
♦
Like perineural cells, this tumor is S-100 protein− and EMA+
Malignant Peripheral Nerve Sheath Tumor
General
-
♦
A rare, primary cutaneous malignancy frequently associated with neurofibromatosis type 1 when primary in the skin
-
♦
These lesions are discussed in detail in the chapter on soft tissue pathology
Cutaneous Meningothelial Heterotopias/Meningiomas (Fig. 18.33)

Meningioma.
Clinical
-
♦
Classic meningocele is typically a transilluminating mass along the lower spine and represents a congenital defect
-
♦
Rudimentary meningocele is thought to be a herniation of the meninges into the superficial tissues of the scalp with a subsequent loss of its intracranial attachment
-
♦
Cutaneous meningioma comes in three forms: type I is congenital lesion involving the head and paravertebral regions of children and is secondary to misplaced arachnoid cells during embryogenesis; type II occurs on the head and neck region of adults and is thought to be secondary to a proliferation of arachnoid cells through a cranial foramina; type III represents a metastasis or direct extension of tumor into skin from an intracranial primary lesion
Microscopic
-
♦
Meningoceles are typically cyst-like structures lined by arachnoid cells and having surrounding dense fibrous tissue with occasional collections of meningothelial cells in whorl-like structures
-
♦
Meningiomas are usually well-circumscribed deep dermal to subcutaneous proliferations composed of spindle cells arranged in fascicles and whorls with or without psammoma body formation
-
♦
Nuclear pleomorphism and mitotic activity may be seen, particularly in the type III variants
-
♦
Special studies
-
♦
Meningothelial proliferations are usually vimentin and EMA+
-
♦
Cytokeratin and S-100 protein may also be expressed by these tumors
Heterotopic Glial Tissue (Nasal Glioma)
Clinical
-
♦
Flesh-colored mass on the nasal bridge of infants to young adults. Intranasal involvement may also be present
-
♦
Radiographic studies should be performed to exclude an intracranial attachment
Microscopic
-
♦
Nodules of benign eosinophilic, fibrillar, glial tissue within the deep dermis and subcutis
-
♦
Rarely, neuronal cells may also be seen
Smooth Muscle-Derived Tumors and Proliferations
Smooth Muscle Hamartoma
Clinical
-
♦
A congenital, sometimes pigmented, indurated plaque on the trunk which typically presents in infancy
Microscopic
-
♦
A haphazard proliferation of smooth muscle fascicles in the dermis with or without basilar epidermal hyperpigmentation
Becker Nevus
Clinical
-
♦
An acquired, organoid, hyperpigmented plaque with hypertrichosis on the back of young adults and in adolescents
-
♦
This lesion may be associated with other congenital abnormalities
Microscopic
-
♦
Epidermal acanthosis and basilar hyperpigmentation occasionally associated with a mild haphazard proliferation of smooth muscle fascicles within the dermis
Piloleiomyoma (Pilar leiomyoma, Fig. 18.34)

Piloleiomyoma.
Clinical
-
♦
Multiple, somewhat painful papules or nodules on the trunk or extremities of young adults
-
♦
May be inherited in an autosomal dominant fashion
Microscopic
-
♦
A fairly well-circumscribed yet irregular proliferation of smooth muscle fascicles within the dermis
-
♦
The individual cells have elongated eosinophilic cytoplasm and cigar-shaped nuclei
-
♦
No nuclear pleomorphism, mitotic activity, or necrosis is evident
Angioleiomyoma (Fig. 18.35)

Angioleiomyoma.
Clinical
-
♦
A solitary, sometimes painful nodule on the extremities of adults
Microscopic
-
♦
A nodular, well-circumscribed proliferation of smooth muscle in fascicles admixed with numerous, variably sized vessels
-
♦
Degenerative changes are frequent
Leiomyosarcoma (Fig. 18.36)

Leiomyosar coma.
Clinical
-
♦
Two clinical variants exist: a superficial or cutaneous variant and a deep or subcutaneous variant
-
♦
The former predominates on the limbs of young adults and is likely derived from the arrector pili muscle
-
♦
This variant may locally recur but generally does not metastasize
-
♦
The subcutaneous variant predominates on the limbs of the elderly and has both local recurrence and metastatic potential
Microscopic
-
♦
The cutaneous variant demonstrates an irregular, infiltrating, and haphazard proliferation of smooth muscle bundles reminiscent of piloleiomyoma
-
♦
However, unlike piloleiomyoma, this tumor has low-grade nuclear pleomorphism, mitotic activity, and, rarely, necrosis
-
♦
The deep or subcutaneous variant is akin to leiomyosarcomas arising elsewhere and consists of a nodular, at least focally infiltrating, proliferation of smooth muscle fibers in well-formed to ill-defined bundles with varying degrees of nuclear pleomorphism, mitotic activity, and necrosis
Fibrohistiocytic, Histiocytic, and Langerhans Cell-Derived Proliferations
Fibrous Histiocytoma (Dermatofibroma, Fig. 18.37)

Dermatofibroma.
Clinical
-
♦
Usually single, occasionally multiple, slightly elevated, smooth, flesh-colored to hyperpigmented nodules on the extremities or trunk of adults
Microscopic
-
♦
Numerous subtypes have been described, but all are generally made up of a proliferation of histiocytes, fibroblasts, and collagenous tissue in varying proportions
-
♦
The prototypical lesion (dermatofibroma) consists of a fairly well-circumscribed, unencapsulated, middermal proliferation with feathery edges, an overlying Grenz zone, and epidermal hyperplasia with basilar hyperpigmentation
-
♦
The cellular component consists of spindled, fibroblast-like cells admixed with plump histiocytic cells in an irregular fashion
-
♦
Storiform areas may be evident, and there may be focal extension into the subcutis
-
♦
Chronic inflammatory cells, multinucleated giant cells, xanthomatized histiocytes, and hemosiderin-laden histiocytes are also frequently identified within these lesions
-
♦
Important variants include atypical dermatofibroma (dermatofibroma with monster cells), aneurysmal fibrous histiocytoma, and epithelioid cell histiocytoma, all of which may be mistaken for other more aggressive entities
-
♦
Atypical dermatofibroma is a lesion showing large, hyperchromatic, multinucleated giant cells in addition to typical dermatofibroma features and should be distinguished from atypical fibroxanthoma and malignant fibrous histiocytoma
-
♦
Aneurysmal fibrous histiocytoma is a fibrous histiocytoma with prominent intralesional hemorrhage and cystic, pseudovascular spaces
-
♦
This lesion should be distinguished from angiomatoid fibrous histiocytoma, a lesion of intermediate-grade malignancy occurring in the pediatric population
-
♦
Epithelioid cell histiocytoma is composed of a polypoid well-circumscribed proliferation of angulated, epithelioid, histiocytic-appearing cells surrounded by an epidermal collarette
-
♦
This lesion should be distinguished from melanocytic tumors, both Spitz nevus and melanoma
Special Studies
-
♦
Most fibrous histiocytomas express FXIIIa but are negative for CD34
-
♦
Dermatofibroma sarcoma protuberans tends to have the opposite staining pattern, but overlap and divergent staining patterns occasionally occu r
Angiomatoid Fibrous Histiocytoma (Fig. 18.38)

Angiomatoid fibrous histiocytoma (A, B).
Clinical
-
♦
A fairly deep-seated, usually subcutaneous, nodule or mass within the extremities of children and adolescents
-
♦
This lesion is considered to be of borderline or intermediate malignancy and may recur and, rarely, metastasize
Microscopic
-
♦
A circumscribed, partially cystic and lobular mass usually centered on subcutaneous tissue
-
♦
This tumor is composed of an admixture of cystic, blood-filled pseudovascular spaces, myxoid lobules of histiocytic-appearing cells, and peripheral lymphocytic inflammation and fibrosis
-
♦
The neoplastic cells are somewhat spindled to plump, epithelioid cells with eosinophilic to amphophilic cytoplasm and mildly pleomorphic nuclei
-
♦
Mitotic figures may be evident
Special Studies
-
♦
The histiocytic-appearing cells often show expression of smooth muscle actin, desmin, and CD34, suggesting to som e a myofibroblastic derivation to this tumor
Plexiform Fibrohistiocytic Tumor
Clinical
-
♦
A slowly growing deep dermal to subcutaneous mass on the extremities of children to young adults
-
♦
This is a tumor of intermediate malignancy that may recur and rarely metastasizes
Microscopic
-
♦
An unencapsulated, irregular biphasic tumor consisting of short fibromatosis-like fascicles of plump spindle cells admixed with nodules of histiocytic and osteoclast-like giant cells with minimal nuclear pleomorphism
-
♦
The admixture of nodules and fascicles gives this tumor a plexiform appearance at low power
Juvenile Xanthogranuloma (Fig. 18.39)

Juvenile xanthogranuloma.
Clinical
-
♦
Solitary to multiple, yellow to red papules on the head and neck region of infants are the most common presentation
-
♦
However, adolescents and adults may also be affected, and other body sites may be involved
-
♦
Visceral involvement may be evident with the eye being the most common extracutaneous site of involvement
-
♦
Typically, the cutaneous lesions regress over time
Microscopic
-
♦
Fairly well-circumscribed collection of histiocytes within the dermis admixed with Touton giant cells, xanthomatized histiocytes, and chronic inflammatory cells
-
♦
The epidermis is spared, but periadnexal involvement is common
-
♦
Spindle cell and inflammatory cell-rich variants exist
Reticulohistiocytoma and Multicentric Reticulohistiocytosis
Clinical
-
♦
Solitary and multicentric variants exist
-
♦
The former is usually a yellow to brown nodule on the upper body of adults, while the latter shows multiple lesions associated with a destructive arthritis and constitutional symptoms, also in adults
-
♦
Occasionally, the multicentric variant is associated with visceral neoplasia
Microscopic
-
♦
Both variants are characterized by fairly well-circumscribed proliferations of large, eosinophilic histiocytes with “glassy” cytoplasm
-
♦
The individual cells may contain more than a single nucleus, but Touton giant cells are usually absent, and xanthomatized histiocytes are not generally present
-
♦
Mild nuclear pleomorphism and admixed inflammation with eosinophils and lymphocytes may be evident
Atypical Fibroxanthoma (Fig. 18.40)

Atypical fibroxanthoma.
Clinical
-
♦
Typically a solitary, often ulcerated polypoid nodule on the sun-exposed skin (head and neck) of the elderly
-
♦
A less common variant occurs on the trunk and extremities of young adults
-
♦
These tumors, when limited to superficial tissues, may locally recur but have minimal metastatic potential
Microscopic
-
♦
A nodular, often well-circumscribed, proliferation of very pleomorphic epithelioid to spindle cells with frequent mitoses, often atypical
-
♦
These tumors are usually centered on the dermis and frequently about the dermal–epidermal junction where they stop abruptly
-
♦
Epidermal ulceration is common, but true epidermal involvement with pagetoid spread should raise concerns about malignant melanoma or squamous cell carcinoma
-
♦
Rarely, the tumor is composed of spindle cells in poorly defined fascicles and may be mistaken for leiomyosarcoma
-
♦
While occasional tumors may show superficial involvement of the subcutaneous tissues, extensive subcutaneous involvement and/or prominent vascular invasion and necrosis should lead to an alternate diagnosis (e.g., malignant fibrous histiocytoma)
Special Studies
-
♦
This tumor is a diagnosis of exclusion; therefore, S-100 protein, cytokeratin, and desmin should be negative by immunoperoxidase technique to exclude malignant melanoma, carcinoma, and leiomyosarcoma, respectively
-
♦
Smooth muscle actin may be expressed by a subset of these tumors and is not indicative of smooth muscle differentiation (leiomyosarcoma) in the absence of desmin positiv ity
Malignant Fibrous Histiocytoma
General
-
♦
These tumors are rarely primary cutaneous lesions and have overlapping histologic features with atypical fibroxanthoma
-
♦
The latter tumor is often considered to be a superficial variant of malignant fibrous histiocytoma with minimal metastatic potential
-
♦
The term malignant fibrous histiocytoma should be used for those tumors that demonstrate deep tissue involvement, vascular invasion, or extensive necrosis as detailed above
-
♦
The histologic subtypes and clinical distribution of this tumor are detailed in the chapter on soft tissue tumor
Xanthomas and Xanthelasma (Fig. 18.41)

Verruciform xanthoma.
Clinical
-
♦
Numerous clinical and histologic subtypes exist, many of which are related to systemic lipid abnormalities and represent storage disorders
-
♦
Eruptive
-
Yellow papules on the buttocks and other sites associated with type I hyperlipoproteinemia
-
-
♦
Tuberous
-
Yellow papules and nodules on the extensor surfaces associated with hyperlipoproteinemia types II–IV
-
-
♦
Tendinous
-
Nodules or masses on the tendons of the extremities associated most frequently with type II hyperlipoproteinemia
-
Planar
-
Yellow papules and plaques that may involve intertriginous sites, palmar creases, or more multiple sites in a diffuse fashion
-
The intertriginous variant is associated with type II hyperlipoproteinemia, the palmar variant with type III hyperlipoproteinemia, and the diffuse variant with hematopoietic disorders
-
-
♦
Xanthelasma
-
Yellow plaques on the eyelids, which are associated with lipid abnormalities in only approximately 50% of patients (type III hyperlipoproteinemia)
-
-
♦
Xanthoma disseminatum
-
Not a true storage disorder but, rather, a non-X histiocytosis that presents as yellow-red papules and plaques on the flexural surfaces and mucosal membranes of young adults
-
There is no association between lipid abnormalities and this disorder
-
-
♦
Verruciform xanthoma
-
Usually a solitary, yellow-red, papillomatous lesion of the mouth, this localized process may be seen at a number of cutaneous sites as a primary lesion or as a secondary phenomena in other disorders (e.g., squamous cell carcinoma, epidermal nevi, lupus erythematosus)
-
Microscopic
-
♦
All of the above lesions show an admixture of xanthomatized histiocytes, nonxanthomatized histiocytes, and chronic inflammatory cells in varying proportions depending on the age and evolution of the lesion
-
♦
These lesions are typically dermal limited but, occasionally, show more extensive cutaneous involvement
-
♦
Epidermal involvement is not evident
-
♦
Occasional cases will have numerous multinucleated giant cells and/or Touton giants cells and, hence, show overlap with juvenile xanthogranuloma
-
♦
This is particularly true of xanthoma disseminatum, which should be distinguished by clinical criteria
-
♦
Verruciform xanthoma is a special histologic variant characterized by epidermal acanthosis, papillomatosis, parakeratosis, intraepidermal neutrophils, and a subepidermal proliferation of markedly xanthomatized histiocytes
Special Studies
-
♦
Xanthomas and the non-X histiocytoses are S-100 protein−, CD1a–, and macrophage markers+ (CD68), with Birbeck granule
Langerhans Cell Histiocytosis (LCH , Histiocytosis X, Fig. 18.42)

Langerhans cell histiocytosis (A, B).
Clinical
-
♦
Three clinical variants of this disease have historically been described
-
♦
Letterer–Siwe disease is an acute disseminated form characterized by numerous brown papules on the scalp or face of infants with visceral involvement
-
♦
Hand–Christian–Schuller disease is a chronic, multifocal variant with osseous and localized visceral involvement that affects older children and adults and only occasionally involves the skin
-
♦
Eosinophilic granuloma is a chronic, focal variant that typically involves osseous sites in adults but may involve the skin
-
♦
Many cases of LCH do not fit into the above categories and can show a wide spectrum of manifestations
Microscopic
-
♦
Nodular or loose aggregates of Langerhans cells within the dermis variably admixed with multinucleated cells, eosinophils, neutrophils, and chronic inflammatory cells
-
♦
Epidermal involvement is common and aids in distinguishing this lesion from the non-X histiocytoses and urticaria pigmentosa
-
♦
Proper diagnosis rests on identifying the Langerhans cell that is a histiocyte-like cell with abundant, eosinophilic to amphophilic cytoplasm and a reniform, sometimes twisted nucleus with occasional longitudinal grooves
Immunoperoxidase
-
♦
Langerhans cells are S-100 protein+ and CD1a+
Electron Microscopy
-
♦
Birbeck granules are considered diagnostic of Langerhans cell differentiation
Congenital Self-Healing Reticulohistiocytosis
Clinical
-
♦
Single or multiple, sometimes ulcerated, papules or nodules on the face, trunk, and extremities of newborns
-
♦
Lesions are usually present at birth but occasionally will develop during the perinatal period
-
♦
Lesions typically regress within 2–4 months
Microscopic
-
♦
The histologic appearance of this lesion is similar to that of LCH, from which it cannot be reliably separated on histologic grounds alone
-
♦
In general, this entity has larger, more eosinophilic cells with “glassy” cytoplasm than LCH
-
♦
PASD-positive intracytoplasmic inclusions may be seen in this tumor but are apparently not present in LCH
-
♦
Epidermal involvement may rarely be present
Immunoperoxidase
-
♦
S-100 protein+, CD1a+
Electron Microscopy
-
♦
In addition to Birbeck granules, dense, myelin-like bodies with lamination are evident in this entity and may allow distinction from LCH
Differential Diagnosis
-
♦
This entity is best separated from LCH using clinical criteria; the electron microscopic findings may aid in this process
Indeterminate Cell Histiocytosis
General
-
♦
Occasional histiocyte-like proliferations demonstrate S-100 protein+ and CD1a+ on immunoperoxidase studies but no Birbeck granules on electron microscopy
-
♦
These proliferations have no distinct clinical or histologic characteristics at present
Benign Cephalic Histiocytosis
Clinical
-
♦
A non-X histiocytosis usually presenting as multiple yellow to red papules on the face of young children which completely regress with time
Microscopic
-
♦
A cellular, somewhat cohesive infiltrate of plump histiocytes often with admixed eosinophils is evident within the dermis
-
♦
The overlying epidermis may be attenuated or ulcerated, but epidermotropism is not evident
-
♦
Mild nuclear pleomorphism may be seen
Eruptive Histiocytoma
Clinical
-
♦
A non-X histiocytosis characterized by numerous, flesh-colored to red papules occurring in crops on the trunk, proximal extremities. and, occasionally, the mucosal membranes of adults
-
♦
Lesions may regress, persist, and/or recur
Microscopic
-
♦
A bland infiltrate of histiocytes with or without co-infiltration of other inflammatory cells within the dermis
Fibrous Proliferations and Tumors
Hypertrophic Scar and Keloid
Clinical
-
♦
Hypertrophic scars are slightly raised, red, smooth, and firm lesions at sites of previous injury which have no tendency for recurrence and no racial predilection
-
♦
Keloids are raised to polypoid, red to flesh-colored lesions usually, but not always, occurring at sites of injury and growing beyond the limits of the injured site
-
♦
These lesions may recur and are more common in Blacks
Microscopic
-
♦
A fairly cellular, often nodular proliferation of dermal fibroblasts in a variably collagenized stroma with only minimal hyalinization characterizes the hypertrophic scar
-
♦
Keloids show more extensive and, often, less cellular nodular fibroblastic proliferations with extensive hyalinization of collagen
Nodular Fasciitis /Proliferative Fasciitis /Proliferative Myositis
Clinical
-
♦
Reactive, nonneoplastic proliferations presenting as rapidly growing, deep nodules or masses on the trunk or extremities of adults
-
♦
Virtually any site may be affected
Microscopic
-
♦
All are proliferations of bland, reparative, bipolar spindle cells embedded in a variably myxoid to collagenized stroma
-
♦
Most lesions are centered on the fascia/subcutaneous tissue interface, but dermal, vascular, and skeletal muscle variants are not uncommon
-
♦
The spindle cells have bland nuclear features, scattered normal mitotic figures and wispy, pointed cytoplasm, giving these lesions a “tissue culture” appearance
-
♦
Extravasated erythrocytes and admixed chronic inflammatory cells are additional features
-
♦
The proliferative variants have, in addition to the above, a population of large, ganglion-like cells admixed within the spindle cells
Fibroma of Tendon Sheath
Clinical
-
♦
Slowly growing, benign fibrous nodule firmly attached to the tendon sheath on the distal extremities of adults
Microscopic
-
♦
A well-circumscribed, lobulated proliferation composed of densely hyalinized, paucicellular collagen centrally and more cellular fibroblastic proliferations peripherally
-
♦
The individual lobules often have peripheral stromal clefting but lack nuclear pleomorphism, mitotic activity, or necrosis
Giant Cell Tumor of Tendon Sheath (Fig. 18.43)

Giant cell tumor of tendon sheath.
Clinical
-
♦
Similar to fibroma of tendon sheath (see above)
Microscopic
-
♦
A well-circumscribed, nodular to multilobular tumor composed of a proliferation of plump histiocyte-like cells admixed with multinucleated giant cells, spindle cells, foam cells, and hemosiderin-laden cells in a variably collagenized matrix
-
♦
Mitotic figures may be evident, but no cytologic atypia or necrosis is evident
-
♦
The latter aids in distinguishing this lesion from epithelioid sarcoma
Acrochordons (Soft Fibroma, Skin Tags, Fibroepithelial Polyps)
Clinical
-
♦
Polypoid, filiform, or pedunculated flesh-colored lesions typically involving the groin, axilla, and neck region of adults
Microscopic
-
♦
A polypoid lesion with epidermal acanthosis overlying a variably hyalinized fibrovascular core
-
♦
Adipocytes may be abundant in the central aspect of the lesion
Pleomorphic Fibroma
Clinical
-
♦
A benign polypoid to dome-shaped, flesh-colored lesion on the trunk or extremities of adults
Microscopic
-
♦
A paucicellular, polypoid proliferation of large, pleomorphic cells with hyperchromatic nuclei, small nucleoli, and scant cytoplasm embedded in a fibrous stroma
-
♦
Rare mitotic figures may be seen in these lesions and do not imply an aggressive course
Sclerotic Fibroma
Clinical
-
♦
Usually a solitary, flesh-colored nodule in adult patients
-
♦
Multiple lesions may be associated with Cowden disease
Microscopic
-
♦
A well-circumscribed, nodular proliferation of hyalinized, paucicellular fibrous tissue with laminated, cleft-like stromal spaces
Angiofibroma (Fibrous Papule , Oral Fibroma , Acquired Digital Fibrokeratoma , Pearly Penile Papules )
Clinical
-
♦
Papular to polypoid, flesh-colored lesions usually in adults
Microscopic
-
♦
A faintly polypoid, well-circumscribed proliferation of fibrovascular tissue with scattered hyperchromatic, occasionally multinucleated, stellate cells within the upper dermis
-
♦
In the digital variant, there are overlying epidermal acanthosis and hyperkeratosis with the dermal collagen fibers oriented parallel to the long axis of the lesion
Elastofibroma
-
♦
Typically a deep-seated, subscapular mass in older adults
-
♦
Occasionally other sites are involved
Microscopic
-
♦
An irregular, unencapsulated proliferation of paucicellular collagen admixed with enlarged and often globular elastic fibers best visualized with elastic stains
Dermatomyofibroma
Clinical
-
♦
A benign, solitary, flesh-colored to hyperpigmented plaque on the shoulder region of young adults
Microscopic
-
♦
A well-circumscribed proliferation of spindled, bland myofibroblastic cells in thin fascicles within the dermis
-
♦
The fascicles are oriented parallel to the epidermis except near adnexal structures where they assume a perpendicular growth pattern relative to the epidermis
-
♦
No nuclear pleomorphism, necrosis, or significant mitotic activity is evident
Myofibroma/Myofibromatosis
Clinical
-
♦
Solitary and multifocal variants exist
-
♦
The solitary variants may be seen in infants, young children, and adults and typically present as a dermal or subcutaneous nodule on the head, neck, trunk, or extremities
-
♦
The multifocal variants are seen in infancy or as congenital lesions
-
♦
Multiple soft tissue lesions may be seen, and, if visceral involvement is present, there are increased morbidity and mortality
-
♦
The solitary variants in children, however, have a tendency to regress
Microscopic
-
♦
An unencapsulated, well-circumscribed, biphasic dermal, and/or subcutaneous tumor composed of an admixture of peripheral smooth muscle-like fascicles admixed with more centrally located immature, mesenchymal-like spindle cells embedded in a myxoid background
-
♦
The latter component often has a hemangiopericytoma-like proliferation of blood vessels
-
♦
Mitotic figures and necrosis may be seen and usually do not herald an aggressive course
Infantile Digital Fibroma/Fibromatosis
Clinical
-
♦
A benign, rapidly growing nodule on the fingers or toes of infants and young children
-
♦
Lesions may be multiple and typically regress over time
Microscopic
-
♦
A moderately cellular, usually well-circumscribed proliferation of spindled myofibroblasts embedded in a collagenous stroma
-
♦
The spindle cells have characteristic actin-positive intracytoplasmic eosinophilic inclusions
Fibrous Hamartoma of Infancy (Fig. 18.44)

F ibrous hamartoma of infancy (A, B).
Clinical
-
♦
A hamartomatous lesion typically presenting as a deep dermal to subcutaneous nodule or plaque on the trunk of young children (usually less than 3 years of age)
Microscopic
-
♦
A deep dermal to subcutaneous, irregular, triphasic proliferation that merges with adjacent tissue
-
♦
The proliferation is composed of an admixture of densely collagenized, fibromatosis-like fascicles of bland spindle cells, myxoid and myofibroblastic lobules, and adipocytes showing a range of differentiation from lipoblast-like to mature univacuolated cells
-
♦
The collagenized fascicles frequently appear to arise from the deep dermis and “rain down” into the subcutaneous tis sue
Fibromatosis
General
-
♦
A variety of fibromatoses may present as cutaneous masses, and these are discussed within the chapter on soft tissue pathology
Giant Cell Fibroblastoma (Fig. 18.45)

Giant cell fibroblastoma.
Clinical
-
♦
A tumor of intermediate-grade malignancy occurring almost exclusively in children as a nodule or plaque on the torso or extremities
-
♦
This tumor shows a tendency to local recurrence but has minimal to no metastatic potential
-
♦
Giant cell fibroblastoma is frequently associated with dermatofibroma sarcoma protuberans (see below) and may precede, follow, or occur with this related lesion
Microscopic
-
♦
An infiltrative, dermal, and often subcutaneous tumor composed of mildly pleomorphic spindle cells embedded in a variably myxoid stroma
-
♦
The hallmark of this tumor is the presence of pseudovascular spaces lined by pleomorphic, hyperchromatic, and multinucleated-appearing cells that are not truly of endothelial origin
Special Studies
-
♦
Similar to DFSP, these tumors may express CD34
Dermatofibroma Sarcoma Protuberans (DFSP , Fig. 18.46)

Dermatofibrosarco.ma protuberans.
Clinical
-
♦
An indurated, red to blue, plaque-like. or multinodular lesion on the trunk or extremities of young to middle-aged adults
-
♦
Childhood variants also exist and may have co-infiltrating giant cell fibroblastoma
-
♦
This tumor has a significant local recurrence rate but rarely metastasizes
-
♦
When a fibrosarcoma component is present, the risk of metastases increases significantly
Microscopic
-
♦
An infiltrative, dermal, and subcutaneous proliferation of monotonous spindle cells in distinctly storiform pattern
-
♦
Unlike dermatofibroma, there typically is no epidermal hyperplasia, but basilar hyperpigmentation may be seen
-
♦
Tumor cells infiltrate the subcutaneous fat in a characteristic lacelike fashion
-
♦
The tumor cells are remarkably bland appearing and monomorphic
-
♦
The mitotic rate is usually low
-
♦
Occasional tumors have a prominent myxoid background, while others show transition to higher-grade fibrosarcoma
-
♦
DFSP usually lacks the co-infiltration of inflammatory cells, giant cells, and xanthoma cells typically present in dermatofibroma
-
♦
A pigmented variant of DFSP, the Bednar tumor, exists and has in addition to the above variable numbers of melanin-laden, dendritic-appearing cells
Special Studies
-
♦
DFSP is typically CD34+, S-100 protein−, and FXIIIa–
Fibrosarcoma
Clinical
-
♦
Two clinical variants exist: an infantile (congenital) form and an adult form
-
♦
The former typically presents as a large mass on the extremities of infants and has a relatively good prognosis compared to its adult counterpart
-
♦
The adult variant also typically involves the extremities but has a high recurrence and metastatic rate with subsequent increased mortality
Microscopic
-
♦
Both variants are characterized by a proliferation of mildly pleomorphic spindled cells embedded in a variably collagenized matrix
-
♦
The spindle cells are arranged in fascicles with a herringbone pattern that is more cellular than the fascicles of the fibromatoses
-
♦
Mitotic activity is always present but varies in quantity
-
♦
The infantile variant may have more immature rounded cells with a less prominent herringbone pattern
-
♦
Chronic inflammatory cells are frequently admixed within this variant
Special Studies
-
♦
Vimentin+; some are actin+
-
♦
This tumor is a diagnosis of exclusion, and other sarcomas and the fibromatoses should be considered prior to diagnosis
Epithelioid Sarcoma
Clinical
-
♦
A malignant tumor of uncertain origin typically presenting as firm, often ulcerated nodules on the hand, wrist, or forearm of adolescents and young adults
-
♦
This tumor frequently shows multiple recurrences as well as metastases
Microscopic
-
♦
Usually a multinodular tumor involving the dermis and/or subcutaneous tissue
-
♦
The nodules frequently are well demarcated and have central necrosis, simulating necrotizing epithelioid granulomas
-
♦
The lesional cells are plump, round, histiocyte-like cells with abundant eosinophilic cytoplasm and relatively uniform ovoid nuclei
-
♦
An admixed spindle cell component may be evident
-
♦
There is usually a faint, collagenized stroma surrounding the individual cells
-
♦
Multinucleated giant cells are not typically seen in this tumor, a feature that aids in distinguishing this lesion from giant cell tumor of tendon sheath
Special Studies
-
♦
The lesional cells have a relatively unique immunophenotype being EMA+, vimentin+, and cytokeratin+
Synovial Sarcoma
General
-
♦
Synovial sarcoma may rarely present as a cutaneous mass and is discussed in detail in the chapter on soft tissue pathology
Vascular Proliferations, Malformations, and Tumors
Reactive, Nonneoplastic Vascular Proliferations, and Telangiectasias
Nevus Flammeus
Clinical
-
♦
A congenital vascular telangiectasia/malformation with many clinical forms including the salmon patch and the port-wine stain
-
♦
The former is a pink-red, macule/patch on the glabella that regresses during childhood
-
♦
The latter is a large, unilateral, red facial plaque that persists and may be associated with Sturge–Weber, Klippel–Trenaunay, or other vascular syndromes
Microscopic
-
♦
Dilated (telangiectatic), thin-walled vessels are present within the papillary and superficial reticular dermis
Phakomatosis Pigmentovascularis
General
-
♦
A group of hamartomatous lesions consisting of nevus flammeus in combination with a variety of pigmented lesions (Mongolian spot, nevus spilus, and nevus pigmentosus)
Eccrine Angiomatous Hamartoma
Clinical
-
♦
An angiomatous, sometimes painful, nodular lesion on the acral regions of children
Microscopic
-
♦
A hamartomatous proliferation of mature eccrine glands and thin-walled vessels in the deep dermis or subcutaneous fat
-
♦
Occasionally, other mesenchymal elements, particularly adipocytes, may also be admixed with the above
Nevus Anemicus
Clinical
-
♦
A solitary, circumscribed, pale, macule, or patch on the torso thought to be secondary to vascular hyperreactivity to catecholamines
Microscopic
-
♦
No histologic abnormalities are evident within this clinical lesion
Lymphangioma Circumscriptum (Fig. 18.47)

L ymphangioma.
Clinical
-
♦
Grouped, vesicle-like lesions arranged in a plaque-like form on any cutaneous surface and appearing at birth or early in life
Microscopic
-
♦
Dilated, thin-walled lymphatic structures lined by flattened, bland endothelial cells are evident within the superficial dermis and are intimately associated with an acanthotic, surrounding epidermis
-
♦
Occasional cases have a deeper dermal component, and these variants may recur if superficially excised
Cavernous Lymphangioma
Clinical
-
♦
A congenital or infantile, doughy mass involving the head, neck, or extremities which may recur if incompletely excised
Microscopic
-
♦
Numerous, variably sized lymphatic spaces are evident within the dermis and subcutaneous tissues
-
♦
The lymphatic spaces are lined by flattened, bland endothelium and are variably filled with eosinophilic proteinaceous material
-
♦
Chronic inflammatory cells may be seen within the vessel walls or the stroma of this proliferation
Cystic Hygroma
Clinical
-
♦
A large, cystic mass of the posterior neck of infants that is usually congenital and may be associated with Turner syndrome
Microscopic
-
♦
Numerous, large, and cystically dilated lymphatic spaces within the dermis and subcutaneous tissues are evident in this lesion
-
♦
Lymphoid aggregates are frequently present in the walls of these structures and aid in differentiating this lesion from other hemangiomatous processes
Lymphangiomatosis
Clinical
-
♦
A rare, often fatal, congenital disease which typically presents as spongelike masses involving the skin of the extremities along with bone and visceral involvement
-
♦
Rare cases are limited to the extremities and a have a better prognosis than their systemic counterparts
Microscopic
-
♦
Infiltrating, interanastomosing, and variably dilated lymphatic structures are evident in the dermis and underlying soft tissues in this entity
Spider Angioma (Nevus Araneus )
Clinical
-
♦
A red papule with “spidery” red legs on any cutaneous surface in both children and adults
-
♦
These lesions occur with an increased incidence in pregnancy, liver disease, and thyrotoxicosis
Microscopic
-
♦
A central, dilated dermal arteriole is present and is interconnected to a superficial network of dilated capillaries
Venous Lake
Clinical
-
♦
A dark blue papule on the sun-damaged skin of older adults, especially the ears, lips, and face
Microscopic
-
♦
A superficial, dilated venous structure is evident within the dermis
Hereditary Hemorrhagic Telangiectasia (Osler–Weber–Rendu Syndrome )
Clinical
-
♦
An autosomal dominant inherited disorder characterized by cutaneous and visceral telangiectasias beginning in childhood
Microscopic
-
♦
Telangiectatic superficial vessels are present in the dermis
Angiokeratoma (Fig. 18.48)

Angiokeratoma.
Clinical
-
♦
Four clinical variants exist
-
Fordyce: multiple, dark papules on the scrotum or vulva of the elderly
-
Mibelli: an autosomal dominant inherited disease characterized by warty papules on the extremities of children
-
Angiokeratoma corporis diffusum: widespread cutaneous lesions with a bathing-trunk distribution and an association with Fabry disease (X-linked, alpha-galactosidase deficiency)
-
Solitary
-
Microscopic
-
♦
The microscopy of all these variants is similar consisting of superficial, thin-walled, ectatic vessels closely associated with an acanthotic epidermis
-
♦
The Fabry-associated variant may show vacuolization of endothelial and smooth muscle cells which corresponds to glycolipid lamellar deposits on electron microscopy
Angiolymphoid Hyperplasia with Eosinophils (ALH , Epithelioid Hemangioma)
Clinical
-
♦
Red-blue papules and nodules on the head of adults of uncertain etiology
-
♦
Occasional patients will have peripheral blood eosinophilia
Microscopic
-
♦
Well-circumscribed nodule or nodules are evident within the dermis and/or subcutaneous tissue and are composed of an admixture of variably sized vessels, a polymorphous lymphoid infiltrate, and a variable number of eosinophils
-
♦
Enlarged, often vacuolated, and hobnailed endothelial cells line the vessels
-
♦
The lymphoid infiltrate is composed of an admixture of T and B lymphocytes on immunoperoxidase studies and, rarely, forms germinal centers
Differential Diagnosis
-
♦
ALH should be distinguished from Kimura disease, which it vaguely resembles clinically and histologically
-
♦
The latter is more common in adolescents and young adults of Asian descent and is characterized by cutaneous nodules with a wider cutaneous distribution associated with lymphadenopathy and peripheral eosinophilia
-
♦
Histologically, Kimura disease lacks the vascular proliferation of ALH and has more prominent lymphoid follicles with germinal center formation
Pyogenic Granuloma (Lobular Capillary Hemangioma )
Clinical
-
♦
A hyperplastic, possibly neoplastic, lesion typically presenting as a solitary (occasionally multiple), polypoid, glistening red mass which may locally recur
Microscopic
-
♦
A polypoid, intradermal lesion frequently surrounded by an epidermal collarette and characterized by a lobular proliferation of bland capillaries and venules in a myxoid background
-
♦
Overlying ulceration and prominent inflammation are frequently present
Bacillary Angiomatosis
Clinical
-
♦
An infectious disease mimicking a vascular neoplasm, this lesion is most commonly seen as an angiomatous lesion in immunosuppressed patients but may also affect the immunocompetent. Bartonella quintana and henselae are the responsible organisms
Microscopic
-
♦
A pyogenic granuloma-like vascular proliferation with the additional features of numerous neutrophils, leukocytoclasia, and granular, basophilic, intracytoplasmic masses within the endothelial cells lining the vascular proliferation
-
♦
The masses prove to be clumps of bacteria that stain nicely by the Warthin–Starry technique
Differential Diagnosis
-
♦
Verruga peruana is a related disease that is endemic in Peru and caused by Bartonella bacilliformis
Intravascular Papillary Endothelial Hyperplasia (Masson Hemangioma )
Clinical
-
♦
A proliferative/reorganizing thrombus that may involve any cutaneous or mucosal surface but is frequently seen in rectal tissue
Microscopic
-
♦
Typically a localized process involving a single vessel or occasionally multiple adjacent vessels and characterized by numerous, intraluminal, endothelial-lined papillary structures with hylanized connective tissue cores
-
♦
The endothelial cells lack nuclear atypia or significant mitotic activity and, generally, do not “pile up” or stratify
Pseudo-Kaposi Sarcoma
Clinical
-
♦
A group of pseudoneoplastic lesions including acroangiodermatitis and Stewart–Bluefarb syndrome
-
♦
The former is a variant of severe stasis dermatitis that typically involves the lower extremities of older adults
-
♦
The latter is an arteriovenous malformation unilaterally involving a lower extremity in a young adult
Microscopic
-
♦
Acroangiodermatitis is characterized by a relatively superficial proliferation of small, bland vascular structures which are often thick walled and may be arranged in a lobular architecture
-
♦
There is associated chronic inflammation, dermal hemosiderin deposition, erythrocyte extravasation, and overlying epidermal acanthosis and hyperkeratosis
-
♦
The Stewart–Bluefarb syndrome shows a transdermal proliferation of similar vessels, and, occasionally, an arteriovenous malformation may identified in the deeper tissues
Differential Diagnosis
-
♦
These reactive proliferations should be distinguished from Kaposi sarcoma which is characterized by a more infiltrative vascular proliferation which surrounds the adnexa, dissects dermal collagen, and shows a vessel-around-vessel growth pattern (the promontory sign)
Benign Vascular Neoplasms
Angioma Serpiginosum
Clinical
-
♦
Multiple, gyrate papules on the extremities of children and young adults
Microscopic
-
♦
A clustered proliferation of thick-walled capillaries is evident within the papillae of the superficial dermis
Hemangiomas (Infantile, Cavernous, Capillary, Superficial, and Deep, Fig. 18.49)

C avernous hemangioma.
Clinical and General
-
♦
A variety of confusing terms have been utilized for hemangiomas rapidly developing in infancy, shortly after birth
-
♦
Traditionally, pathologists have classified these lesions as capillary or cavernous hemangiomas, with the thought that the former regress while the latter do not
-
♦
It is now clear that this division is erroneous and that, instead of representing distinct histologic entities, capillary and cavernous histologic changes are merely the histologic findings along points of time in the evolution of all infantile hemangiomas
-
♦
Dermatologists instead classify infantile hemangiomas as superficial or deep depending on whether the overlying skin surface is bright red or largely normal
-
♦
Further, almost all infantile hemangiomas experience some regression after their initial period of rapid growth, regardless of the histologic type
Microscopic
-
♦
Early lesions (“cellular hemangioma”) show a highly cellular, often lobular proliferation of endothelial cells with indistinct lumina and scattered mitosis
-
♦
These lesions may be dermal limited or extend into the underlying soft tissue
-
♦
As the lesions age, vascular lumina become more apparent being composed of small capillary-sized vessels (“capillary hemangioma”) which then progress to larger cavernous-sized vessels (“cavernous hemangiom a”)
Cherry Angiomas
Clinical
-
♦
Acquired, small, red papules on the trunk of adults
Microscopic
-
♦
Dilated, mildly thickened capillary blood vessels in the papillary dermis
Acral A-V Tumor (Arteriovenous Hemangioma, Cirsoid Aneurysm)
Clinical
-
♦
Small, red-blue papules on the head, neck, or extremities of adults
Microscopic
-
♦
Localized, mid to upper dermal proliferation of variably sized, thick-walled vessels having features of both arteries and veins
Tufted Angioma (Tufted Angioblastoma)
Clinical
-
♦
Angiomatous appearing, red to brown macules or plaques on the neck, torso, and shoulders of children and young adults
Microscopic
-
♦
Multiple, cellular lobules of endothelial cells with peripheral, slit-like spaces are evident within the dermis and superficial subcutaneous tissue, giving this lesion a “cannonball”-like pattern
Microvenular Hemangioma (Fig. 18.50)

Microvenular hemangioma.
Clinical
-
♦
An acquired, slowly growing red-blue papule on the extremities of young adults
Microscopic
-
♦
A poorly circumscribed, dermal proliferation of monomorphic, thin-walled, branching venules lined by bland endothelium
-
♦
The venules dissect through the collagen raising some concern for Kaposi sarcoma or low-grade angiosarcoma, but the atypia associated with these two lesions is absent
Targetoid Hemosiderotic Hemangioma
Clinical
-
♦
A red papule surrounded by clear and ecchymotic halos in succession on the trunk or extremities of adults
Microscopic
-
♦
Thin-walled, somewhat dilated vascular structures with intraluminal papillae and hobnailed endothelium characterize this lesion centrally
-
♦
The peripheral and deep aspects of this tumor show interanastomosing vascular spaces that dissect the dermal collagen in association with hemosiderin deposition and chronic inflammatory cells
Glomeruloid Hemangioma
Clinical
-
♦
An unusual vascular proliferation that occurs in the setting of POEMS syndrome, these lesions are typically red, dome-shaped to flat papules and macules on the trunk and extremities of adults
Microscopic
-
♦
A glomerulus-like proliferation of tightly entwined capillary-sized blood vessels is present in the upper dermis
-
♦
The endothelial cells have characteristic, intracytoplasmic, eosinophilic, PAS+ inclusions that represent absorbed immunoglobulin
Kaposiform Hemangioendothelioma
Clinical
-
♦
A childhood neoplasm with a predilection for the retroperitoneum that rarely involves the skin
Microscopic
-
♦
A multinodular, cellular neoplasm involving the dermis and underlying soft tissue
-
♦
The nodules are composed of fascicles of bland spindle cells, small congested capillaries, slit-like vascular spaces, and epithelioid endothelial cells with hemosiderin, hyaline globules, and primitive cytoplasmic lumina
-
♦
No significant mitotic activity is evident
-
♦
The multinodularity, the lack of plasma cells, and the lack of atypia all aid in distinguishing this lesion from the histologically similar Kaposi sarcoma
Spindle Cell Hemangioendothelioma
Clinical
-
♦
Single or multiple, red-blue, often painful nodules on the extremities of children and young adults
Microscopic
-
♦
A fairly well-circumscribed, dermal and/or subcutaneous, nodular tumor composed of an admixture of large, cavernous vascular spaces admixed with a spindle cell to faintly epithelioid, cellular component
-
♦
The large vascular spaces frequently have thrombosis with intravascular papillary projections
-
♦
The spindle cells often have vacuole-like, intracytoplasmic lumina
Acquired Progressive Lymphangioma (Benign Lymphangioendothelioma )
Clinical
-
♦
An acquired, slowly enlarging, bruise-like plaque on the extremities or trunk of young adults
Microscopic
-
♦
Thin-walled, anastomosing, irregular vascular channels are evident within the dermis and predominate superficially where they are oriented horizontally to the epidermis
-
♦
The deeper dermis also has scattered irregular lumina that are oriented haphazardly or perpendicularly to the overlying epidermis
-
♦
The vascular lumina are lined by bland, flattened endothelium and lack any significant intraluminal contents
Angiomatosis
Clinical
-
♦
A rare, benign, vascular proliferation of childhood characterized by an angiomatous growth involving a large area of the trunk and/or extremity with or without hypertrophy of the affected segment
Microscopic
-
♦
An irregular and haphazard proliferation of variably sized vessels and adipocytes is evident within the dermis and underlying soft tissues
-
♦
A characteristic finding is the presence of small vascular structures clustered near or within the wall of a large, thick-walled vein
Vascular Tumors of Low-Grade Malignancy
Epithelioid Hemangioendothelioma
Clinical
-
♦
Solitary or multiple, cutaneous, and/or visceral masses with a wide age range and geographic distribution
-
♦
These lesions may recur and occasionally metastasize
Microscopic
-
♦
A proliferation of epithelioid to spindled endothelial cells as cords and nests in a myxoid to hylanized stroma
-
♦
Intracytoplasmic lumina with erythrocytes are evident within the epithelioid cells, but well-formed vascular structures are rarely identified
-
♦
The tumor often seems to arise from a large vessel wall, often preserving its vascular architecture
Retiform Hemangioendothelioma
Clinical
-
♦
A plaque-like or nodular tumor on the extremities of young adults characterized by frequent recurrences and low metastatic potential
Microscopic
-
♦
An irregular proliferation of branching, angulated blood vessels lined by hobnailed endothelial cells is present within the dermis and has been likened to similar appearing structures within the rete testis
-
♦
A deeper, more solid component with spindled and epithelioid cells and papillary structures may also be evident
Dabska Tumor (Malignant Endovascular Papillary Angioendothelioma)
Clinical
-
♦
A rare tumor typically presenting as a mass on the head, neck, or extremities of children and adolescents
Microscopic
-
♦
An irregular, dermal proliferation of vascular structures lined by hobnailed endothelium and having numerous papillary, intraluminal projections lined by atypical, hyperchromatic endothelial cells with occasional mitoses
-
♦
Admixed lymphocytes are also frequently present
Kaposi Sarcoma
Clinical
-
♦
Five different clinical subtypes exist
-
♦
Classic
-
Red-blue plaques on the lower extremities of elderly men of Mediterranean descent
-
-
♦
African, endemic variants
-
A nodular, indolent variant affecting the limbs of young to middle-aged men
-
A lymphoadenopathic, aggressive variant affecting young children
-
-
♦
Immunosuppression-associated variant
-
Usually related to transplantation with a potentially aggressive course
-
-
♦
AIDS-related variant
-
An aggressive variant that may involve any anatomic site
-
-
♦
Kaposi sarcoma has been recently linked to human herpes virus type 8 which may play an important role in its pathogenesis
Microscopic
-
♦
The microscopic characteristics are similar in all of the above variants
-
♦
In the patch stage, a few, irregular, and infiltrating small vessels are present predominantly within the superficial dermis
-
♦
The vessels infiltrate the adnexa and frequently grow in a vessel-around-vessel pattern, the “promontory sign”
-
♦
Scattered lymphocytes, plasma cells, and extravasated erythrocytes are evident within the dermis, and hemosiderin deposition is also frequently present
-
♦
The plaque stage shows, in addition to the above, a transdermal infiltrate with spindle cell areas arranged in irregular fascicles
-
♦
The spindle cell component has characteristic sievelike spaces with extravasated erythrocytes, mild nuclear pleomorphism, occasional mitotic figures, and eosinophilic hyaline globules
-
♦
The nodular variant is composed almost exclusively of a fairly well-circumscribed, nodular, dermal, and/or subcutaneous proliferation of spindle cells in fascicles with similar features to the plaque stage
Malignant Vascular Tumors
Angiosarcoma (Fig. 18.51)

A ngiosarcoma.
Clinical
-
♦
Three clinical variants exist
-
♦
Idiopathic angiosarcoma of the face and scalp of the elderly
-
This variant presents as multiple bruise-like, infiltrating plaques and nodules
-
-
♦
Postirradiation angiosarcoma
-
Infiltrating plaques, ulcers, or nodules occurring years after radiation to the involved site
-
-
♦
Lymphedema-associated angiosarcoma (Stewart–Treves syndrome )
-
Angiosarcomas arising in the setting of prolonged lymphedema, usually postmastectomy patients
-
-
♦
The overall survival for patients with cutaneous angiosarcoma is poor with frequent recurrences and early lymph node and visceral metastases characterizing their clinical course
Microscopic
-
♦
All three clinical variants of angiosarcoma show the same spectrum of histologic findings
-
♦
Well-formed, small, often slit-like vessels that interanastomose and dissect the dermal collagen in an infiltrative fashion characterize the low-grade variants
-
♦
The endothelial cell lining may be flattened and nondescript, but areas with nuclear hyperchromasia, mitotic activity, and stratification are usually evident
-
♦
A papillary network lined by atypical endothelial cells may be prominent
-
♦
High-grade lesions are typically more cellular and are composed of sheets or fascicles of polygonal, epithelioid, or spindle cells with nuclear pleomorphism, mitoses, and often prominent nucleoli
-
♦
Well-formed vascular structures may be scant, but intracytoplasmic lumina are often identified and aid in the differential diagnosis
Special Studies
-
♦
CD31, CD34, FVIII, and Ulex europaeus I lectin stain, to a variable degree, endothelial-derived tumors
-
♦
CD31 is probably the most specific and sensitive endothelial cell marker among this group
Tumors of Perivascular Cells
Glomus Tumor (Fig. 18.52)

Glomus tumor.
Clinical
-
♦
These tumors of specialized arteriovenous anastomoses (Sucquet–Hoyer canal) most often present as painful, red-blue nodules on the fingers, but any cutaneous site may be involved
-
♦
A multicentric variant with autosomal dominant inheritance exists
Microscopic
-
♦
These tumors are characterized by a well-circumscribed, deep dermal proliferation of small vessels and a variable number of round to polygonal cells with eosinophilic cytoplasm and uniform, round to ovoid nuclei
-
♦
Rarely, mild, degenerative nuclear pleomorphism may be present
-
♦
The glomangioma, a common variant, has, in addition to the above, a component of large, cavernous vascular structures
-
♦
Tumors that also have a proliferation of smooth muscle, usually perivascular, have been called glomangiomyoma
-
♦
Rare malignant glomus tumors have also been described
Special Studies
-
♦
The glomus cells are smooth muscle a ctin+ and vimentin+ and may stain for desmin
Hemangiopericytoma
General
-
♦
A controversial neoplasm that rarely involves the skin; this tumor is a diagnosis of exclusion as its histologic pattern may be mimicked by a wide variety of neoplasms
-
♦
This tumor is discussed in more detail in the chapter on soft tissue pathology
PEComa
General
-
♦
A rare benign cutaneous neoplasm with morphologic and immunohistochemical evidence of perivascular epithelioid cell (PEC) differentiation
-
♦
Like systemic PEComas (renal angiomyolipoma, lymphangiomyomatosis, etc), they show a female predilection
-
♦
No known association with tuberous sclerosis
-
♦
Most reported cases occur on the extremities
Microscopic
-
♦
Dermal proliferation with neoplastic cells arranged in sheets, nests, or trabeculae, separated by thin capillaries; may extend into subcutis
-
♦
The lesional cells are epithelioid, spindled, or both and have a central round nucleus and clear or granular eosinophilic cytoplasm
-
♦
Mitotic activity is usually absent
Special Studies
-
♦
The neoplastic cells variably express melanocytic (HMB45, melan-A, MiTF) and muscle markers (desmin, actin)
-
♦
The cells are negative or only focally positive for S-100
-
♦
No expression of cytokeratins or epithelial membrane antigen
Melanocytic Proliferations and Pigmentary Disorders
Pigmentary Disorders of the Skin
Melasma
Clinical
-
♦
An acquired, symmetrical, brown hypermelanosis of the face that is more common in women
Microscopic
-
♦
An increase in melanin deposition within the basal epidermis and/or within dermal melanophages
Freckle (Ephelid)
Clinical
-
♦
Small, well-demarcated red-brown macules on sun-exposed areas. The lesions darken with sun exposure
Microscopic
-
♦
Basal keratinocyte hyperpigmentation without elongation of the rete ridges
Postinflammatory Hyperpigmentation
Clinical
-
♦
An acquired excess of melanin pigmentation in areas of preceding inflammation
Microscopic
-
♦
Increased melanophages within the superficial dermis with/without basilar keratinocyte hyperpigmentation
Dowling–Degos Disease
Clinical
-
♦
An autosomal dominant disorder characterized by reticulated, pigmented macules of the flexural areas in combination with pitted, perioral, acneiform scars and comedone-like lesions on the neck and back
Microscopic
-
♦
Filiform to antler-like epidermal downgrowths in association with basilar keratinocyte hyperpigmentation, dermal melanosis, and mild dermal lymphohistiocytic inflammation
Kitamura Reticulate Hyperpigmentation
Clinical
-
♦
An autosomal dominant disorder characterized by reticulated, depressed pigmented macules on the dorsal hands and feet with pits and breaks on the palms and soles
Microscopic
-
♦
Basilar hyperpigmentation with elongation of the rete ridges and epidermal atrophy
Vitiligo
Clinical
-
♦
Acquired, depigmented, white patches surrounded by a normal or hyperpigmented border
Microscopic
-
♦
Absence of melanocytes within the depigmented areas
Albinism
Clinical
-
♦
An inherited disorder of the tyrosinase gene characterized by the lack of ocular pigment (ocular albinism; X-linked recessive) or the lack of ocular, follicular, and cutaneous pigment (oculocutaneous albinism; autosomal recessive)
Microscopic
-
♦
Normal-appearing epidermis containing a normal complement of melanocytes but a complete or markedly reduced amount of melanin production
Piebaldism
Clinical
-
♦
An autosomal dominant disorder with onset at birth characterized by a stationary hypomelanosis of the skin and hair involving the lateral trunk, arms, legs, and forehead (white forelock)
Microscopic
-
♦
Absence of melanocytes and melanin within affected regions
Nevus Depigmentosus
Clinical
-
♦
A congenital, stable hypopigmented macule or patch on the trunk or extremities
Microscopic
-
♦
Normal number of melanocytes but reduced melanin production within the lesional areas
Idiopathic Guttäte Hypomelanosis
Clinical
-
♦
Numerous, small hypopigmented macules on the sun-exposed surface of the extremities
Microscopic
-
♦
Marked reduction of melanin granules within lesional skin in association with epidermal atrophy and flattening of the rete ridges
Café-au-Lait Spot
Clinical
-
♦
Light brown, pigmented macule that may be found on any cutaneous surface and, if numerous, may be associated with neurofibromatosis
Microscopic
-
♦
Increased melanocytes and increased melanin production within the basal epidermis
Electron Microscopy
-
♦
Macromelanosomes
Becker Nevus (Becker Melanosis )
Clinical
-
♦
A hamartomatous lesion characterized by a hyperpigmented patch with hypertrichosis over the shoulder region or back
Microscopic
-
♦
Slight epidermal acanthosis/papillomatosis with basal keratinocyte hyperpigmentation and dermal melanosis
-
♦
A dermal, smooth muscle hamartomatous component may also be present
Mucosal Melanotic Macules
Clinical
-
♦
A pigmented macule/patch on the mucosa of the oral or genital region
Microscopic
-
♦
Basilar keratinocyte pigmentation with or without dermal melanosis
Benign Melanocytic Proliferations
Mongolian Spot
Clinical
-
♦
A slate-blue patch on the lower back of newborns and infants, often of Asian or African descent
-
♦
The lesions typically regress over time
Microscopic
-
♦
Long, wavy, variably pigmented, individual melanocytes are present within the deep dermis and are oriented parallel to the overlying epidermis
Nevus of Ito and Ota
Clinical
-
♦
Both of these lesions present as a slate-blue to mottled macule or patch which may be congenital or develop in adolescence
-
♦
The nevus of Ito typically involves the skin of the scapular, deltoid, or supraclavicular regions, while the nevus of Ota involves the skin of the face, usually in a unilateral fashion
-
♦
The nevus of Ota may be associated with ipsilateral scleral, conjunctival, corneal, or retinal pigmentation
-
♦
The pigmentation persists
-
♦
These lesions may be present individually or in combination with one another or with the Mongolian spot
Microscopic
-
♦
Both of these entities are characterized by the presence of pigmented, spindled, and dendritic, individual melanocytes within the mid and upper dermis
Blue Nevi (Figs. 18.53 and 18.54)

C ommon blue nevus.

Cellular blue nevus (A, B).
Clinical
-
♦
Two subtypes exist
-
A small, well-circumscribed blue to blue-black papule on the hands or feet characterizes the common blue nevus
-
A 1–3 cm or larger blue to blue-gray plaque on the sacrum or buttocks typifies the cellular blue nevus
-
Microscopic
-
♦
Common blue nevus
-
A symmetrical and fairly well-circumscribed proliferation of spindled to dendritic nevomelanocytes within the dermis
-
The dermis frequently is sclerotic within the lesional area
-
-
♦
Cellular blue nevus
-
Typically a large, dermal and/or subcutaneous, symmetrical nodule composed of an admixture of spindled, dendritic, and rounded nevomelanocytes
-
The spindled and dendritic component predominates at the periphery of the lesion, while nests of more rounded nevomelanocytes with melanophages are more common centrally
-
-
♦
Atypical variants may show nuclear pleomorphism, mitotic activity, an infiltrating architecture, and even necrosis
Solar Lentigo
Clinical
-
♦
A uniformly pigmented macule/patch on areas chronically exposed to sunlight
-
♦
Solar lentigines are frequently multiple and are markers of increased risk of melanoma development
Microscopic
-
♦
Elongation of the rete ridges with basilar keratinocyte hyperpigmentation and a mild to marked proliferation of basilar melanocytes in a lentiginous (single cell, nonnested) fashion
Lentigo Simplex
Clinical
-
♦
A congenital or acquired, sharply demarcated, round to oval, macular area of hyperpigmentation, usually less than 5 mm in diameter
-
♦
Most lesions develop in childhood, but new lesions may form in adulthood
-
♦
Multiple lesions may be associated with the LEOPARD, NAME, or Peutz–Jeghers syndromes
-
♦
The speckled lentiginous nevus (nevus spilus) is a variant characterized by a light brown patch with superimposed, darkly pigmented macules
Microscopic
-
♦
Mild to moderate elongation of the rete ridges in association with basilar and, often, suprabasilar keratinocyte hyperpigmentation and a lentiginous proliferation of bland nevomelanocytes
-
♦
Some lentigines show focal junctional nesting and, hence, overlapping features with a junctional nevus
-
♦
The term “ jentigo” has, at times, been used for such lesions
Common Melanocytic Nevi
Clinical
-
♦
Benign, melanocytic proliferations that typically develop in childhood and adolescence
-
♦
The appearances of common melanocytic nevi vary from pigmented macules/papules, to flesh-colored nodules, to papillomatous lesions depending on the relative degree of junctional versus dermal activity and the site of origin
-
♦
These nevi are typically small (<1 cm), evenly pigmented, symmetrical, and sharply bordered
-
♦
The presence of large numbers of nevi on a single individual is a marker of increased risk of melanoma
Microscopic
-
♦
Common melanocytic nevi are characterized by symmetrical and well-circumscribed proliferations of bland, round nevomelanocytes as nests along the dermal–epidermal junction and/or within the dermis
-
♦
The dermal component, if present, shows maturation and lacks significant mitotic activity or cytologic atypia
-
♦
The junctional component may show nevomelanocytic nests with or without an accompanying lentiginous melanocytic proliferation
-
♦
The nests within the junctional component are uniform in size and spacing and are typically limited to the basal epidermis
Dysplastic Nevus (Clark Nevus , Atypical Nevus , B-K Mole )
Clinical
-
♦
A tan-brown to black, irregularly and asymmetrically pigmented macule/papule, usually >5 mm in diameter
-
♦
Multiple lesions may be inherited as the B-K mole (dysplastic nevus) syndrome or the familial atypical mole syndrome
-
♦
This syndrome(s) is associated with a markedly increased risk of melanoma development. Most lesions are sporadic and are associated with a lesser risk of melanoma development
Microscopic
-
♦
Typically a compound nevomelanocytic proliferation showing a spectrum of architectural and cytologic features which include the following:
-
Junctional shouldering
-
Lamellar dermal fibrosis
-
Bridging of the rete ridges by melanocytic nests
-
Melanocytic nuclear pleomorphism with nucleoli
-
Early upward migration of melanocytes within the epidermis
-
Perivascular chronic inflammation at the base of the lesion
-
Pigmented Spindle Cell Nevus of Reed (Fig. 18.55)

Pigmented spindle cell nevus of Reed.
Clinical
-
♦
Sharply defined, heavily pigmented, symmetrical papule on the trunk or extremities of adolescents/young adults
Microscopic
-
♦
Symmetrical and well-circumscribed proliferation of monomorphic, spindled melanocytes along the dermal–epidermal junction and, usually, the papillary dermis
-
♦
The individual melanocytes may have nucleoli, and mitotic figures are commonly seen
-
♦
There may be prominent upward migration of melanocytes within the epidermis
-
♦
Coarse melanin is frequently seen within the melanocytes and associated melanophages
Spitz Nevus (Spindle and Epithelioid Cell Nevus , Fig. 18.56)

Spitz nevus (A, B).
Clinical
-
♦
Smooth-surfaced, round, sharply circumscribed, pink to red papule most commonly involving the face and/or the extremities of children to young adults
Microscopic
-
♦
Spitz nevi are generally well-circumscribed and symmetrical proliferations which may be junctional, compound, or dermal
-
♦
The nuclear pleomorphism that is present within these lesions may be mistaken for malignant melanoma
-
♦
The prototypical Spitz nevus has the following histologic features:
-
Epidermal hyperplasia
-
Hypergranulosis
-
Kamino bodies (cytoid bodies)
-
Large junctional nests of epithelioid to spindled melanocytes
-
Clefting between the junctional nests and the epidermis
-
Deep dermal maturation
-
Nuclear pleomorphism with nucleoli
-
Additional features that may be present and may mimic melanoma include the following:
-
•
Brisk mitotic activity
-
•
Upward epidermal migration of melanocytes
-
•
Adnexal involvement
-
•
-
Congenital Nevus
Clinical
-
♦
A variant of the melanocytic nevus which is present at birth
-
♦
Congenital nevi are often divided into three groups based on their size: small (<1.5 cm), medium (1.5–20 cm), and large (>20 cm)
-
♦
These nevi are typically brown to black and frequently show an irregular surface with hypertrichosis
-
♦
Congenital nevi are associated with an increased risk of melanoma development; the risk is the greatest for the large congenital nevi, which may show malignant transformation in up to 20% of cases
Microscopic
-
♦
Congenital nevi are similar to the common melanocytic nevi in that they are symmetrical, well-circumscribed proliferations with deep maturation
-
♦
They differ from common melanocytic nevi by having the involvement of the deep reticular dermis/subcutis and by showing frequent involvement of adnexal structures
Deep Penetrating Nevus (Fig. 18.57)

Deep penetrating nevus (A, B).
Clinical
-
♦
A darkly pigmented, uniform papule/nodule most often presenting on the trunk or extremities of young adults
Microscopic
-
♦
A distinctly, wedge-shaped proliferation of uniformly atypical melanocytes within the dermis and, occasionally, along the dermal–epidermal junction
-
♦
The nevomelanocytes are arranged into poorly formed nests and irregular fascicles which extend into the deep reticular dermis and/or subcutis without deep maturation
-
♦
These nevomelanocytes have nuclear pleomorphism and nucleoli, but mitotic figures are absent to scarce
-
♦
Dense melanin pigmentation is present throughout the lesion within the melanocytes and adjacent melanophages
Halo Nevus
Clinical
-
♦
A typical melanocytic nevus with a surrounding zone of depigmentation
Microscopic
-
♦
A chronically inflamed nevus of any type
-
♦
The lymphocytes are densely arranged within the dermal component of the nevus and may completely obscure the underlying melanocytic lesion
-
♦
The remaining melanocytes may show some degree of atypia and disorganization, but the typical features of a regressing melanoma are absent
Pigmented Epithelioid Melanocytoma
Clinical
-
♦
A heavily pigmented lesion that usually occurs in children and young adults but can affect any age or ethnic background, a wide variety of anatomic sites, and either gender
-
♦
A controversial and provisional entity, considered as a “borderline” melanocytic neoplasm or low-grade melanoma with a low risk of recurrence, but metastatic potential
-
♦
Nearly half of all patients have metastases in sentinel lymph node biopsies but with only rare reports of spread to viscera. Some authors recommend lymph node biopsy in all cases
-
♦
No adverse outcomes in short-term data but long-term follow-up is currently unavailable
-
♦
There is no known association with Carney complex, although microscopically it resembles epithelioid blue nevus
Microscopic
-
♦
A nonulcerative, circumscribed, or infiltrative dermal mass composed of sheets of epithelioid or spindle cells. May extend into the subcutis along adnexa
-
♦
The epithelioid cells have large round nuclei with or without large nucleoli. Spindle cells may have long dendritic cytoplasmic processes
-
♦
Resembles epithelioid blue nevus of Carney complex and is so-called equine or animal-type melanoma based on heavily pigmented cells
-
♦
Marked cytoplasmic pigmentation may obscure nuclear details, and bleached sections may be necessary to evaluate
-
♦
Mitotic activity is usually absent but may have up to 3/mm2
-
♦
May be part of a combined nevus
Malignant Melanoma (Fig. 18.58 and 18.59)

Superficial spreading malignant melanoma.

Nevoid malignant melanoma .
Clinical
-
♦
The majority of melanomas show a variegated, asymmetrical distribution of dark brown to black pigment within a lesion of greater than 0.5 cm in diameter
-
♦
However, amelanotic melanomas do exist and may mimic other neoplasms
-
♦
Melanomas are divided clinicopathologically into four basic subtypes:
-
Superficial spreading malignant melanoma
-
•
Accounts for approximately 60% of melanomas
-
•
Related to sun exposure
-
•
Shows both a macular and a nodular appearance clinically
-
•
May affect all age groups but predominates in adults
-
•
-
Lentigo maligna melanoma
-
•
Accounts for approximately 10–15% of melanomas
-
•
Related to sun exposure
-
•
Largely a disease of the elderly
-
•
Grows initially as dark macule or patch (lentigo maligna) and develops a papular or nodular component when invasive (lentigo maligna melanoma)
-
•
Head and neck region most commonly affected
-
•
-
Nodular malignant melanoma
-
•
Accounts for approximately 10–20% of all melanomas
-
•
Nodular, often symmetrical appearance clinically
-
•
May be amelanotic
-
•
-
Acral-lentiginous melanoma
-
•
Accounts for 5–10% of all melanomas
-
•
Tumors of the palms, soles, nails, and genitalia
-
•
Most common melanomas of dark-skinned races
-
•
-
Prognostic Factors
-
♦
Tumor thickness is the most important prognostic factor at present, as measured by Clark level or Breslow depth
-
♦
Ulceration
-
♦
Lymphatic invasion
-
♦
Location of the primary melanoma
-
♦
Signs of regression
-
♦
Sex
-
♦
Age
Microscopic
-
♦
Almost all melanomas begin as epidermal proliferations which, if left unchecked, may invade into the dermis and underlying tissues
-
♦
Melanomas have a constellation of atypical cytologic and architectural features that may be present in varying portions within a given lesion including the following:
-
Architectural asymmetry
-
Poor circumscription
-
Upward epidermal migration of melanocytes, nested or single
-
Melanocytic nests vary in size, shape, and distribution
-
No deep maturation of melanocytes
-
Cytologic atypia in the form of nuclear pleomorphism, prominent nucleoli, and mitotic figures
-
Invasion of lymphatic spaces and nerves
-
Adnexal involvement
-
-
♦
The lentiginous variants of melanoma show a predominant single, nonnested proliferation of melanocytes within the epidermis with or without upward epidermal migration
-
♦
The invasive component may be nested or may show a distinct spindled appearance with or without neurotropism (desmoplastic melanoma)
-
♦
The superficial spreading variant of melanoma shows a nested epidermal component with prominent upward epidermal migration, and the invasive component is typically nested but may be spindled
-
♦
The nodular melanoma is largely a dermal tumor with a minor, overlying epidermal component
Staging (see TNM classifications)
-
♦
Stage I
-
Tumor thickness 2.0 mm or less without ulceration
-
-
♦
Stage II
-
Tumor thickness 1.01–2.00 mm with ulceration or tumor thickness > 2.01 mm
-
-
♦
Stage III
-
Any tumor thickness with nodal and/or satellite metastases
-
-
♦
Stage IV
-
Tumor metastatic to distant sites
-
Lymphoproliferative Disorders and Leukemias (also see Chap. 15)
Classification of Cutaneous Lymphomas
-
♦
A variety of cutaneous lymphomas exist, many of which differ significantly from their systemic counterparts in terms of histologic features, behavior, and/or treatment
-
♦
In 1997, the European Organisation for Research and Treatment of Cancer (EORTC) proposed a new cutaneous lymphoma classification based on clinical, histologic, and immunophenotypic criteria with an emphasis on disease entities rather than histologic subgroups. In 2005, the WHO recognized that differences exist between cutaneous lymphomas and their systemic counterparts resulting in the WHO–EORTC classification for cutaneous lymphoma
-
♦
The following lymphoma discussion will focus on the WHO–EORTC classification of lymphoma, and the reader is urged to refer to the systemic lymphoma chapter for comparison (Chap. 15)
WHO–EORTC Classification (2007 update)
-
♦
Cutaneous T-cell and NK-cell lymphomas :
-
Mycosis fungoides (MF)
-
MF variants and subtypes:
-
•
Folliculotropic MF
-
•
Pagetoid reticulosis
-
•
Granulomatous slack skin
-
•
-
Sézary syndrome
-
Adult T-cell leukemia/lymphoma
-
Primary cutaneous CD30+ lymphoproliferative disorders:
-
•
Primary cutaneous anaplastic large cell lymph oma
-
•
Lymphomatoid papulosis
-
•
-
Subcutaneous panniculitis-like T-cell lymphoma
-
Extranodal NK-/T-cell lymphoma, nasal type
-
Primary cutaneous peripheral T-cell lymphoma , unspecified:
-
•
Primary cutaneous aggressive epidermotropic CD8+ T-cell lymphoma (provisional)
-
•
Cutaneous γ/δ T-cell lymphoma
-
•
Primary cutaneous CD4+ small/medium-sized pleomorphic T-cell lymphoma (provisional)
-
•
-
-
♦
Cutaneous B-cell lymphomas :
-
Primary cutaneous marginal zone B-cell lymphoma
-
Primary cutaneous follicle center cell lymphoma
-
Primary cutaneous diffuse l arge B-cell lymphoma, leg type
-
Primary cutaneous diffuse large B-cell lymphoma, other type:
-
•
Intravascular B-cell lymphoma
-
•
-
-
♦
Precursor hematologic neoplasm :
-
Blastic plasmacytoid dendritic cell neoplasm (formerly CD4+, CD56+ hematodermic neoplasm, and blastic NK-cell lymphoma )
-
Primary Cutaneous Marginal Zone B-Cell Lymphoma (Fig. 18.60)

Marginal zone lymphoma (A, B).
Clinical
-
♦
Solitary or multiple tumors/nodules
-
♦
Extremities most often involved
-
♦
Excellent long-term survival ~100%
Microscopic
-
♦
Nodular or diffuse, often bottom-heavy infiltrates
-
♦
Benign germinal centers usually present
-
♦
Malignant small lymphocytes, plasmacytoid lymphocytes, plasma cells, and centrocyte-like cells infiltrate diffusely outside of the germinal centers and may encroach upon the germinal centers,
-
♦
Reactive T cells, eosinophils, and histiocytes are frequently admixed throughout the neoplasm
Immunophenotype
-
♦
CD20+, CD79a+, CD43+/−, Sig+, and cytoplasmic immunoglobulin (Cig)+
-
♦
CD5–, CD23–, and cyclin D1–
Differential Diagnosis
-
♦
Lymphoid hyperplasia
-
♦
Follicular lym phoma
Primary Cutaneous Follicle Center Cell Lymphoma
Clinical
-
♦
Solitary or grouped papules, nodules, or plaques
-
♦
Head and neck region most commonly involved
-
♦
May be associated with annular erythemas
-
♦
Rarely disseminate but frequently recur
Microscopic
-
♦
A tumor composed of follicular center cells either in the form of centrocytes (cleaved cells) or centroblasts
-
♦
Tumor cells are arranged into ill-defined nodules or diffuse sheets
-
♦
Germinal center formation may or may not be present
Immunophenotype
-
♦
CD20+, CD79a+, and usually surface immunoglobulin (Sig)+, and CD21 highlights background follicular dendritic cells
-
♦
CD5–, CD10–, and bcl-2+/– (may have weak positivity)
Differential Diagnosis
-
♦
Marginal zone lymphoma
-
♦
Lymphoid hyperplasia
-
♦
Systemic follicular lymphoma (bcl-2+)
Primary Cutaneous Diffuse Large B-Cell Lymphoma of the Leg (Fig. 18.61)

L arge B-cell lymphoma of the leg (A, B).
Clinical
-
♦
Red to blue nodules/plaques involving one or both legs; may also occur on other cutaneous sites
-
♦
Typically affects older patients, >70 years old
-
♦
Frequently disseminates
-
♦
~50% 5-year survival
Microscopic
-
♦
Diffuse, sheetlike proliferation of large atypical lymphocytes
-
♦
Epidermotropism is generally absent
-
♦
The large lymphocytes may have centrocytic, centroblastic, or immunoblastic features
Immunophenotype
-
♦
CD20+, CD79a+, bcl2+, Sig+/−, and MUM1+
Genotype
-
♦
No t(14,18) translocatio n
Intravascular Large B-Cell Lymphoma
Clinical
-
♦
Violaceous, indurated plaques or patches
-
♦
Lower extremities most often involved
-
♦
Central nervous system involvement may also be present
-
♦
Poor prognosis
Microscopic
-
♦
Large atypical lymphocytes are present within dilated vessels of the dermis and/or subcutis
-
♦
Rarely, atypical lymphocytes may be present adjacent to the vessels
Immunophenotype
-
♦
CD20+, CD79a+, and Sig+; frequently express M UM1 and CD5
Mycosis Fungoides (Fig. 18.62)

Mycosis fungoides (A, B).
Clinical
-
♦
Persistent, erythematous patches and/or plaques which may progress to tumors over the course of many years
-
♦
Annular and serpiginous plaques may be present
-
♦
Trunk and extremities most commonly involved
-
♦
Generally an indolent disease with tumor formation and systemic spread occurring only after many years to decades
Microscopic
-
♦
A band-like, epidermotropic proliferation of variably sized lymphocytes is present in the superficial dermis
-
♦
The epidermotropic lymphocytes frequently populate the basal layer of the epidermis and are generally unassociated with spongiosis
-
♦
The epidermotropic lymphocytes may aggregate into intraepidermal microabscesses (Pautrier microabscesses)
-
♦
The epidermotropic lymphocytes are frequently larger than those within the dermis and display varying degrees of nuclear convolution and cerebriform change
-
♦
The tumor stage shows a more diffuse, often sheetlike, proliferation of atypical, often large, lymphocytes with or without epidermotropism
Immunophenotype
-
♦
CD3+, CD4+, CD7+/−, CD8-, and CD30-
-
♦
Rare CD8+ variants exist
Folliculotropic Mycosis Fungoides
Clinical
-
♦
Erythematous papules or plaques typically affecting the head and neck region
-
♦
Hair loss within the affected regions
-
♦
Typically affects adult patients
Microscopic
-
♦
Marked folliculotropism of atypical lymphocytes
-
♦
Mucinous degeneration of follicular epithelium variably present
-
♦
Lymphocytes usually have the atypical nuclear features of mycosis fungoides, and epidermotropism may be evident
-
♦
Eosinophils are often present
Immunophenotype
-
♦
Similar to mycosis fungoides
Differential Diagnosis
-
♦
Primary (idiopathic) variants of follicular mucinosis affect younger individuals and appear unrelated to mycosis fungoides
-
♦
Other systemic diseases may show secondary follicular mucinosis (e.g., lupus erythematosus)
Pagetoid Reticulosis
Clinical
-
♦
Hyperkeratotic patches or plaques limited to a distal extremity (Woringer–Kolopp type)
-
♦
No systemic involvement present
-
♦
Excellent prognosis
-
♦
The systemic or disseminated form (Ketron–Goodman type) is best considered to be a variant of primary cutaneous CD-8-positive aggressive epidermotropic cytotoxic T-cell lymphoma or γ/δ-positive T-cell lymphoma
Microscopic
-
♦
A distinctly epidermotropic proliferation of large atypical lymphocytes with irregular, often cerebriform, nuclei
-
♦
Minimal to no dermal component
Immunophenotype
-
♦
May be CD4 or CD8 predominant; frequent expression of CD30
Granulomatous Slack Skin
Clinical
-
♦
Pendulous plaques involving the axilla and groin regions
-
♦
Probably a rare variant of mycosis fungoides
-
♦
Males are affected more often than females
Microscopic
-
♦
Dense, dermal, atypical lymphocytic infiltrate admixed with numerous multinucleated histiocytes
-
♦
Multinucleated cells often have a wreath-like arrangement of nuclei
-
♦
Elastolysis is frequently present
-
♦
Dermal lymphocytes are generally small and have cerebriform nuclear features
Immunophenotype
-
♦
Similar to mycosis fungoid es
Sézary Syndrome
Clinical
-
♦
Generalized erythroderma in association with generalized lymphadenopathy and leukemic infiltration of the blood by malignant T cells
-
♦
Alopecia, palmoplantar keratoderma, and leonine facies are common findings
-
♦
Poor prognosis with a 5-year survival of less than 50%
-
♦
Demonstration of a T-cell clone and one of the following are suggested as minimum criteria for diagnosis: absolute Sézary cell count of at least 1000 cells/mm³, demonstration of immunophenotypic abnormalities (CD4/CD8 ratio of more than 10), and loss of any of the T-cell antigens
Microscopic
-
♦
Similar to mycosis fungoides but epidermotropism may be absent
Immunophenotype
-
♦
Similar to mycosis fungoides
Adult T-Cell Leukemia/Lymphoma (ATLL)
General
-
♦
A leukemia/lymphoma associated with the human T-cell leukemia virus (HTLV-1)
Clinical
-
♦
ATLL is endemic in Japan, South America, Central Africa, and the Caribbean
-
♦
ATLL generally develops many years (decades) after infection with HTLV-1
-
♦
Preleukemic, smoldering, chronic, lymphomatous, and acute clinical variants exist
-
♦
The acute phase is characterized by leukemia, lymphadenopathy, organomegaly, hypercalcemia, and cutaneous lesions that may include erythroderma, plaques, papules, nodules, or macules
Microscopic
-
♦
Skin biopsies may resemble mycosis fungoides with an epidermotropic infiltrate of cerebriform lymphocytes or may be considerably more pleomorphic with medium to large-sized lymphocytes with tumor formation
-
♦
The peripheral blood contains pleomorphic lymphocytes with hyperlobated nuclei resembling a clover leaf
Immunophenotype
-
♦
The immunophenotype is similar to mycosis fungoides, and CD25 is frequently expressed
Genetic Findings
-
♦
HTLV-1 genes are clonally integrated into the T-cell tumor DNA by Southern blot analysis
Primary Cutaneous CD30+ Lymphoproliferative Disorders Including Lymphomatoid Papulosis and Primary Cutaneous Anaplastic Large Cell Lymphoma (Fig. 18.63)

CD30+ large T-cell lymphoma.
General
-
♦
Lymphomatoid papulosis (LyP) and primary cutaneous anaplastic large cell lymphoma are part of a spectrum of related clinicopathologic entities having in common a good prognosis and numerous CD30+ large lymphocytes histologically (see Table 18.1)
Table 18.1. Comparison of Lymphomatoid Papulosis (LyP) and CD30+ Cutaneous T-cell Lymphoma (CTCL ) -
♦
At least five morphologic and immunophenotypic variants of LyP are recognized:
-
Type A: composed of clusters CD30+ T cells with an abundant background of mixed inflammation
-
Type B: a CD30-negative variant with histologic features similar to mycosis fungoides and distinguished from the latter on clinical grounds
-
Type C: a monotonous population of large CD30+ T cells with less background inflammation than type A
-
Type D: a CD8+, CD30+ variant
-
Type E: a CD30+, angioinvasive variant
-
Subcutaneous, Panniculitis-Like T-Cell Lymphoma (Fig. 18.64)

Subcutaneous, panniculitis-like T-cell lymphoma.
Clinical
-
♦
Subcutaneous nodules or plaques typically involving the lower extremities
-
♦
Frequent, severe constitutional symptoms
-
♦
Hepatosplenomegaly may be present
-
♦
Hemophagocytic syndromes are common
-
♦
Systemic dissemination is uncommon
-
♦
Often has an indolent clinical course
Microscopic
-
♦
A variably dense, polymorphous, panniculitis-like infiltrate is present with no or minimal dermal involvement
-
♦
The pleomorphic lymphocytes may be small, medium, or large T cells which characteristically “ring” around the adipocytes
-
♦
Lipophages, plasma cells, eosinophils, neutrophils, and, occasionally, lymphoid follicles may be present
-
♦
Necrosis, karyorrhexis, hemophagocytosis, and angiodestruction are common
Immunophenotype
-
♦
CD3+, CD8+, Tia-1+, porin+, α/β+, and CD56–
Genotype
-
♦
Clonal T-cell receptor, alpha/beta genotype
-
♦
EBV negative
Extranodal NK-/T-Cell Lymphoma, Nasal Type
General
-
♦
An aggressive form of NK or cytotoxic T-cell lymphoma characterized by cutaneous and/or nasal involvement
Clinical
-
♦
This form of NK-/T-cell lymphoma most frequently affects adults and is most common in East Asian and South American countries
-
♦
The trunk and extremities are most often involved by tumors, plaques, nodules, or ulcers
-
♦
There may be an associated hemophagocytic syndrome
-
♦
The prognosis is poor with survival rates typically less than a year
Microscopic
-
♦
A dense dermal and/or subcutaneous infiltrate is present with regions of angiocentricity and angiodestruction
-
♦
The tumor cells vary from small- to large-sized cells with hyperchromatic to vesicular nuclei
-
♦
A background mixed inflammatory infiltrate is common
Immunophenotype
-
♦
CD2+, surface CD3–, cytoplasmic CD3+, CD56+, TIA-1+, EBV+, and T-cell recepto r–
Primary Cutaneous Aggressive Epidermotropic CD8+ Cytotoxic T-Cell Lymphoma
Clinical
-
♦
An aggressive form of cutaneous lymphoma characterized by disseminated papules, nodules, or ulcers
-
♦
Systemic involvement may occur, and the overall survival is poor (mean survival of 32 months)
Microscopic
-
♦
A pleomorphic infiltrate of small- to medium-sized atypical lymphocytes is present with marked epidermotropism
-
♦
The atypical lymphocytes frequently invade adnexal structures, and angioinvasion may also be present
Immunophenotype
-
♦
CD3+, CD8+, TIA-1+, beta F1+, CD4–, CD7–, CD56–, and EBV–
Cutaneous Gamma/Delta T-Cell Lymphoma
Clinical
-
♦
An aggressive form of cutaneous lymphoma characterized by disseminated plaques, nodules, or ulcers typically involving the extremities and, frequently, the trunk
-
♦
Involvement of other sites (mucosa and other extranodal regions) is common, and a hemophagocytic syndrome may occur
Microscopic
-
♦
Epidermotropic, dermal, and subcutaneous infiltrative patterns occur and may coexist
-
♦
The individual lymphocytes are medium to large in size with pleomorphic nuclear features and a clumped chromatin pattern
-
♦
Individual cell necrosis and confluent necrosis may be prominent
-
♦
Angioinvasion and angiodestruction are frequent findings
Immunophenotype
-
♦
CD3+, CD2+, CD5–, CD4–, CD8-, and beta F1–
Genetics
-
♦
The T cells have a clonal rearrangement of the TCR gamma gene. EBV is typically negative
Pleomorphic Small/Medium-Sized Cutaneous T-Cell Lymphoma
Clinical
-
♦
A solitary nodule, plaque, or papule on the head and neck region is the most common presentation
-
♦
Rarely multiple cutaneous lesions may be present
-
♦
This entity has a good prognosis, particularly when a single lesion is present
Microscopic
-
♦
A dense dermal lymphocytic infiltrate with polymorphous features is evident
-
♦
Epidermotropism is generally minimal or absent
-
♦
The infiltrate frequently surrounds and may infiltrate adnexal structures, but no follicular mucinosis is evident. The bulk of the infiltrate is dermal based and not follicular
-
♦
The individual cells are small- to medium-sized lymphocytes that are frequently admixed with background histiocytes, reactive lymphocytes, eosinophils, and, occasionally, plasma cells
Immunophenotype
-
♦
CD3+, CD4+, CD8–, and CD30–
Genetics
-
♦
The TCR is clonally rearranged. Molecular studies are generally needed for diagnosis to exclude reactive etiologies (lymphoid hyperplasia, florid rosacea, etc .)
Primary Cutaneous Peripheral T-Cell Lymphoma, Unspecified
General
-
♦
A cutaneous T-cell lymphoma that does not meet the criteria of the previously defined cutaneous T-cell lymphomas
Clinical
-
♦
These tumors typically present with multiple tumors, nodules, or plaques without a site predilection
-
♦
The prognosis is generally poor with 5-year survival rates of less than 20%
Microscopic
-
♦
A diffuse, destructive dermal infiltrate is present without significant epidermotropism or folliculotropism
-
♦
The tumors are composed of at least 30% large lymphocytes, but sheets of large lymphocytes may be present
Immunophenotype
-
♦
CD3+, CD4+, CD30–, and CD56–
Blastic Plasmacytoid Dendritic Cell Neoplasm
General
-
♦
An aggressive neoplasm thought to be derived from a plasmacytoid dendritic cell precursor
Clinical
-
♦
Patients may present with solitary or generalized cutaneous involvement in the form of tumor nodules or plaques
-
♦
There is typically concurrent or subsequent involvement of the bone marrow, peripheral blood, and lymph nodes
Microscopic
-
♦
A diffuse dermal and/or subcutaneous infiltrate of medium-sized, blastic lymphocytes is present
-
♦
No significant angioinvasion or epidermotropism is evident
Immunophenotype
-
♦
CD4+, CD56+, CD123+, CD3−, CD8−, MPO−, TdT+/−, and CD68+/−
Leukemia Cutis (Fig. 18.65)

Leukemia cutis.
General
-
♦
All forms of leukemia may involve the skin during the course of their evolution
-
♦
Most often, this occurs in patients with a known diagnosis of leukemia
-
♦
However, cutaneous disease may be the first manifestation of a leukemic process in evolution
Clinical
-
♦
Macules, papules, nodules, tumors, plaques, and ulcers may all be manifestations of leukemia cutis
-
♦
Any cutaneous surface may be involved
-
♦
Gingival involvement is particularly characteristic of acute myelogenous leukemia of the monocytic type (AML, M5)
Microscopic
-
♦
The most common pattern of leukemic infiltration of the skin is the diffuse dermal, reticular, or splaying pattern where the neoplastic cells splay apart the dermal collagen fibers in a discohesive fashion
-
♦
Perivascular to angiocentric infiltrates are also seen frequently in chronic lymphocytic leukemia (CLL)
-
♦
In AML, nodular patterns of infiltration are also common
-
♦
The cytologic features of a particular leukemic infiltrate reflect their systemic cell of origin:
-
CLL: Small, monotonous lymphocytes
-
AML: Myeloblasts with or without eosinophilic myelocytes, differentiated monocytes, etc
-
CML (chronic myelogenous leukemia): A spectrum of granulocytic cells and myeloblasts
-
ALL (acute lymphoblastic leukemia): Medium-sized, fairly monotonous lymphoblasts
-
Immunophenotype
-
♦
CLL: CD20+, CD23+, CD5+, CD43+/−, and CD3–
-
♦
AML: CD3–, CD20–, CD43+, MPO+/−, CD68+/−, and CD117+/–
-
♦
CML: CD3–, CD20–, CD43+, and MPO+
-
♦
ALL: CD3 or CD20+, TdT+/−, and MPO –
Immunodermatology
Methods, Terminologies, and Techniques
Direct Immunofluorescence (DIF)
-
♦
A skin biopsy that has been snap frozen or placed in transport media (such as Michel media) is incubated with fluorescein-conjugated antibodies against immunoglobulin and complement
-
♦
Standard panel of conjugates includes IgG, IgA, IgM, C3, and fibrinogen
Indirect Immunofluorescence (IIF)
-
♦
The patient’s serum is incubated with normal human skin that has been split at the level of the lamina lucida using 1.0 M NaCl (salt-split skin)
-
♦
Fluorescein-conjugated antibodies to IgG are then added
-
♦
If circulating antibody to basement membrane zone is present, the conjugate will localize to the epidermal side, the dermal side, or both
-
♦
This pattern reflects the location of the immune deposits (eg., hemidesmosome or sublamina densa) and allows distinction between certain immunobullous diseases
-
♦
The titer of the circulating antibody is determined by incubating the patient’s serum with fluorescein-conjugated antibodies to IgG on an epithelial substrate, usually monkey esophagus
-
♦
Other substrates may be used in specific conditions, such as rat bladder epithelium for paraneoplastic pemphigus or guinea pig esophagus for Pemphigus foliaceus
-
♦
Progressively more dilute samples of patient serum are used (1:5, 1:10, 1:20, 1:40, 1:80, and so on)
-
♦
The dilution at which fluorescence can no longer be subjectively identified is the antibody titer
-
♦
Indirect immunofluorescence can also be performed using fluorescein-conjugated antibodies to IgA
-
♦
This is helpful for diseases involving IgA, such as linear IgA bullous dermatosis and dermatitis herpetiformis
Western Immunoblotting
-
♦
A more specific technique to identify the antigens that the patient’s antibodies are directed against
Elisa
-
♦
Enzyme-linked immunosorbent assays have recently been developed for a number of immunobullous diseases
-
♦
These allow rapid, sensitive, and specific identification of antibodies
Immunobullous Diseases
Patterns of Antibody Deposition
-
♦
Linear deposition along the basement membrane zone
-
♦
Deposition in intercellular spaces
-
♦
Granular deposition along the basement membrane zone
-
♦
Granular deposition in the dermal papillae
-
♦
Cytoid bodies and shaggy deposition along the basement membrane zone
-
♦
Thick linear deposition along the basement membrane zone and perivascular deposition
-
♦
Deposition on eosinophils and diffuse deposition on connective tissue
-
♦
Deposition in blood vessels
Linear Deposition along the Basement Membrane Zone
Bullous Pemphigoid (BP)
Clinical
-
♦
Most commonly occurs in the elderly but has been reported in children and neonates
-
♦
Clinical presentation characteristic for pruritic tense bullae (negative Nikolsky sign) that heal without scarring
-
♦
The primary lesion is often urticarial
-
♦
Brunsting–Perry pemphigoid is a clinical subtype with scarring
-
♦
Distribution is mainly flexural, lower extremities and trunk
-
♦
Mucous membrane lesions occur in 10–30%
Microscopic
-
♦
Typically shows subepidermal separation with inflammatory infiltrate of eosinophils and lymphocytes (Fig. 18.66)
Fig. 18.66. 
Bullous pemphigoid. Subepidermal separation with eosinophils and lymphocytes.
-
♦
Eosinophilic spongiosis may be present
-
♦
Neutrophils may also be seen but are not prominent
-
♦
Basal layer spongiosis without frank separation may be seen in early or perilesional biopsies

Electron Microscopy
-
♦
Separation occurs within the lamina lucida
Immunopathology
-
♦
DIF on a perilesional skin biopsy specimen shows linear deposition of antibody (IgG > IgA) and complement at the basement membrane zone (Fig. 18.67)
Fig. 18.67. 
Bullous pemphigoid. Linear deposition of IgG along with basement membrane zone.
-
♦
Eosinophils are often prominent
-
♦
IIF using salt-split human skin demonstrates localization of the antibody to the epidermal side of the split (Fig. 18.68)
Fig. 18.68. 
Bullous pemphigoid. Antibody localizes to the epidermal side of salt-split skin.
-
♦
A combined pattern (epidermal and dermal) is occasionally seen
-
♦
Indirect immunofluorescence detects circulating IgG basement membrane zone antibodies in 50–70% of patients
-
♦
The antibody titer is not predictably correlated with disease activity or prognosis
-
♦
Implicated Antigens
-
Most commonly detected antigen is a 230-kD hemidesmosomal cytoplasmic protein (BP antigen I)
-
The second most commonly detected is a 180-kD hemidesmosomal transmembrane protein (BP antigen II)
-


Cicatricial Pemphigoid
Clinical
-
♦
Characterized by inflammation and scarring of the mucosal membranes, most commonly the conjunctiva
-
♦
May also involve the oral and genital mucosa
-
♦
Primary oral lesion is often desquamative gingivitis
-
♦
Skin lesions are less common but can occur
-
♦
Ocular scarring may lead to symblepharon, decreased tear production, entropion, and blindness
Microscopic
-
♦
May see subepithelial separation but usually see nonspecific mucositis with inflammatory infiltrate of eosinophils, plasma cells, and lymphocytes
-
♦
Neutrophils may also be present but are not prominent
Electron Microscopy
-
♦
Separation occurs at the level of the lamina lucida
Immunopathology
-
♦
DIF pattern is identical to that seen in bullous pemphigoid
-
♦
There is linear deposition of IgG, IgA, and C3 along the basement membrane zone
-
♦
Eosinophils are often present in the lamina propria
-
♦
IIF usually does not detect circulating antibodies
-
♦
When antibodies are present, IIF using salt-split skin localizes the antibodies to the epidermal side in some cases and to the dermal side in others
Implicated Antigens
-
♦
Most commonly implicated antigens are the same as for bullous pemphigoid (230-kD and 180-kD hemidesmosomal proteins), corresponding to the epidermal pattern of binding on salt-split skin
-
♦
Some patients have antibodies to epiligrin (laminin 5), a component of the anchoring filaments
-
♦
This subset of patients has been associated with the dermal pattern of binding on salt-split skin
Herpes Gestationis (Pemphigoid Gestationis)
Clinical
-
♦
Occurs exclusively in women
-
♦
Characterized by pruritic tense bullae (negative Nikolsky sign) that heal without scarring
-
♦
Primary lesion is often urticarial
-
♦
May begin around the umbilicus
-
♦
Usually most prominent on the abdomen and flexural skin
-
♦
Mucosal lesions are very rare
-
♦
Most commonly occurs during the second or third trimester of pregnancy and resolves after delivery
-
♦
Postpartum flares can occur
-
♦
In subsequent pregnancies, the eruption occurs earlier and is more severe
-
♦
May also occur with hormonal medication or menses in susceptible women
-
♦
Has been reported with molar pregnancy and gestational malignancy
Epidemiology
-
♦
Increased frequency of HLA-B8, DR3, and DR4
Microscopic
-
♦
Usually identical to bullous pemphigoid
-
♦
Typically see subepidermal separation with inflammatory infiltrate of eosinophils, lymphocytes, and occasionally neutrophils
-
♦
Early or perilesional biopsies may not show frank separation
-
♦
Basal cell necrosis may be more prominent than in bullous pemphigoid
-
♦
Might see eosinophilic spongiosis and/or an inverted teardrop pattern of epidermal edema (Fig. 18.69)
Fig. 18.69. 
Herpes gestationis. Eosinophilic spongiosis and subepidermal separation with eosinophils.

Ele ctron Microscopy
-
♦
Separation occurs within the lamina lucida
Immunopathology
-
♦
DIF shows linear deposition of complement along the basement membrane zone (Fig. 18.70)
Fig. 18.70. 
Herpes gestationis. Linear deposition of complement along the basement membrane zone.
-
♦
Linear deposition of IgG may also be present but is less prominent than complement
-
♦
This pattern reflects the nature of the circulating antibody, referred to as “herpes gestationis factor” (HG factor)
-
♦
HG factor is an IgG antibody (usually IgG1) that avidly fixes complement
-
♦
It is often present in such low titers that DIF and IIF fail to identify it, but the complement it fixes can be detected
-
♦
IIF is usually negative
-
♦
Low titers of circulating IgG antibodies to basement membrane zone are identified in less than 20% of patients
-
♦
When present, salt-split skin localizes these antibodies to the epidermal side of the separation

Implicated Antigens
-
♦
The majority of patients have antibodies that are directed against the minor bullous pemphigoid antigen, BP antigen II (180-kD transmembrane hemidesmosomal protein)
-
♦
A smaller group of patients have antibodies directed against the major bullous pemphigoid antigen, BP antigen I (230-kD cytoplasmic hemidesmosomal protein )
Epidermolysis Bullosa Acquisita (EBA)
Clinical
-
♦
Adults are affected more commonly than children
-
♦
Racial differences are seen, with Blacks affected more frequently
-
♦
Three different clinical patterns are observed:
-
A mechanobullous eruption with noninflammatory blisters and increased skin fragility in an acral distribution that heals with scarring and milia. This is the most frequent presentation
-
An inflammatory (“bullous pemphigoid-like”) vesiculobullous eruption that heals without scarring or milia
-
Mucosal erosions with scarring (“cicatricial pemphigoid-like”)
-
All three types of lesions may be present; considerable overlap exists
-
Associated diseases include systemic lupus erythematosus, other diseases of autoimmunity (inflammatory bowel disease, Goodpasture syndrome, glomerulonephritis, rheumatoid arthritis, thyroiditis, diabetes), and malignancy (multiple myeloma, chronic lymphocytic leukemia)
-
Prognosis is generally poor
-
Epidemiology
-
♦
Increased incidence of HLA-DR2
Microscopic
-
♦
If a noninflamed mechanobullous lesion is biopsied, microscopic characteristic will show a subepidermal separation with minimal inflammation (Fig. 18.71)
Fig. 18.71. 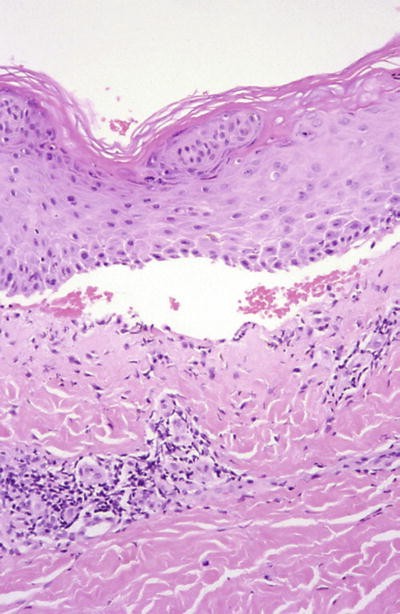
E pidermolysis bullosa acquisita. Subepidermal separation with minimal inflammation.
-
♦
If clinical lesion is inflamed, biopsy will have subepidermal separation with neutrophils, eosinophils, and lymphocytes along the basement membrane and in the upper dermis
-
Neutrophils tend to predominate over eosinophils
-
Basal layer spongios is without frank separation may be seen in early or perilesional biopsies
-

Electron Microscopy
-
♦
Separation usually occurs at the level of the lamina densa/sublamina densa
-
♦
Occasionally occurs in the lamina lucida
Immunopathology
-
♦
DIF has a pattern identical to bullous pemphigoid, with linear deposition of IgG and complement along the basement membrane zone
-
♦
IgA, IgM, and fibrinogen are less commonly present. Indirect immunofluorescence is necessary to distinguish EBA from pemphigoid
-
♦
IIF on salt-split skin shows a dermal pattern of binding (Fig. 18.72)
Fig. 18.72. 
Epid ermolysis bullosa acquisita. Antibody localizes to the dermal side of salt-split skin.
-
♦
Circulating IgG antibody to basement membrane zone is commonly present

Implicated Antigens
-
♦
The majority of patients have antibodies that are directed against the 290-kD noncollagenous domain (NC-1) on the alpha chain of collagen type VII (anchoring fibrils)
-
♦
Rarely, antibodies to a 145-kD noncollagenous globular domain on the alpha chain of collagen type VII have been identified
Bullous Systemic Lupus Erythematosus (BSLE)
Clinical
-
♦
Patients with systemic lupus erythematosus may also develop autoimmunity to basement membrane zone
-
♦
These patients present with a blistering eruption, especially on sun-exposed skin
-
♦
They will also have other signs and symptoms of systemic lupus
-
♦
They do not usually have other cutaneous manifestations of lupus
-
♦
Patients with systemic lupus can also have blistering for other reasons, such as concurrent primary bullous disease or severe medication or photosensitivity reaction
Epidemiology
-
♦
Increased incidence of HLA-DR2
Microscopic
-
♦
Typically shows subepidermal separation with inflammatory infiltrate of neutrophils and lymphocytes in the dermal papillae (as in dermatitis herpetiformis) and along the basement membrane zone (Fig. 18.73)
Fig. 18.73. 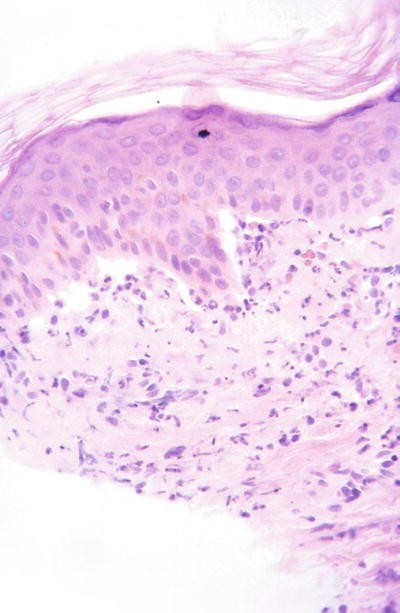
Bullous systemic lupus erythematosus . Subepidermal separation with neutrophils and lymphocytes in dermal papillae and along the basement membrane zone.
-
♦
N eutrophils predominate

Immunoelectron Microscopy
-
♦
IgG and complement are deposited in the sublamina densa
-
♦
Separation occurs at the level of the sublamina densa
Immunopathology
-
♦
DIF shows either linear (Fig. 18.74) or granular to fibrillar deposition of IgG and complement along the basement membrane zone (Fig. 18.75)
Fig. 18.74. 
Bullous systemic lupus erythematosus . Linear deposition of IgG along the basement membrane zone.
Fig. 18.75. 
Bullous systemic lupus erythematosus . Linear to granular deposition of IgG along the basement membrane zone and epidermal ANA.
-
♦
IgM and IgA are occasionally present
-
♦
IIF using salt-split skin demonstrates immune deposits on the dermal side of the separation
-
♦
Circulating IgG to basement membrane zone is present in some but not all patients
-
♦
Antinuclear antibodies are often seen


Implicated Antigens
-
♦
As in EBA, the majority of patients have antibodies that are directed against the 290-kD noncollagenous domain (NC-1) on the alpha chain of collagen type VII (anchoring fibrils)
-
♦
Rarely, antibodies to a 145-kD noncollagenous globular domain on the alpha chain of collagen type VII have been identified
-
♦
Antibody specificity is the same as that seen in epidermolysis bullosa acquisita
-
♦
In some cases, antibodies to type VII collagen cannot be detected
-
♦
Some authors propose two subtypes, BSLE 1 and BSLE 2, based on the presence (BSLE 1) or absence (BSLE 2) of antibodies to type VII collagen
Linear IgA Bullous Dermatosis ( Chronic Bullous Disease of Childhood)
Clinical
-
♦
Occurs in adults and children, probably more common in children and in women
-
♦
Clinically heterogeneous
-
♦
Clinical exam shows a vesiculobullous eruption on normal or erythematous skin
-
♦
May have a “cluster-of-jewels” appearance
-
♦
Commonly occurs on the trunk and flexures in adults and on the lower abdomen, groin, and periorificial in children
-
♦
Oral lesions occur in about 70%
-
♦
Other mucosal surfaces, including conjunctivae, may be involved
-
♦
Disease associations include:
-
Medications (captopril, vancomycin, lithium), gastrointestinal diseases (inflammatory bowel disease, gluten-sensitive enteropathy), malignancy (hematogenous, carcinoma, melanoma), various infections, and other diseases of autoimmunity
-
-
♦
Prognosis is generally good
Microscopic
-
♦
Usually shows subepidermal separation with inflammatory infiltrate of neutrophils, eosinophils, and lymphocytes (Fig. 18.76)
Fig. 18.76. 
Linear IgA bullous dermatosis . Subepidermal separation with neutrophils greater in number than lymphocytes and eosinophils.
-
♦
Neutrophils predominate over eosinophils, especially in early lesions
-
♦
May see neutrophilic microabscesses in dermal papillae, similar to dermatitis herpetiformis

Immunoelectron Microscopy
-
♦
Mixed findings occur
-
♦
In some cases, there is IgA deposition in the lamina lucida (beneath the hemidesmosomes)
-
♦
In other cases, IgA is found in the sublamina densa, in association with anchoring fibrils
-
♦
IgA may also be found deposited in both locations
Immunopathology
-
♦
DIF shows linear deposition of IgA along the basement membrane zone (Fig. 18.77)
Fig. 18.77. 
Linear IgA bullous dermatosis . Linear deposition of IgA along the basement membrane zone.
-
♦
IgG, IgM, C3, and fibrinogen may be present but are of lower intensity than IgA
-
♦
IIF on salt-split skin may show an epidermal pattern (most common), a dermal pattern, or both
-
♦
Circulating IgA antibodies (usually IgA1) to basement membrane zone can be identified in 60–70%

Implicated Antigens
-
♦
Several different antigens have been identified
-
♦
Most common is a 97-kD component of the anchoring filaments termed LAD-1
-
♦
Immune deposition here corresponds to an epidermal pattern of binding on salt-split skin
-
♦
Antibodies to a 290-kD component of collagen type VII have also been identified
-
♦
Epitope is different than that of EBA
-
♦
Immune deposition here corresponds to a dermal pattern of binding on salt-split skin
-
♦
Other antibodies have also been identified
-
♦
LABD is likely a heterogeneous group of diseases, with a variety of autoantibodies
Deposition in Intercellular Spaces
Pemphigus
-
♦
A group of diseases all characterized clinically by cutaneous and/or mucosal blistering or erosions and histologically by acantholysis
-
♦
Immunopathology
-
Autoantibodies to epithelial cell surfaces giving an intercellular space pattern of antibody deposition (ICS pattern)
-
Variant s
-
♦
Pemphigus vulgaris
-
♦
Pemphigus vegetans
-
♦
Drug-induced pemphigus
-
♦
Pemphigus foliaceus
-
♦
Pemphigus erythematosus
-
♦
IgA pemphigus
-
♦
Paraneoplastic pemphigus
Pemphigus Vulgaris
Clinical
-
♦
Most commonly occurs in adults (mean age 50–60) but has been reported in children
-
♦
Increased incidence with Ashkenazi Jewish or Mediterranean heritage, but no race is exempt
-
♦
Oral lesions (erosions) usually develop first
-
♦
Disease may be confined to the oral cavity
-
♦
Skin lesions are typically flaccid bullae that rupture easily leaving erosions and crusts
-
♦
Gentle pressure on the blister roof will cause extension of the bulla (positive Nikolsky sign) due to the fragility of the surrounding skin
-
♦
Any stratified squamous epithelial surface may be involved, including other mucosal surfaces
-
♦
Pemphigus vegetans is a clinical subtype characterized by chronic lesions that develop into hyperkeratotic plaques, often in intertriginous sites
-
♦
Most commonly implicated medications in drug-induced pemphigus are penicillamine and captopril
Microscopic
-
♦
Characteristic for suprabasilar separation with acantholysis (Fig. 18.78)
Fig. 18.78. 
Pemphigus vulgaris. Suprabasilar separation with acantholysis.
-
♦
Basal layer remains attached, with separation at the lateral and apical margins (“tombstoning”) (Fig. 18.79)
Fig. 18.79. 
Pemphigus vulgaris. “Tomb stoning” of basal layer.
-
♦
Acantholysis extending down hair follicles helps to distinguish pemphigus from other causes of acantholysis such as Hailey–Hailey and Darier disease
-
♦
Eosinophilic spongiosis may be present
-
♦
There is a mixed inflammatory infiltrate in the dermis
-
♦
Pemphigus vegetans has more acanthosis and eosinophilic spongiosis with relatively subtle suprabasilar separation and acantholysis


Electron Microscopy
-
♦
First sign is loss of attachment of cell membrane between adjacent keratinocytes, at the level of the desmosome
-
♦
Widening of intercellular spaces follows, as desmosomes pull apart
-
♦
Intracellular keratin filaments begin to show perinuclear clustering, and the acantholytic cells then “round up” and float free
Immunopathology
-
♦
DIF shows IgG and C3 bound to the keratinocyte cell surface in an ICS pattern; also referred to as intercellular substance (Fig. 18.80)
Fig. 18.80. 
Pemphigus vulgaris . IgG bound to keratinocyte cell surface in an ICS pattern.
-
♦
May be seen throughout the thickness of the epidermis or only in the deeper levels
-
♦
In active disease, IIF is nearly always positive for circulating IgG antibodies to ICS (Fig. 18.81)
Fig. 18.81. 
Pemphigus vulgaris . Circulating IgG to ICS on monkey esophagus.
-
♦
False negatives are more likely in drug-induced and early disease
-
♦
Antibody titer correlates fairly well with disease activity
-
♦
False-positive “pemphigus-like” antibodies are not uncommon and can be seen with medications (penicillin), infections (dermatophytes), and full-thickness epidermal disruption (burns)
-
♦
The titer of false-positive antibody is usually low (less than 1:80)


Implicated Antigens
-
♦
Autoantibodies (IgG4 > IgG1 and IgG3) are directed against desmoglein 3, a 130-kD transmembrane glycoprotein located in desmosomes
-
♦
It exists in a molecular complex with plakoglobin, an 85-kD intracellular protein
Pemphigus Foliaceus
Clinical
-
♦
Characterized by superficial erosions and crusts, flaccid vesicles, or bullae may be present
-
♦
Usually begins on the head/neck (seborrheic distribution) and spreads acrally
-
♦
Mucosal lesions are rare
-
♦
May be exacerbated by sunlight
-
♦
Clinical variants include a sporadic form, a drug-induced form, and an endemic form (fogo selvagem)
-
♦
Fogo selvagem is seen in agricultural and poverty-stricken regions of Brazil and South America
-
♦
Familial cases are frequently seen
-
♦
Peak incidence in the second and third decade
-
♦
The black fly (Simulian pruinosum) has been epidemiologically implicated as a vector
-
♦
Sporadic form occurs in elderly patients with no family history
-
♦
No environmental factors have been implicated
-
♦
Drug-induced form most commonly linked to “thiol” drugs (penicillamine and captopril) but has also been seen with “masked thiols” (penicillins and cephalosporins) and nonthiols (enalapril)
-
♦
Other associations include myasthenia gravis and thymoma (benign and malignant)
Microscopic
-
♦
As in pemphigus vulgaris but more superficially located
-
♦
A cantholysis occurs in a subcorneal or intraepidermal location (Fig. 18.82)
Fig. 18.82. 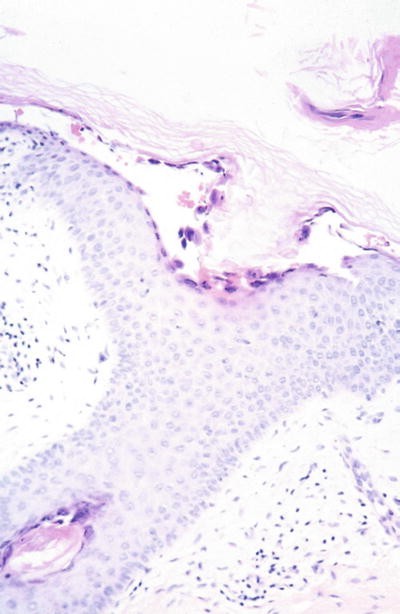
Pe mphigus foliaceus. Subcorneal acantholysis.

Electron Microscopy
-
♦
Acantholysis affects all layers, including the basal layer
Immunopathology
-
♦
DIF and IIF have findings similar or identical to those seen in pemphigus vulgaris (Fig. 18.83)
Fig. 18.83. 
Pemphigu s foliaceus. IgG bound to keratinocyte cell surface in an ICS pattern.
-
♦
DIF cannot reliably distinguish pemphigus vulgaris from pemphigus foliaceus
-
♦
In active disease, IIF is nearly always positive for circulating IgG antibodies to ICS
-
♦
Antibody titer correlates fairly well with disease activity
-
♦
Guinea pig esophagus appears to be better than monkey esophagus as a substrate for the detection of antibodies

Implicated Antigens
-
♦
Autoantibodies are directed against desmoglein 1, a 160-kD transmembrane glycoprotein located in desmosomes
-
♦
Like desmoglein 3 (antigen in pemphigus vulgaris), desmoglein 1 exists in a molecular complex with plakoglobin
Pemphigus Erythematosus
Clinical
-
♦
A rare disease characterized by facial lesions with features of both lupus erythematosus and pemphigus foliaceus (or seborrheic dermatitis) and lesions on the trunk more suggestive of pemphigus (flaccid bullae, erosions, and crusts)
-
♦
Usually photodistributed
-
♦
Mucosal lesions are rare
-
♦
May occur in any age; mean onset 40–60 years
-
♦
Clinical signs of lupus may be present but usually are not
-
♦
When present, lupus is usually mild or localized only
-
♦
Antinuclear antibodies are present in 30–60%
-
♦
Most commonly associated medications are penicillamine and captopril
-
♦
Various autoimmune diseases (myasthenia gravis) and malignancies (bronchogenic carcinoma) have also been associated
Microscopic
-
♦
Superficial acantholysis (similar to pemphigus foliaceus) is the main feature (Fig. 18.84)
Fig. 18.84. 
Pemphigus erythematosus . Subcorneal acantholysis.
-
♦
A subcorneal separation or pustule may be present
-
♦
Lichenoid dermatitis may be seen, but changes characteristic of lupus are not usually found

Electron Microscopy
-
♦
De monstrates findings similar to early pemphigus
-
♦
Most marked changes occur at the level of the stratum granulosum and upper stratum spinosum
Immunopathology
-
♦
DIF characterized by the combination of a typical ICS pattern with IgG and/or C3 (Fig. 18.85), as well as granular to linear deposition of IgM along the basement membrane zone (Fig. 18.86)
Fig. 18.85. 
Pemphigus erythematosu s. IgG bound to keratinocyte cell surface in an ICS pattern.
Fig. 18.86. 
Pemphigus erythematosus . Granular deposition of IgM along the basement membrane zone and cytoids.
-
♦
A lupus band is usually not present
-
♦
As in pemphigus vulgaris and pemphigus foliaceus, IIF is usually positive for circulating antibodies against ICS


Implicated Antigens
-
♦
Unknow n
IgA Pemphigus
-
♦
Numerous synonyms: intraepidermal neutrophilic IgA dermatosis, atypical neutrophilic dermatosis, intercellular IgA vesiculopustular dermatosis, and IgA pemphigus foliaceus
Clinical
-
♦
A rare disease, only reported in Caucasians
-
♦
Has been reported in children
-
♦
Clinical lesions include flaccid vesicles and pustules, sometimes in an annular or circinate pattern
-
♦
Distribution is often central
-
♦
Mucosal lesions do not occur
-
♦
The clinical course is fairly mild
-
♦
Two subtypes are IgA pemphigus of the subcorneal pustular dermatosis type (SPD) and IgA pemphigus of the intraepidermal neutrophilic type (IEN)
Microscopic
-
♦
SP D type has subcorneal separation with neutrophils (Fig. 18.87)
Fig. 18.87. 
IgA pemphigus . Subcorneal separation with neutrophils.
-
♦
IEN type has an intraepidermal cleft with neutrophils (slightly deeper than the SPD type) (Fig. 18.88)
Fig. 18.88. 
IgA pemphigus . Subcorneal separation with intraepidermal neutrophils.
-
♦
Suprabasilar separation may be seen
-
♦
In both types, acantholysis is sparse
-
♦
Neutrophilic microabscesses, as seen in dermatitis herpetiformis, have been reported


Immunopathology
-
♦
DIF is characterized by the deposition of IgA in an ICS pattern (Fig. 18.89)
Fig. 18.89. 
IgA pemphigus. IgA bound to keratinocyte cell surface in an ICS pattern.
-
♦
In general, deposition of C3 and other immunoglobulins does not occur
-
♦
Circulating IgA against ICS present in less than half of the reported cases
-
♦
Circulating anti-ICS IgG (lower titer than anti-ICS IgA) has been rarely reported

Implicated Antigen(s)
-
♦
Most likely a heterogeneous group of diseases with antibodies directed against several different antigens
-
♦
Most strongly implicated antigen is desmocollin 1, a 115-kD protein found on the extracellular surface of the desmosome, which has been linked to the SPD type
-
♦
A 120-kD protein has been linked to the IEN type
-
♦
Other antigens, including some linked to pemphigus vulgaris, have also been associated
Paraneoplastic Pemphigus
Clinical
-
♦
Association between pemphigus and malignancy has long been recognized
-
♦
Described as a distinct entity in 1
-
♦
More common in older adults but has been reported in children
-
♦
Malignancy usually presents first
-
♦
Prognosis is very poor; both malignancy and pemphigus are usually treatment resistant
-
♦
Hematopoeitic malignancies (CLL, Castleman tumor, Waldenstrom macroglobulinemia, and non-Hodgkin lymphoma) have been most commonly associated, but poorly differentiated sarcomas, adenocarcinoma, and even benign thymoma have been linked
-
♦
Clinically characterized by severe, painful, and recalcitrant erosions of mucosal surfaces
-
♦
Oral mucosa most commonly involved
-
♦
May also affect conjunctivae, genital mucosa, and respiratory epithelium
-
♦
Cutaneous eruption is polymorphous
-
♦
Initially may have a pruritic papulosquamous eruption
-
♦
Blisters may later develop, including on palms and soles (reminiscent of erythema multiforme)
-
♦
Chronic lichenoid changes have also been described
Microscopic
-
♦
In about half of the cases, a combination of histologic features is seen, including:
-
Suprabasilar separation and acantholysis (Fig. 18.90)
Fig. 18.90. 
Paraneoplastic pemphigus . Mucosa with suprabasilar.
-
Lichenoid changes (vacuolar degeneration, a band-like infiltrate, and exocytosis of inflammatory cells) (Fig. 18.91)
Fig. 18.91. 
Paraneoplastic pemphigus . Another zone with lichenoid mucositis.
-
Dyskeratotic and necrotic keratinocytes (as seen in erythema multiforme)
-
Many cases will not have all of these features
-
Eosinophilic infiltration is not typically seen
-
Atypia of infiltrating cells also not seen
-
-
-


Immunoelectron Microscopy
-
♦
Immune complexes present in a variety of locations, including the hemidesmosomes, desmosomal plaques, keratinocyte plasma membrane, and extracellular regions of desmosomes
Immunopathology
-
♦
DIF has the characteristic combination of an ICS pattern with IgG +/− C3 and linear to granular deposition of C3 +/− IgG along the basement membrane zone (Fig. 18.92)
Fig. 18.92. 
Paraneoplastic pemphigu s. Complement bound to cell surface in an ICS pattern and in a linear to granular pattern along the basement membrane zone.
-
♦
Other lichenoid features, such as cytoids (dyskeratotic keratinocytes) and shaggy deposition of fibrinogen, are variably present
-
♦
Circulating IgG against epithelial cell surfaces has been detected on many substrates, including stratified squamous (as in other forms of pemphigus) as well as transitional and columnar epithelium
-
♦
Best sensitivity/specificity profile in urinary bladder epithelium (rat and mouse)

Implicated Antigens
-
♦
Autoantibodies are directed against a complex of four antigens
-
♦
Most strongly and consistently detected are antibodies a gainst:
-
A 190-kD protein (identity unknown)
-
A 210-kD protein (desmoplakin 2)
-
-
♦
Also detected are antibodies against:
-
A 230-kD hemidesmosomal protein (bullous pemphigoid antigen 1)
-
A 250-kD protein (desmoplakin 1 )
-
Granular Deposition along the Basement Membrane Zone: Lupus Erythematosus
-
♦
Lupus Variants
-
Discoid lupus erythematosus
-
Localized
-
Disseminated
-
Subacute cutaneous lupus erythematosus
-
Systemic lupus erythematosus
-
Bullous systemic lupus erythematosus
-
Discoid Lupus Erythematosus (DLE)
Clinical
-
♦
DLE is a cutaneous disease, usually not accompanied by systemic signs of lupus
-
♦
It is photodistributed and thus typically affects the face, head and neck, chest, and upper back
-
♦
Disease may be localized or widespread (disseminated)
-
♦
More common in young women
-
♦
Increased incidence in Blacks
-
♦
Clinical lesions are patches, papules, and plaques
-
♦
Characteristic features include telangiectasia, atrophy, scarring, and follicular plugging
-
♦
Scalp involvement results in scarring alopecia
-
♦
Response to treatment (photoprotection, topical steroids, and systemic antimalarials) is variable but tends to be good
Microscopic
-
♦
Epidermal atrophy, hyperkeratosis, and thickening of the basement membrane accompany basal cell liquefactive degeneration, pigment incontinence, and a variable degree of lichenoid inflammation (Fig. 18.93)
Fig. 18.93. 
Discoid lupus erythematosus . Interface dermatitis.
-
♦
Periadnexal and perivascular infiltrate is present in the upper and mid dermis
-
♦
Follicular infundibular plugging is often seen
-
♦
Dermal mucinosis often present

Immunopathology
-
♦
On involved or sun-exposed skin, DIF shows granular deposition along the basement membrane zone with IgM, sometimes referred to as a lupus band (Fig. 18.94)
Fig. 18.94. 
Discoid lupus erythematosu s. Granular deposition of IgM along the basement membrane zone and cytoids.
-
♦
The strict definition of a lupus band reserves the use of the term for the presence of granular IgM along the basement membrane zone in uninvolved and non-sun-exposed skin, as seen in systemic LE (Fig. 18.95)
Fig. 18.95. 
Discoid lupus erythemat osus. The “lupus band” of systemic lupus erythematosus is granular deposition of IgM along the basement membrane zone in non-sun-exposed skin.
-
♦
Granular deposition with other conjugates, including C3, IgA, and IgG, is usually present, which helps to confirm the diagnosis
-
♦
Fibrinogen often forms a shaggy band along the basement membrane zone, typical for a lichenoid reaction
-
♦
DIF may be negative (or only have minimal granular IgM deposition) in a biopsy from an old “burned-out” lesion or from the atrophic center of a lesion, making site selection for biopsy critical for the diagnosis
-
♦
DIF is negative in uninvolved and non-sun-exposed skin
-
♦
May also see epidermal antinuclear antibodies, most commonly with IgG
-
♦
Indirect immunofluorescence is negative


Subacute Cutaneous Lupus Erythematosus (SCLE)
Clinical
-
♦
SCLE is a photodistributed, symmetric, and often widespread eruption, most commonly seen in females
-
♦
Mean age of presentation is around 40, which is slightly older than other types of LE
-
♦
There is a strong association with the presence of anti-Ro (SS-A) antibodies and Sjögren syndrome
-
♦
Systemic lupus erythematosus is present in 50%
-
♦
ANA is positive in about half; other antibodies including anti-La (SS-B), antithyroid, and anticardiolipin are variably present
-
♦
Lesions are nonscarring and nonindurated
-
♦
May see annular/polycyclic plaques with central clearing or papulosquamous lesions (scaly pink-red papules)
-
♦
Lesions LACK atrophy, scarring, and follicular plugging
-
♦
Clinical course is usually relatively benign, but a subset of patients may go on to develop severe systemic disease
Epidemiology
-
♦
Increased incidence of HLA-DR3 and HLA-DR2 as well as inherited homozygous C2 and C4 deficiency
Microscopic (Fig. 18.96)
-
♦
Many features are similar to changes seen in discoid LE, but histologic distinction between the two can sometimes be made
Fig. 18.96. 
Subacute cutaneous lupus erythematosus. Interface dermatitis.
-
♦
In general, SCLE has less:
-
Hyperkeratosis
-
Basement membrane thickening
-
Follicular involvement
-
Follicular plugging
-
Dermal infiltrate, and it is more superficially located
-
-
♦
SCLE tends to have more:
-
Epidermal atrophy
-
Liquefactive degeneration
-
Cytoid bodies
-
Pigment incontinence
-
Satellite cell necrosis
-
Lymphocyte exocytosis
-
-
♦
Exceptions to these rules are frequent, and in many cases, SCLE cannot be histologically distinguished from other types of LE

Immunopathology
-
♦
DIF has findings that are distinct from other types of LE
-
♦
There is a discrete “particulate” or speckled pattern of epidermal deposition with IgG that occurs predominantly in the basal layer and is associated with the presence of anti-Ro (SS-A) antibodies (Fig. 18.97)
Fig. 18.97. 
Subacute c utaneous lupus erythematosus. Speckled or “particulate” pattern of intercellular epidermal IgG deposition.
-
♦
P articulate dermal–epidermal deposition can be seen in other types of lupus and is not suggestive of SCLE
-
♦
Other DIF changes typical for LE (granular deposition along the basement membrane zone with IgM and other conjugates) may be present but often are not
-
♦
May also see epidermal antinuclear antibodies, most commonly with IgG
-
♦
Circulating antinuclear antibodies are detected in 50%
-
♦
Indirect immunofluorescence is usually otherwise negative

Bullous Systemic Lupus Erythematosus
-
♦
DIF is characterized by linear or granular deposition along the basement membrane zone
-
♦
See description under the section “Linear Deposition along the Basement Membrane Zone”
Systemic Lupus Erythematosus
Clinical
-
♦
SLE is an autoimmune disease with a wide variety of possible systemic manifestations
-
♦
Over 75% of patients will have some form of cutaneous involvement, including malar erythema, photosensitivity, oral involvement (cheilitis, ulcers, petechiae, and gingivitis), or discoid lesions
-
♦
Nonspecific lesions may be seen in SLE but may also be seen in a variety of other conditions or in normal patients
-
♦
These include vasculitis and vasculopathy, Raynaud phenomenon, livedo reticularis, perniosis, urticaria and urticarial vasculitis, nonscarring alopecia, and rheumatoid nodules
-
♦
Most common in women of childbearing age (F:M 9:1) and dark-skinned patients (Black, Hispanic, and so on)
-
♦
Increased incidence of complement deficiency, both due to excessive consumption by immune complexes and an increased incidence of inherited deficiencies of complement components (most commonly homozygous C2 deficiency)
-
♦
Mean age of onset is in the 30s
-
♦
May be induced by medication
-
♦
Clinical course is variable; may be mild and controlled with medication or severe and recalcitrant
-
♦
Most commonly affected systems include the joints (90%), kidneys (50%), lungs (40%), and the central nervous system (30%), but a wide variety of other organs may also be affected
-
♦
Constitutional signs are frequent and include fatigue, fever, weight loss, and malaise
-
♦
Most common cause of mortality is due to renal involvement
Microscopic
-
♦
Microscopic characteristics depend on the type of lesion biopsied
-
♦
No changes diagnostic for systemic LE exist
-
♦
Discoid lesions show changes as described for discoid LE
-
♦
Vasculitic lesions clinically associated with lupus anticoagulant syndrome show thrombotic microangiopathy, indistinguishable from other types of thrombotic microangiopathy (such as cryoglobulin-associated microangiopathy)
-
♦
Biopsy of malar erythema is nonspecific, with telangiectasia and rarely liquefactive degeneration or interface dermatitis
Immunopathology
-
♦
As discussed above, the strict definition of a positive lupus band test is the presence of granular deposition of IgM (and other conjugates) along the basement membrane zone in a biopsy from non-sun-exposed and uninvolved skin (Fig. 18.95)
-
♦
The presence of a lupus band is correlated with a higher incidence of systemic disease
-
♦
Granular deposition with other conjugates (IgG, IgA, and C3) is usually seen
-
♦
Circulating antinuclear antibodies may be detected on indirect immunofluorescence, but IIF is otherwise negative
Granular Deposition in the Dermal Papillae
Dermatitis Herpetiformis (DH)
Clinical
-
♦
DH is a chronic, intensely pruritic eruption with usual onset in the second to fourth decade, though it may occur at any age
-
♦
Primary lesions are pruritic urticarial papules that develop into small tense vesicles
-
♦
Due to the intense pruritus of the lesion, an excoriation is usually all that remains at the time of exam
-
♦
Most commonly affects extensor surfaces, particularly on pressure points, including the extensor surfaces of the forearms (elbows), knees, back, buttocks, and sacrum
-
♦
Associated with gluten-sensitive enteropathy which is clinically significant in 10% or less but histologically detectable (by villous atrophy and increased lymphocytic infiltrate) in 60–70% of patients
-
♦
Cutaneous disease and small bowel disease both respond to gluten-free diet
-
♦
Also clinically characterized by a rapid (within 24–48 h) response to dapsone
-
♦
DH i s also associated with an increased incidence of GI lymphoma and other malignancies
-
♦
Other organs with associated conditions include the thyroid (hyper- and hypothyroidism, thyroid nodules, and malignancy) and stomach (atrophy and hypochlorhydria)
-
♦
A variety of other autoimmune diseases have also been associated (Sjögren syndrome, insulin-dependent diabetes, rheumatoid arthritis, myasthenia gravis, and SLE, among others)
Epidemiology
-
♦
Increased frequency of HLA haplotypes B8, A1, DR3, and DQw2
Microscopic
-
♦
Early lesions show neutrophils along the basement membrane zone and in the dermal papillae, accompanied by fibrin deposition, leukocytoclasis, and rare eosinophils
-
♦
Clefts appear at the sites of neutrophil accumulation, termed papillary microabscesses (Fig. 18.98)
Fig. 18.98. 
Dermatitis herpetiformis. Papillary microabscesses.
-
♦
Perivascular lymphohistiocytic infiltrate is often present in the upper and middle dermis
-
♦
As vesicles or bullae develop, findings become nonspecific (subepidermal separation with neutrophils and eosinophils)

Immunopathology
-
♦
DIF characteristically has granular deposition of IgA in the dermal papillae and along the basement membrane zone (Fig. 18.99)
Fig. 18.99. 
Dermatitis herpetiformis . Granular deposition of IgA in dermal papillae and along basement membrane zone.
-
♦
Granularity is most pronounced in the dermal papillae
-
♦
Granular deposition with other conjugates (C3, IgG, and IgM) is rarely present but has been reported
-
♦
These changes are found in perilesional (within 3–5 mm) normal-appearing skin
-
♦
Several a ntibodies can be produced by patients with dermatitis herpetiformis and/or gluten-sensitive enteropathy, including IgG and/or IgA antiendomysial antibodies, antigliadin antibodies, and antireticulin antibodies
-
♦
The patient’s titer of IgA antiendomysial antibody, detected using monkey esophagus substrate, correlates with disease activity as well as patient’s compliance with the gluten-free diet

Implicated Antigens
-
♦
Unknow n
Clumped Cytoid Bodies and Shaggy Deposition of Fibrinogen along the Basement Membrane Zone
Lichenoid Tissue Reaction
-
♦
Cytoid bodies are round, homogeneously fluorescent cells that appear scattered as single cells or clumped in groups along the basement membrane zone
-
♦
They can also be seen in the epidermis (erythema multiforme) or upper dermis
-
♦
They are thought to represent necrotic keratinocytes and/or fragments of basement membrane
-
♦
Scattered cytoids can be seen nonspecifically in many conditions
-
♦
Shaggy deposition of fibrinogen along the basement membrane zone gives a pattern that has been likened to “dripping paint”
-
♦
While neither of these two findings is specific, the combination of clumped cytoids and shaggy deposition of fibrinogen is seen in lichenoid tissue reactions
-
♦
The diagnosis in each of these entities is dependent on the appropriate histopathology being present
Variants
-
♦
Lichen planus
-
♦
Lupus erythematosus
-
♦
Dermatomyositis
-
♦
Erythema multiforme
-
♦
Paraneoplastic pemphigus
-
♦
Lichenoid dermatitis
-
♦
Lichenoid drug reaction
-
♦
Graft versus host disease
-
♦
Other dermato ses
Lichen Planus
Immunopathology
-
♦
The “classic” lichenoid tissue reaction is often seen, with clumped cytoid bodies along the basement membrane zone and shaggy deposition of fibrinogen along the basement membrane zone (Fig. 18.100)
Fig. 18.100. 
Lichen planus. Shaggy deposition of fibrinogen and clumped cytoids along the basement membrane zone.
-
♦
Mucosal lesions are less likely to have cytoid bodies; shaggy fibrinogen may be the only finding present
-
♦
Yeast (Candida) can sometimes be found in mucosal lesions
-
♦
Although clumped cytoids are quite characteristic of LP, LP cannot be diagnosed on immunopathology alone. Microscopic characteristics consistent with LP must also be present to make the diagnosis

Lupus Erythematosus
-
♦
See section above
Immunopathology
-
♦
The typical features seen in lupus erythematosus are listed above. In addition, lupus may also demonstrate lichenoid features on immunopathology, often in combination with typical granularity along the basement membrane zone
-
♦
Immunofluorescence of aged or “burned-out” lesions may only have lichenoid changes
Dermatomyositis
Immunopathology
-
♦
Although granularity along the basement membrane zone similar to that seen in lupus erythematosus (the lupus band) has been reported, immunofluorescence usually does not demonstrate these changes
-
♦
A lichenoid tissue reaction and nonspecific discontinuous granularity along the basement membrane zone are more commonly seen
-
♦
Subepidermal fibrin deposition may also be seen
Erythema Multiforme
Immunopathology
-
♦
Erythema multiforme is characterized by epidermal cytoid bodies and weak perivascular deposition of IgM in the superficial dermis
-
♦
Shaggy deposition of fibrinogen and cytoids in the dermis and at the dermal–epidermal junction may also be seen
-
♦
Granular deposition of IgM, C3, and fibrinogen along the dermoepidermal junction is occasionally present
Paraneoplastic Pemphigus
-
♦
See section above
Immunopathology
-
♦
In addition to the characteristic features described above, clumped cytoids and shaggy deposition of fibrinogen along the basement membrane zone can also be seen
Lichenoid Dermatitis
Immunopathology
-
♦
Dermatitis due to any number of causes may also demonstrate a lichenoid tissue reaction
-
♦
This pattern is more likely to be seen in chronic dermatitis
Lichenoid Drug Reaction
Immunopathology
-
♦
In addition to lichenoid changes, drug reactions will also have eosinophils in the superficial and middle dermis
Graft Versus Host Disease
Immunopathology
-
♦
Lichenoid features can occasionally be seen in chronic graft versus host disease
-
♦
Epidermal cytoids may also be observed
-
♦
Granular deposition of IgM along the basement membrane zone is observed in about 40% of patients with acute disease and around 85% of patients with chronic disease
-
♦
In addition, IgM and C3 can sometimes be found within dermal vessel walls
Weak Thick Linear Deposition along the Basement Membrane Zone and Perivascular Deposition
Porphyrias
-
♦
The porphyrias are a group of inherited or acquired diseases that result from deficiency in the activities of enzymes of the heme biosynthetic pathway
-
♦
The characteristic clinical appearance of each of the subtypes results from the accumulation of intermediaries or their byproducts
-
♦
While the clinical appearance, course, and prognosis of the porphyrias with cutaneous manifestations vary from type to type, the microscopic characteristics and immunofluorescence are the same or very similar. The variants tend to vary by degree
Variants
-
♦
Aminolevulinic acid dehydratase porphyria (ALA)
-
♦
Acute intermittent porphyria (AIP)
-
♦
Congenital erythropoietic porphyria (CEP)
-
♦
Porphyria cutanea tarda (PCT)
-
♦
Hepatoerythropoietic porphyria (HEP)
-
♦
Hereditary coproporphyria (HCP)
-
♦
Variegate porphyria (VP)
-
♦
Erythropoietic protoporphyria (EPP)
-
♦
Pseudoporphyria (PP) (drug induced)
Clinical
-
♦
The following discussion pertains to the porphyrias with cutaneous manifestations
-
♦
Cutaneous changes can either immediate or delayed
-
♦
An immediate reaction, as seen in EPP, includes erythema, pain, edema, and purpura
-
♦
The other types of cutaneous porphyria show delayed phototoxicity, presenting as fragility, blistering, scarring, and hypertrichosis
-
♦
Other reported clinical findings include sclerodermoid changes, alopecia, and hyperpigmentation
-
♦
In inherited homozygous PCT, abnormal enzyme levels are seen in the liver and the red blood cells
-
♦
In heterozygous PCT, where abnormal enzyme levels are expressed in the liver, disease expression usually requires a “second hit” to the liver such as concomitant infection (hepatitis or HIV), alcohol ingestion, estrogen therapy, or pregnancy
-
♦
Diagnosis and subtyping of porphyria are based in part on the clinical presentation, microscopic characteristic, and immunofluorescence. However, the porphyrin levels in the urine, stool, and red blood cells are the gold standard of diagnosis
Microscopi c
-
♦
The subtypes demonstrate similar findings to varying degrees
-
♦
They are characterized by a pauci-inflammatory subepidermal separation with upward protrusion of the dermal papillae (“festooning”) (Fig. 18.101)
Fig. 18.101. 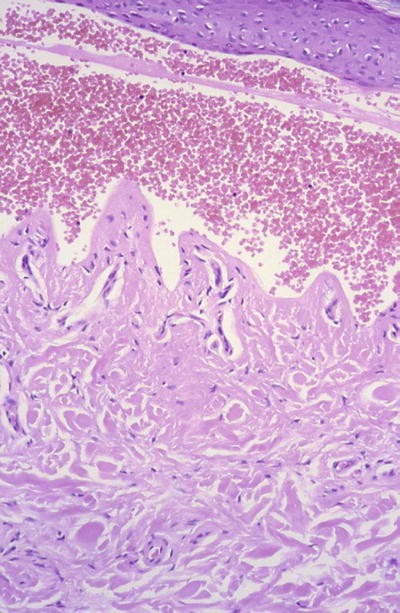
Porphyria . Subepidermal. Separation with minimal inflammation and “festooning”.
-
♦
There is homogeneous thickening of the blood vessels in the dermal papillae
-
♦
There is PAS-positive deposition of material in and around the upper dermal blood vessels as well as along the basement membrane zone
-
♦
Actinic elastosis is usually present
-
♦
Thickening of the basement membrane zone, hyperkeratosis, acanthosis, and hypergranulosis are variably present
-
♦
Occasionally, PAS-positive globules arranged in a linear fashion may be seen in the blister roof (“caterpillar bodies”) (Fig. 18.102)
Fig. 18.102. 
Porphyria . Subepidermal. “Caterpillar bodies”.


Electron Microscopy
-
♦
EM shows extensive reduplication of the basal lamina of the upper dermal blood vessels and basement membrane zone
-
♦
There are widened perivascular spaces containing fibrillar material and small collagen fibrils
-
♦
In some cases, there are irregular clumps of amorphous material embedded in the perivascular material
-
♦
The site of separation is the lamina lucida
Immunopathology
-
♦
Again, the subtypes demonstrate similar findings to varying degrees
-
♦
There is marked deposition of immunoglobulin and complement (IgG, IgM, C3, IgA, and fibrinogen) in and adjacent to the upper dermal blood vessels (Fig. 18.103)
Fig. 18.103. 
Porphyria . Subepidermal. Strong deposition of IgG in and adjacent to papillary dermal blood vessels and weak thick linear deposition along the basement membrane zone.
-
♦
In addition, there is weak thick deposition of immunoglobulin and complement along the basement membrane zone
-
♦
In general, these changes are more pronounced in involved sun-exposed skin and in active lesions
-
♦
EPP demonstrates changes more marked than PCT, VP, or P P

Deposition on Eosinophils and Diffuse Deposition on Connective Tissue
Urticaria
Clinical
-
♦
Referred to as hives or wheals, they are characterized by pruritic, erythematous, or white, nonpitting edematous papules or plaques that change in size and shape over hours
-
♦
They vary in size from small papules to large plaques
-
♦
The depth of involvement varies from superficial to deep
-
♦
Episodes of urticaria are arbitrarily defined as either acute or chronic
-
♦
Chronic includes episodes persisting for longer than 6 weeks
-
♦
While the cause of acute urticaria is often established (usually food, drug, or contact), the cause of chronic urticaria is usually not identified
-
♦
There are many implicated etiologic factors and associations, including foods and food additives, medications and hormonal perturbations, inhaled allergens, various internal diseases and malignancies, contactants (via both immunologic and non-immunologic mechanisms), primary skin diseases (e.g., immunobullous diseases), and genetic diseases
-
♦
Urticaria may be separated into a variety of subtypes based on the etiology
Clinical Subtypes
-
♦
Physical urticarias
-
♦
Dermatographism
-
♦
Pressure urticaria
-
♦
Cholinergic urticaria
-
♦
Exercise-induced urticaria
-
♦
Solar urticaria
-
♦
Cold urticaria
-
♦
Heat, water, and vibrational urticaria
-
♦
Aquagenic pruritus
-
♦
Angioedema
-
♦
Acquired angioedema
-
♦
Hereditary angioedema
-
♦
Contact urticaria
-
♦
Urticaria secondary to an ingested substance (food, medication, or others)
-
♦
Pruritic and urticarial papules and plaques of pregnancy
-
♦
Urticarial vasculitis
Microscopic
-
♦
All of the subtypes of urticaria demonstrate similar histopathologic features
-
♦
Acute urticaria shows dermal interstitial edema, dilated venules with endothelial swelling, and a minimal degree of inflammation, including intravascular neutrophils and perivascular lymphocytes and eosinophils
-
♦
In chronic urticaria, there is interstitial edema with a perivascular and interstitial polymorphous infiltrate of neutrophils, eosinophils, and lymphocytes, as well as intravascular neutrophi ls
-
♦
The deeper the clinical form of urticaria, the deeper the extension of the histopathologic findings
-
♦
Angioedema extends into the subcutaneous tissue
-
♦
Hereditary angioedema demonstrates deep dermal and subcutaneous edema with minimal accompanying inflammation
Immunopathology
-
♦
DIF demonstrates deposition on eosinophils with IgA and, to a lesser degree with IgG, IgM
-
♦
Fibrinogen shows diffuse deposition on the connective tissue throughout the dermis
-
♦
This pattern is nonspecific but consistent with the clinical diagnosis of urticari a
Deposition in Blood Vessels
Vasculitis
Immunopathology
-
♦
In general, vasculitis is characterized by intravascular deposition of immunoglobulins and complement
-
♦
IgM is usually the predominant immunoglobulin deposited, but IgG and IgA are also seen
-
♦
Fibrinogen is often deposited in a perivascular pattern, with diffusion into the surrounding interstitial tissue
-
♦
The diagnosis of vasculitis should be reserved for specimens that show intravascular deposition with multiple immunoreactants
-
♦
Further, because vascular fluorescence can be seen nonspecifically in various inflammatory conditions, as well as in dependent locations (such as lower extremity), histopathology that is typical for vasculitis must also be present to justify the diagnosis
-
♦
Some of the clinical subtypes of vasculitis have more distinctive immunopathologic findings
-
♦
For example, Henoch–Schönlein purpura has a granular deposition of IgA in the superficial vessels that predominates over the deposition of other immunoglobulins
-
♦
Urticarial vasculitis has findings typical for urticaria in addition to immunoglobulin deposition in blood vessels
-
♦
Further, a subset of patients with urticarial vasculitis have systemic lupus erythematosus (either overt or in evolution) and demonstrate (in addition to features of urticarial vasculitis) granular deposition of IgM and other immune reactants along the base ment membrane zone, typical for lupus erythematosus
TNM Classification of Malignant Melanoma of the Skin (2010 Rs)
-
♦
T: Primary Tumor
-
T0: No evidence of primary tumor
-
Tis: Melanoma in situ (Clark level I)
-
T1: Melanoma ≤1.0 mm in thickness
-
T1a: Melanoma ≤1.0 mm in thickness without ulceration and mitoses ≤1 per square mm
-
T1b: Melanoma ≤1.0 mm in thickness with ulceration or mitoses greater than or equal (insert symbol) 1 per square mm
-
T2: Melanoma 1.01–2 mm in thickness with or without ulceration
-
T2a: Melanoma 1.01–2 mm in thickness, no ulceration
-
T2b: Melanoma 1.01–2 mm in thickness, with ulceration
-
T3: Melanoma 2.01–4 mm in thickness with or without ulceration
-
T3a: 2.01–4 mm in thickness, no ulceration
-
T3b: 2.01–4 mm in t hickness, with ulceration
-
T4: Melanoma greater than 4.0 mm in thickness with or without ulceration
-
T4a: Melanoma >4.0 mm in thickness, no ulceration
-
T4b: Melanoma >4.0 mm in thickness, with ulceration
-
-
♦
N: Regional Lymph Nodes
-
NX: Regional node s cannot be assessed
-
N0: No regional lymph node metastasis
-
N1: Metastasis in one lymph node
-
N1a: Clinically occult (microscopic) metastasis
-
N1b: Clinically apparent (macroscopic) metastasis
-
N2: Metastases in two to three regional nodes or intralymphatic regional metastasis without nodal metastasis
-
N2a: Clinically occult (microscopic) metastasis
-
N2b: Clinically apparent (macroscopic) metastasis
-
N2c: Satellite or in-transit metastasis without nodal metastasis
-
N3: M etastasis in four or more regional nodes, or matted metastatic nodes, or in-transit metastasis or satellite(s) with metastasis in regional node(s)
-
-
♦
M: Distant Metastasis
-
MX: Distant metastasis cannot be assessed
-
M0: No distant metastasis
-
M1: Distant metastasis
-
M1a: Metastasis to the skin, subcutaneous tissue, or distant lymph nodes
-
M1b: Metastasis to the lung
-
M1c: Metastasis to all other visceral sites or distant metastasis at any site associated with an elevated serum lactic dehydrogenase (LDH )
-
TNM Classification of Cutaneous SQU Amous Cell Carcinoma (CSCC) and Other Cutaneous Carcinomas (2010 Edition, AJCC)
-
♦
T: Primary TumorFootnote 1
-
T0: No evidence of primary tumor
-
Tis: Carcinoma in situ
-
T1: Tumor 2 cm or less with less than two high-risk featuresFootnote 2
-
T2: Tumor greater than 2 cm or any size with two or more high-risk features (see Footnote 1)
-
T3: Tumor with invasion of the maxilla, mandible, orbit, or temporal bone
-
T4: Tumor with invasion of the skeleton (axial or appendicular) or perineural invasion of the skull base
-
-
♦
N: Regional Lymph Nodes
-
NX: Regional lymph nodes cannot be assessed
-
N0: No regional lymph node metastases
-
N1: Metastasis in a single ipsilateral lymph node, 3 cm or less
-
N2: Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm; or in multiple ipsilateral lymph nodes, none more than 6 cm; or in bilateral or contralateral lymph nodes, none more than 6 cm
-
N2a: Metastasis in a single ipsilateral lymph node more than 3 cm but not more than 6 cm
-
N2b: Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm
-
N2c: Metastasis in bilateral or contralateral lymph nodes, none more than 6 cm
-
N3: Metastasis in a lymph node more than 6 cm
-
-
♦
M: Distant Metastasis
-
M0: No distant metastasis
-
M1: Distant metastasis
-
TNM Classification of Merkel Cell Carcinoma (2010 Edition, AJCC)
-
♦
T: Primary Tumor
-
T0: No evidence of primary tumor (e.g., nodal/metastatic presentation without known primary)
-
Tis: In situ primary tumor
-
T1: Less than or equal to 2 cm maximum tumor dimension
-
T2: Greater than 2 cm but not more than 5 cm maximum tumor dimension
-
T3: Greater than 5 cm maximum tumor dimension
-
T4: Tumor invades the bone, muscle, fascia, or cartilage
-
-
♦
N: Regional Lymph Nodes
-
NX: Regional lymph nodes cannot be assessed
-
N0: No regional lymph node metastases
-
cN0: Nodes negative by clinical exam (inspection, palpation, and/or imaging)
-
pN0: Nodes negative by pathologic exam
-
N1: Metastasis in regional lymph node(s)
-
N1a: Micrometastasis (diagnosed after sentinel or elective lymphadenectomy)
-
N1b: Macrometastasis (clinically detectable metastasis confirmed by lymphadenectomy or biopsy)
-
N2: In-transit metastasis (a tumor distinct from the primary lesion and located either between the primary lesion and draining regional lymph node or distal to the primary lesion)
-
-
♦
M: Distant Metastasis
-
M0: No distant metastasis
-
M1: Metastasis beyond regional lymph nodes
-
M1a: Metastasis to the skin, subcutis, or distant lymph nodes
-
M1b: Metastasis to the lung
-
M1c: Metastasis to all other visceral sites
-
Notes
- 1.
Excludes CSCC of the eyelid.
- 2.
High-risk features
-
Depth invasion: >2 mm thickness, Clark level ≥ IV, and perineural invasion
-
Anatomic locations: Primary sites – ear and hair-bearing lip
-
Differentiation: Poorly differentiated or undifferentiated
-
Suggested Reading
Cutaneous Neoplasms and Developmental Anomalies
Argenyi ZB. Newly recognized neural neoplasms relevant to the dermatopathologist. Dermatol Clin. 1992;10:219–34.
Argenyi ZB. Cutaneous neural heterotopias and related tumors relevant for the dermatopathologist. Semin Diagn Pathol. 1996;13:60–71.
Beltraminelli H, Leinweber B, Kerl H, Derroni L. Primary cutaneous CD4+ small/medium-sized pleomorphic T-cell lymphoma: a cutaneous nodular proliferation of pleomorphic T lymphocytes of undetermined significance? A study of 136 cases. Am J Dermatopathol. 2009;31:317–22.
Bobos M, Hytiroglou P, Kostopoulos I, Karkavelas G, Papadimitriou C. Immunohistochemical distinction between merkel cell carcinoma and small cell carcinoma of the lung. Am J Dermatopathol. 2006;28:99–104.
Burg G, Kempf W, Cozzio A, et al. WHO/EORTC classification of cutaneous lymphomas 2005: histological and molecular aspects. J Cutan Pathol. 2005;32:647–74.
Cibull T, Thomas A, O’Malley D, Billings S. Myeloid leukemia cutis: a histologic and immunohistochemical review. J Cutan Pathol. 2008;35:180–5.
Cruz DJ. Sweat gland carcinomas: a comprehensive review. Semin Diagn Pathol. 1987;4:38–74.
Fabrizi G, Pagliarello C, Prente P, Massi G. Atypical nevi of the scalp in adolescents. J Cutan Pathol. 2007;34:365–9.
Fetsch J, Laskin W, Hallman J, Lupton G, Miettinen M. Neurothekeoma: an analysis of 178 tumors with detailed immunohistochemical data and long-term patient follow-up information. Am J Surg Pathol. 2007;31:1103–14.
González SB. Histopathologic diagnosis of pigmented lesions of the skin. Pathol Res Pract. 1991;187:387–431.
Groben P, Harvell J, White W. Epithelioid blue nevus: neoplasm or Sui generis or variation on a theme? Am J Dermatopathol. 2000;22:473–88.
Kempf W, Kasakov D, Kerl K. Cutaneous lymphomas: an update. Part 1: T-cell and Natural Killer/T-cell lymphomas and related conditions. Am J Dermatopathol. 2014;36:105–23.
Olsen E, Vonderheid E, Pimpinelli N, et al. Revisions to the staging and classification of mycosis fungoides and Sézary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110:1713–22.
Massa M, Medenica M. Cutaneous adnexal tumors and cysts: a review. II. Tumors with apocrine and eccrine glandular differentiation and miscellaneous cutaneous cysts. Pathol Annu. 1987;22:225–76.
Massone C, El-Shabrawi-Caelen L, Kerl H, Cerroni L. The morphologic spectrum of primary cutaneous anaplastic large T-cell lymphoma: a histopathologic study on 66 biopsy specimens from 47 patients with report of rare variants. J Cutan Pathol. 2008;35:46–53.
McQuitty E, Curry JL, Teztlaff MT, Prieto VG, Duvic M, Torres-Cabala C. The differential diagnosis of CD8-positive (“type D”) lymphomatoid papulosis. J Cutan Pathol. 2014;41:88–100.
Mentzel T, Kutzner H. Dermatomyofibroma: clinicopathologic and immunohistochemical analysis of 56 cases and reappraisal of a rare and distinct cutaneous neoplasm. Am J Dermatopathol. 2009;31:44–9.
Plaza J, Torres-Cabala C, Evans H, Diwan A, Prieto V. Immunohistochemical expression of S100A6 in cellular neurothekeoma: clinicopathologic and immunohistochemical analysis of 31 cases. Am J Dermatopathol. 2009;31:419–22.
Reichard K, Burks E, Foucar K, et al. CD4(+) CD56(+) lineage-negative malignancies are rare tumors of plasmacytoid dendritic cells. Am J Surg Pathol. 2005;29:1274–83.
Requena C, Requena L, Kutzner H, Yus E. Spitz nevus: a clinicopathologic study of 349 cases. Am J Dermatopathol. 2009;31:107–16.
Requena L, Sangueza OP. Cutaneous vascular anomalies. Part I. Hamartomas, malformations, and dilatation of preexisting vessels. J Am Acad Dermatol. 1997a;37:523–49.
Requena L, Sangueza OP. Cutaneous vascular proliferations. Part II. Hyperplasias and benign neoplasms. J Am Acad Dermatol. 1997b;37:887–919.
Requena L, Sangueza OP. Cutaneous vascular proliferations. Part III. Malignant neoplasms, other cutaneous neoplasms with significant vascular component, and disorders erroneously considered as vascular neoplasms. J Am Acad Dermatol. 1998;38:143–75.
Singh R, Grayson W, Redston M, et al. Site and tumor type predicts DNA mismatch repair status in cutaneous sebaceous neoplasia. Am J Surg Pathol. 2008;32:936–42.
Slater DN. The new World Health Organization-European Organization for Research and Treatment of Cancer classification for cutaneous lymphomas: a practical marriage of two giants. Br J Dermatol. 2005;153:874–80.
Swanson PE, Cherwitz DL, Neumann MP, Wick MR. Eccrine sweat gland carcinoma: an histologic and immunohistochemical study of 32 cases. J Cutan Pathol. 1987;14:65–86.
Tardio J. CD34-reactive tumors of the skin. An updated review of an ever-growing list of lesions. J Cutan Pathol. 2008;35:1079–92.
Walsh N, Crotty K, Palmer A, McCarthy S. Spitz nevus versus spitzoid malignant melanoma: an evaluation of the current distinguishing histopathologic criteria. Hum Pathol. 1998;29:1105–12.
Wick MR, Goellner JR, Wolfe III JT, Su WPD. Adnexal carcinomas of the skin, I: eccrine carcinomas. Cancer. 1985a;56:1147–62.
Wick MR, Goellner JR, Wolfe III JT, Su WPD. Adnexal carcinomas of the skin, II: extraocular sebaceous carcinomas. Cancer. 1985b;56:1163–72.
Willemze R, Jaffe E, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3768–85.
Zelger BWH, Sidoroff A, Orchard G, Cerio R. Non-Langerhans cell histiocytoses. Am J Dermatopathol. 1996;18:490–504.
Immunodermatology
Abell E, Presbury DG, Marks R, et al. The diagnostic significance of immunoglobulin and fibrin deposition in lichen planus. Br J Dermatol. 1975;93:17–24.
David-Bajar KM, Bennion SD, DeSpain JD, et al. Clinical, histologic and immunofluorescent distinctions between subacute cutaneous lupus erythemaatosus and discoid lupus erythematosus. J Invest Dermatol. 1992;99:251–7.
Gammon WR, Briggaman RA, Woodley DT, et al. Epidermolysis bullosa acquisita: a pemphigoid-like disease. J Am Acad Dermatol. 1984;11:820–32.
Gately LE, Nesbitt LT. Update on immunofluorescent testing in bullous diseases and lupus erythematosus. Dermatol Clin. 1994;1:133–42.
Jones RR, Bhogal B, Dash A, et al. Urticaria and vasculitis: a continuum of histological and immunopathological changes. Br J Dermatol. 1983;108:695–703.
Korman NJ. Pemphigus. Immunodermatology. 1990;8:689–700.
Leonard JN, Tucker WFG, Fry JS, et al. Increased incidence of malignancy in dermatitis herpetiformis. Br J Med. 1983;286:16–8.
Logan RA, Bhogal B, Das AK, et al. Localization of bullous pemphigoid antigen: an indirect immunofluorescence study of 228 cases using a split-skin technique. Br J Dermatol. 1987;117:471–8.
Mutasim DF, Pelc NJ, Anhalt GJ. Paraneoplastic pemphigus. Dermatol Clin. 1993;11:473–81.
Olansky AJ, Briggaman RA, Gammon WR, et al. Bullous systemic lupus erythematosus. J Am Acad Dermatol. 1982;7:511–20.
Person JR, Rogers III RS. Bullous and cicatricial pemphigoid: clinical, histologic, pathogenic and immunopathological correlations. Mayo Clin Proc. 1977;52:54–66.
Peters MS, Rogers III RS. Clinical correlations of IgA deposition at the cutaneous basement membrane zone. J Am Acad Dermatol. 1989;20:761–70.
Schroeter AL, Copeman PWM, Hordon RE, et al. Immunofluorescence of cutaneous vasculitis associated with systemic disease. Arch Dermatol. 1971;104:254–9.
Shornick JK. Herpes gestationis. Dermatol Clin. 1993;11:527–33.
Zone JJ, Taylor TB, Meyer LJ. Identification of the cutaneous basement membrane zone antigen and isolation of antibody in linear immunoglobulin A bullous dermatosis. J Clin Invest. 1990;85:812.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Vandersteen, D.P., Jokinen, C.H. (2016). Neoplasms of the Skin and Immunodermatology. In: Cheng, L., Bostwick, D. (eds) Essentials of Anatomic Pathology. Springer, Cham. https://doi.org/10.1007/978-3-319-23380-2_18
Download citation
DOI: https://doi.org/10.1007/978-3-319-23380-2_18
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23379-6
Online ISBN: 978-3-319-23380-2
eBook Packages: MedicineMedicine (R0)