
Abstract
Home ventilators with built-in software provide substantial information for monitoring home noninvasive ventilation, such as compliance, pattern of ventilator use, leaks, respiratory rate, percentage of respiratory cycles triggered and cycled by the device, and apnea-hypopnea index. Certain values are reliable and useful, however, reliability of data is not equivalent between all ventilators. The clinician should thus not rely only on these data for adjusting ventilator settings.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
During the past 20 years, long-term noninvasive ventilation (NIV) has become the key treatment for chronic hypercapnic respiratory failure. Technical advances, in particular in bi-level pressure-cycled ventilators, have been tremendous over the years in terms of pressurization, compensation for leaks, size, noise, and improvement of patient-ventilator synchronization through adjustable inspiratory and expiratory triggers. Many newer bi-level ventilators designed for home care are provided with built-in software that supplies detailed information about compliance, tidal volume (VT), minute ventilation (VE), respiratory rate (RR), estimated leaks, respiratory cycles triggered by the patient (%Trigg), and apnea-hypopnea index (AHI) [1, 2]. This chapter discusses the reliability of data recorded by software for home ventilators and highlights their clinical utility based on the published evidence.
2 Compliance
Data recorded by ventilator software are extremely useful for assessing compliance and pattern of ventilator use. The pattern of ventilation is an indirect indicator of tolerance of NIV and comfort. For example, multiple interruptions during the night after short periods of NIV or an erratic pattern of use over several days is suggestive of poor adaptation to NIV and patient discomfort (Fig. 8.1). Conversely, a rapid increase in NIV use may suggest imminent exacerbation in patients who are not ventilator dependent (Fig. 8.2). A study by Borel et al. [3] assessed whether data retrieved from a NIV device could be used to predict the risk of exacerbation in patients with chronic obstructive pulmonary disease (COPD) treated by home NIV. In this selected population, some patients increased their adherence to NIV prior to exacerbations (because NIV alleviates dyspnea), whereas other patients reduced its use (reflecting intolerance and/or inadequacy of ventilator settings during exacerbations). As reported by our group, compliance may also be related to the underlying chronic respiratory condition. For instance, neuromuscular patients, especially those suffering from progressive disease, tend to increase their use of NIV over time compared with patients treated for obesity hypoventilation syndrome (OHS) [2]. Monitoring of daily use of NIV may also detect progression of highly dependent patients who need a second ventilator with an internal battery for security reasons.

(a) Graphic transcription of daily compliance and pattern of use of a ventilator provided by ventilator software in a patient who is well adapted to his ventilator, with excellent compliance. Use of the ventilator during the night is continuous, without interruption, suggesting acceptable quality of sleep. (b) Graphic transcription of daily compliance and pattern of use of ventilator provided by ventilator software in a patient who tolerates his treatment poorly, revealing multiple interruptions during the night, and days without ventilator use (Adapted from Ref. [2])

Upper graph: pattern of use; Lower graph: total daily use. Graphic illustration of pattern of use and total daily use in a COPD patient with poor adaptation to NIV. Note frequent interruption during treatment, days with no treatment, and daily use <4 h. Six days before admission to the respiratory ward for acute exacerbations of COPD, the patient complained of shortness of breath that was alleviated by NIV, as evidenced by a rapid increase in daily use
A detailed report on compliance is important for deciding whether or not to pursue ventilatory support, discussing alternate patterns of daily use of NIV in case of poor tolerance during the night (i.e., daytime sessions), and understanding insufficient impact of NIV on arterial blood gases (ABG) or clinical symptoms.
3 VT and Minute Ventilation
Although leaks have traditionally been a problem in volume-cycled NIV, pressure cycling and advances in blower technology now allow a certain amount of unintentional leakage without affecting pressurization capabilities and efficient delivery of VT, at least in some ventilators [4]. This is of major importance because unintentional leaks are a clinical reality in unsupervised patients treated by domiciliary NIV.
In single-limb circuits with a vented mask, the built-in flow sensor monitors total gas flow, that is, the sum of respiratory flow and unintentional and intentional leaks (Fig. 8.3). Because there is no direct measurement of expiratory flow in a single-limb circuit, VT can only be estimated by taking into account changes in flow and unintentional leaks (from the mask or from the mouth), assuming that the intentional leak is known. For most ventilators, built-in software underestimates VT and this underestimation is little affected by leaks. Conversely, higher pressure support increases underestimation of VT [5, 6]. Sogo et al. [7] developed a bench model presented as more representative of clinical leaks by inducing random dynamic leaks during inspiratory or expiratory phases. Unlike previous studies, the authors found that the four ventilators tested significantly overestimated VT (with differences ranging from 18 % ± 7 % to 36 % ± 18 %) suggesting that a portion of the identified leak was erroneously considered by the software as volume delivered to the patient. The inaccuracy in VT estimation has direct clinical implications: commercial software can unpredictably either underestimate or overestimate VT. For these reasons, clinicians should minimize unintentional leaks by adjusting mask fit or changing mask type or ventilator settings. Once leaks have been corrected, clinicians must remain aware of differences in estimation of VT between ventilators and not rely only on information provided by ventilator software to monitor efficacy of NIV.

Flow and leaks during NIV with a bi-level pressure support ventilator (single-tube system and nasal mask vented)
4 Leaks
Unintentional leaks are major contributors to NIV intolerance, patient-ventilator asynchrony, suboptimal correction of ABGs, and nocturnal hypoventilation. Estimation of leaks by the ventilator – if reliable – is a useful contribution to NIV monitoring.
Rabec et al. [8] showed that leaks assessed by built-in software of the VPAPTM III-ResLinkTM (ResMed, North Ryde, Australia) ventilators were highly correlated with bench test measurements. These results cannot, however, be extrapolated to all home bi-level ventilators because bench testing of different commercially available home ventilators has demonstrated important discrepancies in leak estimation between devices [5–7]. One important caveat is that devices do not all report estimations of leaks in the same way. For instance, leaks are reported either as an estimation of unintentional leaks or as an estimation of total leaks (i.e., leaks through mask exhalation valves plus unintentional leaks) (Fig. 8.3). Physicians monitoring patients on home NIV should therefore be aware of these differences. Manufacturers have determined an arbitrary threshold for leaks below which pressurization is considered effective. In case of major leaks, the leak compensation may be insufficient and impair efficacy of ventilation, as shown in Fig. 8.4 [8]. Conversely, thresholds reported by manufacturers are not necessarily relevant, inasmuch as recent home ventilators have a high capacity for leak compensation.

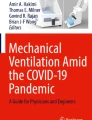
VPAP-Reslink™ characteristic tracing showing – from top to bottom – respiratory rate, leaks (unintentional leaks in liters/second), minute ventilation, and SpO2. Important unintentional leaks (>0.4 l/s) are associated with a prolonged decrease in SpO2 directly measured by the device’s pulse oximetry module (Adapted from Ref. [8])
5 Respiratory Rate and Percentage of Respiratory Cycles Triggered by the Patient
Most ventilator softwares provide information about spontaneous RR and %Trigg. This information must be interpreted with caution according to the clinical scenarios. For instance, a low %Trigg may occur when the patient has a backup RR above his or her spontaneous RR. In this situation, the patient is assumed to be treated with a “controlled ventilation mode.” However, in conditions in which inspiratory efforts are potentially not detected by the ventilator (major leaks, patients with severe neuromuscular disease and low inspiratory muscle strength, intrinsic positive end-expiratory pressure in severe COPD, upper airway closure), a low %Trigg may in fact reflect the inability of the ventilator to respond to the patient’s inspiratory efforts, leading to patient-ventilator asynchrony. Conversely, a high value of RR above backup rate and a high %Trigg can represent appropriate detection of triggering efforts in a “spontaneous mode” as well as auto-triggering in case of important unintentional leaks or clinical conditions with low respiratory drive.
Whether it is preferable to use a high or a low backup rate for home NIV is still a matter of debate. It has been a long tradition to “capture” the patient with a backup rate in neuromuscular diseases. In OHS, evidence suggests that using a backup rate may prevent central and obstructive respiratory events [9]. In COPD, evidence as to increasing backup rate is scarce: high-intensity NIV with high inspiratory pressures and a high backup rate improves physiological endpoints [10]; however, a recent randomized controlled trial demonstrated no advantage of associating a high backup rate to high pressure support in night-time ventilator adherence or any of the other measured physiological parameters (including PaCO2) [11]. These data suggest that it is the high-pressure component of the high-intensity NIV approach that plays the therapeutic role in the management of hypercapnic respiratory failure, at least in the COPD population. Using a telemetry approach, Borel et al. [3] recently demonstrated that daily variations in RR and %Trigg are predictors of acute exacerbations in patients with COPD. This “proof of concept” study provides a potentially simple predictive approach through telemonitoring, which requires neither the patient’s active involvement nor additional sensors in their environment.
6 Apnea-Hypopnea Index
To our knowledge, the validity and accuracy of AHI provided by home ventilators has not been thoroughly studied. The lack of standardized definitions for respiratory events occurring under positive-pressure ventilation and their mode of detection is problematic. In an observational study of OHS patients under NIV, the correlation between AHI provided by the ventilator software and AHI measured simultaneously by polysomnography was high, with a low bias. An arbitrary threshold value of 10 for AHI proved to be sensitive and specific for discriminating between patients appropriately ventilated versus those requiring further adjustment of ventilator settings [12]. This study had, however, a few limitations and should be repeated in other patient groups with different NIV devices before one can determine whether it is possible to rely on AHI indices provided by ventilator software.
7 Conclusion
Home ventilators with built-in software provide substantial information for monitoring home NIV, such as compliance, pattern of ventilator use, leaks, RR, %Trigg, and AHI. This information may be used to adapt ventilator settings and can have a direct impact on patient management. However, reliability of data is not equivalent between all ventilators. The NIV physician therefore should not completely rely on these data to adapt ventilator settings. Presently, data provided by ventilator software are a useful adjunct to recommended tools for basic monitoring of NIV, such as ABG analysis, nocturnal pulse oximetry, nocturnal capnography, and polygraphy.
Key Points
-
A detailed report on compliance is important for deciding whether or not to pursue ventilatory support, discussing alternate patterns of daily use of NIV in case of poor tolerance during the night (i.e., daytime sessions), and understanding insufficient impact of NIV on ABG or clinical symptoms.
-
Clinicians monitoring patients on home NIV should be aware of differences in the estimation of leaks between ventilators. They should aim to maintain the 95th percentile of leak values at the lowest possible level by adjusting interface and ventilator settings.
-
Home ventilator softwares (see above) does not provide accurate and reliable values of VT and VE. Discrepancies exist between home ventilators and are influenced by leaks. Clinicians should thus not rely only on these data for adjusting ventilator settings.
-
RR and %Trigg can help the clinician to better set the backup RR on the home ventilator.
Abbreviations
- %Trigg:
-
Percentage of respiratory cycles triggered by the patient
- ABG:
-
Arterial blood gases
- AHI:
-
Apnea-hypopnea index
- COPD:
-
Chronic obstructive pulmonary disease
- NIV:
-
Noninvasive ventilation
- OHS:
-
Obesity hypoventilation syndrome
- RR:
-
Respiratory rate
- VE:
-
Minute volume
- VT:
-
Tidal volume
References
Janssens JP, Borel JC, Pépin JL. Nocturnal monitoring of home non-invasive ventilation: the contribution of simple tools such as pulse oximetry, capnography, built-in ventilator software and automatic markers of sleep fragmentation. Thorax. 2011;66:438–45.
Pasquina P, Adler D, Farr P, Bourqui P, Bridevaux PO, Janssens JP. What does built-in software of home ventilators tell us? An observational study of 150 patients on home ventilation. Respiration. 2012;83:293–9.
Borel JC, Pelletier J, Taleux N, Briault A, Arnol N, Pison C, Tamisier R, Timsit JF, Pepin JL. Parameters recorded by software of non-invasive ventilators predict COPD exacerbation: a proof-of-concept study. Thorax. 2015;70:284–5.
Battisti A, Tassaux D, Janssens JP, Michotte JB, Jaber S, Jolliet P. Performance characteristics of 10 home mechanical ventilators in pressure-support mode: a comparative bench study. Chest. 2005;127:1784–92.
Contal O, Vignaux L, Combescure C, Pepin JL, Jolliet P, Janssens JP. Monitoring of noninvasive ventilation by built-in software of home bilevel ventilators: a bench study. Chest. 2012;141:469–76.
Luján M, Sogo A, Pomares X, Monsó E, Sales B, Blanch L. Effect of leak and breathing pattern on the accuracy of tidal volume estimation by commercial home ventilators: a bench study. Respir Care. 2013;58:770–7.
Sogo A, Montanyà J, Monsó E, Blanch L, Pomares X, Lujàn M. Effect of dynamic random leaks on the monitoring accuracy of home mechanical ventilators: a bench study. BMC Pulm Med. 2013;13:75.
Rabec C, Georges M, Kabeya NK, Baudouin N, Massin F, Reybet-Degat O, Camus P. Evaluating noninvasive ventilation using a monitoring system coupled to a ventilator: a bench-to-bedside study. Eur Respir J. 2009;34:902–13.
Contal O, Adler D, Borel JC, Espa F, Perrig S, Rodenstein D, Pépin JL, Janssens JP. Impact of different back up respiratory rates on the efficacy of noninvasive positive pressure ventilation in obesity hypoventilation syndrome: a randomized trial. Chest. 2013;143:37–46.
Dreher M, Storre JH, Schmoor C, Windisch W. High-intensity versus low-intensity non-invasive ventilation in patients with stable hypercapnic COPD: a randomised crossover trial. Thorax. 2010;65:303–8.
Murphy P, Brignall K, Moxham J, Polkey M, Davidson C, Hart N. High pressure versus high intensity noninvasive ventilation in stable hypercapnic chronic obstructive pulmonary disease: a randomized crossover trial. Int J Chron Obstruct Pulmon Dis. 2012;7:811–8.
Georges M, Adler D, Contal O, Espa F, Perrig S, Pépin JL, Janssens JP. Reliability of apnea-hypopnea index measured by a home bi-level pressure support ventilator versus a polysomnographic assessment. Respir Care. 2015;60(7):1051–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Pasquina, P., Janssens, JP., Contal, O., Adler, D. (2016). Software for Home Ventilators and Leak Compensation: Key Technical and Practical Applications. In: Esquinas, A. (eds) Noninvasive Mechanical Ventilation. Springer, Cham. https://doi.org/10.1007/978-3-319-21653-9_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-21653-9_8
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-21652-2
Online ISBN: 978-3-319-21653-9
eBook Packages: MedicineMedicine (R0)