
Abstract
A 57-Year-old man presented to emergency department complaining palpitations during effort. The family history and an echocardiogram revealed the patient was affected by hypertrophic cardiomyopathy. Hence, we assessed the sudden cardiac death risk of the patient using the appropriate risk score calculator. Palpitations appeared to be related to non-sustained ventricular tachycardias that is one of the risk factors.The patient’s estimated risk of sudden cardiac death at 5 years was 5% and supported the indication for ICD (implantable defibrillator) implant in primary prevention.We performed the implant of a subcutaneous ICD, according to primary prevention, no need for anti-bradycardia pacing and patient’s choice.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Case Report
-
A 57-year-old man presented to the emergency room complaining palpitations that started suddenly few hours before, during a moderate walking. Palpitations were accompanied by dyspnea and mild dizziness. Symptoms lasted for about 10 min, forcing the patient to rest. The episode interrupted abruptly and spontaneously, and the patient did not remember if heartbeat was regular during the episode. He never had arrhythmias before and he denied syncope or angina.
-
The patient presented completely asymptomatic to the emergency room.
1.1 Medical History and Cardiovascular Risk Factors
-
The family history revealed that his mother was affected by hypertrophic cardiomyopathy (HCM). There was not any case of sudden cardiac death in the family.
-
At 20 years old, HCM was incidentally diagnosed during a sport screening and since pre-participation screening and since then he was regularly followed up.
-
He was a smoker.
1.2 Allergies
None
1.3 Medications
Verapamil 80 mg BID
1.4 Vital Signs
-
Temperature: 36.3 °C
-
Resting heart rate: 58 bpm
-
Blood pressure: 125/90 mmHg
-
Respiratory rate: 18 breaths per minute
-
Oxygen saturation while breathing in room air: 99 %
1.5 Physical Examination
The patient appeared in good clinical condition.
At physical examination, the relevant findings were the following:
Cardiovascular: Apical precordial impulse was forceful but not displaced laterally. Regular rate and rhythm; S1 and S2 were normal with an adjunctive S4. Systolic ejection late-peaking murmur was best heard between the apex and left sternal border without radiation to the neck, and it was increased by Valsalva maneuver. Mild diastolic decrescendo murmur was detected in Erb auscultator focus.
Lungs: No rales at auscultation neither rhonchi nor wheezes bilaterally.
Abdomen: Plain and tractable; no hepatosplenomegaly.
Extremities: No lower limb edema.
1.6 Routine Laboratory Tests
-
Complete blood count: normal
-
Cholesterol (total, HDL, LDL) and TG: normal
-
Fasting blood glucose: 78 m/dl (4.33 mmol/L)
-
Hepatic function (GOT, GPT, γ-GGT, ALP, total bilirubin, direct and indirect): normal
-
Thyroid function (TSH, FT3, FT4): normal
-
Renal function (creatinine, BUN): normal
-
Electrolytes (Na + , K + , Ca ++ , Mg ++ , Cl − ): normal
1.7 EKG
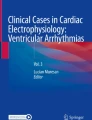
A routine EKG at rest was performed (Fig. 11.1).

12-lead ECG
The initial EKG showed sinus rhythm at 58 bpm, normal atrioventricular conduction (PR interval 160 s), normal QRS duration (0.08 s), absent Q wave, and horizontal QRS axis (+15°). Increased amplitude and duration (>0.04 s) of the terminal negative portion of P wave in V1. High-voltage QRS complexes. T-wave inversion in the left precordial leads, reciprocal ST-segment elevation, and tall T wave in the right precordial leads. ST-segment depression and T-wave inversion in lead I and aVL.
The Sokolow diagnostic criteria for left ventricular hypertrophy (LVH) were satisfied: R wave in V6 + S wave in V1 >3.5 mV.
Asymmetrical configuration of inverted T waves suggested a nonischemic origin.
Conclusion: sinus rhythm, normal conduction, possible left atrial enlargement, and left ventricular hypertrophy with secondary anomalies of repolarization
We hypothesized that the described palpitations were provoked by a hyperkinetic arrhythmia (supraventricular or ventricular), and we explored the different secondary causes of arrhythmic events:
-
Hyperthyroidism
-
Fever
-
Anxiety
-
Anemia
-
Use of medications containing stimulant, caffeine, or nicotine
-
Strenuous exercise, poor training
He did not report any specific stress condition or recent changes in his lifestyle. He was walking slowly, when the arrhythmia occurred, which therefore can be excluded a physiologic activity response and poor training. According to physical examination, fever was excluded, and the laboratory tests did not show any anemia and thyroid dysfunction.
The most probable cause of symptoms was spontaneous arrhythmia.
1.8 Transthoracic Echocardiography (TTE)
A TTE showed (Figs. 11.2, 11.3, and 11.4):

Parasternal long-axis view shows septal hypertrophy

Parasternal short-axis ventricle view

Apical four-chamber view
-
Left ventricular volumes at lower normal limits (iLVEDV 35 mL/m2) with massive asymmetrical hypertrophy with septal wall thickness that reached 35 mm; the posterior wall was 15 mm with a septum to posterior wall ratio of 2.4.
-
Ejection fraction with the biplane Simpson method was 65 % without regional wall motion abnormalities.
-
Diastolic dysfunction grade II with normal estimated filling pressure (E/E’ 6).
-
Severe left atrial enlargement (LA diameter 55 mm, iLAV >40 mL/m2).
-
Systolic anterior motion (SAM) of the anterior mitral valve leaflet, without LVOT obstruction at rest, but with mild flow acceleration during Valsalva (peak gradient 15 mmHg).
-
Normal size and function of right atrium and ventricle.
-
Normal aortic tricuspid valve with mild central regurgitation
-
Normal tricuspid and pulmonic valves.
-
Normal dimension of inferior vena cava (IVC) with >50 % inspiratory collapse.
-
No pericardial effusion.
According to ESC guidelines, HCM is defined as a wall thickness >15 mm in one or more LV myocardial segments, as measured by any imaging technique (echocardiography, cardiac magnetic resonance imaging (CMR), or computed tomography (TC)), that is not explained solely by chronic loading conditions.
Echocardiographic findings were suggestive of hypertrophic cardiomyopathy: the patient had no history of hypertension or valve disease with elevated afterload. Infiltrative cardiomyopathy was excluded, because the ventricular thickening is usually concentric with characteristic pattern of granular sparkling and different degrees of pericardial effusion.
In a patient with HCM, a sustained episode of palpitation lasting more than few minutes is often caused by supraventricular arrhythmias, especially in the presence of left atrium enlargement; atrial fibrillation is the most common arrhythmia in this population. In our patient, we could not exclude the hypothesis of a ventricular origin, particularly because the symptoms associated with palpitation (dyspnea and dizziness) could point to a hemodynamic distress that is often related to sustained ventricular tachycardias.
In adult patients with HCM, most recent data report on an annual incidence of cardiovascular death near 1–2 % with sudden cardiac death being (SCD) the most common.
Major clinical features associated with an increased risk of SCD are:
-
Young age
-
Non-sustained ventricular tachycardia (NSVT)
-
Maximum left ventricular wall thickness
-
Family history of sudden cardiac death
-
Syncope
-
Left atrial diameter
-
Left ventricular outflow tract obstruction
-
Exercise blood pressure drop
The patient had no family history of SCD and denied syncope, but the risk assessment comprised also of a 24-h ambulatory ECG and an exercise test.
1.9 Exercise Testing with Treadmill
Exercise testing was terminated for asthenia and muscular weakness at a heart rate corresponding to 93 % of maximal heart rate predicted for age. Neither symptoms nor ST-segment depression or elevation occurred. During exercise, arrhythmias were not detected except for two isolated polymorphic ventricular ectopic beats (VE) and one VE couple. Systolic blood pressure and heart rate response were normal.
1.10 24-h Ambulatory ECG
24-h ambulatory ECG was performed to detect atrial or ventricular arrhythmias. The total number of beats analyzed was 82,105. Sinus rhythm at average heart rate of 64 bpm, with minimum of 50 bpm and a maximum of 95 bpm. Two hundred fifty total ventricular ectopic (VE) beats of different morphologies with six VE couples and one NSVT (four beats at 150 bpm). Forty-three total supraventricular ectopic beats with one short run of 12 beats. No significant pauses.
NSVT is defined as ≥3 consecutive ventricular beats at ≥120 bpm lasting <30 s, so only one episode was detected.
In the absence of sustained arrhythmia, the electrophysiological study (EPS) is not specifically recommended.
1.11 Clinical Course
According to HCM guidelines, ICD implantation should be considered in patients with an estimated risk of SCD ≥6 % and a life expectancy of >1 year, and it may be considered in patients with an estimated risk between ≥4 and <6 %, while it is not recommended in patients with an estimated risk <4 % unless they have clinical features that are of proven prognostic importance.
Our patient’s estimated risk of sudden cardiac death at 5 years was 5 % (intermediate), based on severe cardiac hypertrophy and NSVT; that supported the indication for ICD implant in primary prevention.
The patient was informed about his SCD risk and the necessity of an ICD implant. He was made also aware on the risk of inappropriate shocks, implant complications, and the social and occupational implications of an ICD implant.
According to young age, primary prevention indication, good AV conduction, and patient’s preference, we scheduled a subcutaneous ICD (S-ICD) implantation.
At the preimplantation screening test, the patient presented the anatomical and electrocardiographic features ideal for a suitable subcutaneous sensing. An S-ICD was then implanted without complications.
1.12 Chest X-Ray
Chest X-ray was performed the day after implantation (Figs. 11.5 and 11.6).

Chest X-ray anterior-posterior (AP) projection

Chest X-ray lateral view
Conclusion: Correct position of the implanted S-ICD system
1.13 Therapy and Discharge
Because the episode of prolonged palpitation was his first and an S-ICD was implanted, we decided not to give antiarrhythmic therapy and maintained the calcium channel blockers (verapamil) in order to control LVOT gradient.
Moreover, at discharge, the patient was advised to abstain from competitive athletic activity and strenuous physical exertion and was given clinical and echocardiographic follow-up appointments.
2 Hypertrophic Cardiomyopathy
2.1 Introduction and Epidemiology
The most recent expert consensus on cardiomyopathies has adopted a new classification system no more based on primary or secondary involvement of the heart but in which cardiomyopathies are defined by specific morphological and functional phenotypes as they present for the first time to the observer: mainly hypertrophic, dilated, arrhythmogenic cardiomyopathy and restrictive phenotype. Only in the second time, cardiomyopathies are grouped into familial/genetic and nonfamilial/nongenetic subtypes, irrespective of the presence of extra-cardiac disease [1, 2, 3].
Hypertrophic cardiomyopathy (HCM) is defined by the presence of increased left ventricular (LV) wall thickness that is not solely explained by abnormal loading conditions. Many are the secondary causes of hypertrophy (in particular left ventricular hypertrophy) that should be considered in differential diagnosis:
-
1.
Athlete’s heart
-
2.
Hypertensive cardiomyopathy
-
3.
Valve diseases imposing increased afterload (mainly aortic stenosis)
-
4.
Isolated basal septal hypertrophy in elderly people
Moreover hypertrophic phenotype (variable grade and distribution of ventricular wall thickening) could represent a common picture of different pathologic conditions such as infiltrative disorders due to inborn errors of metabolism (e.g., Pompe disease, Fabry disease) or deposition of anomalous misfolded proteins (different types of amyloidosis). Other genetic causes could be mithocondrial diseases, neuromuscular disorders (Friedreich’s ataxia), or malformative syndromes like Noonan or LEOPARD [4].
The true hypertrophic cardiomyopathy is a genetic disease with an autosomal dominant trait caused by mutations in cardiac sarcomere protein genes. In general, patients with a sarcomere protein mutation present earlier and report a higher prevalence of family history of HCM and sudden cardiac death (SCD) than those without a mutation. They also tend to have more severe hypertrophy, microvascular dysfunction, and myocardial fibrosis.
2.2 Incidence
A number of studies worldwide report a prevalence of HCM in the range of 0.02–0.23 % in adults. In pediatric registries, the prevalence of HCM in children is unknown, but population-based studies report an annual incidence of 0.3–0.5 per 100,000. Most studies report a small male preponderance, while the prevalence in different racial groups is similar.
2.3 Diagnosis and Definition
-
In an adult, HCM is defined by a wall thickness ≥15 mm in one or more LV myocardial segments—as measured by any imaging technique such as echocardiography, cardiac magnetic resonance imaging (CMR), or computed tomography (CT)—that is not explained solely by loading conditions.
-
In children as in adults, the diagnosis of HCM requires a LV wall thickness more than two standard deviations greater than the predicted mean z-score.
-
The clinical diagnosis of HCM in first-degree relatives of patients with unequivocal disease (LVH ≥15 mm) is based on the presence of otherwise unexplained increased LV wall thickness ≥13 mm in one or more LV myocardial segments.
2.4 Variants
A particular variant is apical hypertrophic cardiomyopathy (AHCM) that is a rare form of HCM, which usually involves the apex of the left ventricle and rarely involves the right ventricular apex or both. Historically, this condition was thought to be confined to the Japanese population, but it is also found in other populations. Of all the HCM patients in Japan, the prevalence of AHCM was 15 %, whereas in the USA and Europe, the prevalence was only 3 %. The diagnostic criteria for AHCM included demonstration of asymmetrical LV hypertrophy, confined predominantly to the LV apex, with an apical wall thickness ≥15 mm and a ratio of maximal apical to posterior wall thickness ≥1.5. In contrast with the common variant of HCM, up to 54 % of patients with AHCM are symptomatic. This entity should be well known because of its difficult recognition (the apical position of hypertrophic segments represents a limitation for a routine 2D echocardiography) and its high prevalence of complications such as atrial fibrillation, myocardial infarction, apical aneurysm, embolic events, and congestive heart failure [5].
2.5 Differential Diagnosis
Genetic and nongenetic disorders causing hypertrophic phenotype can present with lesser degrees of wall thickening (13–14 mm); in these cases, the diagnosis of true HCM requires evaluation of other features including family history, noncardiac symptoms and signs, electrocardiogram (ECG) abnormalities, laboratory tests, and multimodality cardiac imaging. In any situation, the age of presentation is a fundamental clue to the differential diagnosis. Severe (maximal thickness more than 30 mm or equivalent in children) and concentric ventricular hypertrophy in a child, adolescent, or young adult should rise suspicion of metabolic or storage disorders, in particular Pompe disease in the infantile period and Danon disease in adolescent males. Different degrees of concentric hypertrophy with left ventricular systolic impairment is a clue to infiltrative diseases, because the hypokinetic end-stage phases of a true HCM more often pass through a dilation of left ventricle.
2.6 A New Diagnostic Tool: Cardiac Magnetic Resonance
Cardiac magnetic resonance (CMR) is particularly useful for characterizing the presence, location, and extent of LV hypertrophy, which can be limited to one or two left ventricle (LV) segments. In those cases, CMR offers a superior visualization and a higher diagnostic accuracy respect to 2D echocardiography, particularly when the only segments involved are the basal anterolateral free wall or the apex.
Recent study showed that diffuse hypertrophy, involving >50 % of the left ventricle and 8 or more segments, is present in 54 % of patients with HCM, whereas only 10 % of patients present with single segment involvement [6, 7].
During an exam directed to distinguishing the possible origin of a hypertrophic phenotype found with echocardiography, CMR could add diagnostic clues, demonstrating a constellation of suggestive features of genetic HCM: such as anomalies in papillary muscles, right ventricle, subclinical features, and particularly tissue characterization.
Papillary muscle involvement in HCM consists in apical displacement of its insertion and the presence of multiple or bifid papillary muscles with increased mass. All these variants could favor SAM and outflow tract obstruction perturbing the normal activity of mitral valve apparatus.
In 1/3 of patients with HCM, right ventricular wall thickness and/or mass is increased, including about 10 % of patient with extreme right ventricle (RV) wall hypertrophy (>10 mm). Finally in preclinical (genotype [+]/phenotype [−]) patients with HCM, CMR may show the presence of crypts. Myocardial crypt is a deep fissuring of the muscle orthogonal to the endocardial border (often visualized also in angiography), localized predominately in the inferior septum, although the etiology of these structural abnormalities remains uncertain.
Moreover, CMR is able to accurately define ventricular volume and function, being the gold standard for ejection fraction measurement. Frequently in patients with HCM, the ventricular volumes are reduced, and the hyperkinetic appearance of systolic contraction translates into a supernormal ejection fraction. This is true until the end stage of cardiomyopathy is reached, when the diastolic dysfunction, present from the beginning and related to myocardial thickness and rigidity, is accompanied by a reduced systolic thickening [8, 9, 10].
In 3-chamber view with cine imaging, CMR is able to elucidate the precise mechanism of outflow tract obstruction demonstrating turbulent flow generated by systolic movement of anterior mitral leaflet, chordae, and papillary muscle toward the interventricular septum [11].
Contrast-enhanced CMR with LGE sequences can detect areas of focal abnormality in approximately 50–80 % of patients. There is no specific pattern of LGE characteristic for HCM, although the distribution of LGE in HCM does not correspond to a coronary vascular territory. LGE is most often located in the most hypertrophied segment with an intramyocardial distribution (focal spot or linear deposit). Moreover, recent studies have demonstrated a significant association between the presence of LGE and ventricular tachyarrhythmias on ambulatory 24-h Holter electrocardiography. However, it is not clear whether the presence of LGE provides a strong predictive value in identifying patients with HCM at risk for sudden death, so much so the last ESC guidelines, published in 2014, do not include LGE in risk stratification algorithm [12–17].
2.7 Treatment
Treatment depends on disease expression, which can differ greatly among individuals, even within a single family. The natural history of hypertrophic cardiomyopathy includes those who remain asymptomatic and those who develop symptoms. The latter group can be further divided into those who develop outflow tract obstruction and those who do not.
Outflow tract obstruction at rest with exertional limitations is present in 25 % of all affected patients; an additional 25 % present inducible outflow tract obstruction; other groups of symptomatic patients are those with restrictive physiology and frequent tachyarrhythmias and who may experience exertional limitation because of diastolic dysfunction and those who are at risk or have already experienced ventricular arrhythmias and sudden cardiac death. At last, there is a small proportion of patients (up to 5 %) who may develop the end-stage phase of hypertrophic cardiomyopathy with left ventricular dilation and systolic impairment.
2.7.1 Left Ventricular Outflow Tract Obstruction
Treatment of outflow obstruction should be restricted to patients who exhibit the associated symptoms. Recognition of obstruction-related symptoms may be made challenging by both a patient’s restriction in physical activity and by the presence of latent obstruction (obstruction not present at rest but only under provocative conditions such as exercise, Valsalva maneuver). First-line therapy consists in pharmacologic approach with β-blockers or disopyramide to reduce left ventricular inotropism and to prolong diastolic filling time.
Patients who cannot tolerate or who are refractory to medical therapy are candidates for surgical or catheter-based treatment of outflow obstruction. In experienced centers, both procedures are associated with low rates of complications and high successful rate. There is debate over which procedure is best, but concerns are emerging about the potential for creation of an arrhythmogenic focus with percutaneous septal ablation, as well as the increased risk of complete heart block with that procedure. The routine performance of CMR after septal reduction therapy is not recommended, but it can be of value when questions arise about LV residual function or when gradients do not resolve or recur late after the procedure.
2.7.2 Ventricular Arrhythmias and Sudden Cardiac Death
Ventricular arrhythmias and sudden cardiac death remain dreaded outcomes of HCM, occurring in young, otherwise healthy individuals. Well-known clinical risk factors for sudden cardiac death allow clinicians to target implantable cardioverter defibrillator therapy to those who are at the highest risk. Not all risk factors predict this outcome equally, and placement of this type of device in young patients is associated with an important lifetime risk of complications [18–22].
A personal history of cardiac arrest or sustained ventricular arrhythmia is the most powerful risk factor. Multiple risk factors in an individual strengthen the case for an implantable defibrillator, as stated by the most recent international guidelines (Table 11.1).
References
Elliot PM et al (2014) 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy: the task force for the diagnosis and management of hypertrophic cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J 35(39):2733–2779
Maron BJ, McKenna WJ et al (2003) American college of cardiology/european society of cardiology clinical expert consensus document on hypertrophic cardiomyopathy. Eur Heart J 24:1965–1991
Rapezzi C, Arbustini E et al (2013) Diagnostic work-up in cardiomyopathies: bridging the gap between clinical phenotypes and final diagnosis. A position statement from the ESC working group on myocardial and pericardial diseases. Eur Heart J 34:1448–1458
Nagueh SF (2014) Anderson-fabry disease and other lysosomal storage disorders. Circulation 130:1081–1090
Yusuf SW, Bathina JD et al (2011) Apical hypertrophic cardiomyopathy. World J Cardiol 3(7):256–259
Nagueh SF, Bierig SM et al (2011) American society of echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with hypertrophic cardiomyopathy. J Am Soc Echocardiogr 24:473–498
To ACY, Dhillon A et al (2011) Cardiac magnetic resonance in hypertrophic cardiomyopathy. JACC Cardiovasc Imaging 4(10):1123–1137
Noureldin RA, Liu S et al (2012) The diagnosis of hypertrophic cardiomyopathy by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 14:17. http://www.jcmr-online.com/content/14/1/17
Pedrotti P (2013) La risonanza magnetica cardiaca nella cardiomiopatia ipertrofica. Cardiol Sci 11:70–81
Hundley WG, Bluemke DA et al (2010) ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Circulation 121:2462–2508
Ibrahim M, Rao C et al (2012) Modern management of systolic anterior motion of the mitral valve. Eur J Cardiothorac Surg 41(6):1–11
Maron MS, Houser TH et al (2007) Right ventricular involvement in hypertrophic cardiomyopathy. Am J Cardiol 100:1293–1298
Elliott PM, Anastasakis A et al (2014) ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy. Eur Heart J. doi:10.1093/eurheartj/ehu284
Ellims AH, Iles LM et al (2014) A comprehensive evaluation of myocardial fibrosis in hypertrophic cardiomyopathy with cardiac magnetic resonance imaging: linking genotype with fibrotic phenotype. Eur Heart J Cardiovasc Imaging 15:1108–1116
Kellman P, Hansen MS (2014) T1-mapping in the heart: accuracy and precision. J Cardiovasc Magn Reson 16:1–20
Maron SM (2012) Clinical utility of cardiovascular magnetic resonance in hypertrophic cardiomyopathy. J Cardiovasc Magn Reson 14:13
Shiozaki AA, Kim RJ (2007) Cardiovascular magnetic resonance in hypertrophic cardiomyopathy. Arq Bras Cardiol 88(2):216–221
Christiaans I, van Engelen K et al (2010) Risk stratification for sudden cardiac death in hypertrophic cardiomyopathy: systematic review of clinical risk markers. Europace 12:313–321
Bruder O, Wagner A et al (2010) Myocardial scar visualized by cardiovascular magnetic resonance imaging predicts major adverse events in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol 56:875–887
Maron MS, Appelbaum E et al (2008) Clinical profile and significance of delayed enhancement in hypertrophic cardiomyopathy. Circ Heart Fail 1:184–191
O’Hanlon R, Grasso A et al (2010) Prognostic significance of myocardial fibrosis in hypertrophic cardiomyopathy. J Am Coll Cardiol 56:867–874
Rubinshtein R, Glockner JF et al (2010) Characteristics and clinical significance of late gadolinium enhancement by contrast-enhanced magnetic resonance imaging in patients with hypertrophic cardiomyopathy. Circ Heart Fail 3:51–58
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Marchesini, M., Baiocco, E. (2015). Hypertrophic Cardiomyopathy. In: Capucci, A. (eds) Clinical Cases in Cardiology. Springer, Cham. https://doi.org/10.1007/978-3-319-19926-9_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-19926-9_11
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-19925-2
Online ISBN: 978-3-319-19926-9
eBook Packages: MedicineMedicine (R0)