
Key Points
-
Biomarkers in OA can be categorized using the BIPEDS classification: burden of disease, investigative, prognostic, efficacy of intervention, diagnostic, and safety.
-
Urine CTX-II and serum COMP seemed to have the best performance and promise of all commercially available OA biomarkers.
-
Identification and validation of panels of biomarkers correlated with imaging modalities may provide improved diagnosis, prediction, and understanding of the pathogenesis of OA.
-
Catabolic factors reflecting the degradation of cartilage joint tissue remain the most promising OA biomarkers and are awaiting validation in clinical trials.
-
Omics-based technology platforms, including DNA microarray, transcriptomics, proteomics, and metabolomics, are being increasingly applied in OA research and have identified significant amount of new potential OA biomarkers.
-
Aberrantly expressed miRNAs contribute to the pathogenesis of OA and could serve as potential therapeutic targets to treat OA, as well as diagnostic biomarkers.
-
Circulating miRNAs have emerged as a new class of minimally or noninvasive OA biomarkers due to their highly stability and ease of detection.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Biomarkers
- BIPEDS
- Inflammation
- C-reactive protein (CRP)
- Collagen type II degradation
- Cartilage oligomeric matrix protein (COMP)
- Genomics
- MicroRNAs
-
Biomarkers in OA can be categorized using the BIPEDS classification system: burden of disease, investigative, prognostic, efficacy of intervention, diagnostic, and safety.
-
Urine CTX-II and serum COMP have the best performance and promise of all commercially available OA biomarkers.
-
Identification and validation of panels of biomarkers correlated with imaging modalities may provide improved diagnosis, prediction, and understanding of the pathogenesis of OA.
-
Catabolic factors reflecting the degradation of cartilage joint tissue remain the most promising OA biomarkers and are awaiting validation in clinical trials.
-
Omics-based technology platforms, including DNA microarray, transcriptomics, proteomics, and metabolomics, are being increasingly applied in OA research and have identified significant amount of new potential OA biomarkers.
-
Aberrantly expressed miRNAs contribute to the pathogenesis of OA and could serve as potential therapeutic targets to treat OA, as well as diagnostic biomarkers.
-
Circulating miRNAs have emerged as a new class of minimally or noninvasive OA biomarkers due to their highly stability and ease of detection.
Introduction
The hallmark of osteoarthritis (OA) is progressive degradation of cartilage, leading to whole joint destruction and clinical symptoms of pain and loss of function [1]. The accepted gold standard diagnosis of OA is currently based on radiographic criteria, typically a Kellgren-Lawrence (K-L) grade ≥ 2 with pain and impairment of mobility [2]. However, radiographic measures have limitations with diagnosing and assessing the progression of OA, as radiographs indicate changes in bone and indirectly assess the progression of cartilage loss. Also, radiographic changes characteristic of OA appear after significant joint deterioration, and the change may occur relatively slowly with poor correlation with patient joint function [3]. Given these limitations, there has been considerable interest in the identification and development of biomarkers to quantify joint remodeling and disease progression.
The National Institutes of Health (NIH) defines a biomarker as a characteristic that is objectively measured and evaluated as an indicator of normal biologic processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention [4]. The term biomarker encompasses proteins, protein fragments, metabolites, carbohydrate biomarkers, genomic RNA and DNA biomarkers, cellular biomarkers, and imaging biomarkers [5]. In a systematic review of the literature in OA biomarkers, van Spil et al, identified 84 relevant publications covering 26 different biomarkers published up to 2010 [6].
The goal of biomarkers in OA is to measure and predict disease progression and outcome. Therefore, identifying OA biomarkers that can capture the full spectrum of the pathogenesis of OA is needed.
Classification of Osteoarthritis Biomarkers
In 2006, the NIH funded OA Biomarkers Network proposed a classification scheme for OA biomarkers represented by the acronym BIPED to connote the five categories of markers: Burden of Disease, Investigative, Prognostic, Efficacy of Intervention and Diagnostic [3]. Through the recent Osteoarthritis Research Society International (OARSI)/US Food and Drug Administration (FDA) initiative, the BIPED classification system added a sixth category, Safety of Interventions, to become BIPEDS [7]. The same OA biomarkers working group proposed to divide biomarkers in two major groups: wet biomarkers and dry biomarkers. The soluble or wet biomarkers are measured in blood, serum, plasma, urine, or synovial fluid and represent a modulation of endogenous substances in these fluids, whereas dry biomarkers consist of visual analog scales, performed tasks, or imaging [8].
Based upon the BIPEDS classification, Bauer et al. and Kraus et al. proposed the following clinical use of biological markers in OA [3, 7]. (a) Diagnostic markers : as indicated by Bauer et al., diagnostic markers are defined by the ability to classify individuals as either diseased or non-diseased with good positive and negative likelihood ratios and area under the curve in the receiving operator curve [3]. (b) Burden of disease markers: these markers assess the severity or extent of disease, typically at a single point in time, among individuals with OA [3]. (c) Prognostic markers: prognostic markers predict the future onset of OA among those without OA at baseline or the progression of OA among those with existing disease. These biomarkers may be used to determine risk in those without OA, clinical outcomes in individuals with OA, or the efficacy of potential new disease-modifying osteoarthritis drugs (DMOADs) [3]. (d) Efficacy of intervention markers: these biomarkers provide information about the efficacy of treatment among those with OA or those at high risk of developing OA. These biomarkers can be used in randomized controlled trials (RCTs) to evaluate short- and long-term changes associated with DMOADs [3]. (e) Investigative markers: as stated by Bauer et al., an investigative marker is one on which there is insufficient information to allow inclusion into one of the existing categories [3]. (f) Safety of intervention markers: finally, safety biomarkers provide information about exposure to new potential drugs, radiation, and contrast agents. These biomarkers are expected to be of increasing significance as new biomarkers are identified and studied [7].
Circulatory and Inflammatory Biomarkers
Increasingly, indicators of inflammation have gained credibility as OA biomarkers because they have been shown to predict outcomes in OA.
Adipokines (adiponectin and leptin) are emerging as modulators of joint disease by promoting and perpetuating the inflammatory response. Several studies have revealed associations between adipokines and joint disease. Perruccio and colleagues have shown a dose response association between overall painful joint burden and plasma levels of adipokines in individuals with hip and knee OA [9]. As well, plasma adiponectin levels have been reported to be significantly higher in individuals with OA compared to healthy controls [10]. In a recent study, serum leptin was found to correlate with the severity of knee OA [11]. In another study, the investigators reported a negative association between serum leptin levels and knee cartilage volume [12]. Stannus and associates reported a positive association between serum leptin and radiographic hip joint space narrowing [13].
The presence of high-sensitivity C-reactive protein (CRP) and interleukin 6 (IL-6) has been shown to predict outcomes in OA. In a group of 54 patients with idiopathic OA undergoing total hip and knee arthroplasty, increased synovial inflammation correlated with elevated plasma CRP levels [14]. In a cross-sectional study of 105 women with knee OA who were followed for 2 years, increased levels of CRP were found, which predicted disease progression in these patients compared to 740 women without OA [15]. Increased serum levels of CRP predicted cartilage loss associated with knee OA and poorer functional outcomes post total knee arthroplasty as well [16, 17]. Similar results have been reported for IL-6. In a study of 172 randomly selected patients followed over 3 years, baseline levels of serum IL-6 could predict loss of both medial and lateral tibial cartilage volume, and changes in IL-6 over 3 years were associated with changes in tibial cartilage volume [18]. In a study of 908 women who were followed prospectively for 15 years, Livshits and colleagues reported that prevalent radiographic OA was significantly associated with both increased circulating levels of CRP and IL-6, and incident radiographic OA was significantly predicted by IL-6 [19]. In another study of 161 patients with knee OA followed over 2 years, baseline levels of CRP and IL-6 predicted cartilage volume loss in the medial compartment of the knee [20]. The predictive value of baseline CRP and IL-6 levels on cartilage volume loss was possibly related to the fact that both are known inflammatory biomarkers. Synovitis, followed over 1 year arthroscopically in 422 patients, was a potential predictive factor of rapid progression of cartilage lesions in the medial tibiofemoral compartment [21].
These studies show the involvement of inflammatory biomarkers in OA pathogenesis and support the association between inflammation and joint disease (Table 9.1).
Catabolic Osteoarthritis Biomarkers
A hallmark feature of OA pathology is the higher rate of cartilage degradation than cartilage synthesis, leading to chronic cartilage loss. Cartilage, composed of chondrocytes and the extracellular matrix (ECM), is a connective tissue possessing unique biological and mechanical properties which supports its load-bearing function [22]. The dry weight of cartilage is mainly made of type II collagen and some type I, along with certain amount of proteoglycans and integral proteins. Fragments of these components generated during cartilage degeneration can be released into the bloodstream, synovial fluid, and urine and therefore be utilized as biomarkers [23].
C-Telopeptides of Type II Collagen
Since type II collagen is the major collagen type and most abundant protein in cartilage, C-terminal telopeptides of type II collagen (CTX-II), a catabolic product of type II collagen, has become the widely accepted biomarker for assessing collagen breakdown [24]. Urinary levels of CTX-II (uCTX-II) have been used as a marker for cartilage metabolism, disease severity, and monitoring drug response in OA patients [25–27]. Reijman et al. studied the association between the concentration of uCTX-II and the prevalence and progression of radiographic OA of the knee and hip. The 1,235 subjects were 55 years of age and older and were followed for 6.6 years on average. They found that subjects with a uCTX-II level in the highest quartile had a 4.2-fold increased risk of having radiographic knee or hip OA, compared with subjects with a uCTX-II level in the lowest quartile. Furthermore, subjects with an uCTX-II level in the highest quartile had a 6.0-fold increased risk for progression of radiographic knee OA at the knee and an 8.4-fold increased risk for progression of radiographic hip OA. In addition to its strong correlation with radiographic OA, another advantage of uCTX-II or serum CTX-II is that it is noninvasive. However, as collagen type II breakdown correlates with radiographic features of OA, the use of uCTX-II as a pre-radiographic diagnostic biomarker is limited. Additional biomarkers originated from collagen type II include cleavage of collagen type II triple helix (C2C), triple helix collagen type II cleavage (Coll2-1), nitrated form of Coll2-1 (Coll2-1NO2), collagen type II propeptides (PIINP, PIIANP, PIIBNP, PIICP, CPII), and collagen type I and II cleavage neoepitope (C1, C2). These additional collagenous biomarkers either provide complementary information on collagen type II catabolism or help to distinguish subtypes of OA [28]. For example, Coll2-1 and Coll2-1NO2 are more useful for studying oxidative stress-related collagen II degradation in OA [29, 30].
Cartilage Oligomeric Matrix Protein
Cartilage oligomeric matrix protein (COMP) is a structural glycoprotein binding to and stabilizing type I, II, and IX collagen fibers, fibronectin, and aggrecan [31]. COMP has been considered as an OA biomarker and has been tested in OA diagnosis, prognosis, and therapeutic intervention. Many large population studies have shown that serum COMP (sCOMP) levels correlated with cartilage degradation and disease severity. In the Johnston County OA Project involving 143 patients with radiographic knee OA and 148 healthy controls, a significant elevation of sCOMP levels were detected in the OA group compared to controls. Moreover, sCOMP levels were upregulated with knee OA K-L grade and the number of joints involved [32]. Sharif et al. suggested the use of sCOMP levels to predict OA progression. In this longitudinal study lasting 5 years, 115 patients with OA were grouped as nonprogressors and progressors defined by either a reduction in the tibiofemoral joint space width by at least 2 mm or total knee arthroplasty at follow-up. They found that the chance to have radiographic OA progression was increased by 15 % with every 1 unit increase in sCOMP levels [33]. The existence of COMP fragments and their release into the culture medium were also confirmed recently which may provide complement to total COMP in use as biomarkers [34].
Hyaluronic Acid
Hyaluronic acid (HA) is a common component of most connective tissues, as well as a principal component of the synovial fluid. During the degenerative process, HA is secreted by the synovium and cartilage. Serum levels of HA were proposed to be a marker to predict the progression of knee OA [35]. OA patients had increased serum HA (sHA), and patients with higher initial sHA values displayed a more rapid progression of the disease [36, 37]. More recent studies also suggested that sHA can be available as a burden of disease marker for patients with radiographic or severe OA [38, 39]. The major problem associated with HA as an OA biomarker is its specificity and sensitivity, as HA is ubiquitously present in all connective tissues and tends to be affected by physical activities and food intake [40].
Despite the existence of multiple catabolic biomarkers in research, currently, there is no single biomarker validated for clinical use for OA. Given the unique advantages and disadvantages of these biomarkers, combined use of different biomarkers might be of benefit in the future (Table 9.2). Also, majority of the abovementioned biomarkers are systemic, for example, from serum or urine, and their concentrations are subject to systemic conditions or illnesses. Therefore, obtaining local biomarkers from synovial fluid may provide more specificity and sensitivity. Moreover, local biomarkers would ensure the ability to detect OA in a particular joint.
Post-Genomic Osteoarthritis Biomarkers
Following completion of the Human Genome Project, the generation of massive genomic information has rapidly transformed the field of biomedical research into the post-genomic era [41]. Post-genomics, or so-called system biology, studies the expression and functions of the entire set of genes and proteins present in a whole genome by using high-throughput methodologies including microarray, transcriptomics, proteomics, and metabolomics. With thousands of genes and proteins being analyzed simultaneously, these omics-based technology platforms have significantly contributed to the discovery of the new crop of biomarkers over the past decade [42]. The post-genomic strategies have been applied in various fields, including OA.
Transcriptomic Osteoarthritis Biomarkers
Transcriptome refers to all the ribonucleic acids (RNAs) that are transcribed from the genome containing messenger RNAs (mRNAs), ribosomal RNAs (rRNAs), transfer RNAs (tRNAs), and noncoding RNAs. Transcriptomic analysis has been performed through gene microarrays or RNA sequencing (RNA-Seq) to quantify the abundance of all transcripts in a particular biological specimen [43].
Gene microarrays have been widely used in gene expression studies and have proven to be a powerful tool to identify candidate RNA biomarkers for various pathological conditions including OA. Geyer et al. performed a transcriptomic analysis of affected versus intact articular cartilage from the same joint using high-density synthetic oligonucleotide hybridization arrays (HG-U133 Plus 2.0 GeneChips), and 411 transcripts out of 54,675 probes appeared to be differentially expressed. Of these, 6 genes were upregulated in the affected cartilage of all patients, including insulin-like growth factor-binding protein 3 (IGFBP-3), Wnt-1-inducible signaling protein 1 (WISP-1), aquaporin 1 (AQP-1), delta/notch-like EGF-repeat containing transmembrane (DNER), decay-accelerating factor (DAF), and complement factor I [44]. The Research Arthritis and Articular Cartilage (RAAK) study which involved a larger patient cohort was carried out to determine the genome-wide gene expression in 33 pairs of matched OA affected and intact cartilage from the same joint of patients. About 1,717 genes were found to be differentially expressed, and 18 were present with a change of twofold or higher in OA affected cartilage compared with preserved cartilage.
Comparing gene expression at damaged focal areas of cartilage to those preserved areas provides information of dynamic changes of genes and pathways involved in OA progression [45]. However, macroscopic assessment of damaged or preserved cartilage is relatively subjective and less accurate, which may partially explain the low consistency of the differentially expressed genes between studies with similar design using comparable tissues. Xu et al. identified 998 differentially expressed genes between femoral neck fractures and cartilage from hip OA patient using the Illumina Human HT-12 V3 microarrays. These target genes were enriched within 71 canonical pathways and showed excellent correlation with previous studies using similar tissues but revealed discord between hip and knee OA, indicating different mechanisms may be present for knee and hip OA pathophysiology [46].
The RNA-Seq transcriptome platform, as a relatively new technology still at the development stage and due to high costs, has just started to be applied in OA research. In a study, RNA sequence libraries were prepared from normal cartilage of the metacarpophalangeal joints from 4 young (4 years old) and 4 old (>15 years old) horses, and sequencing was undertaken using the Illumina HiSeq platform. Levels of 396 transcripts, including noncoding RNAs, were significantly different in old compared to young cartilage. The majority of cartilage genes relating to ECM, proteases, matrix synthetic enzymes, cytokines, and growth factors, as well as Wnt signaling, were reduced in old cartilage relative to young cartilage. As aging is an important risk factor of OA, altered expressions of transcripts identified in old cartilage could provide valuable information to understand the pathogenesis of OA [47].
Blood samples have also been subject to transcriptomic analysis in OA. A complementary DNA (cDNA) microarray was used to screen for differentially expressed genes in 85 subjects with mild OA and 76 controls. Six genes were significantly downregulated in mild OA: heat shock 90 kDa protein 1, alpha; inhibitor of kappa light polypeptide gene enhancer in B cells, kinase complex-associated protein; interleukin 13 receptor, alpha 1; laminin, gamma 1; platelet factor 4 (also known as chemokine (C-X-C motif) ligand 4); and tumor necrosis factor, alpha-induced protein 6. A nine-gene signature (abovementioned six genes plus early growth response 1; alpha glucosidase II alpha subunit; and v-maf musculoaponeurotic fibrosarcoma oncogene homologue B) was identified as a diagnostic biomarker to discriminate mild OA from controls, with a higher diagnostic capacity than any of the individual nine genes [48]. Another transcriptomic screen of peripheral blood leukocytes from patients with symptomatic knee OA and controls identified 173 abnormally expressed genes. Cluster analysis revealed 2 distinct OA subgroups: those with or without the interleukin 1-beta (IL-1β) signature, defined as ≥2 fold IL-1β overexpression. Patients with IL-1β signature had more pain, decreased function, and higher risk of radiographic progression of OA [49]. This study suggested a novel method to classify OA based on IL-1β expression and moreover that the transcriptomic profile of peripheral blood leukocytes had the potential as a prognostic biomarker for OA patients.
Transcriptome analysis has generated valuable information on the molecular changes across the whole genome, which will improve our understanding of the complexity of OA phenotypes. With the popularization of the powerful RNA-Seq platform, the discovery of multiple panels of new OA biomarkers is warranted.
Proteomics Biomarkers
By studying the presence and functions of an entire set of proteins in a particular biological sample, proteomics is being increasingly applied in cartilage research and OA pathology [50]. It also elucidates information regarding protein structure and interactions, thereby providing mechanistic insight into disease pathogenesis and a new powerful tool for biomarker exploration. In OA research, proteomic studies have been applied to cartilage tissue, chondrocytes, synovial fluid, serum, urine, and culture supernatant, and have identified significant panels of novel candidate biomarkers [51].
Wu et al. measured the protein compositions in cartilage from OA and healthy donors and found 59 differently expressed proteins by liquid chromatography–mass spectrometry. In particular, HtrA1, a serine protease, was upregulated at high levels in OA cartilage [52]. Another study by Guo et al. performed proteomics on cartilage extractions from individuals with and without OA and identified 16 differentially expressed proteins which belonged to the following five function groups including glycolysis and energy production (ADH, ADK, ENOA, KPYM, and FR), signaling (ANNX-I, PEBP, and TUB), redox (PRDX3 and SODM), and cartilage matrix (COLL-I and COLL-VI) [53]. Proteomic profiling of chondrocytes also revealed that 19 proteins were increased and 9 decreased significantly in OA cells compared to normal. Among these, three stress response proteins (HSP90beta, GRP78, and GRP94) were upregulated and three glycolysis-related proteins (enolase, glyceraldehyde 3-phosphate dehydrogenase, and fructose biphosphate aldolase) were downregulated [54]. This study indicated an impaired glycolytic metabolism and an increased stress response in OA chondrocytes, both of which have been reported previously to be implicated in cartilage degradation [55, 56].
With the goal of searching for new OA biomarkers, intensive proteomic profiling studies have focused on bodily fluids from OA and non-OA individuals. Fernandez-Puente et al. measured protein levels in serum from 50 moderate OA patients, 50 severe OA patients, and 50 non-symptomatic controls using isobaric tags for relative and absolute quantitation (iTRAQ) and matrix-assisted laser desorption/ionization (MALDI)-TOF/TOF mass spectrometry. They identified 349 total proteins in serum, and of these, 6 were modulated only in moderate OA, 13 only in severe OA, and 7 in both groups. In addition to COMP, most of these differentially expressed proteins were novel candidate biomarkers for OA including a few complement components, lipoproteins, von Willebrand factor, tetranectin, and lumican [57]. Han et al. analyzed synovial fluid samples from 36 OA patients and 24 rheumatoid arthritis (RA) patients. Three protein peaks were identified and able to differentiate between OA and RA patients at a sensitivity of 89.4 % and a specificity of 91.2 % by artificial neural networks analysis. One peak was identified as S100A12 which was also reported to be upregulated in human OA elsewhere [58]. Ritter et al. performed a proteomic analysis of knee synovial fluid from 20 OA patients and 10 controls. Sixty-six proteins were differentially present in both OA and control synovial fluid. Analysis showed that these proteins were associated with the acute-phase response pathway, the complement pathway, and the coagulation pathway [59]. The complement pathway has been identified in numerous studies to play a critical role in the pathogenesis of OA and a potential biomarker [60].
While a considerable amount of candidate protein markers have been identified from proteomic studies, the studies are not sufficiently consistent. For example, there was less than 25 % reliability of the synovial fluid protein list between Ritter et al. and Kamphorst et al. studies [59, 61]. However, proteomics has emerged as a powerful approach to identify proteins in pathological conditions and to discover new potential biomarkers.
Metabolomic Biomarkers
Metabolomics, defined as large-scale profiling of small molecular metabolites present in a cell, tissue, body fluids, or any biological system, has opened new avenues for biomarker identification [62]. Metabolites include various low-molecular end products of diverse cellular processes, such as lipids, amino acids, peptides, vitamins, organic acids, carbohydrates, and nuclear acids. The levels of metabolites are considered to be the ultimate response of biological systems to genetic, environmental, and lifestyle factors under normal or diseased states. Current commonly used methods for studying metabolomics are nuclear magnetic resonance and mass spectrometry, along with gas chromatography, liquid chromatography, or capillary electrophoresis for sample separations.
Zhai and coworkers utilized targeted metabolite profiling to investigate the association of metabolite ratios in serum with the development of knee OA. They found 14 ratios that were significantly associated with knee OA at discovery stage in their cohort. By replicating this study in the Chingford cohort, two of these 14 ratios (valine/histidine and xleucine/histidine) were successfully confirmed to correlate with radiographic severity of OA. Mechanically, as these branched-chain amino acids (BCAAs) including valine and xleucine could not be synthesized by the body, an increase in BCAAs metabolites implied the breakdown of collagen [63]. This was the first study using serum-based metabolomics and demonstrated that the BCAAs to histidine ratio have potential clinical use as an OA biomarker.
Jiang et al. reported a mass spectrometry-based metabolic study to identify the global metabolic defects in the serum of four major types of arthritis including RA (n = 27), OA (n = 27), ankylosing spondylitis (n = 27), and gout (n = 33) compared with healthy control subjects (n = 60). They identified a global metabolic profile in all arthritic patients, suggesting these four types of arthritis share common metabolic defects possibly resulting from joint inflammation. Meanwhile, a unique metabolic signature, potential biomarker for diagnosis, was discovered for each type of arthritis. This report demonstrated the applicability of metabolomic profiling as a novel diagnostic tool for arthritis including OA, along with current clinical detection methods [64]. Another group conducted a global metabolite profiling of conditioned medium of synovial tissue cultures from patients with severe OA or non-OA patients undergoing ligament or meniscal repair. They identified 13 compounds significantly elevated in the end stage OA group [65]. Given the difficulty in translating synovium culture method into clinical practice, they also performed metabolomics on ankle synovial fluid of patients with and without ankle OA. One hundred and six metabolites were significantly elevated in the OA sample, representing abnormalities in almost all pathways involving metabolism including amino acid, carbohydrate, mitochondrial oxidation, lipid, peptide, vitamin, nucleotide synthesis, and redox homeostasis [66].
Taken together, these studies have linked abnormal metabolic changes to the pathogenesis of OA, and metabolomics have proven to be a new robust tool for biomarker discovery in OA. This is in accordance with the emerging new subtype of OA, metabolic syndrome OA, which has recently been recognized because of the increased incidence of OA in patients with metabolic syndrome such as dyslipidemia, hypertension, obesity, and type 2 diabetes. Therefore, biomarkers identified by metabolomics will also help discriminate between different OA subtypes.
MicroRNAs Biomarkers in Osteoarthritis
MicroRNA and Its Biogenesis
MicroRNAs (miRNAs) belong to the family of small noncoding RNAs, about 19–23 nucleotides long when eventually processed as functioning mature miRNA. Though not coding for proteins, miRNAs play important roles in regulating gene expression at the posttranscriptional level through complementary base-pairing within 3’ untranslated region (3’UTR) of target mRNA [67]. According to miRNA databases, the targeting strategy between miRNAs and mRNAs is not simply a one to one relationship, rather, one mRNA can be synergistically targeted by multiple miRNAs or a single miRNA can target multiple genes [68, 69]. There are more than 2,000 annotated miRNAs from the human genome and the number is still increasing. It is estimated that human miRNAs regulate as much as 60 % of genes and play pivotal roles in various physiological processes such as cell proliferation, differentiation, genomic stability, metabolism, apoptosis, and aging. Not surprisingly, deregulation of miRNA has been associated with many pathological conditions including OA [70].
There are three forms of miRNAs which are long primary miRNAs (pri-miRNA), hairpin precursor miRNAs (pre-miRNA), and short mature miRNAs. In the nucleus, the miRNA gene is transcribed into large pri-miRNA which is subsequently cleaved by Drosha, an RNase III enzyme, to make pre-miRNA. Pre-miRNA is a 70–125 nucleotide long hairpin structure with 2 nucleotides overhanging at the 3’ end. It is then exported by RanGTP and exportin5 proteins into the cytoplasm where it is processed by a second RNase III enzyme Dicer, to form the short mature miRNA. At this point, it is incorporated into an RNA-induced silencing complex to induce target mRNA degradation and protein translation depression [71].
MicroRNA Biomarkers in Joint Tissues
The critical role of miRNA regulation during skeletal development has been highlighted by a study with Dicer-null mice where chondrocytes from these mice displayed reduced proliferation and accelerated differentiation into cell hypertrophy [72].
MiR-140 is the most studied miRNA involved in OA. It was first reported as cartilage-specific miRNA in mouse and directly targeted HDAC4 [73]. Microarray profiling by Miyaki et al. discovered that miR-140 was upregulated during chondrogenesis but downregulated in OA chondrocytes compared to normal [74]. A further study demonstrated that IL-1β treatment of normal chondrocytes suppressed miR-140 expression, while overexpression of miR-140 downregulated IL-1β-induced ADAMTS5 expression and rescued the IL-1β-dependent repression of AGGRECAN gene expression. An additional study in vivo in mice by the same group showed that MiR-140-null mice developed age-related OA-like phenotypes, including proteoglycan loss and articular cartilage fibrillation. The crucial role of miR-140 in OA cartilage protection was further demonstrated by resistance to antigen-induced arthritis through miR-140 overexpression [75]. Meanwhile, another group identified matrix metalloproteinases-13 (MMP-13) and insulin-like growth factor-binding protein 5 as two more targets for miR-140 [76]. NFAT3 and SMAD3 seemed to activate and repress miR-140 expression respectively, providing novel strategies for treating OA [77].
Similar as miR-140, miR-27b has been shown to be downregulated in IL-1β-stimulated OA chondrocytes. MiR-27b directly targeted MMP-13, indicating that decreased miR-27b might be responsible for the overexpression of MMP-13 in response to IL-1β [78].
Yamasaki et al. reported expression of miR-146a in early-stage OA cartilage compared to normal. Interestingly, miR-146a levels were decreased in later stage OA when Mankin scores were increased [79]. MiR-146a is inducible by IL-1β stimulation in normal human chondrocytes, by lipopolysaccharide in THP-1 cells and by mechanical pressure injury [79–82]. MiRNA-146a has also been linked to pain by modulating inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), COX-2, iNOS, IL-6, IL-8, RANTS, and ion channel TRPV1. Therefore, miRNA-146a may serve as target for therapeutic intervention to alleviate OA-related pain [83, 84].
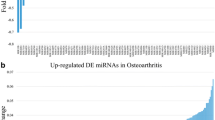
Using human miRNA qPCR array, a few studies have examined the expression of hundreds of miRNAs in chondrocytes, cartilage, or bone tissue. Iliopoulos et al. measured the expression of 352 miRNAs in OA versus normal cartilage. They found that 16 miRNAs were deregulated in OA cartilage and were able to distinguish OA chondrocytes from normal chondrocytes. Among these, nine miRNAs were upregulated and seven downregulated. Interestingly, levels of five miRNA (miR-22, miR-103, miR-25, miR-337, and miR-29a) statistically correlated with body mass index (BMI), suggesting the potential role of these miRNA in lipid metabolism and OA pathology [85]. In another study, Jones and associates identified that some miRNAs were differentially expressed in late-stage human OA, 17 in cartilage, and 30 in bone. Further functional analysis revealed that miR-9, miR-98, and miR-146 might play a role in inflammatory regulation mediating IL-1β-induced TNF-α production and MMP-13 secretion [81]. Another study conducted a profiling of 723 miRNAs in cultured chondrocytes and discovered 1 upregulated (has-miR-483-5p) and 6 downregulated (hsa-miR-149, hsa-miR-582-3p, hsa-miR-1227, hsa-miR-634, hsa-miR-576-5p, hsa-miR-641) miRNAs in OA chondrocytes versus controls [86].
Given the essential regulatory roles of miRNAs in mRNA stability and protein translation, identification of differentially expressed miRNAs in OA joint tissue will deepen our understanding of the mechanism underlying cartilage degradation and OA pathology. Moreover, aberrantly expressed miRNAs involved in the pathogenesis of OA could serve as potential therapeutic targets to treat OA, as well as diagnostic biomarkers.
Promising Circulating MicroRNA Biomarkers
Majority of miRNAs exist and function intracellularly; however, non-tissue and cell-free circulating miRNAs are also present in extracellular compartments in all tested body fluids such as serum, plasma, synovial fluid, urine, cerebrospinal fluid, and saliva [87]. Unlike mRNA and other nuclear acids, miRNAs in human plasma and serum are highly stable and protected from ribonuclease digestion [88]. In addition to its stability, other distinct advantages associated with using miRNAs as biomarkers include high sensitivity, easy accessibility, and detection. Therefore, attention has been drawn to the development of circulating miRNAs as clinical biomarkers in OA [89–90].
In 2010, Murata et al. first investigated the presence of miR-16, miR-132, miR-146a, miR-155, and miR-223 in plasma and synovial fluid, as well as their high stability under multiple freezing–thawing cycles [91]. They found that both synovial fluid and serum miRNAs were quite stable for storage at −20 °C and were still stable after as many as eight freeze–thawing cycles from −20 to 4 °C. The concentrations of the five miRNAs in synovial fluid were found to be much lower than those in plasma in both OA and RA patients. In addition, there was no correlation between plasma and synovial fluid miRNAs. Finally, the authors reported that the levels of miR-132 in plasma of both OA and RA were significantly reduced compared to normal [64].
Subsequently, a 3 miRNAs signature consisting of miR-454, miR-885-5p, and let-7e was identified in serum which could predict the risk of developing severe knee or hip OA [92]. This study followed 816 individuals over a 15-year period and assessed the occurrence of severe knee or hip OA using total knee or hip arthroplasty, with at least one joint as a definitive outcome. At follow-up, 67 individuals had developed severe knee or hip OA. In the initial screening, Taqman qPCR array analyses of 377 miRNAs were performed in 13 individuals with severe OA versus 13 controls matched for sex, menopausal status, age, and BMI. Screening results revealed that 12 miRNAs were differentially expressed, which were subsequently validated in the entire cohort by Taqman qPCR. Validation showed that miR-454, miR-885-5p, and let-7e were strongly associated with the development of severe OA. Let-7e appeared to be the most promising biomarker to predict severe OA. Another study identified 12 differentially expressed miRNAs in the plasma of 54 patients with primary OA at early and intermediate stages (stages 2 and 3, respectively), indicating the value of these miRNAs as disease progression markers. Analysis showed that these miRNAs could regulate mRNAs that are crucial in chondrocyte maintenance and differentiation, including SMAD1, IL-1β, COL3A, VEGFA, and FGFR1 [93].
The origin and functions of circulating miRNAs remain largely unknown. It is widely believed that these miRNAs might be released directly from blood cells into the bloodstream or from circulating cells from damaged tissue at disease states [94]. Murata et al. also reported that the expression patterns of four miRNAs (miR-16, miR-132, miR-146a, and miR-223) in synovial fluid are similar to those in synovial tissue from OA patients, suggesting that synovial tissue might release miRNAs directly into the surrounding extracellular environment through an unknown mechanism [91]. Currently, it is not clear if the secretion of miRNA from synovial tissue is certain miRNA selective or is merely a universal mechanism for all miRNAs. Further studies are also required to clarify the correlation of circulating miRNAs in synovial fluid to OA disease activity as well as to explore the feasibility of use circulating miRNAs as biomarkers in clinical practice (Table 9.3).
Conclusions
Despite much active research into various OA biomarkers, there is no single biomarker that is sufficiently well validated and recognized to diagnose OA or aid the progression of individuals with or without OA [95]. In a systematic review applying the BIPED classification, van Spil and associates indicated that uCTX-II and serum COMP seemed to have the best performance and promise of all commercially available OA biomarkers [6]. However, the authors commented on the current limitations of OA biomarker studies including an overall lack of consistent evidence, differences between the clinical trial populations versus population-based cohort studies, and differences in sample collection and possible publication bias [6]. Presently, no OA biomarker is consistent to function as an OA outcome measure in clinical trials as a secondary or supportive endpoint [96]. As a result, the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) convened a meeting in October of 2012 to discuss the direction of future research in OA biomarkers. The ESCEO group outlined 3 areas of future research including mechanisms of disease and development of new biomarkers, assays and technological development, and prognosis and risk. Briefly, ESCEO discussed research into the underlying mechanism of disease to validate existing biomarkers and identify new candidates, improve assays and standardize protocols that can accurately and reproducibly measure OA biomarkers in serum or urine, and identify biomarkers for early stages of OA so treatments can be started to slow down the progression of OA [95]. Furthermore, future research advancements and refinements in genetic, proteomic, and metabolomics approaches, as well as identification and validation of panels of biomarkers that may be correlated with imaging modalities, may provide improved diagnosis, prediction, and understanding of the pathogenesis of OA [97]. Today, there remains a need for more active research in the area of OA biomarkers.
References
Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice. Lancet. 2011;377:2115–26.
Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, et al. Development of criteria for the classification and reporting of knee osteoarthritis. Arthritis Rheum. 1986;29(8):1039–49.
Bauer DC, Hunter DJ, Abramson SB, et al. Classification of osteoarthritis biomarkers: a proposed approach. Osteoarthritis Cartilage. 2006;14:723–7.
Atkinson AJ, Colburn WA, DeGruttola VG, Biomarkers Definitions Working Group, et al. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther. 2001;69:89–95.
De Gruttola VG, Clax P, DeMets DL, Downing GJ, Ellenberg SS, Friedman L, et al. Considerations in the evaluation of surrogate endpoints in clinical trials. Summary of a National Institutes of Health workshop. Control Clin Trials. 2001;22(5):485–502.
van Spil WE, Degroot J, Lems WF, et al. Serum and urinary biochemical markers for knee and hip-osteoarthritis: a systematic review applying the consensus BIPED criteria. Osteoarthritis Cartilage. 2010;18:605–12.
Kraus VB, Nevitt M, Sandell LJ. Summary of the OA biomarkers workshop 2009–biochemical biomarkers: biology, validation, and clinical studies. Osteoarthritis Cartilage. 2010;18(6):742–5.
Kraus VB, Burnett B, Coindreau J, Cottrell S, Eyre D, Gendreau M, et al. Application of biomarkers in the development of drugs intended for the treatment of osteoarthritis. OARSI FDA Osteoarthritis Biomarkers Working Group. Osteoarthritis Cartilage. 2011;19(5):515–42.
Perruccio AV, Mahomed NN, Chandran V, Gandhi R. Plasma adipokine levels and their association with overall burden of painful joints among individuals with hip and knee osteoarthritis. J Rheumatol. 2014;41(2):334–7.
Laurberg TB, Frystyk J, Ellingsen T, Hansen IT, Jorgensen A, Tarp U, et al. Plasma adiponectin in patients with active, early, and chronic rheumatoid arthritis who are steroid- and disease-modifying antirheumatic drug-naive compared with patients with osteoarthritis and controls. J Rheumatol. 2009;36:1885–91.
Staikos C, Ververidis A, Drosos G, Manolopoulos VG, Verettas DA, Tavridou A. The association of adipokine levels in plasma and synovial fluid with the severity of knee osteoarthritis. Rheumatology. 2013;52:1077–83.
Ding C, Parameswaran V, Cicuttini F, Burgess J, Zhai G, Quinn S, et al. Association between leptin, body composition, sex and knee cartilage morphology in older adults: the Tasmanian older adult cohort (TASOAC) study. Ann Rheum Dis. 2008;67:1256–61.
Stannus OP, Jones G, Quinn SJ, Cicuttini FM, Dore D, Ding C. The association between leptin, interleukin-6, and hip radiographic osteoarthritis in older people: a cross-sectional study. Arthritis Res Ther. 2010;12:R95.
Pearle AD, Scanzello CR, George S, Mandl LA, DiCarlo EF, Peterson M, et al. Elevated high-sensitivity C-reactive protein levels are associated with local inflammatory findings in patients with osteoarthritis. Osteoarthritis Cartilage. 2007;15:516–23.
Spector TD, Hart DJ, Nandra D, et al. Low-level increases in serum C-reactive protein are present in early osteoarthritis of the knee and predict progressive disease. Arthritis Rheum. 1997;40:723–7.
Sharif M, Shepstone L, Elson CJ, et al. Increased serum C reactive protein may reflect events that precede radiographic progression in osteoarthritis of the knee. Ann Rheum Dis. 2000;59:71–4.
Smith JW, Martins TB, Gopez E, et al. Significance of C-reactive protein in osteoarthritis and total knee arthroplasty outcomes. Ther Adv Musculoskelet Dis. 2012;4:315–25.
Stannus O, Jones G, Cicuttini F, et al. Circulating levels of IL-6 and TNF-alpha are associated with knee radiographic osteoarthritis and knee cartilage loss in older adults. Osteoarthritis Cartilage. 2010;18:1441–7.
Livshits G, Zhai G, Hart DJ, Kato BS, Wang H, Williams FMK, et al. Interleukin-6 is a significant predictor of radiographic knee osteoarthritis: the Chingford Study. Arthritis Rheum. 2009;60:2037–45.
Pelletier JP, Raynauld JP, Caron J, Mineau F, Abram F, Dorais M, et al. Decrease in serum level of matrix metalloproteinases is predictive of the disease-modifying effect of osteoarthritis drugs assessed by quantitative MRI in patients with knee osteoarthritis. Ann Rheum Dis. 2010;69(12):2095–101.
Ayral X, Pickering EH, Woodworth TG, et al. Synovitis: a potential predictive factor of structural progression of medial tibiofemoral knee osteoarthritis – results of a 1 year longitudinal arthroscopic study in 422 patients. Osteoarthritis Cartilage. 2005;13:361–7.
Goldring SR, Goldring MB. Clinical aspects, pathology and pathophysiology of osteoarthritis. J Musculoskelet Neuronal Interact. 2006;6(4):376–8.
Garvican ER, et al. Biomarkers of cartilage turnover. Part 1: Markers of collagen degradation and synthesis. Vet J. 2010;185(1):36–42.
Jayabalan P, Sowa GA. The development of biomarkers for degenerative musculoskeletal conditions. Discov Med. 2014;17(92):59–66.
Christgau S, et al. Collagen type II C-telopeptide fragments as an index of cartilage degradation. Bone. 2001;29(3):209–15.
Reijman M, et al. A new marker for osteoarthritis: cross-sectional and longitudinal approach. Arthritis Rheum. 2004;50(8):2471–8.
Gineyts E, et al. Effects of ibuprofen on molecular markers of cartilage and synovium turnover in patients with knee osteoarthritis. Ann Rheum Dis. 2004;63(7):857–61.
Ameye LG, et al. The chemical biomarkers C2C, Coll2-1, and Coll2-1NO2 provide complementary information on type II collagen catabolism in healthy and osteoarthritic mice. Arthritis Rheum. 2007;56(10):3336–46.
Henrotin Y, et al. Collagen catabolism through Coll2-1 and Coll2-`O and myeloperoxidase activity in marathon runners. Springerplus. 2013;2(1):92.
Deberg M, et al. New serum biochemical markers (Coll 2–1 and Coll 2–1 NO2) for studying oxidative-related type II collagen network degradation in patients with osteoarthritis and rheumatoid arthritis. Osteoarthritis Cartilage. 2005;13(3):258–65.
Tseng S, Reddi AH, Di Cesare PE. Cartilage oligomeric matrix protein (COMP): a biomarker of arthritis. Biomark Insights. 2009;4:33–44.
Clark AG, et al. Serum cartilage oligomeric matrix protein reflects osteoarthritis presence and severity: the Johnston County Osteoarthritis Project. Arthritis Rheum. 1999;42(11):2356–64.
Sharif M, et al. Suggestion of nonlinear or phasic progression of knee osteoarthritis based on measurements of serum cartilage oligomeric matrix protein levels over five years. Arthritis Rheum. 2004;50(8):2479–88.
Ahrman E, et al. Novel cartilage oligomeric matrix protein (COMP) neoepitopes identified in synovial fluids from patients with joint diseases using affinity chromatography and mass spectrometry. J Biol Chem. 2014;289(30):20908–16.
Sharif M, et al. Serum hyaluronic acid level as a predictor of disease progression in osteoarthritis of the knee. Arthritis Rheum. 1995;38(6):760–7.
Bierma-Zeinstra SM, Koes BW. Risk factors and prognostic factors of hip and knee osteoarthritis. Nat Clin Pract Rheumatol. 2007;3(2):78–85.
Pavelka K, et al. Hyaluronic acid levels may have predictive value for the progression of knee osteoarthritis. Osteoarthritis Cartilage. 2004;12(4):277–83.
Kaneko H, et al. Reference intervals of serum hyaluronic acid corresponding to the radiographic severity of knee osteoarthritis in women. BMC Musculoskelet Disord. 2013;14:34.
Elliott AL, et al. Serum hyaluronan levels and radiographic knee and hip osteoarthritis in African Americans and Caucasians in the Johnston County Osteoarthritis Project. Arthritis Rheum. 2005;52(1):105–11.
Chua Jr SD, et al. Effect of an exercise and dietary intervention on serum biomarkers in overweight and obese adults with osteoarthritis of the knee. Osteoarthritis Cartilage. 2008;16(9):1047–53.
Peltonen L, McKusick VA. Genomics and medicine. Dissecting human disease in the postgenomic era. Science. 2001;291(5507):1224–9.
Gharbi M, Deberg M, Henrotin Y. Application for proteomic techniques in studying osteoarthritis: a review. Front Physiol. 2011;2:90.
Pedrotty DM, Morley MP, Cappola TP. Transcriptomic biomarkers of cardiovascular disease. Prog Cardiovasc Dis. 2012;55(1):64–9.
Geyer M, et al. Differential transcriptome analysis of intraarticular lesional vs intact cartilage reveals new candidate genes in osteoarthritis pathophysiology. Osteoarthritis Cartilage. 2009;17(3):328–35.
Ramos YF, et al. Genes involved in the osteoarthritis process identified through genome wide expression analysis in articular cartilage; the RAAK study. PLoS One. 2014;9(7):e103056.
Xu Y, et al. Identification of the pathogenic pathways in osteoarthritic hip cartilage: commonality and discord between hip and knee OA. Osteoarthritis Cartilage. 2012;20(9):1029–38.
Peffers M, Liu X, Clegg P. Transcriptomic signatures in cartilage ageing. Arthritis Res Ther. 2013;15(4):R98.
Marshall KW, et al. Blood-based biomarkers for detecting mild osteoarthritis in the human knee. Osteoarthritis Cartilage. 2005;13(10):861–71.
Attur M, et al. Increased interleukin-1beta gene expression in peripheral blood leukocytes is associated with increased pain and predicts risk for progression of symptomatic knee osteoarthritis. Arthritis Rheum. 2011;63(7):1908–17.
Williams A, et al. Applications of proteomics in cartilage biology and osteoarthritis research. Front Biosci (Landmark Ed). 2011;16:2622–44.
Hsueh MF, Onnerfjord P, Kraus VB. Biomarkers and proteomic analysis of osteoarthritis. Matrix Biol. 2014;39C:56–66.
Wu J, et al. Comparative proteomic characterization of articular cartilage tissue from normal donors and patients with osteoarthritis. Arthritis Rheum. 2007;56(11):3675–84.
Guo D, et al. Proteomic analysis of human articular cartilage: identification of differentially expressed proteins in knee osteoarthritis. Joint Bone Spine. 2008;75(4):439–44.
Ruiz-Romero C, et al. Proteomic analysis of human osteoarthritic chondrocytes reveals protein changes in stress and glycolysis. Proteomics. 2008;8(3):495–507.
Kubo T, et al. Stress-induced proteins in chondrocytes from patients with osteoarthritis. Arthritis Rheum. 1985;28(10):1140–5.
Tillmann K. Pathological aspects of osteoarthritis related to surgery. Inflammation. 1984;8(Suppl):S57–74.
Fernandez-Puente P, et al. Identification of a panel of novel serum osteoarthritis biomarkers. J Proteome Res. 2011;10(11):5095–101.
Han MY, et al. Identification of osteoarthritis biomarkers by proteomic analysis of synovial fluid. J Int Med Res. 2012;40(6):2243–50.
Ritter SY, et al. Proteomic analysis of synovial fluid from the osteoarthritic knee: comparison with transcriptome analyses of joint tissues. Arthritis Rheum. 2013;65(4):981–92.
Wang Q, et al. Identification of a central role for complement in osteoarthritis. Nat Med. 2011;17(12):1674–9.
Kamphorst JJ, et al. Profiling of endogenous peptides in human synovial fluid by NanoLC-MS: method validation and peptide identification. J Proteome Res. 2007;6(11):4388–96.
Blanco FJ, Ruiz-Romero C. Osteoarthritis: metabolomic characterization of metabolic phenotypes in OA. Nat Rev Rheumatol. 2012;8(3):130–2.
Zhai G, et al. Serum branched-chain amino acid to histidine ratio: a novel metabolomic biomarker of knee osteoarthritis. Ann Rheum Dis. 2010;69(6):1227–31.
Jiang M, et al. Serum metabolic signatures of four types of human arthritis. J Proteome Res. 2013;12(8):3769–79.
Adams Jr SB, et al. Global metabolic profiling of human osteoarthritic synovium. Osteoarthritis Cartilage. 2012;20(1):64–7.
Adams Jr SB, Setton LA, Nettles DL. The role of metabolomics in osteoarthritis research. J Am Acad Orthop Surg. 2013;21(1):63–4.
Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell. 2004;116(2):281–97.
Li Y, et al. Mirsynergy: detecting synergistic miRNA regulatory modules by overlapping neighbourhood expansion. Bioinformatics. 2014;30(18):2627–35.
Kozomara A, Griffiths-Jones S. MiRBase: annotating high confidence microRNAs using deep sequencing data. Nucleic Acids Res. 2014;42(Database issue):D68–73.
Wu C, et al. MicroRNAs play a role in chondrogenesis and osteoarthritis. Int J Mol Med. 2014;34(1):13–23.
Nair VS, et al. Design and analysis for studying microRNAs in human disease: a primer on -Omic Technologies. Am J Epidemiol. 2014;180(2):140–52.
Kobayashi T, et al. Dicer-dependent pathways regulate chondrocyte proliferation and differentiation. Proc Natl Acad Sci U S A. 2008;105(6):1949–54.
Tuddenham L, et al. The cartilage specific microRNA-140 targets histone deacetylase 4 in mouse cells. FEBS Lett. 2006;580(17):4214–7.
Miyaki S, et al. MicroRNA-140 is expressed in differentiated human articular chondrocytes and modulates interleukin-1 responses. Arthritis Rheum. 2009;60(9):2723–30.
Miyaki S, et al. MicroRNA-140 plays dual roles in both cartilage development and homeostasis. Genes Dev. 2010;24(11):1173–85.
Tardif G, et al. Regulation of the IGFBP-5 and MMP-13 genes by the microRNAs miR-140 and miR-27a in human osteoarthritic chondrocytes. BMC Musculoskelet Disord. 2009;10:148.
Tardif G, et al. NFAT3 and TGF-beta/SMAD3 regulate the expression of miR-140 in osteoarthritis. Arthritis Res Ther. 2013;15(6):R197.
Akhtar N, et al. MicroRNA-27b regulates the expression of matrix metalloproteinase 13 in human osteoarthritis chondrocytes. Arthritis Rheum. 2010;62(5):1361–71.
Yamasaki K, et al. Expression of MicroRNA-146a in osteoarthritis cartilage. Arthritis Rheum. 2009;60(4):1035–41.
Nakasa T, et al. Expression of microRNA-146 in rheumatoid arthritis synovial tissue. Arthritis Rheum. 2008;58(5):1284–92.
Jones SW, et al. The identification of differentially expressed microRNA in osteoarthritic tissue that modulate the production of TNF-alpha and MMP13. Osteoarthritis Cartilage. 2009;17(4):464–72.
Jin L, et al. Role of miR-146a in human chondrocyte apoptosis in response to mechanical pressure injury in vitro. Int J Mol Med. 2014;34(2):451–63.
Li X, et al. MicroRNA-146a is linked to pain-related pathophysiology of osteoarthritis. Gene. 2011;480(1–2):34–41.
Li X, et al. Altered spinal microRNA-146a and the microRNA-183 cluster contribute to osteoarthritic pain in knee joints. J Bone Miner Res. 2013;28(12):2512–22.
Iliopoulos D, et al. Integrative microRNA and proteomic approaches identify novel osteoarthritis genes and their collaborative metabolic and inflammatory networks. PLoS One. 2008;3(11):e3740.
Diaz-Prado S, et al. Characterization of microRNA expression profiles in normal and osteoarthritic human chondrocytes. BMC Musculoskelet Disord. 2012;13:144.
Weber JA, et al. The microRNA spectrum in 12 body fluids. Clin Chem. 2010;56(11):1733–41.
Mitchell PS, et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc Natl Acad Sci U S A. 2008;105(30):10513–8.
Kumar P, et al. Circulating miRNA biomarkers for Alzheimer’s disease. PLoS One. 2013;8(7):e69807.
Ward J, et al. Circulating microRNA profiles in human patients with acetaminophen hepatotoxicity or ischemic hepatitis. Proc Natl Acad Sci U S A. 2014;111(33):12169–74.
Murata K, et al. Plasma and synovial fluid microRNAs as potential biomarkers of rheumatoid arthritis and osteoarthritis. Arthritis Res Ther. 2010;12(3):R86.
Beyer C, et al. Signature of circulating microRNAs in osteoarthritis. Ann Rheum Dis. 2015;74(3):e18.
Borgonio Cuadra VM, et al. Altered expression of circulating microRNA in plasma of patients with primary osteoarthritis and in silico analysis of their pathways. PLoS One. 2014;9(6):e97690.
Redova M, Sana J, Slaby O. Circulating miRNAs as new blood-based biomarkers for solid cancers. Future Oncol. 2013;9(3):387–402.
Lotz M, Martel-Pelletier J, Christiansen C, Brandi ML, Bruyère O, Chapurlat R, Collette J, Cooper C, Giacovelli G, Kanis JA, Karsdal MA, Kraus V, Lems WF, Meulenbelt I, Pelletier JP, Raynauld JP, Reiter-Niesert S, Rizzoli R, Sandell LJ, Van Spil WE, Reginster JY. Republished: Value of biomarkers in osteoarthritis: current status and perspectives. Postgrad Med J. 2014;90(1061):171–8.
Kraus VB. Biomarkers in osteoarthritis. Curr Opin Rheumatol. 2005;17(5):641–6.
Mobasheri A, Henrotin Y. Biomarkers of osteoarthritis: a review of recent research progress on soluble biochemical markers, published patents and areas for future development. Recent Pat Biomarkers. 2011;1:25–43.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Li, YH., Kim, C., Gandhi, R. (2015). Osteoarthritis Biomarkers. In: Kapoor, M., Mahomed, N. (eds) Osteoarthritis. Adis, Cham. https://doi.org/10.1007/978-3-319-19560-5_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-19560-5_9
Publisher Name: Adis, Cham
Print ISBN: 978-3-319-19559-9
Online ISBN: 978-3-319-19560-5
eBook Packages: MedicineMedicine (R0)