
Abstract
Figure 2.1 illustrates the surface anatomy of the cervical spine (C-spine). The C-spine consists of seven vertebrae (C1–C7) and supports the weight of the head (approximately 14 lb). The first two vertebrae are called the axis and atlas, respectively, and do not have a disc between them but are closely bound together by a complex of ligaments. The C1 (atlas) “ring” rotates around the odontoid or “peg” of C2 (axis), allowing for almost 50 % of total cervical rotation. The spinal canal is housed within the cervical vertebrae and is widest between the C1 and C3 levels (A-P diameter 16–30 mm) and narrows as it progresses caudally (14–23 mm). When the neck is fully extended, this canal can narrow an additional 2–3 mm.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Ottawa neck rules
- Hoffman’s sign
- Spurling’s maneuver
- Cervical spine
- Radicular symptoms
- Facet joint
- Spinal stenosis
- Whiplash-associated syndrome
- Physical exam
- Curriculum
- Primary care musculoskeletal conditions
Functional Anatomy
Figure 2.1 illustrates the surface anatomy of the cervical spine (C-spine). The C-spine consists of seven vertebrae (C1–C7) and supports the weight of the head (approximately 14 lb). The first two vertebrae are called the axis and atlas, respectively, and do not have a disc between them but are closely bound together by a complex of ligaments. The C1 (atlas) “ring” rotates around the odontoid or “peg” of C2 (axis), allowing for almost 50 % of total cervical rotation. The spinal canal is housed within the cervical vertebrae and is widest between the C1 and C3 levels (A-P diameter 16–30 mm) and narrows as it progresses caudally (14–23 mm). When the neck is fully extended, this canal can narrow an additional 2–3 mm.

Surface anatomy of cervical spine
Cervical spine vertebrae differ from lumbosacral vertebrae in several ways. First, there are foramina on each side which allow passage of the vertebral arteries. Additionally, the facet joints in the C-spine have steeper angles which allow for more rotation between vertebrae without subluxation. The most important difference, however, is the nonsynovial joint, known as the uncovertebral joint or “joint of Luschka.” During midlife, this joint prevents a disc rupture from directly pressing onto the nerve root. This means that most disc herniations in the neck occur posteriorly (unlike the LS spine, in which most herniations occur laterally). As we age, these joints can form osteophytes that can impinge upon the nerve root or compress the cervical cord directly causing cervical myelopathy. Figure 2.2 shows the major differences between lumbar and cervical vertebrae.

Comparison of lumbosacral (left) and cervical (right) vertebrae
Red Flags
Some serious conditions can present as neck pain, and the following are considered “red flag” conditions which should spur further evaluation.
-
1.
Trauma: Neck pain in the setting of trauma should receive emergent evaluation and is best managed in an emergency department. If there is any fear of spine instability, the patient should be immobilized with an appropriate cervical collar and transferred by emergency medical personnel.
-
2.
History of neck surgery: New neck pain in a patient who has had prior neck surgical intervention must be approached with caution. Strong consideration to immediate referral should be given in all but the most clear-cut cases.
-
3.
Rapidly progressing neurological deficit: Patients who present with rapid, progressive neurologic deficits should be suspected of having CNS involvement and should be urgently referred.
-
4.
Neck and/ or jaw pain associated with cardiac risk factors and exertion: Referred pain with cardiac ischemic pattern or associated with diaphoresis should be urgently referred.
Epidemiology of Cervical Spine Pathology
Neck pain is common, occurring half as often as low-back pain; almost 70 % of the population experiences neck pain at some time. Women are affected more than men. Other risk factors are cigarette smoking, advancing age, and certain occupations. The prevalence of neck pain at any given time is 15 %.
The most common post-traumatic cause of neck pain is a whiplash injury, typically following an automobile accident. The mechanism of injury is a hyperextension motion followed by deceleration and may damage anterior muscles, ligaments, and discs. A number of high-quality studies have shown that a certain percentage of patients, on average 33 %, reported chronic symptoms after sustaining this type of injury. The Quebec task force recommends that only patients with peripheral neurological findings and those with fracture dislocation require surgical intervention. These types of injuries often involve litigation and, under our current tort system, encourage expensive imaging, most of which have no proven value in improving the course of clinical improvement.
Patients who work in occupations which involve repetitive use of the upper extremities, such as machine operators, office workers, and carpenters, are also prone to neck pain. These types of disorders often involve nerve entrapment, and nerve conduction studies may be useful to localize the origin of entrapment neuropathies.
A careful history is the most useful tool in differentiating C-spine pathologies. Important questions include the nature, duration, and location of the pain, associated numbness or tingling in either or both upper extremities, other musculoskeletal symptoms, and any history of trauma.
In patients presenting with neck pain, the physical exam must include a neurologic evaluation. The necessary exam will differ depending on patient presentation (evaluation is described in detail below). Most patients with neck pain and an absence of neurologic findings will have benign neck pain and require no further workup. Two different sets of rules have been created to assist healthcare providers in determining when imaging is appropriate (the Canadian Task Force (CTF) X-ray Rules and the Nexus Rules). It has been suggested that the CTF rules are more relevant in the primary care setting. These rules are shown in Table 2.1.
Common Clinical Presentations
Myofascial (Mechanical) Neck Pain
This is by far the most common neck condition the primary care provider will encounter. Mechanical neck pain is typically reported as diffuse and nonspecific and made worse with neck movement. Two-thirds of these patients have pain in their shoulders and upper arms in a nonradicular pain pattern. The other one-third of these patients will present with headaches sometimes radiating to the front of the head. Upon examination, there may be localized “trigger” points in the cervical and peri-scapular musculature. Injection of 2 cc 0.5 % bupivacaine or 1 % lidocaine into the trigger point can be both diagnostic and therapeutic.
The primary goal in evaluation of patients with myofascial neck pain is to exclude worse pathology. In the absence of neurologic symptoms or neurologic findings, these patients can be managed conservatively. Management strategies include use of NSAIDs, activity and postural modification, physical therapy (PT), muscle relaxants, and, occasionally, limited use of opioids.
Cervical Spondylosis
Cervical spondylosis is a general and nonspecific term that encompasses a broad spectrum of afflictions but, for purposes of clarity, can be organized into three clinical syndromes: spondylosis with joint pain, spondylosis with cervical radiculopathy, and spondylosis with cervical myelopathy. It is important to remember that shoulder problems can masquerade as neck pain, such as in the case of shoulder impingement or rotator cuff disorders.
Spondylosis with Joint Pain
Degenerative arthritic changes, such as foraminal narrowing or spurring of vertebral bodies, will often be seen on radiographic imaging. This condition of cervical joint pain is often chronic, increases with advancing age, and may respond to NSAIDs, gentle range of motion exercises, and physical therapy.
Whiplash-Associated Disorder
Whiplash-associated disorder (WAD) commonly occurs in “rear-end” motor vehicle crashes. There are many theories as to why patients have so much discomfort after sustaining this type of injury. Facet joints may be the primary generators.
These patients will generally complain of symptoms similar to those associated with mechanical neck pain. Headaches are common, but physical examination will reveal no evidence of neurologic compromise. Treatment of WAD generally mimics that for mechanical neck pain.
Cervical Spondylosis with Radiculopathy
Cervical radiculopathy is the result of nerve root irritation or ischemia and can occur at multiple levels. This most commonly occurs at the interval foramina. It usually presents with nonspecific neck pain, but the most prominent symptom is that of weakness, numbness, and tingling in one of the upper extremities. Patients with these symptoms that occur before the age of 35 should be suspected of having congenital abnormalities. The pain pattern may help make the diagnosis of cervical radiculopathy (see Fig. 2.3).

Pain patterns at each cervical level (Adapted from Grubb SA, Kelly CK, Bgoduk N. Cervical discography: clinical implications from 12 years of experience. Spine. 2000; 25:1382–9)
At times it is difficult to determine if a patient’s pain is coming from the C-spine, the shoulder, or both. Patients complaining of pain in the posterior part of their shoulder or who have symptoms below their elbow often have a cervical pathology as the source of their pain. In addition to this, patients with C-spine pathology will complain of increased symptoms doing overhead work and will sometimes have their symptoms relieved by abducting their shoulder and resting their hand on the top of their head. Figure 2.4 describes the common motor and sensory evaluation of nerve roots C5–T1.

Motor, sensory, reflex evaluation of cervical spine nerve roots
There have been a large number of studies to identify clinical signs or symptoms best associated with the diagnosis of nerve root impingement. Perhaps the most clinically useful set was described by Dr. Weiner et al., who identified a test item cluster. In this study, the authors found that there were four predictable variables that most likely identified patients with cervical radiculopathy:
-
1.
Cervical rotation of less than 60° to the ipsilateral side.
-
2.
A positive Spurling’s test. This test is performed with the patient in a seated position. The patient laterally flexes the neck to the ipsilateral side, and the examiner places pressure on the top of the patient’s head. If the pressure on the patient’s head reproduces the patient’s symptoms into the arm, then the test is positive (see Fig. 2.5).
Fig. 2.5 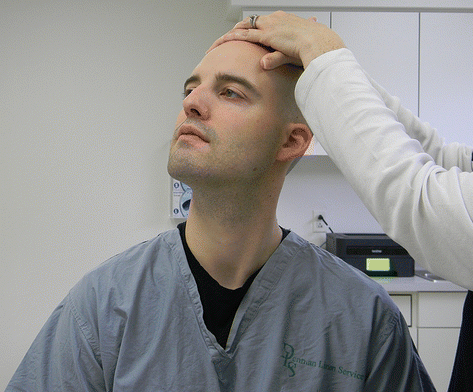
Spurling’s maneuver
-
3.
A positive distraction test. This test is performed with the patient in a supine position. The examiner cradles the patient’s neck on the occiput and exerts traction. If this relieves some of the patient’s symptoms, it is positive.
-
4.
A positive upper limb test. This test is performed with the patient in a seated position. The patient abducts the arm to 90°, and with the elbow completely extended, the examiner dorsiflexes the wrist. This maneuver can reproduce patient’s symptoms if the cause is cervical nerve related.

These four tests combined are useful for the evaluation of radiculopathy: if three of the signs are present, the LR+ for radiculopathy is 6.1; if all four are present, the LR+ is 30.3; fewer than three of the signs are less helpful for predicting radiculopathy.
In most cases, physical therapy and pain control are reasonable treatment modalities for radiculopathy. An MRI should be ordered to confirm the diagnosis and to identify any other anomalies; if this is negative, the patient generally does not need orthopedic referral. If the MRI shows significant findings, or if the patient does not respond to PT, referral should be considered. Steroid injections have sometimes been used but are somewhat technically difficult, and there are concerns about potential complications.
The Stinger Injury
The stinger or burner is an injury associated with contact sports, especially football. The primary symptom is burning pain radiating down one upper extremity. Most cases involve the brachial plexus and may also involve cervical nerve roots. The usual mechanism of injury is traction with the shoulder depressed and the neck forced into lateral flexion. Treatment consists of restoring range of motion and improving neck and shoulder strength. Return to sports participation is dependent upon restoring pain-free range of motion and full recovery of strength and function. Protective devices, such as cowboy collars, may be useful to prevent these types of injuries.
Cervical Myelopathy
Cervical myelopathy occurs when the spinal cord is either directly compressed or rendered ischemic by compression. This can be caused by a congenitally small spinal canal or the normal “degeneration” of structures of the cervical spine. The most common culprits include thickening of the ligamentum flavum and spurring of the uncovertebral joint. The uncovertebral joint “protects” the cord from lateral disc herniation in midlife, but as a patient ages and osteophytes start to form in this joint, they can exert direct pressure on the spinal cord. This is most commonly seen in the sixth decade of life and may present acutely as a result of a minor fall or injury. There are a number of other entities that can also masquerade as cervical myelopathy. These include peripheral neuropathy, upper motor neuron disease, multiple sclerosis, cerebra vascular disease, and syringomyelia.
Cervical myelopathy may present with neck pain and bilateral upper extremity symptoms (pain, numbness, or tingling as in radiculopathy), along with report of loss of balance or lack of coordination. Most commonly, patients with cervical myelopathy present with clumsiness or lack of fine motor skills in the hands or an increasingly awkward gait and difficulty in maintaining balance. Patients may also complain of urinary urgency and hesitation but rarely of incontinence.
Physical exam findings include abnormal reflexes often found in patients with cervical radiculopathy. These patients are often hyperreflexic and may have upgoing Babinski reflexes, inverted radial reflex (flexor tendons of the wrist are struck on the radial aspect of the forearm with a reflex hammer, and the index finger will flex), and Hoffman’s reflex (flexion of the index finger and thumb when the examiner “flicks” the patient’s middle finger nail) (Fig. 2.4).
Occasionally, these patients may present acutely after falling or may present when ischemic insult occurs in the cord such as a thrombosis of the posterior inferior cerebral artery. Patients with these symptoms should be evaluated and referred on for further evaluation.
Patients with suspected or confirmed cervical myelopathy should be referred to an orthopedic or spinal surgeon. MRI can confirm the diagnosis, but if clinical symptoms are suggestive without imaging, referral should be made at that time.
Conclusion
Most patients with neck pain have benign myofascial neck pain. The primary goal in evaluation of these patients is to rule out more serious pathology. Those with serious pathology require more intense workup and management, while those with mechanical symptoms can be reassured and managed conservatively. Careful history and physical exam can easily distinguish between potentially serious and benign causes of pain.
Please refer to Fig. 2.6 for the C-spine meaningful use form.


The C-spine meaningful use form
Suggested Readings
Ahn NU, Ahn UM, Ipsen B, An HS. Mechanical neck pain and cervicogenic headache. Neurosurgery. 2007;60(1 Supp1 1):S21–7.
Binder AI. Cervical spondylosis and neck pain. BMJ. 2007;334:527–31. http://bmj.com/cgi/content/full/334/7592/527. Retrieved 17 July 2008.
Boyce RH, Wang JC. Evaluation of neck pain, radiculopathy and myelopathy: imaging, conservative treatment, and surgical indications. AAOS Instr Course Lect. 2003;52:489–95.
Cleland J. Orthopaedic clinical examination: an evidence-based approach for physical therapists. Philadelphia: Saunders; 2007. p. 133.
Cleland JA, Childs JD, Fritz JM, Whitman JM. Interrater reliability of the history and physical examination in patients with mechanical neck pain. Arch Phys Med Rehabil. 2006;87(10):1388–95.
Couglass AB, Bope ET. Evaluation and treatment of posterior neck pain in family practice. J Am Board Fam Pract. 2004;17(Suppl):S13–22. http://www.jabfp.org. Retrieved 17 July 2008.
Devereaux MW. Neck and low back pain. Phys Med Rehabil Clin N Am. 2003;87:643–62.
Freedman MK, Overton A, Saulino MF, Holding MY, Kornbluth ID. Interventions in chronic pain management. 2. Diagnosis of cervical and thoracic pain syndromes. Arch Phys Med Rehabil. 2008;89(1):S41–6.
Gore DR. The epidemiology of neck pain. Med Gen Med. 1999;1(1) [formerly published in Medscape Orthopaedics & Sports Medicine eJournal. 1998;2(5)].
Haldeman S, Carroll LJ, Cassidy JD. The empowerment of people with neck pain: introduction. Spine. 2008;33(4S):S8–13.
Hardin J. Pain and the cervical spine. Bull Rheum Dis. 2001;50(10):1–4.
Honet JC, Ellenberg MR. What you always wanted to know about the history and physical examination of neck pain but were afraid to ask. Phys Med Rehabil Clin N Am. 2003;14:473–91.
Kuhlman GS, McKeag DB. The burner: a common nerve injury in contact sports. Am Fam Physician. 1999;1:60(7).
Manchikanti L, Damron K, Cash K, Manchukonda R, Pampati V. Therapeutic cervical medial branch blocks in managing chronic neck pain: a preliminary report of randomized, double-blind, controlled trial: clinical trial NCT0033272. Pain Physician. 2006;9:333–46.
Mazanec D, Reddy A. Medical management of cervical spondylosis. Neurosurgery. 2007;60(1):S1-43–S1-50.
Paul A, Lewis M, Saklatvala J, et al. Cervical spine magnetic resonance imaging in primary care consulters with shoulder pain: a case-control study. Ann Rheum Dis. 2007;66:1363–8.
Rao R. Neck pain, cervical radiculopathy, and cervical myelopathy. J Bone Joint Surg Am. 2002;10:1872–81.
Rao R. Neck pain, cervical radiculopathy, and cervical myelopathy: pathophysiology, natural history and clinical evaluation. AAOS Instr Course Lect. 2003;52:479–88.
Rao R, Currier B, Albert T, et al. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. J Bone Joint Surg Am. 2007;89:1360–78.
Ross A. Managing cervical spondylosis. Practitioner. 2005;249(1676):762, 764, 766–8.
Thompson JC. Netter’s concise atlas of orthopaedic anatomy. San Diego: ICON; 2001. p. 9–25.
Tong C, Barest G. Approach to imaging the patient with neck pain. J Neuroimaging. 2003;13(1):5–16.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Mathews, W.A., Arguelles, C.S. (2015). The Cervical Spine. In: Daniels, J. (eds) Common Musculoskeletal Problems. Springer, Cham. https://doi.org/10.1007/978-3-319-16157-0_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-16157-0_2
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-16156-3
Online ISBN: 978-3-319-16157-0
eBook Packages: MedicineMedicine (R0)