
Abstract
Plague and tularemia are diseases caused by gram-negative bacteria Yersinia pestis and Francisella tularensis, respectively. Transmission occurs mainly through vectors, affecting humans and other mammals, causing fever and lymphadenopathy. These infectious diseases present very similar clinical and epidemiological characteristics; therefore, it is appropriate to study them jointly. On the other hand, there also are important differences as to their clinical and epidemiological aspects, as well as their etiologic agents. Among the reservoirs common to both microorganisms, rodents are worthy of mention, as well as lagomorphs and wild and domestic carnivores. The primary mode of plague transmission is through the bite of infected fleas, while transmission of tularemia is caused through the bite of several hematophagous arthropods. These diseases can be found throughout the world: the plague persists in natural foci in countries Africa, Asia, Europe, and the Americas, while tularemia is restricted to countries in the northern hemisphere. Treatment for both diseases consists of similar antimicrobials, where streptomycin and gentamicin are the drugs of choice. Without prompt treatment, these diseases can cause serious illness and even death. Bacterial culture and inoculation of animals infected with plague and tularemia should be carried out in a biosafety level 3 (BSL3) laboratory. Both diseases are categorized as international public health emergencies, given their ability to cause significant impact on public health and their potential for rapid international spread.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Plague and tularemia are caused by the gram-negative bacteria Yersinia pestis and Francisella tularensis , respectively. These bacteria were both initially classified as belonging to the genus Pasteurella ; however, biochemical and genetic differences were sufficient to subdivide them into two genera: Yersinia in honor of Alexandre Yersin, the discoverer of the bacillus responsible for plague, and Francisella in honor of Edward Francis, a scholar of tularemia.
The clinical and epidemiological similarities between the two diseases justify presenting them together. They are vector-transmitted zoonoses that occasionally affect humans, causing fever, lymphadenopathy, and pulmonary impairment in infected individuals. Plague transmission occurs primarily through the bite of infected fleas, while tularemia is vectored by blood-sucking arthropods (i.e., fleas, ticks, mites, and mosquitoes). Rodents, lagomorphs, and wild and domestic carnivores are reservoirs for both bacterial strains.
The Centers for Disease Control and Prevention (CDC) classifies both bacterial species as biosafety level 3 and within category A of the bioterrorism agent/disease list, considering the severity of disease and the potential use of these pathogens as agents of bioterrorism.Footnote 1
According to the World Health Organization (WHO) , 12,503 cases of human plague were documented between 2004 and 2009, causing 843 deaths across 16 countries in Africa, Asia, and the Americas, with a case fatality rate of 6.7 %. Africa was the continent most affected; eight countries reported 12,209 cases in total, with 814 deaths. Asia reported 149 cases in four countries with 23 deaths, while in the Americas, 145 cases were reported in two countries, resulting in six deaths.
Between 1900 and 2010, 999 suspected cases of human plague were reported in the United States, and over 80 % of these cases were the bubonic form. In the last decade, an average of seven cases of human plague was reported each year (range: 1–17 cases per year). Cases are reported in both men and women, although historically infection is more common among men, likely due to outdoor activities that put them at higher risk.
Tularemia affects countries in the northern hemisphere, principally North America, South America (Venezuela), and most countries in Europe and Asia (including China and Japan). In 2000, the WHO indicated 56 cases of tularemia in Pristina, Kosovo. Tularemia was more common in the United States in the early twentieth century than today; the case frequency has declined since 2003, and currently, there are fewer than 200 cases reported per year, despite occurring in every state except Hawaii. Infection occurs sporadically throughout the year with prevalence in adult males, possibly due to greater involvement in outdoor activities such as hunting. Cases are also reported in children, especially in the summer, probably due to high seasonal abundance of ticks and horse flies.
2 History
2.1 Plague
Plague probably originated in the Central Asian Plateau and has been responsible for high mortality rates in some time periods. Numerous references in art, literature, and historical monuments attest to the horrors and devastation of the plague. During the Christian era, three major pandemics were characterized. The first, called the Plague of Justinian (542–605 AD) , originated in Egypt and spread throughout the civilized world, reaching Asia, Africa, and Europe. The second, the dreaded Black Death , began in Asia and extended throughout Europe and North Africa, persisting from the fourteenth to sixteenth centuries and killing a quarter of the European population. The third, the contemporary pandemic , originated in 1891 in Yunnan, China and, in 1894, extended to Hong Kong and quickly spread across the continents via sea transport, leaving natural foci scattered among all continents with the exception of Australia (Perry and Fetherston 1997).
Three relevant events occurred throughout the history of plague: first, the etiologic agent was isolated in 1894 by Alexandre Yersin; second, fleas were discovered as agents of disease transmission in 1898 by Paul-Louis Simond; last, the pandemics created natural foci in various (previously unaffected) regions of the world .
2.2 Tularemia
During research on the plague in endemic areas, tularemia was discovered and initially identified as a kind of plague called “pseudo-plague .” In 1911, the etiologic agent, initially named Bacterium tularense , was isolated from squirrels in the city of Tulare, California (USA). The syndrome was characterized in 1912, with the first human cases observed in 1914. Studies of this zoonotic disease progressed in all aspects thereafter, with much of the work conducted by researcher Edward Francis. Because of his commitment to research on this zoonosis, the name of the bacillus was changed to Francisella tularensis in his honor (Eigelsbach and McGann 1984).
Tularemia has been reported to occur in Japan since 1837, described as a disease acquired by ingestion of hare meat. The degree of pathology to humans was discovered in the laboratory after accidental infection. The existence of tularemia was then acknowledged in 1928, after long being mistaken for a type of plague. From 1929 to 1945, it was also acknowledged in Norway, Sweden, Turkey, Austria, Czechoslovakia, and France (Eigelsbach and McGann 1984).
3 Etiology
3.1 Plague
The causative agent of plague , Yersinia pestis , belongs to family Enterobacteriaceae. The genus Yersinia consists of 17 species that can be differentiated by their pathogenicity. Yersinia pseudotuberculosis and Y. enterocolitica are enteropathogenic, transmitted by oral-fecal route and causing a clinical condition called Yersiniosis (Perry and Fetherston 1997). One of these pathogens, Y. pseudotuberculosis, is considered the ancestor of Y. pestis and is thought to have diverged approximately 1.5–20 thousand years ago (Achtman et al. 1999).
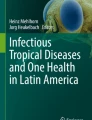
Yersinia pestis is a gram-negative bacillus, short and ovoid (0.5–0.8 mm diam. × 1–3 mm length), and having intense bipolar coloration when impregnated with specific dyes (Fig. 11.1a1). Yersinia pestis is aerobic or facultative anaerobic, non-sporulating, and does not ferment lactose, sucrose, or rhamnose; it acidifies glucose, mannitol, and salt without producing gas and does not hydrolyze urea. The results of nitrate reduction and glycerol fermentation tests are variable and important for the identification of different geographic varieties or biovars.

Yersinia pestis bacillus and intense bipolar coloration when impregnated with specific dyes (a1), bubonic plague (a2), septicemic plague (a3) image of Francisella tularensis bacillus (b1), ulceroglandular tularemia (b2). Source: (a) CDC/Plague 2012 and (b) CDC/Tularemia 2011
Yersinia pestis grows well on ordinary media, such as peptone agar base and blood agar base (BAB) . Growth can occur at temperatures ranging from 4 to 37°C, but 28°C is ideal, producing slow growth. After 48 h, colonies measure from 1 to 2 mm in diameter, whitish with convex shape, shiny, translucent, and non-mucoid. In broth (brain-heart infusion , or BHI), this microorganism exhibits flocculent (i.e., clumped) growth, resulting in nonuniform medium turbidity (Perry and Fetherston 1997).
Yersinia pestis is cold resistant and is well preserved in corpses and in sputum of patients with pneumonic plague and in flea droppings. It can be eliminated by common disinfectants like antiseptic soap and hypochlorite or by sun exposure, boiling water (for a few minutes), or moist heat at 60 °C (40 min). Cultures can be maintained on peptone agar at 4 °C for decades, but the safest way is via lyophilization .
Yersinia pestis strains are considered highly phenotypically homogeneous , having a serotype and phagotype. The biovars and geographical varieties have acquired recent classifications that reflect global diversity based on single nucleotide polymorphism (SNP) type and biochemical characteristics. In accordance with the International Code of Nomenclature of Bacteria (ICNB) , Y. pestis has been subdivided into two major subspecies: Y. pestis pestis and Y. pestis microtus. Yersinia p. microtus comprises of a group of biovars that typically do not cause disease in humans (bv. caucasica, bv. angola, bv. talassica, bv. qinghaiensis, bv. xilingolensis, bv. altaica, bv. hissarica, and bv. ulegeica). Yersinia pestis pestis includes four biovars (bv. intermedium, bv. antiqua, bv. medievalis, and bv. orientalis) (Platonov et al. 2013).
The Y. pestis genome consists of a single circular chromosome of about 4.6 Mb with a GC content of 47 %, with approximately 4200 genes and three prototypical plasmids: pPCP1, PMT1, and pCD1 (9.5, 100, and 70 kb, respectively). Its pathogenicity is attributed to several factors, including the presence of invasins, adhesins, and toxins, as well as intracellular and antibiotic resistance encoded by plasmid and chromosomal genes (Perry and Fetherston 1997; Parkhill et al. 2001; Deng et al. 2002).
In addition to the murine toxin, the pPCP1 plasmid appears to play an essential role in the transmission of Y. pestis by fleas. The PMT1 plasmid codes for one of the envelope proteins (F1) of Y. pestis, and is highly immunogenic for humans and animals, making it useful in diagnostic tests such as enzyme-linked immunosorbent assay (ELISA) . The pCD1 plasmid, also present in other pathogenic Yersinia, is responsible for a complex type III secretion system (TTSS) , which neutralizes host antibacterial defenses.
The absence of one of these plasmids or the presence of atypical or cryptic plasmids has been observed in Y. pestis strains worldwide. These events may be fostered by the presence of insertion sequences (IS1541A, IS100, IS285, IS1661) in the genome of the bacterium, as well as by insertion of plasmid sequences on the chromosome, recombination events, genetic reorganization, and inversion of genome segments (Carniel 2008).
The Y. pestis chromosome contains a region called the pgm locus (102 kb), which is composed of two segments. The first segment is a high-pathogenicity island (HPI) associated with iron acquisition, involved in the synthesis of siderophores (Yersiniabactin), and essential for the dissemination of bacteria in mammals; the other segment is the hemin storage (HMS) and is involved in the colonization and blockage of the flea proventriculus by the production of biofilm . The pgm locus is unstable and may delete or block other gene segments resulting in variations in virulence. This deletion is attributed to homologous recombination resulting from the presence of IS in this region (Prentice and Rahalison 2007).
The complete genomes of various Y. pestis strains have been sequenced (Parkhill et al. 2001; Deng et al. 2002). Genome comparisons, including between ancestral and current strains, have elucidated mechanisms of pathogen evolution and adaptation for emerging countries and reemerging infections and have contributed to an understanding of the evolution of pathogenicity of the plague (Seifert et al. 2013; Wagner et al. 2014). They have also been useful for reconstruction of the history of the plague, observation of diversity in characteristics, and identification of new virulence factors. However, future experiments involving full characterization of the pathogenicity and lifestyle of Y. pestis are still needed.
3.2 Tularemia
The causative agent of tularemia , Francisella tularensis (Francisella: Francisellaceae), is classified into three subspecies, all of them pathogenic to humans. The first is F. tularensis tularensis , also called type A , which is highly virulent and occurs only in North America. It is distributed into two subpopulations (A1 and A2), with the A1 population further subdivided into A1a and A1b, each having have different geographic distributions, hosts and vectors. Francisella tularensis holarctica is also called type B . It is less virulent and endemic to many countries in the northern hemisphere. Francisella tularensis mediasiatica is equivalent to holarctica in virulence and can be found only in Central Asia. Although species within genus Francisella generally differ in virulence and geographic distribution, they have a high degree of antigenic and genomic similarity (Molins et al. 2014).
Tularemia caused by A1b strains usually exhibit severe clinical progression and are associated with high mortality rates, in contrast to infections with strains A1a, A2, or type B. Recently, subspecies A1b was also discovered in Tasmania and Australia.
Francisella tularensis is a gram-negative coccobacillus (Fig. 11.1b1) that is pleomorphic and non-spore-forming, strictly aerobic, oxidase-negative, and H2S-positive and that ferments carbohydrates without the presence of gas. This species requires specific cultures rich in cystine and cysteine (e.g., agar blood glucose-cysteine) for growth, incubated at 37 °C for 2–4 days.
Although considered an obligatory intracellular pathogen in vivo, F. tularensis can be cultured in vitro, in which case proper environmental maintenance is strongly dependent on temperature. Francisella tularensis can survive for months at temperatures below 0 °C in water, straw, grain, and carcasses. However, survival is only possible for a few days at temperatures above 10 °C. The bacteria are killed at 56 °C in 10 min or at 45 °C in 60 min. It can be stored in the laboratory in glycerol at −80 °C or lyophilized.
Some Francisella species genomes have been sequenced, including F. tularensis (Larsson et al. 2005; Antwerpen et al. 2013). Subspecies tularensis has a high degree of genetic similarity with other subspecies. The F. tularensis genome consists of a circular chromosome of approximately 1.8 MB, with a GC content of 32.2 % and approximately 1800 genes.
The F. tularensis chromosome contains genes that are important for cell maintenance, carbohydrate metabolism, amino acid biosynthesis, metabolic transport, energy metabolism, DNA modifications/restrictions, and maintenance of environmental homeostasis.
Francisella tularensis pathogenicity involves several virulence factors that are important for the development of the disease, including growth in macrophages, degradation of the phagosome membrane and release into the cytosol by the action of the phospholipase family proteins, ammonia production, production of pili, and acquisition of iron. Pathogenic Francisella genomes contain a “Francisella pathogenicity island ” (FPI) of 33.9 kb. The FPI carries 16–19 genes composing a type VI secretion system. Deletions of many of these genes within the FPI generate mutants that do not grow in macrophages and with severely attenuated virulence in mice. Additionally, five types of insertion elements (ISFtu1–ISFtu5) have been described in the F. tularensis genome. The ISs are responsible for the inactivation of genes in the Francisella genome, as well as duplication of the FPI (Kingry and Petersen 2014).
The complete genomes of various F. tularensis strains and subspecies have been sequenced (Larsson et al. 2005; Antwerpen et al. 2013). The comparison among different genomes has elucidated aspects of bacterial evolution and biogeographical distribution and increased our knowledge of pathogenic factors. Access to complete genome information has also improved microbial diversity research and our understanding of the epidemiology and expansion of the disease. However, studies are still needed in some areas, such as pathogenicity factors, biodiversity, and taxonomy .
4 Epidemiology
4.1 Plague
Yersinia pestis has two distinct life cycles . The natural life cycle is known as a zoonotic-sylvatic (Fig. 11.2a), wherein the bacterium is transmitted primarily by the bite of infected fleas. When this vector encounters a similar host in urban setting, the cycle is called zoonotic-urban (Fig. 11.2b). If at some point in these cycles a human or other mammal (dog, cat, rabbit, camel, etc.) comes into contact with any infectious component (fleas, tissues, aerosols), they can become infected with bacteria and develop symptoms of the plague.

Plague epidemiological cycles . (a) Sylvatic zoonotic cycle and (b) urban zoonotic cycle
The main sources of plague infection in nature are wild rodents, where seemingly every region has a distinct endemic reservoir fauna. It is estimated that roughly 200 species are involved in plague epidemiological cycles. Some rodent species (e.g., Rattus rattus ) may present a higher resistance, resulting in persistence of infection in regions such as Madagascar. Other species are subject to heavy mortality during epidemics (e.g., Cynomys and Necromys sp.) or even targets of poaching (e.g., Marmota spp.), increasing the risk of contamination and spread of infection among domestic animals and humans.
The primary means of plague transmission is by bite from infected fleas. More than 200 flea species have been found infected with Y. pestis . Among these, the “rat flea ” ( Xenopsylla cheopis ) has wide geographic distribution, is highly susceptible to infection, and is thus considered the primary plague vector (Eisen and Gage 2009). Other recognized vector species include X. brasiliensis in Africa, India, and South America; X. astia in Indonesia and Southeast Asia; X. vexabilis in the Pacific Islands; Nosopsyllus fasciatus , with nearly worldwide distribution in temperate climates; Malaraeus telchinus, Oropsylla montana, Opisocrostis spp., and Hoplopsyllus anomalus in the United States; Stivalius cognatus in Indonesia; and Polygenis spp. in foci of Brazil and Peru. Fleas in the genus Ctenocephalides are also considered possible vectors in Africa and Brazil.
When infected hosts die, fleas abandon the cadaver to seek new sources of food; this new host needs not be the preferred host type, resulting in possible parasitism and infection of humans. There are three different mechanisms of transmission, which may be more or less important according to flea vector species and epizootiological stage (Hinnebusch and Erickson 2008). Biological transmission depends on bacterial proliferation and biofilm production in the intestine and proventriculus of the flea, where growth must be sufficient to block (completely or partially) these organs. The plague bacilli are then regurgitated during attempted feeding on a new host. Early transmission does not depend on the development of the bacteria in the fleas, but it too results from regurgitation of infectious material during the biting of an uninfected host. Mechanical transmission occurs when the flea feeds on a septicemic host and soon thereafter feeds on a new host, inoculating the new host with bacteria residing outside the flea mouthparts.
As described above, the HMS locus is important for colonization of the digestive tract of the flea. Phospholipase D is required for bacterial survival in biofilm and in the flea midgut, apparently because it prevents/blocks bacterial autolysis by subproducts of the digested plasma. Phospholipase D is encoded by the ymt gene , which is located on one of the exclusive Y. pestis plasmids (PMT1) essential for bacillus transmission by fleas. Other environmental and bacterial factors involved in flea colonization and biofilm formation are poorly understood.
In addition to acting as plague vectors, fleas act as reservoirs of zoonosis, playing an important role in the maintenance of disease due to their ability to live for months within rodent holes/habitats. This microclimate favors Y. pestis survival, which is eliminated with flea feces and deposited on the ground. Recent studies indicate that blow flies may act as mechanical vectors of Y. pestis, but the epidemiological impact of these organisms is still being discussed.
Pet dogs and pet cats may carry Y. pestis-infected fleas and can also develop the infection by acting as predators (e.g., by eating infected rodents). Dogs usually do not develop clinical manifestations, while cats may show the nodal forms, including pneumonic and pharyngeal disease. If they survive the infection, these animals will produce specific antibodies for up to a year, making them important sentinels for epidemiological surveillance in plague outbreaks. Birds in general are refractory to infection, but birds of prey are important in the epidemiological cycle because they may transport infected rodent carcasses and fleas over long distances. Transmission between humans can occur via aerosols due to accidents involving contaminated tissues (e.g., during field work or from lab material) or during utilization of plague bacteria as a weapon of biological warfare. Displacement of humans or animals infected with plague (or carcasses) should also be taken into consideration, because of the potential for transmission and formation of allochthonous epidemics. Transmission between humans by vectors occurs rarely and is characteristic of homes with ectoparasite infestations, such as lice ( Pediculus humanus ) and fleas ( Pulex irritans ). In the Andes, the habit of killing these insects with the teeth causes a syndrome characterized by cervical buboes, peritonsillar abscesses, and pneumonia .
4.2 Tularemia
Francisella tularensis infection has been demonstrated in more than 250 vertebrates (mammals, birds, reptiles, amphibians) and invertebrates (arthropods) around the world. Thus, there is no exclusive reservoir/host association for the disease. The fauna involved in epidemiological cycles varies from region to region, where mammalian hosts (e.g., rabbits, hares, muskrats, prairie dogs, skunks, raccoons, mice, rats, squirrels, sheep, cattle, and cats) are more commonly associated with human infection risk (Harik 2013).
Two biological cycles are currently described: terrestrial and aquatic (Carvalho et al. 2014). Tularemia type A (F. tularensis subsp. tularensis) is more associated with the terrestrial disease cycle (Fig. 11.3a), with wild rabbits and hares acting as main hosts and arthropod vectors (ticks and horse flies) as the agents spreading the pathogen. Tularemia type B (F. tularensis holarctica) is most often associated with aquatic cycles (Fig. 11.3b) but can also be transmitted by ticks. In this cycle, muskrats, beavers, and voles spread the bacteria in their aquatic habitat, and humans become infected directly by ingesting contaminated water or infected animals (e.g., fish and crayfish). There is also evidence that F. tularensis may persist in water sources in association with intracellular protozoa, aiding epidemiological maintenance.

Tularemia epidemiological cycles . (a) Terrestrial cycle and (b) aquatic cycle
In North America, ticks of the genera Dermacentor (dog tick and wood tick), Amblyomma americanum (lone star tick), and Chrysops spp. (deer flies) are the main vectors of tularemia. The animal reservoirs consist of lagomorphs, squirrels, prairie dogs, beavers, groundhogs, deer, sheep, and occasionally humans. Wild predators , such as foxes, coyotes, birds of prey, and snakes, as well as domestic dogs and cats (by nature of carnivorous behavior), typically become infected by coming into contact with infected tissues or prey.
In ticks , bacteria penetrate the midgut and migrate to the salivary glands, where they are inoculated in a new host during a blood meal. Transovarial infection has been confirmed in ticks, and they are known to remain infective during all phases of their life cycle (larva, nymph, adult). It is believed that mites and fleas are also involved in the transmission of tularemia but with lower epidemiological impact.
In Europe and in other regions of the world, the ticks Ixodes ricinus , Haemaphysalis concinna , and Dermacentor sp. are involved in the transmission of tularemia. Mosquitoes of the genera Aedes , Culex , and Anopheles are also implicated; these hematophagous insects act as mechanical vectors for the spread of bacteria, which occur via contaminated mouthparts during blood feeding after previous contact with an infected host.
Another way in which humans acquire F. tularensis is through contact with contaminated tissues or carcasses or by inhaling aerosols from contaminated land, grain , or hay during hunting activities, taxidermy, shearing, field work, land clearing, grass cutting, during the trading of wild animals, or via laboratory accidents. Interhuman transmission has not been documented for tularemia, even in cases of the pneumonic form. As with the plague, epizootics occurring in rodents and lagomorphs typically precede human cases, but the detection of infection sources can be extremely difficult due to host diversity .
5 Clinical Manifestations
The manifestation of these diseases depends on host inoculation route. The strength of invasion and the ability of the bacterium to infect and cause disease vary among different clinical presentations.
5.1 Plague
Clinically, human plague has three main forms: bubonic, septicemic, and pneumonic.
5.1.1 Bubonic Plague
Bubonic plague is the most common form of the disease, contracted after the bite of an infected flea. When bacilli are inoculated, buboes form in the lymph nodes, frequently in the inguinal-crural (70 %), axillary (20 %), and cervical (10 %) regions. In the absence of appropriate treatment, mortality rate ranges between 40 and 70 % (Koirala 2006; Prentice and Rahalison 2007). The buboes have a reddish color, glossy surface and are very painful (Fig. 11.1a2). The disease presents with chills, headache, fever, myalgia, anorexia, nausea, vomiting, generalized pain, and tachycardia (Prentice and Rahalison 2007). The incubation period is between 2 and 6 days and faster in some cases (Carniel 2008).
5.1.2 Septicemic Plague
Septicemic plague is characterized by severe toxemia and an abundance of bacilli in the blood. Bacteremia can result in necrosis due to accumulation of bacilli and their toxins in the limbs (Fig. 11.1a3), being lethal in 30–50 % of cases with improper treatment. In general, 10–20 % of cases result from progression of improperly treated bubonic plague (Koirala 2006). Clinically, septicemic plague resembles other types of septicemia caused by gram-negative bacteria . It presents a clinical picture with abrupt temperature rise, chills, arrhythmia , hypotension, nausea, vomiting, asthenia, and mental disturbance . This form has a high mortality if left untreated (Koirala 2006; Prentice and Rahalison 2007).
5.1.3 Pneumonic Plague
In clinical form, pneumonic plague is the most severe and dangerous, due to the high degree of contagion, high mortality rates (approximately 100 % if untreated and >50 % with antibiotic therapy), and high capacity to cause epidemics by spread of aerosols. Infection may occur by the introduction of bacilli into respiratory mucosa or secondarily by progression of untreated bubonic and septicemic forms (Carniel 2008). This form presents sudden onset with severe and rapid symptom progression, with abrupt temperature rise, chills, arrhythmia, hypotension, nausea, vomiting, and mental disturbance (Koirala 2006, Prentice and Rahalison 2007). Initially, signs of infection and pulmonary symptoms are either mild or absent and later arise with chest pain, shortness of breath and fast, bloody, and sputum rich in plague bacilli. Without early treatment, symptoms include delirium and coma and may cause death .
5.2 Tularemia
Depending on the route of entry of the bacteria , the disease can manifest itself in several ways (Ellis et al. 2002). Ulceroglandular tularemia is the most common form of the disease, which typically results from the bite of an infected arthropod vector or through direct contact with the tissues of infected animals. An ulcer can form and persist for several months at the site of infection (Fig. 11.1b2). After an incubation period of 3–6 days, infected persons have sudden onset of flu-like symptoms, mainly chills, fever, headache, and general aches/pains. Bacteria are spread through the lymphatic system to local lymph nodes where swelling occurs, the result often resembling plague buboes (Ellis et al. 2002). Francisella tularensis can be transmitted from the site of infection to other organs/tissues, such as the spleen, liver, lungs, kidneys, gut, central nervous system, and skeletal muscles, with less than 3 % mortality (Evans et al. 1985). A rare variation of this clinical presentation is oculoglandular tularemia , wherein the entrance of the bacterium is the conjunctiva, usually as a result of hand-eye contamination. The disease is characterized by the appearance of ulcers or nodules on the conjunctiva, with untreated infection spreading to local lymph nodes (Ellis et al. 2002).
Oropharyngeal or gastrointestinal tularemia occurs through ingestion of contaminated food or water (Berdal et al. 2000). The symptoms are described as a sore throat, enlarged tonsils, and formation of a yellow-white pseudomembrane. This form is usually accompanied by swelling of cervical lymph nodes. This clinical presentation may vary from mild diarrhea to fatal acute disease with intestinal ulceration (Ellis et al. 2002).
Pulmonary and respiratory tularemia is the most severe form, with the inhalation of aerosols as the (rare) route of infection. Any cases of natural inhalation often appear from agricultural activities that involve manipulation of hay, a common habitat of infected rodents. In most cases, this form of tularemia occurs as a clinical progression from other forms (Ellis et al. 2002).
6 Diagnosis
6.1 Plague
The diagnosis of plague can be accomplished through bacteriological, serological, and molecular techniques. These techniques can be used separately or in combination, which allows greater precision of results. For plague diagnosis, the isolation of the bacteria is still considered the gold standard (BCCDC, BC Centre for Disease Control 2013). However, not all samples from human cases are appropriate for this type of diagnosis. Automated systems for biochemical testing are not considered effective in the identification of Y. pestis ; however, biochemical tests performed with the API20E kit are accepted.
Laboratory investigation consists of bacterioscopy of smears stained using specific methods, direct immunofluorescence (DIF) with specific antibodies for F1, use of antiplague phage plaques on agar (by determining a lysis area to confirm the culture), and inoculation into laboratory animals (BCCDC, BC Centre for Disease Control 2013).
Depending on observed clinical manifestations, different sample types (e.g., bubo fluid, blood, sputum, cerebrospinal fluid, etc.) are collected for diagnostic purposes. If the patient has the bubonic form of the disease, blood and bubo fluid are collected. In cases of pneumonic plague, blood and sputum fluid are collected. In recently obtained infection, it is possible to obtain material from the mouth or from nasal secretions or through a venous or bubo puncture. Samples are packaged in the Cary-Blair transport medium , and bacilli may be maintained in these preparations for several weeks at room temperature. In rodents, the blood, liver, or spleen samples are collected. If the animal is decomposing, the femur is obtained to sample bone marrow, where plague bacilli are abundant. These techniques can also be used to identify Y. pestis in flea vectors (BCCDC, BC Centre for Disease Control 2013).
In cases where bacterial culture presents negative results but disease is still suspected, serological testing is recommended to confirm diagnosis. Serological diagnosis is mainly by hemagglutination (HA) assays , typically via hemagglutination inhibition (HI) tests . F1-sensitive sheep erythrocytes are used for the detection of anti-F1 antibody in blood serum of patients or people at risk of contact with animals. For diagnosis of plague in humans, it is recommended to collect two serum samples: one in the acute phase of the disease and another after 3 weeks. In most patients, seroconversion occurs within 1–2 weeks of the onset of symptoms, occasionally earlier (~5 days). The disease is confirmed when there is a fourfold increase in reaction titer.
The HA/HI assay is also used for diagnosis and serological surveillance of serum samples from live-captured rodents and for domestic and wild carnivore predators of rodents. The enzyme-linked immunosorbent assay (ELISA) is useful for diagnosis of human disease, used in detection of IgM or IgG and for F1 antigen capture. However, these techniques are not universally applicable in serological surveillance activities, as they require the use of different (nonhuman) species-specific antibodies, such as from rodents, dogs, cats, etc., for use in human sera tests.
Molecular techniques have some advantages over bacteriological techniques in plague diagnosis. Molecular assays are rapid techniques that eliminate the need for cultivation of samples and in which detection is possible even when bacteria are not viable. Several protocols based on polymerase chain reaction (PCR) and its variations (nested PCR, multiplex PCR, real-time PCR) have been used for this purpose. These tests are used for diagnosis in human or animal material, by means of identifying virulence genes present in the three plasmids and/or on the chromosome of Y. pestis (Dalmasso et al. 2014).
6.2 Tularemia
Tularemia diagnosis can also be done by bacteriological, serological, and molecular methods. Francisella tularensis is a challenging pathogen in relation to nutrients and has slow growth. Despite these characteristics, bacterial isolation remains the most recommended method, since it allows a conclusive diagnosis of infection and serves as a valuable resource for molecular epidemiology (Hepburn and Simpson 2008).
Appropriate sample type for use in laboratory diagnosis depends on patient clinical manifestations and can include sore throat swabs, blood or urine samples, biopsy, aspiration or scraping of ulcers, lymph node tissue, affected corneal tissue, sputum samples, and bronchial or pleural lavage. Samples of vectors, carcasses, natural host or reservoir feces, and water are all recommended for epidemiological investigations (BCCDC, BC Centre for Disease Control 2013).
Different sample types require different preparations for transportation. Skin lesion samples are stored in the Amies agar with activated charcoal. Sputum, pharyngeal secretions, and lymph node aspirate may be packed, transported, and stored at −80 °C until culture procedures for isolation of the microorganism are performed. Traditional blood transport systems are used for blood samples.
Alternatively, specimens can be plated in appropriate solid media immediately after collection, and sealed plates may then be forwarded to a biosafety level 3 (BSL3) laboratory. Bacteria grow well on chocolate agar medium supplemented with cystine/cysteine (CHAB) II or GC agar with 1 % hemoglobin and 1 % IsoVitaleX plus antibiotic when the specimen is subject to contamination by other microorganisms. Growth can be visualized after 24–48 h at 37 °C, and small, transparent colonies can be identified by slide agglutination (5 min) or by immunofluorescence using specific antibodies (IgG3, IgG2a, IgG1).
Commercially available biochemical test systems for the identification of F. tularensis fail, and conventional biochemical tests are limited by the nutritional requirements of the bacteria. Currently, conventional techniques and quantitative PCR are used to identify genes encoding F. tularensis outer membrane proteins. PCR can also detect the microorganisms directly on tissues, including skin lesions, lymph nodes, spleen, liver, kidneys, heart, lungs, oropharynx, and meninges. Recently, we developed a “toolbox” which includes all the tools, equipment, and solutions required for conventional PCR identification of bioterrorism agents in the field; the development of this system is a breakthrough for detection of this pathogen in outbreak situations.
In terms of clinical management and treatment, identification of F. tularensis at the species level is sufficient. In other situations, it is important to extend the studies to distinguish between the various F. tularensis subspecies, particularly subsp. tularensis and holarctica. This is because when they are endemic, the difference in virulence between these two particular subspecies impacts treatment and control methods, as well as the types of molecular tests that should be used.
Tularemia diagnosis can also be performed by serological methods. Antibody production in response to F. tularensis infection is commonly demonstrated by several methods, including agglutination tests , immunofluorescence assays , ELISA , Western blot (WB) , and microarray . The most commonly used method is the microscopic agglutination (MA); however, this method has some limitations (Chaignat et al. 2014).
After F. tularensis infection, antibodies appear following the end of the 2nd week of onset of symptoms, reaching titers of 1:320–1:1280; antibodies decline 2–3 months after treatment. In some cases, even after clinical recovery, antibody titers may persist for several years. Two serum samples should be collected for proper diagnosis, one in the acute phase of the disease and another in a few weeks.
Another utilized technique corresponds to ELISA but allows differentiation of immunoglobulin class; however, in tularemia, this does not differentiate between an acute episode and prior infection. Alternately, there are commercially available immunochromatographic methods, which detect specific IgM, IgG, and IgA antibodies against F. tularensis lipopolysaccharide (LPS) . These methods have high sensitivity and specificity and represent an alternative to presumptive diagnoses of tularemia in remote areas (Sharma et al. 2014).
All diagnostic procedures for both plague and tularemia should be performed in laboratories that have specialized facilities, due to the risk that these pathogens present (Fig. 11.4). Cultures and animal inoculations must be conducted in biosafety level 3 (BSL3) laboratories, while serologic tests can be performed in level 2 (NB2) .

Diagram of the different methods used for the diagnosis of plague and tularemia
7 Treatment
The treatment of plague early and intensive due to the gravity and speed of progression of these diseases and the possibility for Y. pestis and F. tularensis use as bioterrorism agents . For plague, patient isolation is recommended during the first 48 h of treatment for pneumonic forms to minimize the risk of contamination.
Both diseases may be treated with the antimicrobial aminoglycosides streptomycin and gentamicin, which are basically functionally equivalent. Both antibiotics are considered the drugs of first choice. In cases of plague, streptomycin and gentamicin use is recommended for a period of 10 days. Streptomycin is considered the gold standard, especially in cases of pneumonic plague, whereas gentamicin is prescribed for all forms of the disease, especially for pregnant women and children. Currently, gentamycin is the drug of choice for all clinical forms of plague and for tularemia (BCCDC, BC Centre for Disease Control 2013). Tularemia treatment should begin within 24 h of first symptoms and should continue for 14 days to reduce the risk of relapse (Harik 2013).
Tetracycline and chloramphenicol are second choice treatments. Tetracycline is prescribed in uncomplicated cases of plague, while chloramphenicol can be used for all clinical forms. These treatments are effective for tularemia if used for 14–21 days. In the absence of these antibiotics, sulfonamides may be used in uncomplicated cases of plague (BCCDC, BC Centre for Disease Control 2013).
The beta-lactam antibiotics (penicillins, cephalosporins, cephamycins, oxacephems, carbapenems, and monobactams), macrolides (erythromycin, clarithromycin, roxithromycin, and miocamycin), and azalides (azithromycin) should not be employed in the treatment or prophylaxis of plague or tularemia (Harik 2013). Despite the antibiotic susceptibility demonstrated for strains of Y. pestis , these antibiotics are ineffective in vivo. Their use may thereby increase the risk of complications (sepsis, pneumonia, and meningitis), including death.
Prophylaxis is recommended for individuals who were exposed to aerosols containing Y. pestis or F. tularensis . In these situations, doxycycline should be initiated immediately after exposure or up to a maximum of 24 h postexposure. However, other tetracyclines and chloramphenicol are also recommended for exposure to patients with pneumonic plague and after contact with infected fleas or bacteria. The fluoroquinolones (ofloxacin, levofloxacin, and ciprofloxacin) may be used in accordance with sensitivity profile and in the case of terrorist attack with Y. pestis (BCCDC, BC Centre for Disease Control 2013).
8 Prevention and Control
For plague and tularemia , adequate prevention through immunization is not yet possible. The available plague vaccine is rarely used because the immunity is short-lived, ineffective against bubonic plague, and fails to protect against the primary pneumonic form. For tularemia, a vaccine developed from live-attenuated microorganisms (derived from an avirulent strain) is used in the United States. This vaccine is still being evaluated for effectiveness, and its utilization is limited to professionals with high risk of exposure, such as laboratory workers that handle the microorganism (CDC 2012; WHO 2003).
For both of these zoonosis , prevention and control measures should be based on knowledge of regional characteristics, including ecological and epidemiological aspects; the presence of hosts/reservoirs and vectors; and degree or type of human exposure to infection sources.
For people who live, work, or vacate in areas of zoonosis occurrence, some measures should be taken to avoid contracting the infection and to prevent spread (CDC 2012; WHO 2003). They are:
-
Eliminate sources of food and shelter for rodents near homes, work places, and camps/recreational areas. When present in these environments, employ methods to eliminate them. Vectors should be eliminated prior to rodents, since without their usual host vectors tend to invade the home environment.
-
Control ectoparasites (fleas, ticks, and horseflies) of pet animals, and prevent pets from coming into contact with wild animals or their carcasses. Animals kept outdoors are more exposed to this contact.
-
Avoid areas infested by arthropod vectors (fleas, ticks, and horse flies). In the case of unavoidable exposure, use appropriate repellent, long-sleeved shirts, long pants tucked inside socks, closed shoes, and wide-brimmed hat to protect the face and neck . Check for fleas and ticks on clothing or skin, and if present, remove them.
-
Avoid contact with wild rodents and their nests/burrows, droppings, and carcasses. Raising guinea pigs in or near the home for human consumption is particularly risky and should be avoided. Avoid keeping exotic animals (hamsters, gerbils, chinchilla, ferret) as “pets,” as they may be carriers of various infectious agents including but not limited to Y. pestis and F. tularensis and may carry infected arthropod vectors into homes, thereby contaminating dogs, cats, and humans.
-
Be careful when handling lagomorphs, rodents, and other wild animals caught during hunting activities. When removing or abrading the skin of these animals, wear gloves, appropriate mask that covers the nose and mouth and eye protection (such as goggles). Wash hands, utensils, and surfaces thoroughly after contact with hunting-acquired raw meat, and thoroughly cook meats prior to consumption.
A public health surveillance system , when properly designed, can identify risk areas, prevent human infection, promote early detection of human cases or outbreaks, reduce mortality, and prevent the occurrence of epidemics (Table 11.1).
A global outbreak alert was established by the WHO to support the implementation of the international aspects of the International Health Regulations. This alert system depends on systematic monitoring of information concerning suspected outbreaks and on providing support for outbreak responses. This support involves the provision of technical assistance to contain the national and international public health consequences of outbreaks and is offered by the WHO upon request and acceptance by member states .
Notes
- 1.
See Chap. 3 for more information on utilization in biological warfare.
References
Achtman M, Zurth K, Morelli G et al (1999) Yersinia pestis, the cause of plague, is a recently emerged clone of Yersinia pseudotuberculosis. Proc Natl Acad Sci U S A 96(24):14043–14048
Antwerpen MH, Schacht E, Kaysser P et al (2013) Complete genome sequence of a Francisella tularensis subsp. holarctica strain from Germany causing lethal infection in common marmosets. Genome Announc 1(1):e00135–12. doi:10.1128/genomeA.00135–12
BCCDC, BC Centre for Disease Control (2013) Available in www.bccdc.ca/dis-cond/a-z/_p/Plague/overview/Plague.htm
Berdal BP, Mehl R, Haaheim H et al (2000) Field detection of Francisella tularensis. Scand J Infect Dis 32:287–291
Carniel E (2008) Pathogenic Yersinia: stepwise gain of virulence due to sequential acquisition of mobile genetic elements. In: Hensel M, Schmidt H (eds) Horizontal gene transfer in the evolution of pathogenesis, vol 8. University Press, Cambridge, pp 193–216
Carvalho CL, Lopes de Carvalho I, Zé-Zé L et al (2014) Tularemia: a challenging zoonosis. Comp Immunol Microbiol Infect Dis 37:85–96
Centers for Disease Control and Prevention (CDC) (2011) Available in www.cdc.gov/tularemia/
Centers for Disease Control and Prevention (CDC) (2012) Available in www.cdc.gov/plague/
Chaignat V, Djordjevic-Spasic M, Ruettger A et al (2014) Performance of seven serological assays for diagnosing tularemia. BMC Infect Dis 14:234. doi:10.1186/1471-2334-14-234
Dalmasso A, Civera T, Filipello V et al (2014) Multiplex primer-extension assay for identification of Yersinia species. Mol Biol Rep 41(10):6329–6333
Deng W, Burland V, Plunket G III et al (2002) Genome sequence of Yersinia pestis KIM. J Bacteriol 184:4601–4611
Eigelsbach HT, McGann V (1984) Francisella. In: Krieg WR, Holt JG (eds) Bergey’s manual of systematic bacteriology, vol 1. Williams and Wilkins, Baltimore, MD, pp 394–399
Eisen RJ, Gage KL (2009) Adaptive strategies of Yersinia pestis to persist during inter-epizootic and epizootic periods. Vet Res 40(2):1
Ellis J, Oyston PC, Green M et al (2002) Tularemia. Clin Microbiol Rev 15(4):631–646
Evans ME, Gregory DW, Schaffner W et al (1985) Tularemia: a 30-year experience with 88 cases. Medicine (Baltimore) 64(4):251–269
Harik NS (2013) Tularemia: epidemiology, diagnosis, and treatment. Pediatr Ann 42:288–292
Hepburn MJ, Simpson AJ (2008) Tularemia: current diagnosis and treatment options. Expert Rev Anti Infect Ther 6:231–240
Hinnebusch BJ, Erickson DL (2008) Yersinia pestis biofilm in the flea vector and its role in the transmission of plague. Curr Top Microbiol Immunol 322:229–248
Kingry LC, Petersen JM (2014) Comparative review of Francisella tularensis and Francisella novicida. Front Cell Infect Microbiol 4:1–12
Koirala J (2006) Plague: disease, management, and recognition of act of terrorism. Infect Dis Clin North Am 20:273–287
Larsson P, Oyston PCF, Chain P et al (2005) The complete genome sequence of Francisella tularensis, the causative agent of tularemia. Nat Genet 37:153–159
Molins CR, Delorey MJ, Yockey BM et al (2014) Virulence difference between the prototypic Schu S4 strain (A1a) and Francisella tularensis A1a, A1b, A2 and type B strains in a murine model of infection. BMC Infect Dis 14:67. doi:10.1186/1471-2334-14-67
Parkhill J, Wren BW, Thomson NR et al (2001) Genome sequence of Yersinia pestis, the causative agent of plague. Nature 413(6855):523–527
Perry R, Fetherston JD (1997) Yersinia pestis – etiologic agent of plague. Clin Microbiol Rev 10:35–66
Platonov ME, Evseeva VV, Dentovskaya SV et al (2013) Molecular typing of Yersinia pestis. Mol Gen Mikrobiol Virusol 2:3–12
Prentice MB, Rahalison L (2007) Plague. Lancet 369(9568):1196–1207
Seifert L, Harbeck M, Thomas A (2013) Strategy for sensitive and specific detection of Yersinia pestis in skeletons of the Black Death pandemic. PLoS One 8(9), e75742. doi:10.1371/journal.pone.0075742
Sharma N, Hotta A, Yamamoto Y et al (2014) Serosurveillance for Francisella tularensis among wild animals in japan using a newly developed competitive enzyme-linked immunosorbent assay. Vector Borne Zoonotoic Dis 14:234–239
Wagner DM, Klunk J, Harbeck M et al (2014) Yersinia pestis and the plague of Justinian 541–543 AD: a genomic analysis. Lancet Infect Dis 14:319–326
World Health Organization (WHO) (2003) Human plague in 2000 and 2001. Wkly Epidemiol Rec 78:130–135
Suggested Reading
Almeida AMP, Alves LC, Amaral RL et al (2003) Transmission of Yersinia pestis cultures with different plasmid content from Xenopsylla cheopis to Calomys callosus. Parasitol Res 89:159–162
Almeida AMP, Tavares C, Leal-Balbino TC (2005) Peste. In: Coura JR (ed) Dinâmica das doenças infecciosas e parasitárias, vol 126, 2nd edn. Guanabara Koogan, Rio de Janeiro, Brasil, pp 1509–1522
Dunkelberg H (2004) The history of the plague and the research on the causative agent Yersinia pestis. Int J Hyg Environ Health 207:165–178
Leal-Balbino TC, Leal NC, Lopes CV et al (2004) Differences in the stability of the plasmids of Yersinia pestis cultures in vitro: impact on virulence. Mem Inst Oswaldo Cruz 99:727–732
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Leal-Balbino, T.C., de Oliveira, M.B.M., de Barros, M.P.S., Sobreira, M., da Mota Silveira-Filho, V. (2017). Plague and Tularemia. In: Marcondes, C. (eds) Arthropod Borne Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-13884-8_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-13884-8_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-13883-1
Online ISBN: 978-3-319-13884-8
eBook Packages: MedicineMedicine (R0)