
Abstract
Invasive fungal infections have become an important cause of morbidity and mortality over the past two decades. More recently, uncommon fungi have been reported more frequently. The increased frequency may be due to an improved identification and reporting system, or an increase in the number of severely immunocompromised hosts. Diagnosing infections due to these rare or uncommon yeasts are a challenge, since the majority of the time we rely on traditional microbiologic assays and not improved diagnostic assays. In addition, the management of these types of fungal infections is difficult because of the lack of data, specifically, the lack of adequate in vitro susceptibility studies, and the paucity of any clinical treatment trials.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Non-Candida yeast
- Trichosporon
- Antifungals
- Rhodotorula
- Saccharomyces
- Malassezia
- Invasive fungal infections
- Fungemia
Introduction
Yeasts exist throughout nature in association with soil, plants, mammals, fish, and insects. For that reason, humans are constantly exposed to many yeast genera through varying routes. Depending on the interaction between host defense mechanisms and fungal virulence factors, the association between yeast and humans can be either transient or persistent, and can associated with either local infection or systemic disease. Most yeast organisms are of low virulence and generally require significant alterations or reductions in host defenses prior to tissue invasion. Recently, however, because of the increased population of immunocompromised patients, the frequency of invasive infections due to yeasts as well as the number of organisms causing disease continues to grow [1–6] (Table 9.1).
Trichosporon
Trichosporon asahii was first described in 1865 by Beigel, who identified it as the causative agent of hair infections [7]. Infections due to Trichosporon may be classified as superficial or deep. Disseminated infections are increasingly recognized in the compromised host over the past decade and are frequently fatal [1–6]. One of the first reported cases of disseminated disease was described in a 39 year-old female with lung cancer who subsequently developed a brain abscess [8].
Etiologic Agents
The genus Trichosporon was first reported by Behrend [9]. Gueho and colleagues have suggested that the species known as T. asahii may include several different Trichosporon species with epidemiological and pathogenic differences [10]. Kemker et al. using isoenzyme delineation and polymerase chain reaction (PCR) DNA fingerprinting suspect that strains that produce superficial infections are distinctly different from those strains that produce invasive infection [11]. There are currently seven species of Trichosporon. These include T. asahii (formerly, T. beigelii), the most frequently recovered species from invasive infections, and T. mucoides and T. inkin, also known to cause systemic infections [1, 2, 12–14]. T. asteroides and T. cutaneum generally produce superficial skin infections, while T. ovoides generally causes white piedra of the scalp and T. inkin, white piedra of the pubic hair. Trichosporon capitatum is now known as Blastoschizomyces capitatus [10, 12, 13].
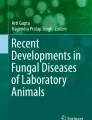
Trichosporon species are characterized by true hyphae, pseudohyphae, arthroconidia, and blastoconidia [10, 15] (Fig. 9.1). T. asahii grows readily on Sabouraud dextrose agar, producing smooth, shiny gray- to cream-colored yeast-like colonies with cerebriform radiating furrows that become dry and membranous with age. All Trichosporon species are easily identified using commercially available carbohydrate assimilation assays.

Trichosporon species produce yeast-like colonies in culture and are unique in their production of hyphae, pseudohyphae, arthroconidia, and blastoconidia (budding) both in culture and in disease. (Courtesy of D. R. Hospenthal)
Epidemiology
T. asahii is generally found in the soil, but may also be recovered from air, rivers and lakes, sewage, and bird droppings [1, 2, 12]. It rarely colonizes the inanimate environment, but can colonize the mucosal surfaces of the oropharynx, the lower gastrointestinal (GI) tract, and the skin of humans [12, 13].
More than 100 documented cases of disseminated infection due to Trichosporon species have been reported, most due to T. asahii [1, 2, 12, 13, 15]. The major risk factors associated with infection include hematologic malignancies (acute leukemia, chronic leukemia, multiple myeloma), solid tumors, and neutropenia [1, 2, 12–15]. In non-neoplastic, non-neutropenic cases, the major risk factors include corticosteroids, prosthetic valve replacement, solid organ transplantation, chronic active hepatitis, and occasionally intravenous drug use (Table 9.2). The most common portal of entry appears to be either the respiratory or GI tracts. Infrequently, central venous catheters and other vascular devices have also been implicated [12–16].
Clinical Manifestations
Trichosporonosis is classified into superficial infections (white piedra (hair shaft infection), onychomycosis, and otomycosis) and invasive infections.
Deep tissue infections may involve either a single organ or multiple organs. The most commonly infected tissue is the lungs, which accounts for approximately 33 % of all localized deep tissue infections [1, 2, 12–19]. Other sites of infection may include the peritoneum, heart valves (natural and prosthetic), retina, liver, spleen, kidneys, gallbladder, and central nervous system (brain abscess and chronic fungal meningitis) [1,2, 10–19].
The signs and symptoms of disseminated infection resemble those of systemic candidiasis and include fungemia with associated organ infection. Moreover, disseminated infections may present as either acute or chronic disease. Acute disseminated trichosporonosis often has a sudden onset and progresses rapidly, especially in neutropenic patients. Patients may develop skin lesions (~ 33 %), pulmonary infiltrates (~ 30–60 %), renal, and ocular involvement.
The metastatic cutaneous lesions generally begin as an erythematous rash with raised papules on the trunk and the extremities. The rash eventually evolves into macronodular lesion, followed by central necrosis of the nodules and occasionally the formation of hemorrhagic bullae. The pulmonary infiltrates may present as lobar consolidations, bronchopneumonia, or reticulonodular patterns.
Renal involvement occurs in > 75 % of the disseminated infection cases. Renal disease may manifest as proteinuria, hematuria, red blood cell (RBC) casts, with either acute renal failure or acute glomerulonephritis [12–16]. Urine cultures are frequently positive for Trichosporon and suggest disseminated disease, especially in immunocompromised patients [19].
Chorioretinitis is not uncommon in disseminated infection and may be a cause of visual alterations due to retinal vein occlusion or retinal detachment [12–14]. For unexplained reasons, Trichosporon has been found to have tropism for the choroid and retina. However, unlike candidal endophthalmitis, Trichosporon infects uveal tissues including the iris, but spares the vitreous [20].
During disseminated infection, any tissue in the body may become infected. The organs most frequently include the liver, spleen, GI tract, lymph nodes, myocardium, bone marrow, pleura, brain, adrenal gland, and thyroid gland [1, 2, 12–20].
In chronic disseminated infection, subtle manifestations may be present for several weeks and frequently include persistent fever of unknown etiology [1, 2, 12, 13]. The infection is similar to the entity known as chronic disseminated (hepatosplenic) candidiasis. It is generally a chronic infection of the liver, spleen, and other tissues after recovery from neutropenia. Laboratory studies frequently reveal an elevated alkaline phosphatase. Computed tomography (CT) scan or magnetic resonance imaging (MRI) frequently reveals hepatic or splenic lesions compatible with abscesses. A tissue biopsy is needed to confirm the diagnosis.
Diagnosis
The diagnosis is made with a biopsy of the skin or involved organs. Blood cultures may occasionally be useful in deep tissue infection, but are positive only late in the course of infection. Trichosporon grows readily in conventional blood culture and on standard fungal media including Sabouraud dextrose agar [15]. The presence of Trichosporon in the urine of a high-risk patient should increase the suspicion of disseminated infection.
Although there are no standardized serologic assays, the serum latex agglutination test for C. neoformans may be positive. A potential usefulness of this assay has been postulated based on the report of positive serum latex agglutination test for C. neoformans in several patients with disseminated Trichosporon infection [21, 22].
Treatment
Disseminated trichosporonosis has a mortality rate of approximately 60–70 % [2–6, 12, 13]. In most cases, however, the underlying disease contributes greatly to the overall mortality. First-line, optimal antifungal therapy has not been established. The initial step in the management of disseminated Trichosporon infection should be to decrease or reverse immunosuppression.
In vitro susceptibility studies of Trichosporon species are limited (Table 9.3). In vitro susceptibility assays of T. asahii reveal fluconazole MIC90 of 4.0 µg/ml, itraconazole MIC90 of 0.25 µg/ml, and amphotericin B MIC90 of 4.0 µg/ml. In general, most strains have relatively high MICs for polyenes, flucytosine, and echinocandins, with relatively low MICs for the azoles. Among the newer triazoles, voriconazole and posaconazole have demonstrated excellent in vitro activity [22–26]. Although not yet approved, isavuconazole also shows significant in vitro activity against most strains of Trichosporon (Table 9.4) [25]. In fact, it appears to have better activity than fluconazole [25]. In vitro and animal models suggest that azoles and not polyenes are more effective in the eradication of Trichosporon species [1, 2, 20]. Suggested therapy for the treatment of disseminated disease includes the use of either voriconazole 3 mg/kg IV or 200 mg orally twice daily, fluconazole 400–800 mg/day, or itraconazole 400–600 mg/day (Table 9.4). A potential option in patients failing azole therapy may also include a combination of an azole with an echinocandin. Serena et al. demonstrated in vitro synergy and improved outcomes in an animal model of trichosporonosis with either the combination of amphotericin B/micafungin or fluconazole/micafungin [12, 14, 24, 25]. However, because of the high MICs to polyenes and echinocandins, these antifungals should not be used alone or as first-line therapy. In a patient with disseminated infection and poor response to therapy, in vitro susceptibility testing of recovered isolates may be a helpful adjunct.
Saccharomyces
Saccharomyces is an ascomycetous yeast found throughout nature. Saccharomyces is commonly known as “brewer’s yeast” or “baker’s yeast.” It is best known for its commercial use in beer and wine production, in health food supplements, and more recently, its use in DNA recombinant technology. Occasionally, these yeasts have been reported to cause severe infection in immunocompromised hosts [15]. Species include S. cerevisiae, S. boulardii (a subtype of S. cerevisiae), S. fragilis, and S. carlsbergensis. Saccharomyces may occasionally be part of the normal flora of the GI and genitourinary tracts [1, 2, 27]. Recently, S. cerevisiae has been found to cause mucosal and disseminated infection in humans, primarily in immunocompromised hosts [27–29].
Etiologic Agents
Cells are oval to spherical and exist as either haploids or diploids. When present, ascospores, one to four in number, are in either tetrahedral or linear arrangement and stain Gram negative; vegetative cells stain Gram positive. Colonies are smooth, moist, and either white or cream colored. Saccharomyces are generally nonpathogenic due to innate low virulence [15, 30–32]. Investigators evaluating more than 3300 yeast cultures obtained from cancer patients found only 19 isolates of S. cerevisiae. Recent studies by Clemons et al. using an animal model have been able to show that some strains of S. cerevisiae, when introduced into CD-1 mice, can proliferate and resist clearance in vivo, supporting the role of S. cerevisiae as a cause of clinical infection in humans [32].
Epidemiology
Isolation of Saccharomyces species from human surfaces is rarely of any clinical significance. It has been recovered from the bloodstream, lungs, peritoneal cavity, esophagus, urinary tract, and vagina [2–6, 27, 30, 33]. Genotyping studies evaluating the relatedness between clinical strains and commercial strains of S. cerevisiae have demonstrated that commercial products may occasionally be a contributing factor in human colonization and infection [34]. Nyirjesy et al. reported that four women suffering from recurrent S. cerevisiae vaginitis had also experienced exposure to bread dough that contained identical strains S. cerevisiae [29].
The risk factors associated with Saccharomyces infections are similar to the risk factors associated with candidemia and systemic candidiasis; including central venous catheters, neutropenia, use of antimicrobials, GI tract surgery, and occasionally HIV [28, 35–37]. The portal of entry for invasive disease is most likely the oropharynx or GI tract [36].
Clinical Manifestations
Manifestations are generally nonspecific and indistinguishable from those associated with candidemia and invasive candidiasis. In addition, Saccharomyces has been associated with bloodstream infections, endocarditis, peritonitis, disseminated disease, and vaginitis [1–6, 29, 33, 35–39].
Fungemia is the most common form of infection, occurring in approximately 70 % of reported cases. As in invasive candidiasis, it is seen primarily in the immunocompromised host and tends to be associated with the use of intravascular catheters, chemotherapy, and/or antimicrobials [27, 28, 36]. Manifestations are similar to those of systemic candidiasis and candidemia. Overall, fever unresponsive to broad-spectrum antimicrobials is the most frequent manifestation. Unlike infections due to Candida species, most patients survive.
In addition, it is not uncommon for other organ systems to become infected, including the respiratory tract, with several documented episodes of pneumonia and empyema. Diagnosis is generally established by histopathology, since Saccharomyces can colonize the respiratory tract without producing invasive disease [27, 36, 40]. Saccharomyces has also been reported to produce peritonitis, cholecystitis, and endocarditis [27, 36]. All cases of endocarditis were associated with prosthetic valves and intravenous heroin use. Furthermore, two out of the three patients were cured with antifungal therapy alone; only one patient had their valve replaced. There have also been several documented cases of urinary tract infections due to S. cerevisiae [29]. All patients had underlying urologic abnormalities or were associated with fungemia [36].
Mucosal infections due to S. cerevisiae have also been reported. Sobel et al. reported on 17 women with difficult to manage vaginitis due to S. cerevisiae [26, 29]. In fact, the women with symptomatic vaginitis had manifestations indistinguishable from those caused by C. albicans. All patients had a history of chronic vaginitis unresponsive to conventional antifungals and all but two had systemic or local predisposing factors.
Diagnosis
Because of the fact that Saccharomyces species have a tendency to be nonpathogenic, the decision to attribute a causal role to S. cerevisiae is difficult [2–6]. Diagnostic difficulty occurs when the organism is recovered from body sites that may be colonized by Saccharomyces, especially in the absence of symptoms of infection. Unless the organism is found in the bloodstream, it is frequently necessary to determine whether these yeasts are causing true infection versus colonization. This is generally done via a histopathologic examination. S. cerevisiae readily grows from blood culture bottles and on Sabouraud dextrose media [2–6, 34].
Treatment
It is often difficult to assess the role of antifungal therapy in patients with infection due to Saccharomyces. There are several reports that document the resolution of fungemia and infection just by removing the intravascular catheter without providing antifungal therapy [35, 36]. Most experts advocate removing the focus of infection, whether it is an indwelling or tunneled intravenous catheter and the concurrent use of antifungal agents [36]. In vitro susceptibility studies reveal that S. cerevisiae, when compared to C. albicans isolates, are less susceptible to most antifungals, including azoles [1–5, 26] (Table 9.3). Although clinical trials have not been conducted and in vitro susceptibility assays are not standardized, Saccharomyces species appear to be susceptible to most antifungals including amphotericin B, 5-flucytosine, ketoconazole, clotrimazole, miconazole, and terconazole [1–5, 26] (Table 9.4).
Rhodotorula
Yeasts of the genus Rhodotorula are found worldwide from a variety of sources and is generally considered a contaminant when identified. Infections are occasionally seen primarily in immunocompromised hosts [2–6].
Etiologic Agents
Yeasts of the genus Rhodotorula are imperfect basidiomycetous yeasts belonging to the family Cryptococcaceae. Currently, eight species in the genus Rhodotorula are recognized [2–6, 41]. Rhodotorula mucilaginosa (formerly R. rubra) is the species most frequently associated with human infections. The other species include R. glutinis, R. pilimanae, R. pallida, R. aurantiaca, R. minuta. Most Rhodotorula species produce red-to-orange colonies due to the presence of carotenoid pigments [15, 42]. The yeast is mucoid, encapsulated, and readily grows on many types of culture media.
Epidemiology
Rhodotorula can be isolated from a variety of sources including seawater, plants, air, food, fruit juices, and occasionally from humans [1–6, 15, 41, 42]. It is not unusual to recover it as an airborne laboratory contaminant. Rhodotorula can also be recovered from shower curtains, bathtub–wall junctions, and toothbrushes. In humans, Rhodotorula can be recovered from skin, nails, respiratory tract, urinary tract, GI tract, and bloodstream [1–6, 15, 41–46].
R. mucilaginosa and R. glutinis account for approximately 0.5 % of yeast isolated from the oral cavity and more than 12 % of yeast isolates recovered from stool and rectal swabs [47]. The recovery of Rhodotorula from non-sterile human sources such as mucosal sites has been of questionable clinical significance. Although a number of invasive infections have been documented, risk factors include underlying immunosuppression (malignancy, neutropenia, corticosteroids, collagen vascular disease, and uncontrolled diabetes mellitus), use of broad-spectrum antimicrobials, and central venous catheters.
Clinical Manifestations
Manifestations are generally nonspecific, and may vary from subtle and mild to severe, including septic shock. Rhodotorula have been incriminated in a wide spectrum of infections including bloodstream infections, endocarditis, peritonitis, meningitis, and disseminated disease [2–6, 41, 43, 46–57] (Table 9.5).
Fungemia is the most common form of infection and is generally due to intravascular catheter infection [1–6, 41, 43, 46–57]. Fever of unknown etiology that is unresponsive to broad-spectrum antimicrobials is the most frequent manifestation associated with fungemia.
Meningitis has also been described in patients with acute leukemia, HIV infection, and postoperatively [52, 53]. The organisms are generally recovered from the cerebrospinal fluid (CSF) on culture, and frequently seen on an India ink stain. In addition, several cases of R. rubra peritonitis have been described in patients undergoing continuous ambulatory peritoneal dialysis. In these patients, environmental cultures revealed a possible common source outbreak. In all patients, the symptoms were subtle and intermittent at first, consisting of abdominal pain, anorexia, nausea, and occasional diarrhea [2, 54, 57].
Diagnosis
In the most proven infections, Rhodotorula is recovered from a sterile site of infection. In these cases, the decision to attribute a causal role to Rhodotorula is relatively simple, and the patient should be treated appropriately for an invasive fungal infection. The more difficult decision is when the organism is recovered from nonsterile body sites that may normally harbor Rhodotorula species, especially in the absence of signs or symptoms of infection [41, 46, 57]. In this setting, it is essential to establish the presence of infection and not just colonization.
Treatment
As with many of the uncommon yeast isolates, it is difficult to assess the role of antifungal therapy in patients infected with Rhodotorula. Optimal management of patients with indwelling catheters and infection due to Rhodotorula has not been well defined. There are several case reports that document the clearance of fungemia and the resolution of infection by removing the intravascular catheter without providing antifungal therapy [2–6, 26, 54–58]. On the other hand, there are also several documented case reports that have suggested that antifungal treatment alone may suffice without having to remove the central venous catheter. Since infections due to Rhodotorula have been severe and life threatening, it is probably best to manage these infections aggressively with catheter removal and antifungal therapy.
In vitro susceptibility studies reveal that Rhodotorula are susceptible to amphotericin B and flucytosine, but less susceptible to azoles and resistant to echinocandins [2–6, 26, 54–58] (Table 9.3). Although clinical trials have not been conducted, it appears that amphotericin B with or without flucytosine is the best recommendation for antifungal therapy at this time [1–6]. In view of the intrinsic resistance of Rhodotorula to the azoles and echinocandins, these agents should not be used as monotherapy unless in vitro susceptibility activity has been assessed.
Malassezia
Malassezia furfur is a yeast commonly found on human skin. It has been well documented to cause superficial skin infections such as pityriasis (tinea) versicolor and folliculitis. In addition, in immunocompromised host, it may occasionally cause invasive infection.
Etiologic Agents
The genus Malassezia consists of several species, the two most frequently isolated species include M. furfur and M. pachydermatis [1–6, 15]. The other less commonly isolated species includes M. sympodialis, M. slooffiae, M. globosa, M. obtuse, and M. restricta. M. furfur is the dominant species recovered in humans as a fungal pathogen. M. furfur is a dimorphic, lipophilic yeast that is unable to synthesize medium- or long-chain fatty acids and thus has a strict in vitro requirement for exogenous fatty acids of the C12 and C14 series [15, 59, 60]. Although it exists primarily in the yeast form, it may also form filamentous structures on the skin when the organism is associated with superficial infections [59, 60]. Because of its nutritional requirements, M. furfur is difficult to recover from clinical specimens unless its presence is suspected and special preparations are made by the microbiology laboratory. The second most common species is M. pachydermatis, which is generally associated with infections in dogs producing otitis externa [59, 60]. Occasionally, however, it has been implicated in human infections [59, 60]. Both Malassezia species, when grown under favorable conditions, produce clusters of oval-to-round, thick-walled yeast cells, with unipolar buds that form repeatedly from the same pole of the parent cell. This gives rise to the characteristic “collarette” at the bud site. Media such as Sabouraud dextrose agar, chocolate agar, trypticase soy agar with 5 % sheep blood all require the addition of supplements such as olive oil, in order to permit the growth of this organism [15]. M. pachydermatis, however, does not require exogenous lipids for growth, can be recovered on conventional fungal media, and its colonies tend to be dry, and white to creamy in color.
Epidemiology
Malassezia is frequently found on normal individuals colonizing the skin. Distribution of this colonization tends to correlate with the more oily areas, most likely because of the organisms’ requirement of exogenous fatty acids found in those areas. Thus, it is found primarily on the scalp, shoulders, chest, and back [60, 61]. The highest colonization rates are found in teenagers (> 90 %).
The isolation of M. furfur from newborns is reported to be less than 10 % in non-intensive care settings. However, it has been reported to be greater than 80 % in neonatal intensive care units [59–61]. Risk factors associated with increased colonization rates in neonates include prematurity, duration of hospitalization in the intensive care unit (ICU), use of occlusive dressings, and prolonged antimicrobial use [59–62]. Although the epidemiology of disseminated infection in adults has not been well studied, there appear to be several risk factors that are frequently associated with deep-seated infections (Table 9.6). These include prematurity, central venous catheters, total parenteral nutrition, parenteral lipid preparations, and immunocompromised state [60, 62–65]. Molecular epidemiologic studies using DNA fingerprinting have concluded that within the neonatal ICU there is longitudinal persistence of both M. furfur and M. pachydermatis strains [60, 62].
Clinical Manifestations
Malassezia generally produces superficial skin infections, such as pityriasis (tinea) versicolor, or folliculitis. From time to time, Malassezia may produce a deep-seated or hematogenous infections [60, 62–65]. The first reported case of systemic infection was described in 1981 in a premature neonate who developed fungemia and vasculitis while on lipid therapy [64]. Since then, numerous reports describing disseminated infection have been published [59–62]. The manifestations of disseminated infection vary from subclinical and mild symptomatology, such as fever, to sepsis with associated multi-organ dysfunction [59–62]. The majority of the Malassezia infections are diagnosed in premature infants. Occasionally, they may be seen in adults. The most commonly reported manifestations of systemic infection include fever unresponsive to broad-spectrum antimicrobials, bradycardia, respiratory distress, hepatosplenomegaly, and lethargy.
Diagnosis
Laboratory findings include leukocytosis and thrombocytopenia. Chest X-ray frequently reveals bilateral pulmonary infiltrates (> 50 %) [1–6, 60, 62]. Occasionally, the diagnosis of disseminated infection can be made by a Gram stain of the buffy coat of blood. The budding yeast cells may be observed using different stains such as Giemsa, periodic acid–Schiff (PAS), Gomori’s methenamine silver (GMS) or Calcofluor white. Blood cultures are usually negative unless the infection is initially suspected and the laboratory uses a lipid-enriched media. The recovery of the organisms is enhanced by using the lysis centrifugation blood culture technique [60, 66]. Palmitic acid (3 %) supplementation may also improve the recovery of Malassezia [60, 66].
Treatment
Management of M. furfur fungemia and disseminated infection are controversial. Most authorities recommend prompt removal of the central venous catheter and discontinuation of intravenous lipids [60, 62–64]. In most cases without a deep-seated infection, removal of the central venous catheter and discontinuation of lipids is all that is needed to clear the infection. This treatment modality accomplishes two objectives: it eradicates the nidus of infection and removes the nutritional requirements of the organism. If fungemia persists or there is evidence of deep-seated infection, it is prudent to initiate antifungal therapy. Fortunately, Malassezia species are susceptible to azoles and polyenes [1–6, 67] (Table 9.3). In vitro susceptibility assays of M. furfur strains demonstrate that most of the isolates are susceptible to amphotericin B, ketoconazole (MIC range < 0.05–0.4 µg/ml), miconazole (MIC range 0.4–> 50 µg/ml), and fluconazole. Most of the isolates are intrinsically resistant to flucytosine (MIC90 > 100 µg/ml) [1–6, 26, 60]. Although randomized clinical trials have not been conducted, in most situations, either fluconazole 400 mg/day or amphotericin B 0.7 mg/kg/day is sufficient to eradicate the infection (Table 9.4). Based on excellent in vitro activity, itraconazole and voriconazole are also alternate choices.
Other Yeast
In addition to the yeasts discussed thus far, fewer reports have been published of infection due to other yeasts. These include Blastoschizomyces, Sporobolomyces, Pichia (formerly Hansenula), and Exophiala.
Blastoschizomyces
Blastoschizomyces capitatus (formerly Geotrichum capitatum or Trichosporon capitatum) infections, although less common than those due to T. asahii, have been well described in the literature [2–6, 67]. B. capitatus is found in wood and poultry, but has also been recovered from sputum and normal intact skin [15]. Geographically, it appears to be the opposite of T. asahii, with B. capitatus infections found primarily in Europe and T. asahii found in North America [2–6, 68]. In most cases, the major risk factors include neutropenia and underlying hematologic malignancies. Although the portal of entry is unknown, it is suspected to be either the respiratory tract, GI tract, or central venous catheter [2–6, 68].
Infection may involve a single organ or multiple organs and may be associated with fungemia. The clinical spectrum of disseminated infection is similar to that of systemic candidiasis and includes fungemia with or without organ infection [2–6, 68]. By and large, the manifestations begin with fever of unknown etiology and unresponsive to antimicrobials. Diagnosis can be made with blood cultures or on biopsy of the skin or affected organs. Blood cultures are reportedly seen in > 80 % of cases [68]. B. capitatus easily grows in blood culture bottles and on fungal specific media [15]. Although skin lesions are commonly seen, fungal stains and cultures from biopsied skin lesions are frequently negative [15, 68].
Mortality rates between 60 and 80 % are generally described [68]. However, underlying disease, persistent neutropenia, and concurrent infections are significant contributing factors to this overall mortality rate. Optimal therapy has not yet been established. Until recently, however, most patients have received amphotericin B [2]. As with all fungal infections, the initial step is to decrease or reverse the immunocompromised state. In vitro susceptibility studies demonstrate that the organism is susceptible to amphotericin B (MIC90 0.12 µg/ml), and less susceptible to azoles such as fluconazole and ketoconazole (0.04–32 µg/ml), but appears to be susceptible to itraconazole and voriconazole. Most isolates are resistant to flucytosine [2, 15] (Table 9.3). The current recommendation is to use amphotericin B at a dose of 1–1.5 mg/kg/day [1–6]. However, since the newer azoles, voriconazole and posaconazole have demonstrated good in vitro activity that they may also be suitable alternatives [69].
Sporobolomyces
Sporobolomyces are yeast-like organisms that belong to the family Sporobolomycetaceae. These yeast are found throughout the world in soil, bark, and decaying organic material. They have occasionally been associated with infections in humans. There are seven known species of Sporobolomyces, but only three have been documented to cause disease, S. salmonicolor, S. holsaticus, and S. roseus. To date, there have been only six documented cases of Sporobolomyces infections; a nasal polyp, one case of dermatitis, one case of infected skin blisters, one case of mycetoma, and two cases of disseminated infection in patients with AIDS (lymph node and bone marrow) [2, 70]. In vitro susceptibility studies show that S. salmonicolor is susceptible to amphotericin B and the imidazoles [1, 2, 15, 69, 70] (Table 9.3). Despite the fact that these organisms are saprophytic, the case reports indicate their potential ability to produce invasive infection in humans, especially, in a compromised host.
References
Hospenthal DR. Uncommon fungi. In: Mandell GL, Bennett JE, Dolin R, editors. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. 7th Ed. Philadelphia: Elsevier Churchill Livingstone; 2010:3365–76.
Vazquez JA. Rhodotorula, Saccharomyces, Malassezia, Trichosporon, Blastoschizomyces, and Sporobolomyces. In: Kauffman CA, Pappas PG, Sobel JD, Dismukes, WE editors. Essentials of clinical mycology. New York: Springer; 2011:227–39.
McCall MJ, Baddley JW. Epidemiology of emerging fungi and fungi-like organisms. Curr Fungal Infect Rep 2010;4:203–09.
Micelli MH, Diaz JA, Lee SA. Emerging opportunistic yeast infections. Lancet Infect Dis. 2011;11:142–51.
Chitasombat MN, Kofteridis DP, Jiang Y, Tarrand J, Lewis RE, Kontoyiannis DP. Rare opportunistic (non-Candida, non-Cryptococcus) yeast bloodstream infections in patients with cancer. J Infect. 2012;64:68–75.
Yamamoto M, Takakura S, Hotta G, Matsumura Y, Matsushima A, Nagao M, Ito Y, Ichiyama S. Clinical characteristics and risk factors of non-Candida fungaemia. BMC Infect Dis. 2013;13:1–6.
Beigel H. The human hair: its growth and structure (1865), as cited by Langenon M. In Darier S, et al: Nouvelle Praqt Dermatol (Paris, Masson, Cie) 1936;2:377.
Watson KC, Kallichurum S. Brain abscess due to Trichosporon cutaneum. J Med Microbiol. 1970;3:191–93.
Behrend G. Ubertrichomycosis nodosa. Berlin Lin Wochenschr. 1890;27:464.
Gueho E, de Hoog GS, Smith MT, Meyer SA. DNA relatedness, taxonomy, and medical significance of Geotrichum capitatum. J Clin Microbiol. 1997;25:1191–4.
Kemeker BJ, Lehman PF, Lee JW, Walsh TJ. Distinction of deep vs. superficial clinical and non-clinical environmental isolates of Trichosporon beigelii by isoenzymes and restriction fragment length polymorphisms of rDNA generated by the polymerase chain reaction. J Clin Microbiol. 1991;29:1677–83.
Colombo AL, Padovan AC, Chaves GM. Current knowledge of Trichosporon spp. and Trichosporonosis. Clin Microbiol Rev. 2011;24:682–700.
Ruan SY, Chien JY, Hsueh PR. Invasive trichosporonosis caused by Trichosporon asahii and other unusual Trichosporon species at a medical center in Taiwan. Clin Infect Dis. 2009;49:e11–17.
Chagas-Neto TC, Chaves GM, Melo ASA, Colombo AL. Bloodstream infections due to Trichosporon spp.: species distribution, Trichosporon asahii genotypes determined on the basis of ribosomal DNA intergenic spacer 1 sequencingm and antifungal susceptibility testing. J Clin Microbiol. 2009;47:1074–1081.
Kwon-Chung KJ, Bennett JE. Infections due to Trichosporon and other miscellaneous yeast-like fungi. In: Medical mycology. Philadelphia: Lea & Febiger; 1992:768–94.
Ebright JR, Fairfax MR, Vazquez JA. Trichosporon asahii, a non-Candida yeast that caused fatal septic shock in a patient without cancer or neutropenia. Clin Infect Dis. 2001;33:28–30.
Keay S, Denning D, Stevens DA. Endocarditis due to Trichosporon beigelii: in vitro susceptibility of isolates and review. Rev Infect Dis. 1991;13:383–86.
Sheikh HA, Mahgoub S, Badi K. Postoperative endophthalmitis due to Trichosporon cutaneum. Brit J Ophthalmol. 1986;58:591–4.
Sun W, Su J, Xu S, Yan D. Trichosporon asahii causing nosocomial urinary tract infections in intensive care unit patients: genotypes, virulence factors and antifungal susceptibility testing. J Med Microbiol. 2012;61:1750–7.
Walsh TJ, Lee JW, Melcher GP, et al. Experimental Trichosporon infection in persistently granulocytopenia rabbits: implications for pathogenesis, diagnosis, and treatment of an emerging opportunistic mycosis. J Infect Dis. 1992;166:121–33.
Seeliger HPR, Schroter R. A serologic study on the antigenic relationships of the form genus Trichosporon. Sabouraudia. 1963;2:248–63.
Campbell CK, Payne AL, Teall AJ, Brownell A, Mackenzie DW. Cryptococcal latex antigen test positive in a patient with Trichosporon beigelii. Lancet. 1985;2:43–44.
Paphitou NI, Ostrosky-Zeichner L, Paetznick VL, Rodriguez JR, Rex JH. In vitro antifungal susceptibilities of Trichosporon species. J Clin Microbiol. 2003;46:1144–6.
Serena C. Pastor FJ, Gilgado F, Mayayo E, Guarro J. Efficacy of micafungin in combination with other drugs in a murine model of disseminated Trichosporonosis. Antimicrob Agents Chemother. 2005;49:497–502.
Hizirolan G, Canton E, Sahin S, Arikan-Akdagli S. Head-to-head comparison of inhibitory and fungicidal activities of fluconazole, itraconazole, voriconazole, posaconazole, and isavuconazole against clinical isolates of Trichosporon asahii. Antimicrob Agent Chemother. 2013;57:4841–7.
Guinea J, Recio S, Escribano P, Palaez T, Gama B, Bouza E. In vitro antifungal activities of isavuconazole and comparators against rare yeast pathogens. Antimicrob Agent Chemother. 2010;54:4012–4.
Enache-Angoulvant A, Hennequin C. Invasive Saccharomyces Infection: a comprehensive review. Clin Infect Dis. 2005;41:1559–68.
Nielsen H, Stenderup J, Bruun B. Fungemia with Saccharomycetaceae. Report of four cases and review of the literature. Scand J Infect Dis. 1990;22:581–4.
Nyirjesy P, Vazquez JA, Ufberg DD, Sobel JD, Boikov DA, Buckley HR. Saccharomyces cerevisiae vaginitis: transmission from yeast used in baking. Obstet Gynecol. 1995;86:326–9.
Morrison VA, Haake RJ, Weisdorf DJ. The spectrum of non-Candida fungal infections following bone marrow transplantation. Medicine. 1993;72:78–89.
Holzschu DL, Chandler FW, Ajello L, Ahearn DG. Evaluation of industrial yeast for pathogenicity. Sabouradia. 1979;17:71–8.
Clemons KV, McCusker JH, Davis RW, Stevens DA. Comparative pathogenesis of clinical and non-clinical isolates of Saccharomyces cerevisiae. J Infect Dis. 1994;169:859–67.
Eng RH, Drehmel R, Smith SM, Goldstein EJ. Saccharomyces cerevisiae infections in man. Sabouraudia. 1984;22:403–7.
McCullough MJ, Clemons KV, Farina C, McCusker JH, Stevens DA. Epidemiological investigation of vaginal Saccharomyces cerevisiae isolates by a genotypic method. J Clin Microbiol. 1998;36:557–62.
Cimolai N, Gill M J, Church D. Saccharomyces cerevisiae fungemia: case report and review of the literature. Diagn Microbiol Infect Dis. 1987;8:113–7.
Aucott JN, Fayen J, Grossnicklas H, Morrissey A, Lederman MM, Salata RA. Invasive infection with Saccharomyces cerevisiae: report of three cases and review. Rev Infect Dis. 1990;12:406–11.
Sethi N, Mandell W. Saccharomyces fungemia in a patient with AIDS. NY State J Med. 1988;88:278–9.
Rubinstein E, Noriega ER, Simberkoff MS, Holzman R, Rahal Jr JJ. Fungal endocarditis: analysis of 24 cases and review of the literature. Medicine. 1975;54:331–44.
Canafax DM, Mann HJ, Dougherty SH. Postoperative peritonitis due to Saccharomyces cervisiae treated with ketoconazole. Drug Intell Clin Pharm. 1982;16:698–9.
Chertow GM, Marcantonio ER, Wells RG. Saccharomyces cerevisiae empyema in a patient with esophagopleural fistula complicating variceal sclerotherapy. Chest. 1991;99:1518–9.
Fell JW, Tallman AS, Ahearn DG. Genus Rhodotorula Harrison. In: Kreger-van Rij NJW, ed. The yeasts: a taxonomic study. 3rd Ed. Amsterdam: Elsevier Science Publishers; 1984:893–905.
Rippon JW. Medical mycology. The pathogenic fungi and pathogenic actinomycetes. 3rd Ed. Philadelphia: W. B. Saunders; 1988:610–1.
Kiehn TE, Gorey E, Brown AE, Edwards FF, Armstrong D. Sepsis due to Rhodotorula related to use of indwelling central venous catheters. Clin Infect Dis. 1992;14:841–6.
Ahearn DG, Jannach JR, Roth FJ. Speciation and densities of yeasts in human urine specimens. Sabouraudia. 1966;5:110–9.
Saez H. Etude ecologique sur les Rhodotorula des homotherms. Rev Med Vet. 1979;130:903–908.
Anaissie E, Bodey GP, Kantarjian H, et al. New spectrum of fungal infections in patients with cancer. Rev Infect Dis. 1989;11:369–78.
Rose HD, Kurup VP. Colonization of hospitalized patients with yeast-like organisms. Sabouraudia. 1977;15:251–6.
Leeber DA, Scher I. Rhodotorula fungemia presenting as “endotoxic” shock. Arch Intern Med. 1969;123:78–81.
Rusthoven JJ, Feld R, Tuffnell PG. Systemic infection by Rhodotorula spp. in the immunocompromised host. J Infect. 1984;8:241–6.
Braun DK, Kauffman CA. Rhodotorula fungemia: a life-threatening complication of indwelling central venous catheters. Mycoses. 1992;35:305–8.
Louria DB, Greenberg SM, Molander DW. Fungemia caused by certain nonpathogenic strains of the family Cryptococcaceae. N Engl J Med. 1960;263:1281–4.
Pore RS, Chen J. Meningitis caused by Rhodotorula. Sabouraudia. 1976;14:331–5.
Gyaurgieva OH, Bogomolova TS, Gorshkova GI. Meningitis caused by Rhodotorula rubra in an HIV-infected patient. J Med Vet Mycol. 1996;34:357–9.
Tuon FF, Costa SF. Rhodutorula infection. A systematic review of 128 cases from literature. Rev Iberoam Micol. 2008;25:135–40.
Garcia Suarez J Gomez Herruz P Cuadros JA Burgaleta C. Epideimiology and outcome of Rhodutorula infection in haematological patients. Mycoses. 2011;54:318–24.
Mori T, Nakamura Y, Kato J, Sugita K, Murata M, Kamei K. Fungemia due to Rhodutorula mucilaginosa after allogeneic hematopoietic stem cell transplantation. Transpl Infect Dis. 2011;14:91–4.
Spiliopoulou A, Anastassiou ED, Christofidou M. Rhodutorula fungemia of an intensive care unit patient and review of published cases. Mycopathologia. 2012;174:301–9.
Diekema DJ, Petroelje B, Messer SA, Hollis RJ, Pfaller MA. Activities of available and investigational agents against Rhodotorula species. J Clin Microbiol. 2005;43:476–8.
Marcon MJ, Powell DA. Human infections due to Malassezia spp. Clin Microbiol Rev. 1992;5:101–19.
Gaitanis G, Magiatis P, Hantscheke M, Bassukas ID, Velegraki A. The Malassezia genus in skin and systemic diseases. Clin Microbiol Rev. 2012;25:106–41.
Ingham E, Cunningham AC. Malassezia furfur. J Med Vet Mycol. 1993;31:265–88.
Marcon MJ, Powell DA. Epidemiology, diagnosis and management of M. furfur systemic infection. Diagn Microbiol Infect Dis. 1987;10:161–75.
Barber GR, Brown AE, Kiehn TE, Edwards FF, Armstrong D. Catheter-related Malassezia furfur fungemia in immunocompromised patients. Am J Med. 1993;95:365–70.
Weiss SJ, Schoch PE, Cunha BA. Malassezia furfur fungemia associated with central venous catheter lipid emulsion infusion. Heart Lung. 1991;20:87–90.
van Belkum A Boekhout T Bosboom R. Monitoring spread of Malassezia infections in a neonatal intensive care unit by PCR-medicated genetic typing. J Clin Microbiol. 1994;32:2528–32.
Nelson SC, Yau YC, Richardson SE, Matlow AG. Improved detection of Malassezia species in lipid-supplemented peds plus blood culture bottles. J Clin Microbiol. 1995;33:1005–7.
Gemeinhardt H. Lungenpathogenitat von Trichosporon capitatum beim menschen. Zentrablatt fur Bakteriolgie (Series A). 1965;196:121–33.
Martino P, Venditti M, Micozzi A, et al. Blastoschizomyces capitatus: an emerging cause of invasive fungal disease in leukemia patients. Rev Infect Dis. 1990;12:570–82.
Espinel-Ingroff A. Comparison of in vitro activities of the new triazole SCH56592 and the echinocandins MK-0991 (L-743,872) and LY303366 against opportunistic filamentous and dimorphic fungi and yeast. J Clin Microbiol. 1998;36:2950–6.
Morris JT, Beckius M, McAllister CK. Sporobolomyces infection in an AIDS patient. J Infect Dis. 1991;164:623–4.
Suggested Reading
Chitasombat MN, Kofteridis DP, Jiang Y, Tarrand J, Lewis RE, Kontoyiannis DP. Rare opportunistic (non-Candida, non-Cryptococcus) yeast bloodstream infections in patients with cancer. J Infect. 2012;64:68–75.
Colombo AL, Padovan AC, Chaves GM. Current knowledge of Trichosporon spp. And Trichosporonosis. Clin Microbiol Rev. 2011;24:682–700.
Diekema DJ, Petroelje B, Messer SA, Hollis RJ, Pfaller MA. Activities of available and investigational agents against Rhodotorula species. J Clin Microbiol. 2005;43:476–8.
Enache-Angoulvant A, Hennequin C. Invasive Saccharomyces Infection: a comprehensive review. Clin Infect Dis. 2005;41:1559–68.
Espinel-Ingroff A. Comparison of in vitro activities of the new triazole SCH56592 and the echinocandins MK-0991 (L-743,872) and LY303366 against opportunistic filamentous and dimorphic fungi and yeast. J Clin Microbiol. 1998;36:2950–6.
Gaitanis G, Magiatis P, Hantscheke M, Bassukas ID, Velegraki A. The Malassezia genus in skin and systemic diseases. Clin Microbiol Rev. 2012;25:106–41.
Garcia Suarez J Gomez Herruz P Cuadros JA Burgaleta C. Epideimiology and outcome of Rhodutorula infection in haematological patients. Mycoses. 2011;54:318–24.
Guinea J, Recio S, Escribano P, Palaez T, Gama B, Bouza E. In vitro antifungal activities of isavuconazole and comparators against rare yeast pathogens. Antimicrob Agent Chemother. 2010;54:4012–4.
Marcon MJ, Powell DA. Human infections due to Malassezia spp. Clin Microbiol Rev. 1992;5:101–9.
Martino P, Venditti M, Micozzi A, et al. Blastoschizomyces capitatus: an emerging cause of invasive fungal disease in leukemia patients. Rev Infect Dis. 1990;12:570–82.
McCall MJ, Baddley JW. Epidemiology of emerging fungi and fungi-like organisms. 2010;4:203–209.
Micelli MH, Diaz JA, Lee SA. Emerging opportunistic yeast infections. Lancet Infect Dis. 2011;11:142–51.
Vazquez JA. Rhodotorula, Saccharomyces, Malassezia, Trichosporon, Blastoschizomyces, and Sporobolomyces. In: Kauffman CA, Pappas PG, Sobel JD, Dismukes, WE. editors. Essentials of clinical mycology. New York: Springer; 2011:227–39.
Yamamoto M, Takakura S, Hotta G, Matsumura Y, Matsushima A, Nagao M, Ito Y, Ichiyama S. Clinical characteristics and risk factors of non-Candida fungaemia. BMC Infect Dis. 2013;13:1–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Vazquez, J. (2015). Infection Due to Non-Candidal Yeasts. In: Hospenthal, D., Rinaldi, M. (eds) Diagnosis and Treatment of Fungal Infections. Infectious Disease. Springer, Cham. https://doi.org/10.1007/978-3-319-13090-3_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-13090-3_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-13089-7
Online ISBN: 978-3-319-13090-3
eBook Packages: MedicineMedicine (R0)