
Abstract
ACE inhibitors are commonly used to treat hypertension and congestive heart failure.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Congestive Heart Failure
- Angiotensin Convert Enzyme
- Angiotensin Convert Enzyme Inhibitor
- Vascular Malformation
- Mucosal Edema
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
43.1 Uses
ACE inhibitors are commonly used to treat hypertension and congestive heart failure.
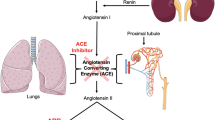
43.2 Mechanism
ACE inhibitors are believed to result in angioedema through increased bradykinin activity, which causes transient vasodilation and extravasation of fluid into the extracellular space, resulting in soft tissue edema. ACE inhibitor-induced angioedema is a class effect and is not dose dependent.
43.3 Discussion
The use of ACE inhibitors is believed to be the most common cause of angioedema, comprising approximately 35 % of all cases of angioedema. Conversely, angioedema occurs in approximately 0.1–1 % of patients treated with ACE inhibitors. ACE inhibitor-induced angioedema is primarily localized in the head and neck, especially in the face, mouth, tongue, lips, and larynx. The distribution of involvement tends to be diffuse and bilateral (Fig. 43.1), although focal or unilateral lingual and peritonsillar edema have been reported (Fig. 43.2). Patients with suspected angioedema are typically assessed clinically and via laryngoscopy, but may present for radiological imaging. The edema of the affected tissues appears as relatively low attenuation on CT and as low T1 and high T2 signal on MRI, without much abnormal enhancement. Patients often present shortly after initiating ACE inhibitors, but can sometimes develop angioedema many years after starting the medication. The severity of angioedema can also vary considerably from benign facial swelling to severe airway obstruction. Treatment consists of stopping the medication, instituting steroids and antihistamines, and supportive care for airway protection, which may require intubation or tracheotomy.

Diffuse AACE inhibitor induced angioedema. Axial contrast-enhanced CT image shows circumferential mucosal pharyngeal swelling (arrows) and diffuse stranding of the parapharyngeal and subcutaneous fat bilaterally

Focal ACE inhibitor angioedema. Sagittal T1-weighted (a), axial (b) and coronal T2-weighted (c), and coronal post-contrast T1-weighted (d) MR images show diffusely massive tongue edema (arrows)
43.4 Differential Diagnosis
Several other drugs, such as rituximab, alteplase, fluoxetine, laronidase, lepirudin, and tacrolimus, can also cause angioedema. Otherwise, the imaging differential diagnosis for angioedema includes infection, longus coli calcific tendonitis, vascular malformations (Fig. 43.5), and neoplasms (Fig. 43.6).
-
Phlegmon appears as ill-defined areas of hypoattenuation and swelling on CT, while abscess is characterized by a rim-enhancing fluid collection (Fig. 43.3). Clinical parameters, such as fever and elevated white blood cell count, are typically present.
Fig. 43.3 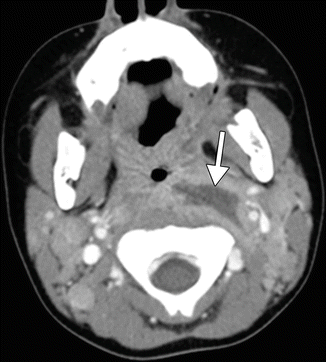
Retropharyngeal abscess. Axial contrast-enhanced CT image shows a discrete rim-enhancing fluid collection in the left retropharyngeal space (arrow), consistent with abscess
-
Longus colli calcific tendonitis can present with prevertebral space edema. Identifying a calcification on CT along the course of the tendon helps to make the diagnosis (Fig. 43.4). Patients can present with neck pain and fever.
Fig. 43.4 
Longus colli calcific tendonitis. Axial contrast-enhanced CT images in the soft tissue (a) and bone (b) windows obtained at different levels show an effusion in the prevertebral space (arrowhead) and a rounded calcification in the left longus colli tendon (arrow)
-
Vascular malformations, such as lymphatic malformations (Fig. 43.5), can present as focal or diffusely infiltrative trans-spatial lesions. These lesions are often initially diagnosed in children or young adults. Patients may present acutely due to hemorrhage within such a lesion.
Fig. 43.5 
Microcystic lymphatic malformation of the tongue. Axial (a) and coronal (b) fat-suppressed T2 and axial (c) and coronal (d) post-contrast fat-suppressed T1 MR images show a lesion mainly in the right oral tongue (arrows)
-
Neoplasms, such as squamous cell carcinoma (refer to Chaps. 1, 2, and 8), can present as an infiltrative mass in the oral cavity or pharynx. Tumors typically demonstrate enhancement, but may contain areas of necrosis that do not enhance.
-
Radiation therapy for head and neck cancers of the aerodigestive track often produces diffuse pharyngeal mucosal edema (Fig. 43.6). This is generally mild and chronic and may be accompanied by other changes, such as subcutaneous fat reticulation.
Fig. 43.6 
Radiation-induced pharyngeal mucosal edema. The patient had a history of head and neck squamous cell cancer treated with chemoradiotherapy. Axial (a) and coronal (b) CT images show diffuse edema in the region of the hypopharynx as well as stranding of the subcutaneous fat




Suggested Reading
Al-Khudari S, Loochtan MJ, Peterson E, Yaremchuk KL. Management of angiotensin-converting enzyme inhibitor-induced angioedema. Laryngoscope. 2011;121(11):2327–34.
Chiu AG, Newkirk KA, Davidson BJ, Burningham AR, Krowiak EJ, Deeb ZE. Angiotensin-converting enzyme inhibitor-induced angioedema: a multicenter review and an algorithm for airway management. Ann Otol Rhinol Laryngol. 2001;110(9):834–40.
Ee YS, Sow AJ, Goh BS. Unilateral tongue angioedema caused by angiotensin-converting enzyme inhibitor. J Laryngol Otol. 2010;124(12):1337–9.
Raman SP, Lehnert BE, Pruthi S. Unusual radiographic appearance of drug-induced pharyngeal angioedema and differential considerations. AJNR Am J Neuroradiol. 2009;30(1):77–8.
Winters ME, Rosenbaum S, Vilke GM, Almazroua FY. Emergency department management of patients with ACE-inhibitor angioedema. J Emerg Med. 2013;45:775–80.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Ginat, D.T., Johnson, J.M. (2015). Angiotensin Converting Enzyme (ACE) Inhibitors. In: Ginat, D., Small, J., Schaefer, P. (eds) Neuroimaging Pharmacopoeia. Springer, Cham. https://doi.org/10.1007/978-3-319-12715-6_43
Download citation
DOI: https://doi.org/10.1007/978-3-319-12715-6_43
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-12714-9
Online ISBN: 978-3-319-12715-6
eBook Packages: MedicineMedicine (R0)