
Abstract
Once the tumor spreads into a lymph node, it expands the node, and the spherical node becomes rounded. Then, the capsule is invaded, leading to extension to adjacent tissues which is called “extracapsular extension”. Extracapsular extension impacts prognosis and survival of patients with head and neck cancers significantly.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Neck Dissection
- Clinical Target Volume
- Extracapsular Extension
- Lateral Neck Dissection
- Retropharyngeal Node
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
FormalPara OverviewThe head and neck region has a rich lymphatic network which is divided into sublevels in order to define the regions for surgical neck dissection and radiotherapy. Head and neck cancers have specific routes for lymphatic spread according to their locations. More than 30 % of head and neck tumors are clinically lymph node positive at the time of diagnosis [1], and more than 30 % of patients who are clinically negative have pathologically involved lymph nodes.
Tumors of certain locations do not require elective nodal treatment, as the risk for lymphatic metastasis is less than 5 % (i.e., small tumors of the lip, T1–T2 tumors of the glottic larynx). For the salivary gland, tonsil, paranasal sinus, and middle ear tumors, small tumors of the buccal mucosa and retromolar trigone, and oral tongue tumors not exceeding midline, ipsilateral neck treatment is adequate, whereas for tumors such as the nasopharynx, supraglottic and infraglottic larynx, hypopharynx, soft palate, and base of tongue, bilateral neck treatment is indicated. In case of ipsilateral positive lymph nodes, contralateral neck is also at risk as the metastatic nodes obstruct the lymphatic trunks.
The risk of lateral retropharyngeal lymph node involvement is related to the primary site and neck stage [2]; the medial retropharyngeal nodes are almost never the site of metastatic disease.
1 Introduction
Once the tumor spreads into a lymph node, it expands the node, and the spherical node becomes rounded. Then, the capsule is invaded, leading to extension to adjacent tissues which is called “extracapsular extension”. Extracapsular extension impacts prognosis and survival of patients with head and neck cancers significantly.
Nodal areas in the neck are divided into superficial and deep chains. Retropharyngeal and parapharyngeal nodes constitute the latter. The sternocleidomastoid (SCM) muscle divides the neck into two large triangles. The external jugular vein and the platysma muscle are located superficially, where the internal jugular vein, the carotid artery, and some of the cranial nerves are located deeply to the SCM muscle. There are seven lymph node levels proposed by the American Joint Committee on Cancer (AJCC) for head and neck cancers and are shown by Roman numerals (levels I–VII) [3]. These levels are not recommended to be used for lymphomas. Beside these lymph nodes, supraclavicular, retrostyloid space, retropharyngeal, preauricular, intraparotid, buccal, retroauricular, suboccipital, facial, and mastoid lymph nodes, which are not routinely dissected, may also be involved in head and neck cancers. Retropharyngeal nodes are divided into two as medial and lateral. They extend through the internal carotid arteries medially and finally drain into level II lymph nodes. Certain lymphatics have special names: Virchow’s node is used for supraclavicular, Delphian’s node is used for the precricoid node, and Rouviere’s node is the most superior node in the retropharyngeal region (alongside the jugular foramen, and clinically inaccessible).
Different types of neck dissection are performed for particular sites. In radical neck dissection , levels I–V lymph nodes along with superficial and deep cervical fascia they are located in are removed together with the SCM muscle, omohyoid muscle, submandibular gland, internal and external jugular veins, and cranial nerve (CN) XI (spinal accessory nerve). In modified radical dissection , same levels are removed with both fascia, but internal jugular vein, CN XI, or one or more leaves of SCM muscle are not removed. These two techniques require at least ten nodes to be removed. If other lymphatic groups (such as retropharyngeal, levels VI and VII) or non-lymphatic structures (such as the carotid artery, the skin, or the parotid gland) are also removed, it is called an “extended radical dissection ”. Selective neck dissection is the technique where one or more levels of lymph nodes are not removed, but at least six nodes should be sent for pathologic evaluation. In supraomohyoid dissection (for small oral cavity tumors) levels I–III, in lateral neck dissection (for larynx, oropharynx, and hypopharynx cancers) levels II–IV, in posterolateral neck dissection levels II–V, and in anterior compartment neck dissection level VI are removed. In superselective neck dissection , only the lymph nodes with the highest potential for spread are removed. Following neck dissection, shunts of lymphatic flow develop towards the opposite neck. Also, a previously irradiated neck may have atypical lymphatic drainage [1].
Risks of clinical and pathological bilateral lymph node metastasis of certain head and neck tumors are shown in Table 3.1 [1, 4–9].
2 Evidence-Based Treatment Approaches
Neck irradiation may be performed in negative necks electively (adjuvant or definitive), and in positive necks either preoperatively or postoperatively [10, 11]. Elective neck radiotherapy (RT) has local control (LC) rates similar to elective neck dissection, and neither has an effect on survival [12, 13]. However, Piedbois et al. showed a survival advantage of elective neck dissection over RT in 233 patients with early-stage oral cavity cancers [14]. The decision between RT and dissection is given according to the treatment method for the primary disease. Indications for an elective neck treatment depend on the stage and the grade of the primary lesion. Radiotherapy (RT) (45–50 Gy) is justified in patients with a 20 % or higher risk of occult lymphatic metastatis. Thus, early lesions of the paranasal sinuses, nasal vestibule and nasal cavity, lip, and glottic larynx do not require elective neck RT [15, 16]. The University of Florida published their results for elective neck RT [17, 18]. They observed neck failure in 5 and 21 % of patients who did and did not receive elective neck RT, respectively.
Neck dissection is indicated following RT in patients with multiple, large, and fixated lymph nodes. If positive lymph nodes regress completely after RT, subsequent neck dissection is not necessary [19–22]. The University of Florida recommends following the patients with CT performed after 4 weeks of the last day of RT, and withholding neck dissection if the risk of residual disease is under 5 % [23].
There are two trials showing the efficacy of neck irradiation with a concomitant boost scheme. Peters et al. treated 100 patients with oropharyngeal cancer who had cervical lymph node metastases [24]. Among 62 patients who had complete response to RT, 7 recurred in the neck. Neck control rate was 86 % at 2 years. Subcutaneous fibrosis rate was not different from a group of patients who received RT and neck dissection. Johnson et al. reported complete response in 72 % of 81 patients with lymph node metastases [25]. Among these, 5 % had recurrence in the neck. 3-year neck control was 94 %, and 86 % for <3-cm and >3-cm lymph nodes, respectively. In Mayo Clinic’s study, 5-year neck recurrence-free survivals in patients treated with neck dissection only were 76 % for N1, 60 % for N2, and 69 % overall [26].
If neck dissection is “planned” after RT, doses of 50–70 Gy are delivered according to the size and the mobility of the lymph nodes [27]. If the nodes are fixed and/or the primary disease is treated with RT, the neck should be treated with RT followed by neck dissection. With a planned dissection following a decreased dose of RT, LC is increased, and complications such as fibrosis and cranial nerve palsy are decreased compared to high-dose RT alone.
If RT is to follow surgery, it is generally performed within 4–6 weeks; however, waiting for 10 weeks at most did not affect LC of the neck negatively [27, 28]. In dissected necks with negative margins, 60–65 Gy are prescribed, whereas higher doses are needed for positive margins or residual disease [28–30].
Chao et al. reported the results of 126 patients with head and neck cancer who were treated with IMRT [31]. They observed that most of neck failures were seen within the high-risk region, which was described as CTV1.
As different doses are prescribed for the primary region and the neck according to the presence of residual disease, lymph node metastatis, or extracapsular extension (ECE), Mohan et al. developed “simultaneous integrated boost” in order to be able to prescribe different doses to different regions without decreasing fraction size [32]. Butler et al. defined “simultaneous modulated accelerated radiation therapy ” (SMART) where they prescribed 2.4 Gy to high-risk disease in order to minimize the overall treatment time [33]. In RTOG 00–22 study, patients with early-stage oropharyngeal cancer, who had no chemotherapy, received 66 Gy with daily fraction sizes of 2.2 Gy to primary tumor and metastatic nodes, where subclinical disease received 54–60 Gy with daily fraction sizes of 1.8–2 Gy [34]. They found 2-year local failure (LF) rate of 9 % with grade 2 or higher xerostomia rates of 16 % and other toxicities even less. In the study of Ozyigit et al., 2 and 1.2 Gy daily were prescribed to high-risk and low-risk diseases, respectively [35]. The patients were also receiving chemotherapy. They reported no increase in LF in areas receiving 1.2 Gy daily. However, 2-year disease-free survival (DFS) was lower compared to high-dose areas (78 % vs. 94 %).
The decision for prophylactic neck treatment depends on the probability of occult metastasis . This limit is 20 % or higher for many American centers, whereas in Europe, neck treatment is performed if the risk is 5–10 % or higher [36]. In N0 necks, retropharyngeal (RP) lymph nodes should be included in tumors infiltrating the posterior pharynx wall (e.g., nasopharyngeal, hypopharyngeal, oropharyngeal). In tumors of the subglottic or transglottic larynx, and hypopharynx with extension to the esophagus, level VI nodes should be delineated. In nasopharynx cancer, bilateral levels I–V together with RP lymph nodes should be irradiated. According to Byers, this is also the case for N1 necks without ECE [37].
In the majority of patients with N2b disease, levels I–V should be treated [1]. However, in larynx and oral cavity tumors, one may omit level I and level V lymph nodes, respectively (in case they are not metastatic). This is also the case in postoperative patients. In tumors located in the midline or have bilateral lymph node drainage, contralateral neck should be treated. In patients with neck dissection who have indication for neck irradiation, levels I–V should be treated with previously described exceptions [1].
Lymph node positivity rates of specific regions are shown in Table 3.2 [1, 2, 4–6, 38, 39].
3 Levels of Drainage for Certain Locations of Tumors
Each head and neck subsite have particular pattern of lymphatic drainage [40]:
-
Level Ia : This level drains the mid-lower lip, anterior oral tongue, anterior floor of the mouth, anterior alveolar mandibular ridge, and skin of the chin.
-
Level Ib : These nodes are sentinel to maxillary sinus and oral cavity tumors. They drain submandibular gland, anterior and lower nasal cavity, upper and lower lips, hard and soft palates, nasopharynx, anterior of oral tongue, cheeks, maxillary and mandibular alveolar ridges, medial canthus, and soft tissues of the midface.
-
Level II : This region contains the sentinel lymph nodes for oropharyngeal, oral cavity, supraglottic laryngeal, hypopharyngeal, and thyroid gland cancers. It also drains lymphatics from the nasopharynx, nasal cavity, glottic and subglottic larynx, salivary glands, paranasal sinuses, face, middle ear, and external auditory canal. Oropharyngeal and nasopharyngeal tumors drain to level IIb lymph nodes.
-
Level III : These lymph nodes are sentinel for subglottic laryngeal and thyroid gland tumors. They also drain nasopharynx, hypopharynx, oropharynx (tonsils, base of the tongue), supraglottic and glottic larynx, paranasal sinuses, and oral cavity tumors.
-
Level IV : It drains the larynx, hypopharynx, nasopharynx, and cervical esophagus.
-
Level V : It drains the nasopharynx, oropharynx (tonsils, base of the tongue), apex of piriform sinus, subglottic larynx, cervical esophagus, thyroid gland, occipital and parietal scalp, postauricular and nuchal regions, and skin of the lateral and posterior neck and shoulder.
-
Level VI : Prelaryngeal lymph nodes are sentinel for glottic and subglottic laryngeal and thyroid gland tumors. They also drain the hypopharynx, cervical esophagus, and apex of the piriform sinus tumors.
-
Retropharyngeal Nodes : They are sentinel for ethmoid sinus, nasal cavity, and nasopharynx cancers, but also drain the oropharynx, hypopharynx, supraglottic larynx, maxillary sinus, and soft palate.
4 Radiologic Boundaries for Lymph Node Levels of the Neck
-
Radiologic boundaries for level I lymph nodes are described in Table 3.3 (Fig. 3.1) [40].
Table 3.3 Radiologic boundaries for level I lymph nodes Fig. 3.1 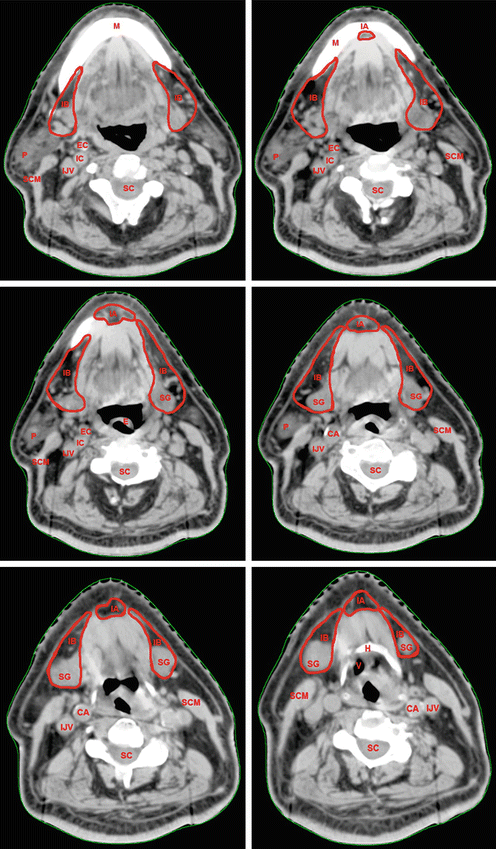
Delineation of level I lymph nodes. Tip: find C1 transverse process to begin level II in case of N(−); otherwise, find jugular foramen (JF) in N(+) neck (see Fig. 3.6 to see JF) (H hyoid bone, IB level IB, IA Level 1A, SG submandibular gland, P parotid gland, SC spinal cord, IJV internal jugular vein, IC internal carotid artery, EC external carotid artery, CA common carotid artery, E epiglottis, V vallecula, M mandible, SCM sternocleidomastoid muscle)
-
Radiologic boundaries for level II lymph nodes are described in Table 3.4 (Fig. 3.2).
Table 3.4 Radiologic boundaries for level II lymph nodes Fig. 3.2 
Delineation of level II lymph nodes. Tip: yellow line just at the posterior edge of IJV divides level II into A and B. (SG submandibular gland, P parotid gland, SC spinal cord, IJV internal jugular vein, IC internal carotid artery, EC external carotid artery, CA common carotid artery, E epiglottis, V vallecula, M mandible, SCM sternocleido mastoid muscle, H hyoid bone, D dens of axis, C1 C1 cervical vertebrae)
-
Radiologic boundaries for level III lymph nodes are described in Table 3.5 (Fig. 3.3).
Table 3.5 Radiologic boundaries for level III lymph nodes Fig. 3.3 
Delineation of level III lymph nodes (SC spinal cord, IJV internal jugular vein, CA common carotid artery, SCM sternocleido mastoid muscle, H Hyoid bone, TC Thyroid cartilage, Cr Cricoid cartilage, TG Thyroid gland, SA Scalenus anterior muscle, JV Jugular vein)
-
Radiologic boundaries for level IV lymph nodes are described in Table 3.6 (Fig. 3.4).
Table 3.6 Radiologic boundaries for level IV lymph nodes Fig. 3.4 
(a, b) Delineation of level IV lymph nodes (SC spinal cord, SCM sternocleido mastoid muscle, H hyoid bone, TC thyroid cartilage, Cr cricoid cartilage, TG thyroid gland, SA scalenus anterior muscle, SP scalenus posterior muscle, Tr trachea,T1 T1 vertebrae, E esophagus, Cl clavicle, RL right lung, LL left lung)
-
Radiologic boundaries for level V lymph nodes are described in Table 3.7 (Fig. 3.5).
Table 3.7 Radiologic boundaries for level V lymph nodes Fig. 3.5 
Delineation of level V lymph nodes (SG submandibular gland, SC spinal cord, IJV internal jugular vein, CA common carotid artery, SCM sternocleido mastoid muscle, PS pyriform sinus, T trapezius muscle, tc transverse cervical vessels, TG thyroid gland, TC thyroid cartilage, Cr cricoid cartilage)
-
Radiologic boundaries for level VI lymph nodes are described in Table 3.8 (Fig. 3.6).
Table 3.8 Radiologic boundaries for level VI lymph nodes Fig. 3.6 
Delineation of level VI lymph nodes (Level VIa red, Level IVb aqua). (EJV external jugular vein, IJV internal jugular vein, CA common carotid artery, SCM sternocleido mastoid muscle, Sc scalenius muscle, E esophagus, TG thyroid gland, LCo longus colli muscle, LCa longus capitis muscle)
-
Radiologic boundaries for retrostyloid space are described in Table 3.9.
Table 3.9 Radiologic boundaries for retrostyloid space -
Radiologic boundaries for supraclavicular fossa lymph nodes are described in Table 3.10.
Table 3.10 Radiologic boundaries for supraclavicular fossa lymph nodes -
Radiologic boundaries for retropharyngeal lymph nodes are described in Table 3.11 (Fig. 3.7).
Table 3.11 Radiologic boundaries for retropharyngeal lymph nodes Fig. 3.7 
Delineation of retropharyngeal lymph nodes. (SG submandibular gland, P parotid gland, SC spinal cord, IJV internal jugular vein, IC internal carotid artery, CA common carotid artery, H hyoid bone, V vallecula, M mandible, SCM sternocleido mastoid muscle, BS brain stem, JF jugular foramen, D Dens of axis, St Styloid process)







5 Target Volume Determination and Delineation Guidelines
-
Gross Tumor Volume for Lymph Nodes (GTVn): It should include the grossly involved lymph nodes detected by clinical examination, CT, MRI, PET/CT, and intraoperative findings, if operated. In postoperative cases, GTVn is not stated as it is assumed to be grossly resected.
-
Clinical Target Volume for Lymph Nodes (CTVn): CTV1 for definitive IMRT is defined as GTV of the primary tumor and GTVn with specific margins. CTV2 is formed by adding high-risk regions for tumor involvement of the primary tumor and metastatic lymph nodes with a 1-cm margin to CTV1. CTV3 includes the uninvolved lymph nodes, and these nodal stations are also called “elective” or “prophylactically treated” nodal regions.
-
For postoperative cases, preoperative GTV with 1–2-cm margin including the whole surgical bed and metastatic lymph nodes with ECE is defined as CTV1. CTV2 includes the uninvolved lymph nodes, which are the elective nodal regions in this case. In regions adjacent to parotid glands, deep lobes of the glands are not delineated as critical organs to prevent a decrease in LC in the parapharyngeal space.
-
The presence of ECE has a significant importance in terms of LC and survival. Huang et al. reported that patients with ECE required RT in order to improve LC as they have higher risk of recurrence in the neck [41]. In patients with neck dissection and no ECE, CTVn should include wider margins than negative necks, and a 2–3 mm of skin sparing is necessary to decrease skin toxicity [1]. In patients with neck dissection who have ECE, CTVn should have wider margins (including sternocleidomastoid (SCM) and/or paraspinal muscles), and in the regions where there is ECE, the skin is more generously included in CTV. If the muscular fascia is invaded, the entire muscle should be delineated as CTV [40].
-
In patients with positive neck, borders of levels differ from the borders in negative necks. If level II lymph nodes are positive, the cranial border starts from the skull base in order to include the jugular fossa. If level IV nodes are positive, the caudal border ends at the clavicular head, to include the supraclavicular region [31].
-
In patients with no neck dissection, studies showed that the size of the lymph node is important on estimating the risk of ECE [42–46]. If the lymph node is smaller than 1 cm, the risk of ECE is 17–43 %. However, when it exceeds 3 cm, the risk may rise up to 95 %. As we do not have pathologic evaluation in patients without neck dissection, the size of the nodes should be taken into account, and generous margins should be added for larger ones. A study from MD Anderson Cancer Center reported that margins of 5 and 10 mm are adequate for covering 90 and 100 % of microscopic ECE, respectively [47].
-
In 2014, radiation oncologists from the Danish Head and Neck Cancer Group (DAHANCA), the European Organization for Research and Treatment of Cancer (EORTC), the Hong Kong Nasopharyngeal Cancer Study Group (HKNPCSG), the National Cancer Institute of Canada Clinical Trials Group (NCIC CTG), the Radiation Therapy Oncology Group (RTOG), and the Trans Tasman Radiation Oncology Group (TROG) published a new recommendation guideline for the delineation of neck node levels with the cooperation of an anatomist and a head and neck surgeon [48].
This recent guidelines divided the neck node levels into ten subsites. There is no significant difference in the description and delineation of levels I, II, and III. However, levels IV, VI, and VII were subdivided into two, whereas level V was subdivided into three subgroups, and levels VIII, IX, and X were recently proposed.
They described level IVa lymph nodes as the previous level IV (e.g., lower jugular lymph nodes) and level IVb as the medial supraclavicular lymph nodes which lie between the anterior border of the scalenus muscle and the apex of the lung. The previously described level V was subdivided into level Va and Vb lymph nodes separated by the caudal edge of the cricoid cartilage. Level Vc was recently proposed for the lateral supraclavicular lymph nodes which lie lateral to the scalenus muscle and lateral border of level IVa. Level VI was also divided into VIa and VIb lymph nodes as anterior jugular, and prelaryngeal, pretracheal, and paratracheal lymph nodes, respectively. The previously defined retropharyngeal and retrostyloid lymph nodes were named as levels VIIa and VIIb, respectively. In level VIIb lymph nodes, lateral retropharyngeal nodes were solely included, excluding the medial nodes. The parotid lymph nodes (e.g., preauricular, intraparotid, and subparotid nodes) were defined as level VIII, whereas the malar and buccofacial nodes were defined as level IX lymph nodes. Level X was subdivided into levels Xa and Xb which contain retro- and subauricular and occipital lymph nodes, respectively.
-
Planning Target Volume (PTV): A margin of 3 mm is added in all directions; however, it may be minimized to 1 mm in areas adjacent to critical structures.
-
Guidelines for Clinical Target Volumes of the Neck
Guidelines for clinical target volumes of the neck are shown in Table 3.12.
Table 3.12 Guidelines for clinical target volumes of the neck -
Recommendations for Target Volume Dose Prescriptions
Recommendations for target volume dose prescriptions are summarized in Table 3.13.
Table 3.13 Recommendations for target volume dose prescriptions
References
Chao KS et al (2002) Determination and delineation of nodal target volumes for head-and-neck cancer based on patterns of failure in patients receiving definitive and postoperative IMRT. Int J Radiat Oncol Biol Phys 53(5):1174–1184
McLaughlin MP et al (1995) Retropharyngeal adenopathy as a predictor of outcome in squamous cell carcinoma of the head and neck. Head Neck 17(3):190–198
Robbins KT et al (2002) Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck Surg 128(7):751–758
Bataini JP et al (1985) Natural history of neck disease in patients with squamous cell carcinoma of oropharynx and pharyngolarynx. Radiother Oncol 3(3):245–255
Byers RM, Wolf PF, Ballantyne AJ (1988) Rationale for elective modified neck dissection. Head Neck Surg 10(3):160–167
Lindberg R (1972) Distribution of cervical lymph node metastases from squamous cell carcinoma of the upper respiratory and digestive tracts. Cancer 29(6):1446–1449
Northrop M et al (1972) Evolution of neck disease in patients with primary squamous cell carcinoma of the oral tongue, floor of mouth, and palatine arch, and clinically positive neck nodes neither fixed nor bilateral. Cancer 29(1):23–30
Woolgar JA (1999) Histological distribution of cervical lymph node metastases from intraoral/oropharyngeal squamous cell carcinomas. Br J Oral Maxillofac Surg 37(3):175–180
Buckley JG, MacLennan K (2000) Cervical node metastases in laryngeal and hypopharyngeal cancer: a prospective analysis of prevalence and distribution. Head Neck 22(4):380–385
Dubray BM et al (1993) Is reseeding from the primary a plausible cause of node failure? Int J Radiat Oncol Biol Phys 25(1):9–15
Mendenhall WM et al (2002) Planned neck dissection after definitive radiotherapy for squamous cell carcinoma of the head and neck. Head Neck 24(11):1012–1018
Vandenbrouck C et al (1980) Elective versus therapeutic radical neck dissection in epidermoid carcinoma of the oral cavity: results of a randomized clinical trial. Cancer 46(2):386–390
Fakih AR et al (1989) Elective versus therapeutic neck dissection in early carcinoma of the oral tongue. Am J Surg 158(4):309–313
Piedbois P et al (1991) Stage I-II squamous cell carcinoma of the oral cavity treated by iridium-192: is elective neck dissection indicated? Radiother Oncol 21(2):100–106
Mendenhall WM et al (1989) Is elective neck treatment indicated for T2N0 squamous cell carcinoma of the glottic larynx? Radiother Oncol 14(3):199–202
Mendenhall WM et al (1988) T1-T2 vocal cord carcinoma: a basis for comparing the results of radiotherapy and surgery. Head Neck Surg 10(6):373–377
Mendenhall WM, Million RR (1986) Elective neck irradiation for squamous cell carcinoma of the head and neck: analysis of time-dose factors and causes of failure. Int J Radiat Oncol Biol Phys 12(5):741–746
Mendenhall WM, Million RR, Cassisi NJ (1980) Elective neck irradiation in squamous-cell carcinoma of the head and neck. Head Neck Surg 3(1):15–20
Bartelink H (1983) Prognostic value of the regression rate of neck node metastases during radiotherapy. Int J Radiat Oncol Biol Phys 9(7):993–996
Bartelink H, Breur K, Hart G (1982) Radiotherapy of lymph node metastases in patients with squamous cell carcinoma of the head and neck region. Int J Radiat Oncol Biol Phys 8(6):983–989
Bataini JP et al (1987) Impact of neck node radioresponsiveness on the regional control probability in patients with oropharynx and pharyngolarynx cancers managed by definitive radiotherapy. Int J Radiat Oncol Biol Phys 13(6):817–824
Maciejewski B (1987) Regression rate of metastatic neck lymph nodes after radiation treatment as a prognostic factor for local control. Radiother Oncol 8(4):301–308
Liauw SL et al (2006) Postradiotherapy neck dissection for lymph node-positive head and neck cancer: the use of computed tomography to manage the neck. J Clin Oncol 24(9):1421–1427
Peters LJ et al (1996) Neck surgery in patients with primary oropharyngeal cancer treated by radiotherapy. Head Neck 18(6):552–559
Johnson CR et al (1998) Radiotherapeutic management of bulky cervical lymphadenopathy in squamous cell carcinoma of the head and neck: is postradiotherapy neck dissection necessary? Radiat Oncol Investig 6(1):52–57
Olsen KD et al (1994) Primary head and neck cancer. Histopathologic predictors of recurrence after neck dissection in patients with lymph node involvement. Arch Otolaryngol Head Neck Surg 120(12):1370–1374
Mendenhall WM et al (1988) Squamous cell carcinoma of the head and neck treated with radiation therapy: the impact of neck stage on local control. Int J Radiat Oncol Biol Phys 14(2):249–252
Amdur RJ et al (1989) Postoperative irradiation for squamous cell carcinoma of the head and neck: an analysis of treatment results and complications. Int J Radiat Oncol Biol Phys 16(1):25–36
Marcus RB Jr, Million RR, Cassissi NJ (1979) Postoperative irradiation for squamous cell carcinomas of the head and neck: analysis of time-dose factors related to control above the clavicles. Int J Radiat Oncol Biol Phys 5(11–12):1943–1949
Million RR (1979) Squamous cell carcinoma of the head and neck: combined therapy: surgery and postoperative irradiation. Int J Radiat Oncol Biol Phys 5(11–12):2161–2162
Chao KS et al (2003) Patterns of failure in patients receiving definitive and postoperative IMRT for head-and-neck cancer. Int J Radiat Oncol Biol Phys 55(2):312–321
Mohan R et al (2000) Radiobiological considerations in the design of fractionation strategies for intensity-modulated radiation therapy of head and neck cancers. Int J Radiat Oncol Biol Phys 46(3):619–630
Butler EB et al (1999) Smart (simultaneous modulated accelerated radiation therapy) boost: a new accelerated fractionation schedule for the treatment of head and neck cancer with intensity modulated radiotherapy. Int J Radiat Oncol Biol Phys 45(1):21–32
Eisbruch A et al (2010) Multi-institutional trial of accelerated hypofractionated intensity-modulated radiation therapy for early-stage oropharyngeal cancer (RTOG 00–22). Int J Radiat Oncol Biol Phys 76(5):1333–1338
Chao KS, Ozyigit G, Thorsdad WL (2003) Toxicity profile of intensity-modulated radiation therapy for head and neck carcinoma and potential role of amifostine. Semin Oncol 30(6 Suppl 18):101–108
Weiss MH, Harrison LB, Isaacs RS (1994) Use of decision analysis in planning a management strategy for the stage N0 neck. Arch Otolaryngol Head Neck Surg 120(7):699–702
Byers RM (1985) Modified neck dissection. A study of 967 cases from 1970 to 1980. Am J Surg 150(4):414–421
Candela FC, Kothari K, Shah JP (1990) Patterns of cervical node metastases from squamous carcinoma of the oropharynx and hypopharynx. Head Neck 12(3):197–203
Shah JP, Candela FC, Poddar AK (1990) The patterns of cervical lymph node metastases from squamous carcinoma of the oral cavity. Cancer 66(1):109–113
Gregoire V et al (2003) CT-based delineation of lymph node levels and related CTVs in the node-negative neck: DAHANCA, EORTC, GORTEC, NCIC, RTOG consensus guidelines. Radiother Oncol 69(3):227–236
Huang DT et al (1992) Postoperative radiotherapy in head and neck carcinoma with extracapsular lymph node extension and/or positive resection margins: a comparative study. Int J Radiat Oncol Biol Phys 23(4):737–742
Johnson JT et al (1981) The extracapsular spread of tumors in cervical node metastasis. Arch Otolaryngol 107(12):725–729
Snow GB et al (1982) Prognostic factors of neck node metastasis. Clin Otolaryngol Allied Sci 7(3):185–192
Snyderman NL et al (1985) Extracapsular spread of carcinoma in cervical lymph nodes. Impact upon survival in patients with carcinoma of the supraglottic larynx. Cancer 56(7):1597–1599
Carter RL et al (1987) Radical neck dissections for squamous carcinomas: pathological findings and their clinical implications with particular reference to transcapsular spread. Int J Radiat Oncol Biol Phys 13(6):825–832
Hirabayashi H et al (1991) Extracapsular spread of squamous cell carcinoma in neck lymph nodes: prognostic factor of laryngeal cancer. Laryngoscope 101(5):502–506
Apisarnthanarax S et al (2006) Determining optimal clinical target volume margins in head-and-neck cancer based on microscopic extracapsular extension of metastatic neck nodes. Int J Radiat Oncol Biol Phys 64(3):678–683
Gregoire V et al (2014) Delineation of the neck node levels for head and neck tumors: a 2013 update. DAHANCA, EORTC, HKNPCSG, NCIC CTG, NCRI, RTOG, TROG consensus guidelines. Radiother Oncol 110(1):172–181
Lee N et al (2002) Intensity-modulated radiotherapy in the treatment of nasopharyngeal carcinoma: an update of the UCSF experience. Int J Radiat Oncol Biol Phys 53(1):12–22
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Ozyigit, G., Sari, S.Y., Gultekin, M., Yazici, G., Hurmuz, P., Cengiz, M. (2015). Management of the Neck. In: Beyzadeoglu, M., Ozyigit, G., Selek, U. (eds) Radiation Therapy for Head and Neck Cancers. Springer, Cham. https://doi.org/10.1007/978-3-319-10413-3_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-10413-3_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-10412-6
Online ISBN: 978-3-319-10413-3
eBook Packages: MedicineMedicine (R0)