
Abstract
Most drugs are prescribed as oral preparations or extravascular injections (other than intravenous injections) for the treatment of systemic diseases. These drugs must therefore be absorbed in order to be transported to the target tissues to produce their pharmacological actions. Consequently, absorption plays a key role in determining whether or not a drug produces a clinical effect and how fast it occurs. The rate and extent to which a drug is absorbed systemically are related to its time-to-peak concentration (Tmax) and fractional bioavailability (F). Often the two pharmacokinetic terms, absorption and bioavailability, are considered synonymously, but there is actually a subtle difference between them. It is possible for drugs to be well absorbed orally because of good lipid solubility and yet not have a good oral bioavailability because of extensive presystemic loss. While the intravenous bioavailability of drugs is always 100 %, the oral bioavailability is usually less than 100 % because of incomplete absorption and/or first-pass elimination. Many factors influence the oral bioavailability of a drug: some are related to the drug while others to the patient. To overcome poor bioavailability, we can increase the dose administered, change the pharmaceutical formulation, or use a different route of administration.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Drug absorption
- Fractional bioavailability
- Time-to-peak concentration
- Ion trapping
- Presystemic metabolism
- First-pass effect
Introduction
Most drugs are prescribed as oral preparations or extravascular injections for the treatment of systemic diseases. These drugs must therefore be absorbed and delivered to the systemic circulation in order to be transported to the target tissues to produce their pharmacological actions. Consequently, absorption plays a key role in determining whether or not a drug produces a clinical effect and how fast it occurs. The rate and extent to which a drug is absorbed systemically are related to its time-to-peak concentration (Tmax) and fractional bioavailability (F).
Absorption or Bioavailability
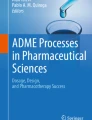
Absorption refers to the transfer of a substance from its site of administration into the bloodstream. This means of course that intravenous route circumvents the absorption process whereas for all other routes, absorption is required for a drug to enter the body and produce its pharmacological effects. Bioavailability however is defined both as the fraction (F) of an administered dose of a substance that enters the systemic circulation in the unchanged form and the rate (Tmax) at which it appears in the systemic circulation. Often these two pharmacokinetic terms (absorption and bioavailability) are considered synonymously, but there is actually a subtle difference between them. It is possible for drugs, such as morphine and nitroglycerin, to be well absorbed orally, as they are lipid soluble and can thus permeate intestinal mucosa readily and yet not have a good oral bioavailability because of extensive presystemic loss. This is because after crossing the intestinal wall, the absorbed drug enters the portal circulation and is carried to the liver before it appears in the systemic circulation (Fig. 3.1). This may result in a loss of drug through metabolism (especially by the cytochrome P450 enzymes) on its first passage through the liver before entering the systemic circulation. Hence, presystemic metabolism is also known as “first-pass effect”.

A schematic diagram showing the enteral routes of drug administration (oral, sublingual and rectal) and their relative susceptibility to first-pass elimination, influencing the absorption and bioavailability of a drug. Following oral administration, Drug A is 100 % absorbed but 40 % bioavailable, while Drug B is 80 % absorbed and 60 % bioavailable. Hepatic first-pass elimination (1 – Fractional bioavailability) of Drug A is 60 % while that of Drug B is 40 %. Following sublingual administration, Drug A is 100 % bioavailable while following rectal administration, Drug A bioavailability is between 40 and 100 %, depending how far up the rectum the drug product is inserted
Measurement of Bioavailability
For intravenous injection, the whole of drug dose is delivered directly into the systemic circulation, thus it will always have 100 % bioavailability (F = 1) and the maximal plasma concentration (Cmax) is reached instantaneously (Tmax = 0 min). For other parenteral routes such as subcutaneous and intramuscular injections, the bioavailability may still be close to 100 % for most therapeutic drugs (F = 0.75−1), since little or no significant metabolism of the drug occurs in the skin or muscle and these small molecules (MW <800) would have no problem permeating the capillary endothelium, but the time to reach its maximum plasma concentration may be relatively slower (Tmax > 0 min) compared to the intravenous route. As for orally administered drugs, their bioavailabilities are often below 100 % (F < 1) because of incomplete absorption and/or first-pass elimination. Their Cmax and Tmax may also differ for the different dosage forms (Fig. 3.2).

Plasma concentration-time curves for a drug given by intravenous (IV) injection and two oral dosage forms (tablet and capsule). Cmax = Peak concentration; Tmax = Time-to-peak concentration; the oral bioavailability is determined by F = AUCoral/AUCiv, where AUC = area under the plasma concentration-time curve for the respective routes

Clinical Relevance of Bioavailability
A low systemic bioavailability will obviously result in the amount of drugs reaching the target tissue being reduced yielding a smaller than expected drug response. If the bioavailability is so poor, it is possible that the administered drug dose may not even reach the minimal effective concentration to produce the desired clinical effect. To overcome this, we can increase the dose administered, change the pharmaceutical formulation, or use a different route of administration.
Drug Permeation
During the process of absorption a drug must cross biological barriers in order to get from the site of administration into bloodstream. There are four major mechanisms by which drug molecules permeate cell membranes: diffusion through lipid, diffusion through aqueous channels, carrier-mediated transports (both active transport and facilitated diffusion) and pinocytosis. Of these mechanisms, diffusion through lipid and carrier-mediated transport are the ones most commonly encountered in drug absorption. The aqueous channels (about 0.4 nm in diameter) are too small to allow most drug molecules (usually >1 nm diameter) to pass through. Pinocytosis appears to be important for the transport of some big molecules (e.g., insulin across the blood brain barrier), but not for small molecules like most drugs.
Diffusion Through Lipid
Non-polar drug molecules passively diffuse across the membrane lipid according to its permeability coefficient, P, and the concentration difference across the membrane. Two physicochemical factors contribute to P, namely the solubility of the drug in the membrane lipid and its diffusivity. Lipid diffusion is by far the most important mechanism by which drugs cross intestinal mucosa to enter portal circulation.
Carrier-Mediated Transport
A number of lipid-insoluble drugs (e.g., levodopa, fluorouracil, iron and calcium) resemble endogenous substances and are carried across cell membranes by forming complexes with specific transmembrane proteins called carriers or transporters. This carrier-mediated transport may operate purely passively (as in facilitated diffusion) or it may be coupled to the electrochemical gradient of Na+ (as in active transport). Carriers are proteins and like receptors, they exhibit selectivity and saturability, and are also subject to competitive inhibition. In addition, active transport may be blocked by inhibitors of cellular metabolism.
Factors Affecting Drug Absorption and Bioavailability
Oral Route
In most instances, absorption occurs when drug molecules are in the form of solutes. If a drug is given in solid form, then the drug must first break down into smaller particles (disintegration) and dissolve in the medium in which it is administered (dissolution) before it can traverse the cell membrane (permeation) and enter the bloodstream (absorption), Fig. 3.3. Thus the rate at which a given medication is absorbed will depend on the relative speed at which these processes occur, and the overall rate of absorption is often determined by the step with the slowest rate. Except for controlled-release medication, disintegration of a solid drug product usually occurs more rapidly than drug dissolution and permeation. Thus, in general, drug absorption may be dissolution rate-limited or permeation rate-limited.

Rate processes involved in drug bioavailability
Dosage Form and Formulation
Dosage form is essentially the pharmaceutical product in the form packaged for use (see Chap. 9). When the same drug is given in different dosage forms, its relative absorption rate will be in this descending order: solution/syrup > suspension > powder > capsule > tablet > coated tablet. This is because drugs in solution form would have avoided the steps of disintegration and dissolution. In contrast, coated tablets (e.g., enteric-coated erythromycin base) or special formulations (e.g., erythromycin stearate ester) are often designed to delay the disintegration and dissolution processes until the drug reaches the small intestine where the condition may be more favorable for its absorption.
The excipient used in different formulation can affect the bioavailability of a drug by influencing the rate of disintegration or dissolution and hence the liberation of the drug from the pharmaceutical preparation (e.g., phenytoin given with lactose as the excipient is better bioavailable compared to when given with calcium sulfate, resulting in unexpected toxicity when the former is replaced with the latter formulation).
Solubility of the Drug
Lipid solubility of a drug is often measured in terms of its octanol-to-water partition coefficient while the degree of ionization is related to its pKa, acid dissociation constant, and the pH of the surrounding medium. For very polar and hydrophilic drugs (e.g., gentamicin and d-tubocurarine), dissolution in the aqueous intestinal medium is not a problem, but permeability through the lipid-rich cell membranes is and this becomes the rate-limiting step to the whole absorption process. The lipid solubility of these drugs is so poor that they are not effective when given orally.
However for a drug with very poor aqueous solubility such as ketoconazole, dissolution is the rate-limiting step in its absorption. Since ketoconazole is weakly basic, it dissolves better in the acidic environment of the gastric juice and absorption occurs more readily there than in the relatively more alkaline intestinal environment. Impairment of ketoconazole absorption secondary to achlorhydria (e.g., resulting from treatment with proton pump inhibitors or H2 antagonists) has been documented for both healthy patients and patients with AIDS, while acidic beverages such as Coca-Cola enhances its absorption. Griseofulvin is another drug with very poor aqueous solubility and moderate lipid solubility and its absorption is increased with fatty meal.
Degree of Ionization
As most drugs are weak acids or bases, their degrees of ionization vary according to the pH at different levels of the gastrointestinal tract. Weak acids such as aspirin are less ionized at the low pH (1–3) of the stomach content and can easily diffuse cross the gastric mucosal membrane to reach the bloodstream on the serosal side. As the pH of the plasma is relatively more basic (pH = 7.4), this results in a relatively greater degree of ionization of the weak acid drug, which discourages back diffusion of the drug into the gastrointestinal lumen (Fig. 3.4). This unequal distribution of drug molecules based on the pH gradient across the gastric membrane is an example of “ion trapping”. The reverse can occur with weak bases. The ion trapping of basic compounds within the gastric lumen is sometimes useful in forensic medicine. Drugs of abuse such as heroin, cocaine and amphetamine, are organic bases. Even when injected intravenously, they tend to accumulate in the stomach by crossing the gastric mucosa in the reverse direction. This drug behavior may find application in forensic medicine.

The influence of pKa on the degree of functional group ionization in basic and acidic drugs relative to the physiologic pH. The increasing depth of color in the arrows reflects increasing ionization relative to the physiologic pH of 7.4. Thus, for basic drugs, the more acidic the solution (i.e., the lower the pH), the greater is the proportion of drug ionized. The converse is true of the acidic drugs. [The pKa of a drug is the pH at which 50 % of the drug molecules in solution are ionized]
Mucosal Surface Area
Despite what is said about the effect of pH on the degree of ionization of a weak acid drug and hence its greater lipid solubility in the gastric lumen, the small intestine is still the optimal site of absorption due to the greatly increased mucosal surface area for absorption. The surface-to-volume ratio in the small intestine is so great that drugs ionized even to the extent of 99 % may still be effectively absorbed.
First-Pass Effect
This is also known as presystemic elimination, which may be caused by gut secretion (e.g., insulin is destroyed by digestive enzymes), or enzymes produced by gut microflora (e.g., digoxin is degraded by bacterial enzymes in the stomach), gut mucosa (e.g., epinephrine and levodopa are degraded by intestinal monoamine oxidase) and liver (e.g., lidocaine, morphine and nitroglycerin). Strictly speaking, hepatic first-pass metabolism does not affect oral absorption but it can affect oral bioavailability. Some drugs (e.g., tetracycline) form complexes with cations such as Ca2+, Mg2+ and Fe2+ in the food or diet supplements and this may also result in presystemic loss. Oral absorption of alendronate is very poor (about 0.6 %) to start with and food decreases it even further. It is thus crucial that this drug should be taken on an empty stomach with just water.
Gut Motility
As the small intestine is the optimal absorption site for most drugs, a decrease in gastric emptying rate (e.g., migraine attack, fatty meals, antimuscarinic medication) generally delays their oral absorption although it may not significantly affect the extent of absorption unless the drug is not stable in the stomach. On the other hand, increased intestinal motility with prokinetic drugs such as metoclopramide would enhance the intestinal absorption of most drugs. Excessively enhanced gut motility (e.g., during diarrhea) however may reduce oral absorption of drugs with poor lipid solubility due to insufficient time for drugs to cross the intestinal mucosa.
Splanchnic Blood Flow
Physiological changes in blood flow have little impact on the rate of extent of gastrointestinal absorption of most drugs. However, splanchnic blood flow may be greatly reduced in shock to such an extent that it may slow the absorption of some drugs.
Non-oral Routes
For other routes of drug administration, the absorption depends mainly on regional blood flow, area of absorption surface, drug properties and formulation in much the same way as are described for oral absorption.
Key Concepts
-
Absorption is the process of transferring a substance from its site of administration into the bloodstream.
-
Bioavailability is defined both as the fraction (F) of an administered dose of a substance that enters the systemic circulation in the unchanged form and the rate (Tmax) at which it appears in the systemic circulation.
-
A low systemic bioavailability can be overcome by increasing the dose administered, changing the pharmaceutical formulation, or using a different route of administration.
-
Most drugs are well absorbed from the gut, and lipid diffusion is the most important mechanism for oral absorption.
-
Absorption from the gut depends on many factors, some of which are related to the drugs (e.g., lipid solubility, degree of ionization) and others to the patients (e.g., gut motility, intestinal pH, splanchnic blood flow).
Summary
Drugs that are prescribed as oral preparations or extravascular injections must enter systemic circulation in order to be able to produce a systemic effect. Consequently, absorption plays a key role in determining whether or not a drug produces a clinical effect and how fast it occurs. The rate and extent to which a drug is absorbed systemically are related to its time-to-peak concentration (Tmax) and fractional bioavailability (F). A drug may be well absorbed orally because of good lipid solubility and yet not has a good oral bioavailability because of extensive presystemic loss. While the intravenous bioavailability of drugs is always 100 %, the oral bioavailability is usually less than 100 % because of incomplete absorption and/or first-pass elimination. Many factors influence the oral bioavailability of a drug; some are related to the drug while others to the patient. To overcome poor bioavailability, we can increase the dose administered, change the pharmaceutical formulation, or use a different route of administration.
Further Reading
Boucher BA, Wood GC, Swanson JM. Pharmacokinetic changes in critical illness. Crit Care Clin. 2006;22:255–71.
Chin TWF, Loeb M, Fong IW. Effects of an acidic beverage (Coca-Cola) on absorption of ketoconazole. Antimicrob Agents Chemother. 1995;39(5):1671–5.
Hughes SG. Prescribing for the elderly patient: why do we need to exercise caution? Br J Clin Pharmacol. 1998;46:531–3.
Rang HP, Dale MM, Ritter JM, Flower RJ, Henderson G. Rang and Dale’s pharmacology. 7th ed. Edinburgh: Churchill Livingstone; 2012.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Sim, D.S.M. (2015). Drug Absorption and Bioavailability. In: Chan, Y., Ng, K., Sim, D. (eds) Pharmacological Basis of Acute Care. Springer, Cham. https://doi.org/10.1007/978-3-319-10386-0_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-10386-0_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-10385-3
Online ISBN: 978-3-319-10386-0
eBook Packages: MedicineMedicine (R0)