
Abstract
Ultrasound images are coupled with anatomical schemes explaining the probe positioning and scanning technique for the extensor muscles. For each muscle, a brief explanation of normal anatomy is also provided, together with a list of tricks and tips and advice on how to perform the ultrasound scan in clinical practice.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
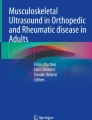
The tibialis anterior, extensor hallucis longus and extensor digitorum longus muscles occupy the anterior compartment of the leg (Fig. 17.1). They are separated from the deep posterior muscles by the tibia, the fibula and the interosseous membrane.

Anatomical scheme of the anterior leg compartment muscles. TA tibialis anterior, EDL extensor digitorum longus, EHL extensor hallucis longus. EHL lies in a deeper layer than TA and EDL and its muscle belly arises more distally
1 Anatomy Key Points
1.1 Tibialis Anterior
1.2 Extensor Hallucis Longus
1.3 Extensor Digitorum Longus
2 Ultrasound Examination Technique
The patient is seated on the examination bed with the knee flexed about 20–45°, and the plantar surface of the foot lies flat on the table (Fig. 17.2).

Leg position to evaluate the anterior leg compartment
Palpate the tibial tuberosity on the anterior aspect of the tibia, which can be considered an important bony landmark, and place the probe on it in an axial position.
Move the transducer slightly lateral and identify the myotendinous junction of the tibialis anterior near the patellar tendon (Fig. 17.3).

(a) Probe position to evaluate the myotendinous junction of the tibialis anterior muscle on axial plane; (b) US axial scan: the myotendinous junction (MJT) lies lateral to the patellar tendon (PT). TT tibial tuberosity
Rotate the probe by 90° to evaluate on a longitudinal plane the proximal attachment of the tibialis anterior tendon on the tibial tuberosity (Fig. 17.4).

(a) Probe position to evaluate the myotendinous junction of the tibialis anterior muscle on longitudinal plane; (b) US longitudinal scan shows the myotendinous junction and the proximal insertion of the tibialis anterior (TA) on the tibial tuberosity (TT)
Replace the probe in a transverse plane and shift it caudally and lateral to identify the cortical surface of the fibula and the anterior tibial crest in the same scan (Fig. 17.5).

(a) Probe position to evaluate the anterior leg compartment at the proximal third of the leg on axial plane. (b) US axial scan at the proximal third of the leg illustrates the relationship between the tibialis anterior (TA), the extensor digitorum longus (EDL) and the peronei muscles (P). The interosseous membrane appears as a hyperechoic line, which extends between the tibia (T) and the fibula (F). TP tibialis posterior muscle
The cortex of the tibia and fibula are identified as continuous hyperechoic lines with posterior shadowing.
The interosseous membrane can be seen as a thin concave hyperechoic layer between the tibial and fibular cortex and opposite to the tibialis posterior muscle.
Power Doppler could be useful in order to identify the anterior neurovascular bundle and the passage of the anterior tibial vessel through the interosseous membrane (Fig. 17.6).

US axial scan at the proximal third of the leg. Power Doppler is useful to identify the anterior tibial artery at the level of the interosseous membrane. TA tibialis anterior muscle, T tibia, F fibula
At this level, it is possible to demonstrate the large muscular belly of the tibialis anterior characterized by a thick central aponeurosis (Fig. 17.7).

US axial scan at the proximal third of the leg. Note the large muscular belly of the tibialis anterior muscle (TA) and the thick central aponeurosis (arrowheads). T tibia, F fibula
This muscle is covered by a thin echogenic fascia (crural fascia) that continues with the anterior fascia of the leg.
A focused evaluation of the integrity of this structure is mandatory if muscle hernia is suspected. A squatting position can be useful to demonstrate the herniation of the muscle and the focal defect of the fascia.
Longitudinal US scan with the probe oriented perpendicular to the skin, in the sagittal plane, is useful to visualize the muscle belly on its long axis. The central aponeurosis appears as a hyperechoic structure that continues from the extra muscular tendon and extends into the muscle dividing in two unipennate halves, above and below the aponeurosis (Fig. 17.8).

EFV US longitudinal scan of the tibialis anterior muscle (TA) from the tibial tuberosity (TT). Note the thick central aponeurosis (arrowheads) that appears as a hyperechoic structure into the muscular belly
At this level, we can measure the muscular thickness and pennation angle (see Chap. 4).
Ask the patient to contract the muscle with dorsiflexion of the foot to evaluate the increasing of the pennation angle.
Always remember to move the transducer caudally following the tibialis anterior muscle belly until the myotendinous junction (Figs. 17.9 and 17.10).

(a) Probe position to evaluate the myotendinous junction of tibialis anterior muscle (TA) on an axial scan. (b) US axial scan of the myotendinous junction of TA. T tibia

(a) Probe position to evaluate the myotendinous junction of the tibialis anterior muscle (TA) on a longitudinal scan. (b) US longitudinal scan of the myotendinous junction of TA
Then place the transducer on the proximal middle third of the tibial shaft and shift the probe laterally to examine the extensor digitorum longus muscle belly on an axial scan. In this scan, the extensor digitorum longus muscle is located laterally to the tibialis anterior muscle (Fig. 17.5).
Then move the transducer caudally, always in a transversal plane, until the middle of the leg to visualize the extensor hallucis longus muscle which arises at this level (Fig. 17.11).

(a) Probe position to evaluate the anterior leg compartment at the distal third of the leg on axial plane. (b) US axial scan at the distal third of the leg. At this level, the myotendinous junction of the tibialis anterior (TA) may be evaluated. The extensor hallucis longus muscle (EHL) lies between the myotendinous junction of the tibialis anterior (TA) and the extensor digitorum longus muscle (EDL) belly. T tibia, F fibula, * interosseous membrane
If the extensor hallucis longus and the extensor digitorum longus muscles are not well separated, an active or passive muscular contraction can be helpful to distinguish them.
Always remember to move the transducer caudally following the extensor digitorum longus and the extensor hallucis longus muscle bellies until the myotendinous junction (Figs. 17.12 and 17.13).

(a) US axial scan of the myotendinous junction of the extensor digitorum longus (EDL) muscle (b) US longitudinal scan of the myotendinous junction of the extensor digitorum longus (EDL) muscle. EHL extensor hallucis longus muscle

(a) US axial scan of the myotendinous junction of the extensor hallucis longus (EHL) muscle (b) US longitudinal scan of the myotendinous junction of the extensor hallucis longus (EHL) muscle. T tibia, Ta talus
Rotate the probe by 90° to assess the internal structure of each muscle belly (Fig. 17.14).

Anatomical scheme correlated to EFV US axial scans at different levels of the anterior compartment of leg muscles. (a) Proximal anterior compartment. EFV axial scan visualizes the relationship between the peroneus muscles (P) and the extensor muscles. The tibialis anterior muscle (TA) lies just lateral to the tibial crest and medial to the extensor digitorum longus muscle (EDL). The interosseous membrane appears as a hyperechoic layer which separates TA from the tibialis posterior muscle (TP). (b) Middle third of leg anterior compartment. EFV axial scan shows TA myotendinous junction with its oval tendon anterior to the tibial edge. Note the EDL and extensor hallucis longus (EHL) muscle bellies. (c) Distal anterior compartment of the leg. EFV US axial scan evaluates the relationship between the peroneus muscle (P) and the extensor muscle at the distal third of the leg. The peroneus brevis and peroneus longus are not well separated. T tibia, F fibula
Place the transducer over the dorsum of the ankle to examine the extensor tendon group in the axial plane. In this scan, it is possible to visualize, from medial to lateral, the tibialis anterior, the extensor hallucis longus and the extensor digitorum longus tendons. Always examine these structures from the myotendinous junction to their distal insertion (Fig. 17.15).

(a) Anatomical scheme of the extensor tendon group and extensor retinacula. SER superior extensor retinaculum, IER inferior extensor retinaculum. (b) Probe position to evaluate the extensor tendon group in the axial plane. (c) US axial scan of the extensor tendon group. TA tibialis anterior tendon, EDL extensor digitorum longus tendon, EHL extensor hallucis longus tendon, arrow deep peroneal nerve
At this level, also examine the deep peroneal nerve, which runs on the medial side of the anterior tibial artery (Fig. 17.16).

US axial scan of the deep peroneal nerve (arrowheads) at the level of the ankle joint. * anterior tibial artery
Focus On
The deep peroneal nerve (deep fibular nerve) originates from the common fibular nerve near the neck of the fibula, between the fibula and upper part of the peroneus longus.
The deep fibular nerve travels in the anterior compartment of the leg on the anterior surface of the interosseous membrane.
It passes inferomedially, deep to extensor digitorum longus and, at the middle of the leg, comes in relation with the anterior tibial artery.
It runs initially lateral to the anterior tibial artery, but in proximity of the ankle joint it crosses over to run on the medial side.
At this level, the extensor hallucis longus muscle and tendon and the inferior extensor retinaculum overly ventrally the nerve that passes through the anterior tarsal tunnel (the space located between the inferior extensor retinaculum and the fascia overlying the talus and the navicular bones).
Just under the inferior extensor retinaculum, the deep peroneal nerve divides into lateral and medial terminal branches.
The lateral terminal branch (external branch) passes across the tarsus anterolaterally and supplies the extensor digitorum brevis and the extensor hallucis brevis muscles. From the enlargement, it gives three small interosseous branches (dorsal interosseous nerves) for the innervation of the tarsal joints and the metatarsophalangeal joints of the second, third and fourth toes.
The medial terminal branch (internal branch) travels medial to the dorsalis pedis artery along the dorsum of the foot. At the first interosseous space, it divides into dorsal digital nerves, which provide sensory innervation to the first webspace and the adjacent dorsum of the foot between the first and second toes.
The deep fibular nerve provides motor innervation to the muscles of the anterior compartment of the leg, the tibialis anterior, extensor digitorum longus, extensor hallucis longus and peroneus tertius muscles.
It also provides sensory innervation to the webspace between the hallux and second digit.
Injury to the deep fibular nerve typically produces loss of dorsiflexion of the foot (foot drop), loss of extension of the toes and loss of sensation in the first webspace.
Complete the examination with dynamics scans in order to evaluate muscles and tendons also during contraction.
Evaluate also the integrity of the superior and inferior extensor retinacula and the relationship between tendons and tibial bony surface at this level (Figs. 17.17 and 17.18).

(a) Anatomical scheme of the extensor tendon group and extensor retinacula. SER superior extensor retinaculum, IER inferior extensor retinaculum. (b) Probe position to evaluate the superior extensor retinaculum at the level of the extensor hallucis longus tendon. (c) US axial scan of the superior extensor retinaculum (arrowheads) at the level of the extensor hallucis longus (EHL) tendon

(a) Anatomical scheme of the extensor tendon group and extensor retinacula. SER superior extensor retinaculum, IER inferior extensor retinaculum. (b) Probe position to evaluate the inferior extensor retinaculum at the level of the extensor digitorum longus tendon. (c) US axial scan of the superior inferior extensor retinaculum (arrowheads) at the level of the extensor digitorum longus tendon (EDL)
3 17.3 Summary Table
Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
Tibialis anterior | Lateral surface of the tibia and neighbouring interosseous membrane in the upper leg | Dorsal aspect of the first metatarsal and medial surface of the medial cuneiform | Deep fibular nerve | Dorsiflexion and inversion of the foot |
Extensor hallucis longus | Distal aspect of the fibula and interosseous membrane | Distal phalanx of the first toe | Deep fibular nerve | Extension of the big toe and assists in dorsiflexion of the foot at the ankle |
Extensor digitorum longus | Inferior aspect of lateral tibial condyle, anterior surface of the interosseous membrane and medial face of fibula | Distal phalanges of the second through fifth toes | Deep fibular nerve | Extension of toes and dorsiflexion of ankle |
Suggested Reading
Bianchi S, Martinoli C (2009) US of the musculoskeletal system. Springer, Berlin
Drake RL, Vogl W, Mitchell AWM (2005) Grey’s anatomy. Elsevier/Churchill Livingstone, Philadelphia
Gokhale S (2007) Three-dimensional sonography of muscle hernias. J Ultrasound Med 26:239–242
Jerome JTJ, Varghese M, Thirumagal K (2008) Tibialis Anterior Rupture: a missed diagnosis. Foot Ankle Online J 3(9):2
Lieber RL, Fridén J (2000) Functional and clinical significance of skeletal muscle architecture. Muscle Nerve 23(11):1647–1666
Maganaris CN, Baltzopoulos V, Sargeant AJ (1998) Changes in the tibialis anterior tendon moment arm from rest to maximum isometric dorsiflexion: in vivo observations in man. Clin Biomech 14:661–666
Maganaris CN, Kawakami Y, Fukunaga T (2001) Changes in aponeurotic dimensions upon muscle shortening: in vivo observations in man. J Anat 199:449–456
Nakhostine M, Styf JR, van Leuven S, Hargens AR, Gershuni DH (1993) Intramuscular pressure varies with depth. The tibialis anterior muscle studied in 12 volunteers. Acta Orthop Scad 64(3):377–381
Peer S, Kovacs P, Harpf C, Bodner G (2002) High-resolution sonography of lower extremity peripheral nerves anatomic correlation and spectrum of disease. J Ultrasound Med 21:315–322
Pillen S (2010) Skeletal muscle ultrasound. Eur J Transl Myol 1(4):145–155
Reneman RS (1975) The anterior and the lateral compartmental syndrome of the leg due to intensive use of muscles. Clin Orthop Relat Res 113:69–80
Silvestri E, Muda A, Sconfienza LM (2012) Normal ultrasound anatomy of the musculoskeletal system. Springer, Milan/New York
Stoller DW (2007) Stoller’s atlas of orthopaedics and sports medicine. Lippincott Williams & Wilkins, Philadelphia
Styf JR, Korner LM (1987) Diagnosis of chronic anterior compartment syndrome in the lower leg. Acta Orthop Scand 58(2):139–144
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Orlandi, D., Arcidiacono, A. (2015). Extensor Muscles. In: Ultrasound Anatomy of Lower Limb Muscles. Springer, Cham. https://doi.org/10.1007/978-3-319-09480-9_17
Download citation
DOI: https://doi.org/10.1007/978-3-319-09480-9_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-09479-3
Online ISBN: 978-3-319-09480-9
eBook Packages: MedicineMedicine (R0)