
Abstract
The aim of this article is to review some common opinions on changes in pubertal timing and shed new light both on the indicators used in assessing pubertal timing and the underlying mechanisms. While emphasis is usually placed on the advancement in timing of female puberty, it appears that timing also changes in males, both towards earliness for the initial pubertal stages and towards lateness for the final stages. Such findings suggest that the environmental influences on pubertal timing are more complex than initially thought. Moreover, self-evaluated pubertal timing versus peers provides information that is not always consistent with observations at physical examination, suggesting that both approaches should be considered, especially when studying the correlation between pubertal timing and psychosocial aspects.
The mechanisms of changes in pubertal timing may involve both central neuroendocrine control and peripheral effects in tissues targeted by gonadal steroids. Though energy availability is certainly a clue to the mechanism of pubertal development, changes in the control of both energy balance and reproduction may vary under the influence of common determinants such as endocrine-disrupting chemicals. These effects can take place right before puberty as well as much earlier, during fetal and neonatal life. Finally, environmental factors can interact with genetic factors in determining changes in pubertal timing. Therefore, the variance in pubertal timing is no longer to be considered under the absolutely separate control of environmental and genetic determinants.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
We review here how studies of the physiological variations in pubertal timing have changed recently with emphasis on the indicators and the mechanisms. The findings suggest that the respective roles of genetic and environmental factors in the control of pubertal timing are complex because they can take place during late prepubertal life as well as fetal/neonatal life. Moreover, both types of factors likely involve intricate mechanisms.
Changes in Indicators of Pubertal Timing
Since the mid-nineteenth century, a so-called secular trend towards earlier menarcheal age has been observed in many countries in Europe and North America. An overall advancement in female pubertal timing that averaged 4 years in a century was derived from those observations (Parent et al. 2003). During the past 50 years, menarcheal age has stabilized in some countries, such as Belgium (Jeurissen 1969; Vercauteren and Susanne 1985; Roelants et al. 2009), where it seemed that the secular advancement in pubertal timing was leveling off as opposed to countries where socio-economical status was still markedly progressing (Parent et al. 2003). It is notable, however, that recent publications have highlighted a persistent but moderate decrease in average menarcheal age in countries like Denmark and the Netherlands (Aksglaede et al. 2009; Talma et al. 2013). Around 2000, a new pattern of changes was observed in several countries such as USA, Denmark and Belgium (Roelants et al. 2009; Aksglaede et al. 2009; Herman-Giddens et al. 1997), with a heterogeneity among pubertal events, i.e., advancement in age at onset of breast development and less or no change in menarcheal age. This finding has led us to revise some issues about indicators and mechanisms of changes in pubertal timing.
Studies of female puberty have been prioritized (Table 1) due to the availability of menarcheal age as a precise timer, and focus on the female has been reinforced by the critical role of weight and the predominance of sexual precocity in girls (Parent et al. 2003). Based on findings about testicular volume increase, voice break and growth spurt, it has appeared recently, however, that male pubertal timing is advancing as well (Roelants et al. 2009; Aksglaede et al. 2008; Sorensen et al. 2010; Juul et al. 2007; Herman-Giddens et al. 2012). As already pointed out in the female, the initial pubertal signs and signs of completion of puberty could show secular changes that are different, suggesting heterogeneity in the response of pubertal events to modulating factors. For example, the first 3–10 % of boys with evidence of initial pubertal increase in testicular volume (≥4 ml) are younger than in the past (Roelants et al. 2009; Herman-Giddens et al. 2012; Mul et al. 2001) whereas the final 3–10 % (centile 90 and 97) appear to attain adult testicular volume (≥15 ml) later (Roelants et al. 2009; Mul et al. 2001). Thus, besides the changes in mean or median ages at a given pubertal sign, subtle changes in the pattern of distribution of timing of pubertal signs may occur, extending the age range beyond the physiological 4–5-year period for both the initial and the late stages of puberty. The latter finding is also consistent with the secular increase in latency between menarche and the occurrence of regular (ovulatory) cycling that was reported in France together with the classical secular trend towards earlier menarche (Clavel-Chapelon et al. 2002).
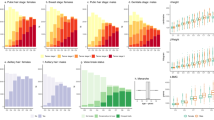
In the evaluation of pubertal development, two distinctive issues can be considered: pubertal status, which refers to the degree of physical changes, and pubertal timing, which refers to the age at attainment of a given degree of physical change. The adolescents are understandably reluctant to allow assessment of pubertal status if not justified by the chief complaint at consultation. Therefore, methods of self-assessment of pubertal status (Table 2) were designed, in comparison with Tanner stages, provided either as pictures or drawings (Duke et al. 1980; Morris and Udry (1980), or as written statements (Petersen et al. 1988). Controversial data have been published regarding the validity of these methods that cannot substitute for a physician’s examination (Hergenroeder et al. 1999; Brooks-Gunn et al. 1987; Bond et al. 2006; Dick et al. 2001; Dorn and Biro 2011). Moreover, the significance of self-assessed pubertal status in determining pubertal timing has been limited to the interpretation of current status with respect to age. In some instances, retrospective assessment of pubertal timing could be interesting. Berg-Kelly and Erdes (1997) proposed an age-independent method of self-assessment of pubertal timing through a global multiple choice question rating maturation versus peers. The answer to this question was found to result in 94 % agreement with physician examination and normal distribution of timing in the studied population (Berg-Kelly and Erdes 1997). We have used a similar question: “Between 8 and 18 years, boys and girls change physically but not all at the same time. If you consider your physical development, how do you evaluate it in comparison with friends of the same age: Very early? A bit early? Same as most friends? A bit late? Very late?” Such a question enables self-evaluation of pubertal timing based on current status, as done in the Swedish study (Berg-Kelly and Erdes 1997), or retrospectively, as done in our study. As shown in Fig. 1, the distribution of responses in two separate studies was found to be asymmetrical, with more adolescents estimating they had matured early than late. Interestingly enough, in a study comparing adolescent self-perception of pubertal timing using both a global question (peer normative) and the pubertal developmental scale (PDS; stage normative), a similar proportion of late timing (12–13 %) was found using both tools whereas the global question resulted in a greater proportion of early timing (28 %) as opposed to the PDS (13 %; Cance et al. 2012). This finding suggests that the comparison with peers involves a factor that accounts for increased self-perception of early timing of maturation. Desirability could play some role: evaluating oneself as early versus peers could be felt as a plus whereas being late would be a minus. Some discrepancies in self-evaluation of pubertal timing could be related to the conditions of evaluation. Agreement with physician evaluation was greater when the sexual maturation scale was administered in a clinical setting rather than at school (Schlossberger et al. 1992). These authors also found a greater proportion of early-maturing subjects based on adolescent global self-rating than based on physician evaluation.

Upper panel: self evaluation of pubertal timing versus peers of the same age in two separate groups of 265 adolescents irrespective of gender and 249 adolescents (108 girls and 141 boys). Lower panel: self evaluation of pubertal timing versus peers of the same age in 52 adolescents with early or precocious pubertal timing, based on physical exam
Our data also raise the question as to whether an increased proportion of self-evaluated earliness is actually consistent with early or precocious puberty. The response is negative since, among a group of adolescents with early or precocious puberty confirmed by physical examination, about 2/3 had a concordant self-evaluated timing whereas 1/3 were felt to be average maturers. Thus, self-perceived pubertal development does not reliably match data from physical exam and provides different information that can have its own significance for adolescent behavior. Such a conclusion has been drawn by Deppen et al. (2012), who reported that adolescent girls with average timing of menarche but early self-perceived pubertal timing were at increased risk of adolescent exploratory behaviors.
Changes in Mechanisms of Pubertal Timing
In searching for possible causes and mechanisms of changes in pubertal timing, the default hypothesis is hypothalamic-pituitary maturation, possibly because central precocity is much more frequent than peripheral precocity (Table 3). It appears, however, that peripheral mechanisms can coexist with central mechanisms or secondarily facilitate them. Such a concept is supported by the dissociation between advancement in age at onset of breast development in Denmark, the Netherlands and Belgium without a parallel change in menarcheal age, suggesting that both events are influenced by different factors, including possible breast development due to estrogenic effects independent of hypothalamic-pituitary maturation (Roelants et al. 2009; Aksglaede et al. 2009; Mul et al. 2001). That dissociation of breast development and menarche could account for the secular reduction in correlation coefficient between the ages at occurrence of the two pubertal events (Biro et al. 2006). The interpretation of the mechanistic role of sex steroids or related environmental factors is complex due to the multiple sites where they can interact between the hypothalamus and the peripheral target tissues. In particular, sex steroids exert potent inhibitory feedback on the pituitary gonadotrophins. As an illustration (Fig. 2), a girl with androgen excess caused by an adrenal adenoma has developed no breasts at 13, possibly due to the androgen/estrogen ratio as well as the negative feedback caused at the pituitary level. However, hypothalamic maturation should have progressed silently since, 6 months after withdrawal from the androgen excess, breast development is nearly adult and menarche occurs. This condition is somehow comparable with the mechanism that we have delineated in a female rodent model (Rasier et al. 2007, 2008) to explain sexual precocity in girls who were previously exposed to the estrogenic insecticide DDT and then withdrawn from that environment after migration to Belgium (Krstevska-Konstantinova et al. 2001).

Growth curve of a female patient presenting at 13 years with no breast development (B1 Tanner’s stage) and adult pubic hair (P6 Tanner’s stage) due to an androgen-secreting adrenal adenoma. Within 6 months after surgical removal of the adenoma, breasts attained B4 stage and menarche occurred. Target height and bone age (X) are indicated
Because nutrition has long been known to be a determinant of puberty, especially in females, a direct causal relationship between obesity and earlier onset of puberty has been hypothesized (Parent et al. 2003). Evidence has indeed accumulated that a sufficient amount of fat mass signaling to the neuroendocrine system through leptin is a prerequisite to the onset of puberty. Leptin can stimulate pulsatile GnRH secretion and is indeed necessary but not sufficient to account for the onset of puberty (Lebrethon et al. 2007). It appears also that both energy balance and pubertal timing share common regulatory factors that could be jointly influenced during prenatal or neonatal organization of the neuroendocrine control of homeostasis (Bourguignon et al. 2010, 2013) Along the same lines, most studies on the role of environmental factors in triggering the onset of puberty were centered on the immediately preceding period. Now, the impact of events during fetal and neonatal periods appears to be equally important. For instance, Ibanez et al. (2011) have provided evidence that, in girls with premature pubarche, menarche is advanced as a function of reduction in birth weight. Studies of the effects of neonatal exposure to endocrine disrupters such as diethylstilbestrol (DES) in the female rat showed opposing effects on GnRH secretion and pubertal timing, depending on the dose (Franssen et al. 2014). Moreover, both prenatal food restriction and neonatal DES exposure resulted in a reduced response of pulsatile GnRH secretion to leptin, with both effects being additive (Franssen et al. 2014). Though the mechanism of variations in pubertal timing caused in fetal or neonatal life is not fully elucidated, it could involve epigenetics that, together with polymorphisms, teach us that the contribution of genetic and environmental factors is intricate in explaining the variance in pubertal timing.
While the pubertal growth spurt is decreasing with age at onset of puberty, the impact of differences in pubertal timing on final height is limited (Bourguignon 1988). Such a finding, however, may be revised based on the dissociated gain in height and progression of bone maturation in two prismatic male cases with estrogen receptor or aromatase deficiency (Smith et al. 1994; Carani et al. 1997). Those observations have highlighted the specific role of estrogens in bone maturation and led some authors to use aromatase inhibitors in short adolescents and demonstrated a significant gain in adult stature (Hero et al. 2006). Such treatment, however, may involve undesirable effects such as vertebral deformities and should be restricted to research protocols that also have to delineate the possible effects of such treatment on brain and behavior.
References
Aksglaede L, Olsen LW, Sorensen TI, Juul A (2008) Forty years trends in timing of pubertal growth spurt in 157,000 Danish school children. PLoS One 3:e2728
Aksglaede L, Sorensen K, Petersen JH, Skakkebaek NE, Juul A (2009) Recent decline in age at breast development: the Copenhagen Puberty Study. Pediatrics 123:e932–e939
Berg-Kelly K, Erdes L (1997) Self-assessment of sexual maturity by mid-adolescents based on a global question. Acta Paediatr 86:10–17
Biro FM, Huang B, Crawford PB, Lucky AW, Striegel-Moore R, Barton BA, Daniels S (2006) Pubertal correlates in black and white girls. J Pediatr 148:234–240
Bond L, Clements J, Bertalli N, Evans-Whipp T, McMorris BJ, Patton GC, Toumbourou JW, Catalano RF (2006) A comparison of self-reported puberty using the Pubertal Development Scale and the Sexual Maturation Scale in a school-based epidemiologic survey. J Adolesc 29:709–720
Bourguignon JP (1988) Linear growth as a function of age at onset of puberty and sex steroid dosage: therapeutic implications. Endocr Rev 9:467–488
Bourguignon JP, Rasier G, Lebrethon MC, Gerard A, Naveau E, Parent AS (2010) Neuroendocrine disruption of pubertal timing and interactions between homeostasis of reproduction and energy balance. Mol Cell Endocrinol 324:110–120
Bourguignon JP, Franssen D, Gerard A, Janssen S, Pinson A, Naveau E, Parent AS (2013) Early neuroendocrine disruption in hypothalamus and hippocampus: developmental effects including female sexual maturation and implications for endocrine disrupting chemical screening. J Neuroendocrinol 25:1079–1087
Brooks-Gunn J, Warren MP, Rosso J, Gargiulo J (1987) Validity of self-report measures of girls’ pubertal status. Child Dev 58:829–841
Cance JD, Ennett ST, Morgan-Lopez AA, Foshee VA (2012) The stability of perceived pubertal timing across adolescence. J Youth Adolesc 41:764–775
Carani C, Qin K, Simoni M, Faustini-Fustini M, Serpente S, Boyd J, Korach KS, Simpson ER (1997) Effect of testosterone and estradiol in a man with aromatase deficiency. N Engl J Med 337:91–95
Clavel-Chapelon F, E3N-Epic group, European Prospective Investigation into Cancer (2002) Evolution of age at menarche and at onset of regular cycling in a large cohort of French women. Hum Reprod 17:228–232
Deppen A, Jeannin A, Michaud PA, Alsaker F, Suris JC (2012) Subjective pubertal timing and health-compromising behaviours among Swiss adolescent girls reporting an on-time objective pubertal timing. Acta Paediatr 101:868–872
Dick DM, Rose RJ, Pulkkinen L, Kaprio J (2001) Measuring and understanding its impact: a longitudinal study of adolescent twins. J Youth Adolesc 30:385–399
Dorn LD, Biro FM (2011) Puberty and its measurement: a decade in review. J Res Adolesc 21:180–195
Duke PM, Litt IF, Gross RT (1980) Adolescents’ self-assessment of sexual maturation. Pediatrics 66:918–920
Franssen D, Ioannou YS, Alvarez-Real A, Gerard A, Mueller JK, Heger S, Bourguignon JP, Parent AS (2014) Pubertal timing after neonatal diethylstilbestrol exposure in female rats: neuroendocrine vs peripheral effects and additive role of prenatal food restriction. Reprod Toxicol 44:63–72
Hergenroeder AC, Hill RB, Wong WW, Sangi-Haghpeykar H, Taylor W (1999) Validity of self-assessment of pubertal maturation in African American and European American adolescents. J Adolesc Health 24:201–205
Herman-Giddens ME, Slora EJ, Wasserman RC, Bourdony CJ, Bhapkar MV, Koch GG, Hasemeier CM (1997) Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network. Pediatrics 99:505–512
Herman-Giddens ME, Steffes J, Harris D, Slora E, Hussey M, Dowshen SA, Wasserman R, Serwint JR, Smitherman L, Reiter EO (2012) Secondary sexual characteristics in boys: data from the Pediatric Research in Office Settings network. Pediatrics 130:e1058–e1068
Hero M, Wickman S, Dunkel L (2006) Treatment with the aromatase inhibitor letrozole during adolescence increases near-final height in boys with constitutional delay of puberty. Clin Endocrinol 64:510–513
Ibanez L, Lopez-Bermejo A, Diaz M, Marcos MV (2011) Endocrinology and gynecology of girls and women with low birth weight. Fetal Diagn Ther 30:243–249
Jeurissen A (1969) Age of the establishment of the menarche and its evolution in Belgium during the last 40 years. Acta Paediatr Belg 23:319–330
Juul A, Magnusdottir S, Scheike T, Prytz S, Skakkebaek NE (2007) Age at voice break in Danish boys: effects of pre-pubertal body mass index and secular trend. Int J Androl 30:537–542
Krstevska-Konstantinova M, Charlier C, Craen M, Du Caju M, Heinrichs C, de Beaufort C, Plomteux G, Bourguignon JP (2001) Sexual precocity after immigration from developing countries to Belgium: evidence of previous exposure to organochlorine pesticides. Hum Reprod 16:1020–1026
Lebrethon MC, Aganina A, Fournier M, Gerard A, Parent AS, Bourguignon JP (2007) Effects of in vivo and in vitro administration of ghrelin, leptin and neuropeptide mediators on pulsatile gonadotrophin-releasing hormone secretion from male rat hypothalamus before and after puberty. J Neuroendocrinol 19:181–188
Morris NM, Udry JR (1980) Validation of a self-administered instrument to assess stage of adolescent development. J Youth Adolesc 9:271–280
Mul D, Fredriks AM, van Buuren S, Oostdijk W, Verloove-Vanhorick SP, Wit JM (2001) Pubertal development in The Netherlands 1965–1997. Pediatr Res 50:479–486
Parent AS, Teilmann G, Juul A, Skakkebaek NE, Toppari J, Bourguignon JP (2003) The timing of normal puberty and the age limits of sexual precocity: variations around the world, secular trends, and changes after migration. Endocr Rev 24:668–693
Petersen AC, Crockett L, Richards M, Boxer A (1988) A self-report measure of pubertal status: reliability, validity, and initial norms. J Youth Adolesc 17:117–133
Rasier G, Parent AS, Gerard A, Lebrethon MC, Bourguignon JP (2007) Early maturation of gonadotropin-releasing hormone secretion and sexual precocity after exposure of infant female rats to estradiol or dichlorodiphenyltrichloroethane. Biol Reprod 77:734–742
Rasier G, Parent AS, Gerard A, Denooz R, Lebrethon MC, Charlier C, Bourguignon JP (2008) Mechanisms of interaction of endocrine-disrupting chemicals with glutamate-evoked secretion of gonadotropin-releasing hormone. Toxicol Sci 102:33–41
Roelants M, Hauspie R, Hoppenbrouwers K (2009) References for growth and pubertal development from birth to 21 years in Flanders, Belgium. Ann Hum Biol 36:680–694
Schlossberger NM, Turner RA, Irwin CE Jr (1992) Validity of self-report of pubertal maturation in early adolescents. J Adolesc Health 13:109–113
Smith EP, Boyd J, Frank GR, Takahashi H, Cohen RM, Specker B, Williams TC, Lubahn DB, Korach KS (1994) Estrogen resistance caused by a mutation in the estrogen-receptor gene in a man. N Engl J Med 331:1056–1061
Sorensen K, Aksglaede L, Petersen JH, Juul A (2010) Recent changes in pubertal timing in healthy Danish boys: associations with body mass index. J Clin Endocrinol Metab 95:263–270
Talma H, Schonbeck Y, van Dommelen P, Bakker B, van Buuren S, Hirasing RA (2013) Trends in menarcheal age between 1955 and 2009 in the Netherlands. PLoS One 8:e60056
Vercauteren M, Susanne C (1985) The secular trend of height and menarche in Belgium: are there any signs of a future stop? Eur J Pediatr 144:306–309
Acknowledgments
Supported by the “Belgian Fonds de la Recherche Scientifique Médicale” , the University of Liège and the Belgian Study Group for Pediatric Endocrinology.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Bourguignon, JP., Domine, F., Glowacz, F., Lebrethon, MC., Parent, AS. (2015). Changes in Pubertal Timing: Past Views, Recast Issues. In: Bourguignon, JP., Carel, JC., Christen, Y. (eds) Brain Crosstalk in Puberty and Adolescence. Research and Perspectives in Endocrine Interactions, vol 13. Springer, Cham. https://doi.org/10.1007/978-3-319-09168-6_12
Download citation
DOI: https://doi.org/10.1007/978-3-319-09168-6_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-09167-9
Online ISBN: 978-3-319-09168-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)