
Abstract
The treatment of uveitis has always been a delicate balancing act of managing complications of the disease and the toxicity of the ensuing therapy. Systemic medications have potential side effects to various organ systems in the body and the inherent risk of infectious complications.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The treatment of uveitis has always been a delicate balancing act of managing complications of the disease and the toxicity of the ensuing therapy. Systemic medications have potential side effects to various organ systems in the body and the inherent risk of infectious complications. Therapies such as topical or injection of local steroids can potentially induce glaucoma and cataract formation but have the advantage of limited systemic complications. While long sustained local therapy has been technologically established such as Vitrasert® (intravitreal ganciclovir) for the treatment of CMV retintitis [1–3], and Retisert® (intravitreal fluocinolone acetonide) for uveitis, these therapies have the disadvantage of requiring insertion in the operating room. Additionally, Retisert has a high incidence of cataract development and glaucoma [4–6]. The advent of an office placed low risk dexamethasone implant has provided a new treatment in our armamentarium against uveitis.
Design Concepts of the Ozurdex® Implant
The Ozurdex® implant develop by Allergan, Inc. is a novel drug delivery system that can be placed in an office setting via a 22 gauge needle thru the pars plana into the vitreous cavity. The injection device delivers an implant that is completely biodegradable, slowly releasing dexamethasone over 90 days. Originally developed by Oculex Pharmaceuticals, the Novadur® drug delivery system uses a d,l-lactide-co-glycolide (PLG) biodegradable polymer matrix that slowly devolves to lactic acid and glycolic acid releasing dexamethasone (Fig. 46.1). The lactic acid and glycolic acid further degrade into carbon dioxide and water (Figs. 46.2 and 46.3). The platform is loaded with 0.7 mg of dexamethasone in a 400 μg diameter cylinder. The implant is FDA approved for the treatment of uveitis, macular edema following branch or central retinal vein occlusion, and more recently diabetic macular edema. The injection device itself is a novel design delivery device unlike a traditional injection needle. The injection device has a “safety pin” that is first removed, then the protective cap from the needle. Instead of pushing a “plunger” to deliver the drug, a push button activates a pin that pushes the drug out thru the bore of the needle and into the eye. The push button has a hard fixed stop with a mild “click” when the button has been fully depressed and drug delivered (Fig. 46.4).

Microscopic appearance of complete Ozurdex implant *courtesy Allergan

Microscopic appearance of Ozurdex after dissolving for 3 weeks *courtesy Allergan

Dissolving Ozurdex 72 days after implantation in human eye

Ozurdex® injector device with dexamethasone pellet highlighted
Clinical Studies
The first large study published reported the efficacy and safety of Ozurdez in the treatment of macular edema (causes of macular included diabetic retinopathy, retinal vein occlusions, uveitis, or Irvine-Gass syndrome with persistent macular edema). This was a 6 month, multi-center trial with 315 patients enrolled. Of the patients randomized to the 0.7 mg dexamethasone implant, 35 % demonstrated a 10 or more letter improvement (via ETDRS testing) at 90 days from injection compared to 13 % of the control group (sham injection). Improvement in BCVA (best corrected visual acuity) of 15 letters or more was achieved in 18 % of patients versus 6 % in controls. Additionally, the concern regarding intraocular pressure (IOP) elevation was lower than expected with 11 % of patients developing a 10 mm hg or higher rise in IOP compared to 2 % of controls.
During the study, OCTs were used to monitor response with a dramatic improvement/resolution of macular edema in those treated with Ozurdex [7]. However, in the entire study, there were only 5 patients with uveitis enrolled.
To further expand the possible benefit of the implant specifically in patients with uveitis, a large scale randomized clinical trial was completed to evaluate the efficacy of the dexamethasone implant in patients with non-infectious posterior uveitis (Huron Study). Patients were randomized to sham injection or one of two dexamethasone dosages (0.35, 0.7 mg).
In this study, 229 patients from 18 countries were enrolled. 81 % had the diagnosis of intermediate uveitis with the remainder having various forms of posterior uveitis. Those patients receiving the 0.7 mg injection had a dramatic improvement in vitreous haze (Fig. 46.5) with nearly half of the patients achieving a haze score of “0”. 90 % had a one step improvement in haze and a significant portion had a two step improvement (Figs. 46.6 and 46.7) with the effect continuing for 6 months.

Demonstration of vitreous haze (vitreous haze score of zero) at various time weekly time points compared to sham. Reprinted from Archives of Ophthalmology; 2011 vol. 129(5) pp. 545–553. Copyright © (2011) American Medical Association. All rights reserved

Percentage of patients with at least a 2 unit improvement in vitreous haze at weekly time points. Reprinted from Archives of Ophthalmology; 2011 vol. 129(5) pp. 545–553. Copyright © (2011) American Medical Association. All rights reserved

Percentage of patients with a >25 mmHg increase in IOP at weekly time points. Reprinted from Archives of Ophthalmology; 2011 vol. 129(5) pp. 545–553. Copyright © (2011) American Medical Association. All rights reserved
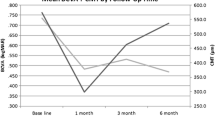
Fortunately, the complications of the sustained release dexamethasone implant were lower than those reported for Retisert. The rate of cataract formation in the implant group was 11.8 % compared to 5.3 % in those receiving sham injection. Additionally, IOP elevation of 10 mm hg over baseline was only seen in 15–20 % of patients, with the majority of patient not requiring IOP lowering medications. With those that required therapy, most only needed one topical drop (Fig. 46.8) compared to 40 % or greater in patients receiving the Retisert® implant.

Number of IOP lowering medications required by patients reveiving the Ozurdex implant at various time points. Reprinted from Archives of Ophthalmology; 2011 vol. 129(5) pp. 545–553. Copyright © (2011) American Medical Association. All rights reserved
Since these initial studies and the subsequent FDA approval, the familiarity and clinical use has become more common in clinical practice. The use has been expanded to pediatric cases and also as a pre-treatment prior to cataract removal [8, 9]. However, there have been reported cases of a higher than expected IOP rise occasionally necessitating removal [10]. Caution should always be taken in the usage in the pediatric population.
In adults, the implant has shown similar success as was demonstrated in the preliminary studies, with newer small clinical studies showing benefit in cases with persistent macular edema [11] and long term uveitic disease [12]. The only new complication that has been described has been the anterior migration of the implant into the anterior chamber in a pseudophakic eyes [13], but this appears extremely uncommon.
Injection Technique and Clinical Use
The eye is prepped in steroid fashion. Topical betadine preparation of the eye with an eyelid speculum is used. Due to the size of the injection needle (22 gauge) subconjunctival lidocaine usually is more comfortable, though topical anesthesia can also be utilized.
Due to the occasional resistance of the needle going thru the scleral and possible reflux of intraocular fluid thru the wound, a toothed forcep helps with counter traction and to pinch the wound closed after the needle is removed.
The needle of the Ozurdex® injection device has a collar to indicate the depth needed before injection of the drug. Typically, the needle is inserted at an angle in a beveled manner after the “safety pin” and cap are removed. Once the needle has been inserted to the collar, the push button is fully depressed injecting the drug.
While the injection technique is extremely easy, the clinical use still requires the “art of medicine” in clinical use. Though it is tempting to use the injection for anterior uveitis, one must remember that the implant has only been FDA approved for the use in posterior segment disease. With most cases of anterior uveitis, inflammation is generally easily controlled with topical drops or local therapy.
With posterior disease the treatment varies. While the initial studies did guide the use, uveitis tends to be a widely varying disease that requires a more balanced management. Typically, in patients with pars planitis, that might wax and wane with occasional cystoid macular edema. Ozurdex tends to be a great treatment protocol as the injection tend to be infrequent with very low chance of cataract or glaucoma development. However, in more serious posterior disease, Ozurdex might not be indicated such as in cases of Behcet’s where long term sustain therapy is more ideal due to possible loss of vision from gaps in treatment such as when the concentration of dexamethasone is at its lowest around 90 days. However, sometimes Ozurdex can be used as a “bridge” in these more serious conditions to rapidly gain control of inflammation or resolve macular edema while systemic therapies are initiated, that typically take 3–4 weeks to become effective.
The most difficult clinical decision is deciding on treatment for chronic, aggressive posterior disease. The typical decision is a tough choice between longterm oral therapy, Retisert® implantation, or repeated Ozurdex. Sometimes the choice can be pretty straightforward, such as a young phakic patient where oral therapy would be more favorable, or a young female trying to have children, where Ozurdex® or Retisert® would be more logical. While longterm repeated Ozurdex has been used successfully with a lower incidence of IOP rise compared to Retisert®, one still worries about aggressive disease and the nadir that occurs every 3 months as the drug runs out subjecting a patient to a possible uveitis flare and irrecoverable loss of vision.
Understanding the clinical disease, the benefits and risk of treatment help guide the clinician in the choice of treatment. The Ozurdex® implant has greatly expanded that choice.
Conclusion
Uveitis tends to be a chronic, smoldering disease. The development of the Ozurdex® implant has allowed a very effective therapy for the treatment of uveitis with a better side effect profile compared to the operating room placed Retisert® implant. The novel development of the polymer used in the implant has the benefit of not leaving any residual implanted material in the eye, dissolving to just water and carbon dioxide. As sustained intraocular delivery of drugs continue to evolve, Ozurdex® represents a significant step in this evolution and treatment of uveitis.
References
Martin DF, Parks DJ, Mellow SD, et al. Treatment of cytomegalovirus retinitis with an intraocular sustained-release ganciclovir implant. A randomized controlled clinical trial. Arch Ophthalmol. 1994;112(12):1531–9.
Musch DC, Martin DF, Gordon JF, Davis MD, Kuppermann BD. Treatment of cytomegalovirus retinitis with a sustained-release ganciclovir implant. The Ganciclovir Implant Study Group. N Engl J Med. 1997;337(2):83–90.
Sanborn GE, Anand R, Torti RE, et al. Sustained-release ganciclovir therapy for treatment of cytomegalovirus retinitis. Use of an intravitreal device. Arch Ophthalmol. 1992;110(2):188–95.
Callanan DG, Jaffe GJ, Martin DF, Pearson PA, Comstock TL. Treatment of posterior uveitis with a fluocinolone acetonide implant: three-year clinical trial results. Arch Ophthalmol. 2008;126(9):1191–201.
Goldstein DA, Godfrey DG, Hall A, et al. Intraocular pressure in patients with uveitis treated with fluocinolone acetonide implants. Arch Ophthalmol. 2007;125(11):1478–85.
Jaffe GJ, Martin D, Callanan D, Pearson PA, Levy B, Comstock T. Fluocinolone acetonide implant (Retisert) for noninfectious posterior uveitis: thirty-four-week results of a multicenter randomized clinical study. Ophthalmology. 2006;113(6):1020–7.
Williams GA, Haller JA, Kuppermann BD, et al. Dexamethasone posterior-segment drug delivery system in the treatment of macular edema resulting from uveitis or Irvine-Gass syndrome. Am J Ophthalmol. 2009;147(6):1048–54, 1054.e1.
Bratton ML, He YG, Weakley DR. Dexamethasone intravitreal implant (Ozurdex) for the treatment of pediatric uveitis. J AAPOS. 2014;18(2):110–3.
Cordero-Coma M, Garzo I, Calleja S, Galan E, Franco M, Ruiz de Morales JG. Preoperative cataract surgery use of an intravitreal dexamethasone implant (Ozurdex) in a patient with juvenile idiopathic arthritis and chronic anterior uveitis. J AAPOS. 2013;17(6):632–4.
Kumari N, Parchand S, Kaushik S, Singh R. Intractable glaucoma necessitating dexamethasone implant (Ozurdex) removal and glaucoma surgery in a child with uveitis. BMJ Case Rep. 2013;2013.
Cao JH, Mulvalhill M, Zhang L, Joondeph BC, Dacey MS. Dexamethasone Intravitreal Implant in the treatment of persistent uveitic macular edema in the absence of active inflammation. Ophthalmology 2014.
Tomkins-Netzer O, Taylor SR, Bar A, et al. Treatment with repeat dexamethasone implants results in long-term disease control in eyes with noninfectious uveitis. Ophthalmology 2014.
Malcles A, Janin-Manificat H, Yhuel Y, et al. Anterior chamber migration of intravitreal dexamethasone implant (Ozurdex(R)) in pseudophakic eyes: report of three cases. J Fr Ophtalmol. 2013;36(4):362–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Wang, R. (2017). Surgical Therapy: Dexamethasone Biodegradable Intravitreal Implant (Ozurdex®). In: Papaliodis, G. (eds) Uveitis. Springer, Cham. https://doi.org/10.1007/978-3-319-09126-6_46
Download citation
DOI: https://doi.org/10.1007/978-3-319-09126-6_46
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-09125-9
Online ISBN: 978-3-319-09126-6
eBook Packages: MedicineMedicine (R0)