
Abstract
Pectus excavatum is a common abnormality of the chest wall that ranges from a mild cosmetic deformity to a severe condition with crippling effects on cardiac and pulmonary function coupled with associated anomalies. As the condition often changes in severity during periods of growth, it is best to wait until late adolescence when operative repair is indicated, if the clinical status of the child allows a period of observation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Pectus excavatum is a common abnormality of the chest wall that ranges from a mild cosmetic deformity to a severe condition with crippling effects on cardiac and pulmonary function coupled with associated anomalies. As the condition often changes in severity during periods of growth, it is best to wait until late adolescence when operative repair is indicated, if the clinical status of the child allows a period of observation.
-
1.
Classification of pectus deformity
-
(a)
Pectus excavatum: “funnel chest” – sunken/concave appearance of the sternum and ribs with a “soup bowl” or “Death Valley” appearance. Approximate occurrence is one in every 400 births.
-
(b)
Pectus carinatum: “pigeon chest” – outward protrusion of the sternum and ribs with a bird-like appearance of the chest.
-
(c)
Combined deformity: asymmetric or mixed deformity with tilt of the sternum off of the coronal plane, flaring of the ribs, and disordered alignment of the ribs.
-
(d)
Chest wall deficits: missing components of the rib cage including missing vertebrae, hemivertibrae, missing ribs, fused ribs, missing clavicles, and can also include deficits in the soft tissue of the chest.
-
(i)
Poland syndrome is characterized by unilateral chest wall deficit and can extend to missing pectoral muscle, breast, and limb component deficits.
-
(ii)
Jeune’s asphyxiating thoracic dystrophy is characterized by failure of rib growth and a bell-shaped chest with a narrow apex. Patients often have difficulty handling secretions and require tracheostomy.
-
(iii)
Jarcho-Levin syndrome (spondylothoracic dysplasia) is characterized by shortened deformed thoracic vertebrae and associated pulmonary, cardiac, and renal anomalies and a corresponding high mortality.
-
(iv)
Pentalogy of Cantrell is a condition with 75 % mortality due to the sequelae of five components:
-
1.
Pericardial defect.
-
2.
Ectopia cordis.
-
3.
Sternal deficit.
-
4.
Anterior diaphragm hernia.
-
5.
Abdominal wall defect.
-
1.
-
(i)
-
(e)
Pectus excavatum can be associated with other disorders:
-
(i)
Marfan syndrome may be present. Individuals often have an earlier presentation and greater severity of defect. Individuals with Marfan syndrome must be evaluated for the presence of aortic root dilation as it carries a risk of aortic dissection.
-
(ii)
Ehlers-Danlos syndromes: soft tissue defect with hyperextensible joints and loose skin.
-
(i)
-
(a)
-
2.
Etiology of pectus excavatum is thought to be related to disordered or rapid growth of costal cartilages during periods of rapid growth, such as adolescence.
-
3.
Clinical effects of pectus excavatum:
-
(a)
Pain: disordered costal-chondral joints at edge of sternum can hurt with activity.
-
(b)
Cardiac: patient may experience palpitations, fainting, or mitral valve prolapse with murmur.
-
(c)
Pulmonary: Shortness of breath, exercise intolerance, and restrictive defect on pulmonary function testing.
-
(d)
Scoliosis is present in 15 % of patients with pectus excavatum.
-
(e)
Psychosocial: Embarrassment when chest is exposed, avoidance of activities such as swimming, use of baggy or loose clothing to hide defect, behavioral changes, teasing in school or sports, depression, and suicidal ideation may be present, and may not be elicited unless specifically queried.
-
(f)
Cosmetic component: This is often erroneously thought to be the only aspect of the disease and can introduce problems for patients when they seek medical insurance approval for treatment.
-
(a)
-
4.
Evaluation of pectus excavatum:
-
(a)
Physical examination:
-
(i)
Examination of chest including ribs, sternum, clavicles, breath sounds, and heart tones/rhythm.
-
(ii)
Look for signs of Marfan syndrome: lens abnormality, high arched palate, tall height, long thin fingers, hyperextensible joints, heart murmur.
-
(iii)
Evaluate for scoliosis.
-
(i)
-
(b)
Other studies:
-
(i)
Chest x-ray: Check cardiac silhouette, ribs and vertebrae
-
(ii)
Spine series: Evaluate for scoliosis.
-
(iii)
Pulmonary function tests: Evaluate for restrictive defect, can be required for insurance approval of repair.
-
(iv)
Echocardiography: Evaluate for dilated aortic root and mitral valve prolapse.
-
(v)
Computed tomography chest:
-
1.
Non-contrast.
-
2.
Calculate Haller index: Measure widest transverse distance across thoracic cavity (inside ribcage) and divide by smallest antero-posterior distance across thoracic cavity (from back of sternum to front of spine). Normal value is 2.5. Haller index greater than 3.2 is considered severe pectus excavatum, and this value is sometimes required for insurance approval of repair. Value less than 2 is abnormal and indicated pectus excavatum. There is a wide crossover between normal and abnormal.
-
3.
Calculate correction index: Measure the antero-posterior distance from most anterior costal ridge to deepest portion of sternal depression and divide by antero-posterior depth of chest, including ribs, as a percentage. This newer index better discriminates between normal and pectus excavatum. Normal value is <10 %.
Fig. 1 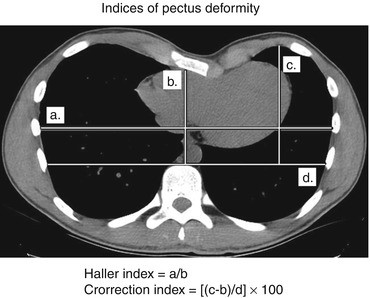
Indices of pectus deformity. The Haller index is obtained by dividing the width of the thoracic cavity by the depth. The Correction index is obtained by dividing the difference between the highest costal ridge and the lowest depth of sternal depression by the width of the thoracic cavity at the anterior vertebral margin. Source: Christopher Coppola
-
4.
Aortic root diameter can also be measured.
-
1.
-
(i)
-
(a)
-
5.
Treatment of pectus excavatum.
-
(a)
When no cardiac or pulmonary disturbance or pain is present, patients and families may choose observation only, and live with the thoracic defect, returning for care if the condition worsens or physiologic symptoms develop.
-
(b)
Surgical repair of defect, when chosen, is best deferred until age 15-years-old or older, because there is a higher incidence of recurrence in children who are repaired younger.
-
(c)
Ravitch repair: This method has been available longer. The anterior chest is incised either transversely or midline. The cartilaginous segments connecting bilateral ribs five to eight (with adjustment for individual cases) are resected. The sternum is fractured transversely between the fourth and fifth ribs, and it is repositioned anteriorly to correct the central depression. A short bar spanning the severed ends of the seventh ribs is used to support the sternum in this position.
-
(d)
Nuss repair: bilateral axillary incisions are made at the same level of the deepest depression of sternum. Using a thoracoscope for guidance, a curved bar is guided in one incision and out the other, passing beneath the sternum to elevate it into a more anterior position. The ends of the bar are secured to the intercostal muscles bilaterally. The bar is removed after 3 years when the corrected shape of chest has stabilized.
-
(e)
Patient may require a chest tube, and a chest x-ray must be obtained after operation.
-
(f)
Recovery: Patients are hospitalized 5–7 days after repair. To avoid bar dislodgement, patients must avoid lying on the side, twisting the torso, or lifting themselves up with the arms. An epidural catheter with local anesthetic improves pain control.
-
(g)
Patients will usually miss school for 3 weeks, no lifting or gym class for 6 weeks, and full impact sports, such as football, are allowed after 3 months. Most patients require oral analgesics for 6 weeks.
-
(h)
Repair may be complicated by hemorrhage, pulmonary injury, cardiac injury, arrhythmia, pneumothorax, infection, effusion, seroma, chronic pain, bar dislodgement, allergy to metal in bar, and recurrence of defect.
-
(a)
-
6.
Treatment of pectus carinatum
-
(a)
Patients can be treated an orthotic brace which places pressure on the protrusion of the sternum. If the child can tolerate wearing the brace for 12 h each day for a year, there is a good success rate. The brace must be individually fit to the patient and adjusted as progress is made. Side effects are pain and damage to skin at the brace contact points.
-
(b)
Pectus carinatum can be surgically repaired by the open Ravitch method.
-
(a)

Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Coppola, C.P. (2014). Pectus Deformity. In: Coppola, C., Kennedy, Jr., A., Scorpio, R. (eds) Pediatric Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-04340-1_57
Download citation
DOI: https://doi.org/10.1007/978-3-319-04340-1_57
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-04339-5
Online ISBN: 978-3-319-04340-1
eBook Packages: MedicineMedicine (R0)