
Abstract
Definition: Sarcoma with alveolar, pseudo-endocrine, and organoid structure.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Definition: Sarcoma with alveolar, pseudo-endocrine, and organoid structure.
Epidemiology: Rare, females, 15–35 years old.

Location: Deep-seated, lower limb within the muscle, thigh.
Clinical: Globose or multinodular mass, slowly increasing, and painless. Tumor may be large, present from many years, and richly vascularized with pulsation on the mass.
Imaging: On CT: an intense uptake of contrast medium. On angiography: tumoral neoangiogenesis and indirect signs of arteriovenous shunt. On MRI: bright on both T1 and T2, homogeneous on the first and inhomogeneous with sharp peripheral demarcation of the mass on the second.
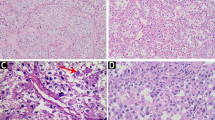
Histopathology: Soft, yellowish-white, or gray-red-purple, with hemorrhagic and necrotic areas, poorly delimited. Typical very glandular, acinar, and alveolar appearance. Nests of tumor cells are separated by thin-walled vascular spaces. Cells are large, epithelioid, globose-polyhedric, with eosinophilic granular to clear cytoplasm. The nucleus is vesicular, the nucleolus evident, mitotic figures rare, pleomorphism and hyperchromia, and sporadic giant cells with monstrous nuclei. Intense neoangiogenesis and frequent vascular invasion. At genetic level, this tumor is characterized by an unbalanced translocation: der(17)t(X;17)(p11;p25), resulting in the fusion of a gene of unknown function ASPL on chromosome 17 to the TFE3 transcription factor gene on the X chromosome.
Course and Staging: Recurrences are frequent when treated inadequately. Metastases may be present at diagnosis and at the first signs of the lesion. At times, they occur very late, even 10 years after the diagnosis. Usually, stage II B or III B.
Treatment: Wide or radical excision associated to adjuvant radio- and/or chemotherapy.
FormalPara Chromosomal Translocationst(X;17) (p11;q25) | ASPL-TFE3 (type 1, type 2) | 100 % |

Eosinophilic wide cells losing cohesion and giving the alveolar appearance

PAS stain with diastase digestion demonstrates rod-shaped crystals (inset: higher magnification)
Selected Bibliography
Agarwal S, Gupta R, Iyer VK, Mathur SR, Ray R (2011) Cytopathological diagnosis of alveolar soft part sarcoma, a rare soft tissue neoplasm. Cytopathology 22:318–322
Folpe AL, Deyrup AT (2006) Alveolar soft-part sarcoma: a review and update. J Clin Pathol 59(11):1127–1132. Review
Khanna P, Paidas CN, Gilbert-Barness E (2008) Alveolar soft part sarcoma: clinical, histopathological, molecular, and ultrastructural aspects. Fetal Pediatr Pathol 27(1):31–40
Weiss SW (2002) Alveolar soft part sarcoma: are we at the end or just the beginning of our quest? Am J Pathol 160(4):1197–1199. Review
Zarrin-Khameh N, Kaye KS (2007) Alveolar soft part sarcoma. Arch Pathol Lab Med 131(3):488–491. Review
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Gambarotti, M. (2014). Alveolar Soft Part Sarcoma. In: Picci, P., Manfrini, M., Fabbri, N., Gambarotti, M., Vanel, D. (eds) Atlas of Musculoskeletal Tumors and Tumorlike Lesions. Springer, Cham. https://doi.org/10.1007/978-3-319-01748-8_77
Download citation
DOI: https://doi.org/10.1007/978-3-319-01748-8_77
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-01747-1
Online ISBN: 978-3-319-01748-8
eBook Packages: MedicineMedicine (R0)