
Abstract
We now regard a 16-year-old female patient, a high school student without previous complaints, who suddenly became ill, experiencing abdominal pain and vomiting. After 3 days, the complaints worsened and the patient was referred to our surgical department. She appeared to be dehydrated, had a fever of 38.7 °C, tachycardia, and she displayed a poor general aspect. Physical examination of the abdomen showed upper abdominal pain with signs of local peritonitis. The laboratory results showed a leukocytosis of 21,000/L and a CRP of 180 mg/L were found. A CT scan with oral and IV contrast was performed. A gastric dilatation with pneumatosis in the stomach wall was found with dilatation of duodenum and possible compression of the horizontal part of the duodenum. Differential diagnosis was made between annular pancreas and duodenal web.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Diagnosis and Indication for Surgery
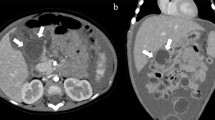
We now regard a 16-year-old female patient, a high school student without previous complaints, who suddenly became ill, experiencing abdominal pain and vomiting. The general practitioner observed her at home under an initial diagnosis of gastro-enteritis. After 3 days, the complaints worsened and the patient was referred to our surgical department. She appeared to be dehydrated, had a fever of 38.7 °C, tachycardia, and she displayed a poor general aspect. Physical examination of the abdomen showed upper abdominal pain with signs of local peritonitis. The laboratory results showed a leukocytosis of 21,000/L and a CRP of 180 mg/L were found. A CT scan with oral and IV contrast was performed. A gastric dilatation with pneumatosis in the stomach wall was found with dilatation of duodenum and possible compression of the horizontal part of the duodenum (Fig. 18.1). Differential diagnosis was made between annular pancreas and duodenal web.

CT scan showing gastric dilatation and pneumatosis. Gas in the portal veins
Operation
At emergency laparotomy, a clear compression of the horizontal part of duodenum by the superior mesenteric vessels against the spine was seen. Moreover, gastric dilatation with necrosis of the fundus was found (Fig 18.2).

Aspect of the operation, stomach is dilated and the greater curvature is necrotic
A resection of the necrotic part of the gastric fundus along the greater curvature was performed by means of staplers and a running suture over it. Moreover, to treat the cause, a side-to-side duodenojejunostomy was performed in two layers (Fig. 18.3).

After resection of the greater curvature and duodenojejnunostomy
Postoperative Course
Postoperatively, the patient recovered very quickly and could initiate oral feeding progressively from the 3rd day on. At day 7 she went home and after a period of 4 weeks she could reinitiate her daily activities and studies.
Discussion
Wilkie’s syndrome is a rare cause of duodenal passage problems. It is produced by compression of the superior mesenteric artery on the horizontal duodenal part. Chronic complaints are typical with dilatation of the duodenum and stomach. Acute complication is very rare and in this young patient led to gastric dilatation and necrosis of the greater curvature.
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Cuesta, M.A., van der Peet, D.L. (2014). Case on An Acute Complication of the Wilkie Syndrome. In: Cuesta, M., Bonjer, H. (eds) Case Studies of Postoperative Complications after Digestive Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-01613-9_18
Download citation
DOI: https://doi.org/10.1007/978-3-319-01613-9_18
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-01612-2
Online ISBN: 978-3-319-01613-9
eBook Packages: MedicineMedicine (R0)