
Abstract
8-Aminoquinolines are an important class of antimalarial drugs because they are effective against the liver stages of Plasmodium infections and thus are administered for radical cure and presumptive antirelapse therapy against relapsing malaria. In this chapter, we discuss two 8-aminoquinolines, primaquine and tafenoquine. Primaquine was identified in 1946 and has been used extensively to clear liver-stage parasites, especially those from Plasmodium vivax. These can persist in the liver for months, as a dormant form of the parasite (the hypnozoite), which re-emerges much later to cause clinical disease. Tafenoquine, a primaquine analog, is currently under advanced clinical development. Tafenoquine has a much longer elimination half-life compared with primaquine (14 days versus 6 h) and is highly effective both in treating relapses of P. vivax malaria and as a causal prophylactic agent against P. falciparum and P. vivax malaria. A major drawback to the 8-aminoquinolines is their toxicity in glucose-6-phosphate dehydrogenase (G6PD)-deficient individuals. We discuss clinical uses, pharmacokinetics and metabolism, safety and tolerability, mechanisms of action and drug resistance for both these drugs.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
The 8-aminoquinolines have a long history, being the first chemotype of synthetic antimalarials when pamaquine was used from the late 1920s [1]. In 1946, the screening of a large number of 8-aminoquinolines identified primaquine as a relatively safe and efficacious compound [2]. Today, additional 8-aminoquinolines have been synthesised as the search for safer and more efficacious compounds continues. From these efforts, tafenoquine is now in advanced clinical development and may become a new addition to the arsenal of antimalarial drugs.
The 8-aminoquinolines are effective against the exo-erythrocytic liver stages of the malaria parasite. This is central to preventing relapsing malaria as well as causal prophylaxis for malaria infections. Causal prophylaxis refers to the killing of parasites while they are in the liver, and thus prevents infection of erythrocytes and any signs of clinical disease. The efficacy of 8-aminoquinolines against liver-stage infection is especially valuable in the clearance of P. vivax and P. ovale, in which latent liver-stage forms known as hypnozoites can persist in the liver for months to years. Relapse infection occurs when the hypnozoites exit dormancy and differentiate into merozoites, which rupture from the hepatocyte to cause a blood-stage infection. In addition to being the only class of drugs with activity against hypnozoites, 8-aminoquinolines are active against gametocytes and thus interfere with malaria transmission.
2 Primaquine
2.1 Chemistry
The chemical name of primaquine is 6-methoxy-8-(4-amino-1-methylbutyl) aminoquinoline and its chemical formula is C15H12N3O, with a molecular weight of 259 (Fig. 1). Primaquine is a racemic mixture composed of d- and l-enantiomers, due to the presence of an asymmetric chiral center. It is water soluble and solutions are stable when protected from light. Primaquine tablets are given in the form of the diphosphate salt containing either 13.2 mg (= ~7.5 mg base) or 26.3 mg (= ~15 mg base).

Structure of Primaquine
2.2 Clinical Use
There are three established indications for the use of primaquine: causal prophylaxis for all species of malaria, presumptive antirelapse therapy (terminal prophylaxis or postexposure prophylaxis) for P. vivax and P. ovale and radical cure of P. vivax and P. ovale infections. Since the use of primaquine depends on the species of parasite, an understanding of malaria endemicity is necessary for adequate prophylaxis use and highlights the importance of diagnostics for appropriate treatment. Primaquine primarily targets the exo-erythrocytic stage of the parasite’s life cycle. It is much less effective at killing the asexual blood-stage parasites of P. falciparum, as evidenced by in vivo and in vitro studies [3–5]. Asexual blood stages of P. vivax, however, are more sensitive to primaquine and administration of a daily dose of 45 mg for 14 days to human subjects demonstrated 80% efficacy in clearing parasitaemia with the primaquine-tolerant Chesson strain of P. vivax [6]. In less tolerant strains of P. vivax, such as those found in Thailand, a daily dose of 30 mg (0.5 mg/kg) of primaquine was 100% effective at clearing blood-stage parasitaemia [7, 8].
2.3 Chemoprophylaxis
Causal prophylaxis of primaquine is dependent on the dose and the timing of administration. Although primaquine is not currently labeled for use as a causal prophylactic agent, in experimental challenge studies, a single 30-mg primaquine dose given 1 day following infection with P. falciparum sporozoites prevented the development of blood-stage parasitaemia. However, lower doses or doses given before or on the day of challenge did not provide adequate protection against P. falciparum [3, 9]. Daily primaquine dosing before infection and throughout the exo-erythrocytic development prevented malaria [9, 10]. These studies demonstrate that there is a small therapeutic window for primaquine.
Discrepancy exists regarding the minimal effective dose of primaquine for causal prophylaxis against Plasmodium spp. [11, 12]. Several studies support that the most effective dose for primaquine prophylaxis is 30 mg daily. A daily dose of 30 mg primaquine was administered for one year to non-immune Indonesian adults and was found to be 90% and 94% efficacious against P. vivax and P. falciparum, respectively [13, 14]. Efficacy dropped when an alternate-day dosing scheme of 30 mg primaquine was administered [15]. Similar results were observed in a prophylaxis study of Colombian soldiers, with protective efficacies of 94% (P. falciparum) and 85% (P. vivax) following 30-mg primaquine daily for 16 weeks [16].
2.4 Presumptive Antirelapse Therapy and Radical Cure
The prevention of P. vivax and P. ovale relapse infection is unique to primaquine. Primaquine is FDA approved and licensed for presumptive antirelapse therapy and radical cure of P. vivax and P. ovale. The licensure approval was based on data gathered from US soldiers returning from the Korean War in the 1950s. To prevent P. vivax relapse from returning soldiers, a daily dose of 15 mg primaquine for 14 days was used. This dose was used for two reasons; the Korean P. vivax strain infecting US military personnel was efficiently cleared with this dosing regimen and haemolytic anaemia in individuals with glucose-6-phosphate dehydrogenase (G6PD) deficiency, a condition more prevalent in African Americans, was less likely to cause a life-threatening condition with this dose [17]. This approved dosing scheme persisted in the face of clinical data suggesting that P. vivax strains from Southeast Asia and Oceania were tolerant of a 15-mg dose and therefore higher doses were required [18]. Subsequently, reports from nearly all P. vivax endemic areas indicate that the standard daily 15 mg primaquine dose for 14 days has failed to prevent relapses [11, 12].
It has been suggested that the total dose of primaquine may be more important than the particular regimen used as presumptive antirelapse or radical cure therapy [19–21]. For example, a total dose of 420 mg was equally effective if given at 30 mg/day for 14 days or 60 mg/day for 7 days [22]. This observation was supported by a recent evaluation of numerous P. vivax antirelapse therapy trials in which total primaquine dose was assessed [23]. Collectively, it was demonstrated that treatment success positively correlated with increasing primaquine dose as a function of body weight. This observation supports recent recommendations of a primaquine therapeutic dose of 0.5 mg/kg daily for 14 days [12]. It was further recognised that additional factors such as geographical-specific relapse rates and tolerance to primaquine should be considered when advocating the most efficacious antirelapse therapy. It should be noted that although higher doses of primaquine have been advocated, US FDA approval is only for the 15 mg/day for 14 days regimen [11].
Poor compliance with the 14-day standard primaquine therapy and treatment studies suggesting total dose is more important than dosing schedule have led to the investigation of regimens using higher doses of primaquine over a shorter time period for radical cure of P. vivax. Studies conducted in Vietnam found that 96% of the subjects treated with 200 mg artesunate twice daily for 2 days followed by 22.5 mg primaquine twice daily for 7 days cleared blood and liver stage infection based on a 28-day follow-up period [24]. A study conducted in Thailand investigated the administration of either a 30-mg primaquine daily dose for 7 days versus a 60-mg primaquine daily dose for 7 days for the treatment of P. vivax. Both dosing regimens were well tolerated and 28-day relapse rates were 11% and 4%, respectively [25]. Similarly, a study testing the antirelapse efficacy of artesunate followed by various doses of primaquine found that 30 mg twice daily for 7 days was as effective as the standard 14 day regimen of 15 mg daily [26]. The short half-life of artesunate suggests that the higher dose of primaquine was the predominant factor for the relative efficacy. Collectively these results suggest that a 1-week course of primaquine could be effective for the treatment of P. vivax.
2.5 Drug Combinations
Several reasons exist to investigate partnering drugs with primaquine: to increase efficacy, shorten the 14-day regime to a dosing schedule that will improve compliance and circumvent the rise of chloroquine-resistant P. vivax. For antirelapse or radical cure therapy, primaquine is usually partnered with another antimalarial drug such as chloroquine (25 mg/kg over 3 days). Since primaquine lacks substantial activity against the asexual erythrocytic stages of P. falciparum and acts slowly against blood stages of P. vivax, a blood schizontocide drug should be administered with primaquine [11]. Early studies suggest that the addition of chloroquine or quinine potentiated the activity of primaquine [27]. A recent report demonstrates that synergy between primaquine and chloroquine may be attributed to the ability of primaquine to increase the accumulation of chloroquine within the parasite [28].
Evaluation of nine different trials that compared a 14-day primaquine plus chloroquine with a 5-day primaquine plus chloroquine regimen concluded that the 14-day primaquine regimen was superior to chloroquine alone or 5-day primaquine plus chloroquine [29]. This evaluation, however, did not take into account the dose of either chloroquine or primaquine. As an alternative to chloroquine plus primaquine for the treatment of vivax malaria, artesunate plus primaquine combinations have been shown to produce markedly shorter parasite and fever clearance times [24, 30]. Although artesunate has no radical curative activity, the rapid action of artemisinins on the blood stages of P. vivax is highly beneficial to the patient, in that infection and malaria symptoms are aborted at a much faster rate than with chloroquine. Furthermore, with increasing reports of chloroquine-resistant P. vivax malaria in Oceania, Southeast Asia, the Indian subcontinent and the Americas [14], artesunate may be considered a potential replacement for chloroquine for aborting an acute attack of vivax malaria.
2.6 Transmission Blocking
In a few malaria-endemic areas, the addition of a single dose of 45 mg primaquine to the treatment regimen had been advocated to reduce gametocyte burden and thus interfere with the transmission cycle of the malaria parasite. Early studies demonstrated that primaquine is a potent gametocytocidal and sporontocidal agent [31]. Several clinical studies demonstrated a primaquine-dependent reduction in gametocyte clearance times, when administered as a single 0.5-mg/kg dose to artesunate or quinine [32], a single 45-mg dose to chloroquine–sulfadoxine–pyrimethamine [33] and a single 0.75-mg/kg dose to artesunate–sulfadoxine–pyrimethamine [34] as compared with treatment groups receiving the various drug combinations without primaquine.
One study did not observe any significant advantage in adding a single 0.75-mg/kg primaquine dose to artesunate–sulfadoxine–pyrimethamine in reducing the gametocyte burden [35]. Discrepancies may be attributed to the methods and the accuracy of detecting submicroscopic levels of gametocytes, as artesunate possesses gametocytocidal activity. The absence of an additive effect of primaquine is consistent with the suggestion that the most effective way to prevent gametocytaemia is to clear asexual blood forms [36]. Since artesunate does not kill mature gametocytes [37], unlike primaquine, and treatment with particular antimalarials induces gametocytogenesis [38], additional transmission-blocking studies are required to address the benefit of adding primaquine to treatment regimens. Future studies are essential since ongoing efforts are aimed at eliminating malaria [39].
2.7 Mechanism of Action
The mechanism of action by which primaquine exerts its antimalarial activity is largely unknown but the mitochondria may be the biological target of primaquine. Specifically, primaquine accumulates within the mitochondria, resulting in swelling and structural changes within the inner membranes [40–44], thus destroying mitochondrial function [45–47]. Primaquine is quickly metabolised to several reactive intermediates that are responsible for toxicity to erythrocytes (discussed below) and also apparently for antimalarial activity [48, 49]. Several of the active metabolites are structurally similar to naphthoquinones [50]. The antimalarial activity of naphthoquinones, such as atovaquone, is due to inhibition of mitochondrial function [51, 52]. Atovaquone has been shown to collapse the mitochondrial electron membrane potential, resulting in disruption of pyrimidine biosynthesis [53, 54]. Since asexual blood stage parasites rely on glycolysis for their energy source rather than oxidative phosphorylation-generated ATP, a role in pyrimidine biosynthesis would support the essentiality of the mitochondria for asexual growth and explain the blood-stage antimalarial activity of atovaquone. Primaquine, however, is not an effective blood-stage antimalarial against P. falciparum. Interestingly, swelling of host cell mitochondria was not observed and hydroxynaphthoquinone and naphthoquinone are approximately 1,000-fold more potent against the plasmodial cytochrome bc 1 complex than the mammalian complex [51]. These selectivity differences are believed to be a result of structural differences within the plasmodial bc 1 complex that increases the affinity for selected antimalarials such as atovaquone and 8-aminoquinolines [55].
The metabolism of primaquine produces reactive intermediates that ultimately results in the accumulation of free radicals, hydrogen peroxides and superoxides which may be responsible for antimalarial activity [56]. Such weak activity of primaquine in vitro may be indicative of the fact that primaquine requires metabolism for antimalarial activity [57]. A similar mode of antimalarial action has been suggested for artemisinins, which are metabolized into free radicals [58]. These free radicals may disrupt oxidation–reduction systems, inactivate specific enzymes or attach to and disrupt biological membranes [59].
Although a generalised mechanism of action has been discussed for Plasmodium, it should be acknowledged that different mechanisms may exist depending on the species of Plasmodium. For example, primaquine appears to be effective against asexual blood stages of P. berghei [43, 60] and P. vivax [6–8]; however, it is a poor inhibitor of P. falciparum asexual stages [3]. Additionally, there are discrepancies and inconsistencies with the mechanisms of action of primaquine when compared with that of artemisinins (free radicals and oxidative stress) and atovaquone (collapse mitochondrial electron membrane potential) because the in vitro and in vivo efficiencies and stage specificity of primaquine are clearly different to artemisinins and atovaquone.
2.8 Pharmacokinetics and Metabolism
An oral dose of primaquine is rapidly absorbed, with a mean bioavailability of 96% [61]. Primaquine exhibits linear and first-order kinetics over the dose range of 15–45 mg. The maximum drug concentration (C max) and the time to achieve the maximum concentration (t max) in plasma were 53 ng/mL and 2 h, respectively, following a single dose of 15 mg primaquine to healthy subjects [56]. Primaquine is extensively distributed into body tissues, with an apparent volume of distribution of 200–300 L and a systemic clearance varying between 30 and 40 L/h. The elimination half-life of primaquine is about 6 h [61, 62]. The pharmacokinetic properties of primaquine are comparable between G6PD-normal and G6PD-deficient healthy subjects [63]. Recently, sex-related differences were reported in the pharmacokinetics of primaquine, following multiple dosing of 30 mg primaquine for 14 days, with females having significantly slower clearance (0.31 L/h/kg versus 0.55 L/h/kg) and a lower apparent volume of distribution (3.42 L/kg versus 4.59 L/kg) when compared with males [64]. Further, studies are required to determine whether the increased exposure to primaquine in females leads to increased risk of toxicity compared with males, given the same maintenance dosage.
Excretion studies using 14C-labeled primaquine demonstrated that 64% of the radio label was found in the urine within 143 h after an oral dose [65]. Primaquine is rapidly and completely metabolised, as only 1–4% of the initial compound is found in the urine [61, 66]. Metabolism of primaquine results in the accumulation of numerous unstable intermediates [48]. The major plasma metabolite of primaquine is the inactive carboxyprimaquine but this is thought to be further metabolised as it is not found in urine [65]. Additional metabolites include 5-hydroxyprimaquine, 5,6-dihydroxy-8-aminoquinoline, 6-desmethylprimaquine, 5,6-dihydroxyprimaquine, and 6-methoxy-8-aminoquinoline. It is these later metabolites that are believed to generate oxygen-active species responsible for toxicity of parasite and host cells.
Several different approaches have been investigated to increase the bioavailability and the stability of primaquine. These include different mechanisms of drug administration such as transdermal delivery systems [67], galactose-coated polypropyleneimine nanoparticles as the primaquine vehicle [68] and primaquine encapsulation into liposomes and nanoparticles [69, 70]. These approaches increased stability or exposure time to drug; however, to date, these approaches have not advanced into clinical development to improve the quality of primaquine.
An additional approach used to increase stability and bioavailability is the conjugation of primaquine with amino acids [71] or with polymers of polyaspartamide [72]. The amino acid derivative demonstrated improved stability; however, these conjugates may be readily removed from primaquine via action of aminopeptidases [73]. Polyaspartamide conjugates significantly decreased parasitaemia levels and increased the survival times of mice infected with P. berghei compared with untreated or glucosamine-conjugated primaquine-treated mice. Radical cure, however, was not achieved, as all tested mice eventually died [72]. Nevertheless, these approaches support the proposal that modification or conjugation of primaquine and its analogs may be a viable alternative to increase the efficacy of primaquine. Detailed pharmacokinetic studies must be completed to assess the improved stability and bioavailability of these conjugates over the parent compound.
2.9 Safety and Tolerability
The toxicities associated with primaquine and other 8-aminoquinolines are well known [74]. Haemolytic anaemia is the most serious condition induced by primaquine in G6PD-deficient individuals [75, 76]. Erythrocytes, especially those infected with malaria parasites are prone to oxidative stress. Reduced glutathione (GSH) is important in the detoxification of free radicals. Once oxidised to glutathione disulfide (GSSG), GSH levels are reinstated by the activity of glutathione reductase and NAPDH. Because erythrocytes lack mitochondria, the pentose-phosphate pathway is the only source of NADPH. In G6PD-deficient individuals, NADPH levels are inadequate to restore GSH levels resulting in a compromised antioxidant system; thus, the erythrocytes do not have efficient protective mechanisms to handle oxidative stress. Primaquine is rapidly metabolised into hydroxylated intermediates that result in the generation of peroxides, superoxides and hydroxyated free radicals [49]. In G6PD-deficient individuals, erythrocytes are susceptible to these free radicals, which denature haemoglobin to form Heinz bodies that then react with erythrocyte membranes. This process causes premature lysis or subsequent clearing by the spleen [77, 78]. Although administration of primaquine to G6PD-deficient individuals can cause haemolytic anaemia, there are several factors such as polymorphic variation in G6PD alleles, total drug dose, and duration of the treatment that may modulate the severity of the haemolysis. Nevertheless, G6PD deficiency should be evaluated before the administration of primaquine [11]. Primaquine at the approved dosages for radical cure and presumptive antirelapse therapy is safe when administered to individuals with normal G6PD levels.
Methaemoglobinaemia is also a common toxicity associated with primaquine, which can, in some cases, require treatment with methylene blue. Methaemoglobin (MetHb) is an oxidised form of haemoglobin that cannot bind and transport oxygen to various tissues. Normal MetHb levels are less than 1% of total haemoglobin; however, in individuals deficient for G6PD or methaemoglobin reductase (an NADH-dependent enzyme that converts MetHb to haemoglobin) or under extreme oxidative stress, the levels of MetHb may increase to harmful levels, resulting in cyanosis. Primaquine increases the rate of MetHb formation [79] through oxidative stress via the free-radical metabolites of primaquine. MetHb levels as high as 11% have been reported in healthy Caucasians treated with primaquine [80]. In individuals without anemia, primaquine-induced methaemoglobinaemia, however, is a well-tolerated condition that is alleviated upon the discontinuation of primaquine dosing [11].
Gastrointestinal (GI) discomfort has been associated with primaquine in a dose-dependent manner [80–82]. Symptoms include cramping, nausea, diarrhoea and vomiting. Most of these symptoms are mild and are often avoided, if primaquine is taken with food [80].
2.10 Primaquine Resistance
Experimentally induced primaquine resistance has been developed in P. berghei and P. knowlesi [83, 84]. These controlled experiments were later supported with field reports that indicated the existence of primaquine-tolerant P. vivax [85]. Several reports suggest resistance to standard antirelapse primaquine therapy; however, factors such as noncompliance with the 14-day treatment [12] or inadequate weight-based dose could also explain the observed failures rather than inherited resistance [86]. P. vivax strains from Southeast Asia and the Southwest Pacific are more tolerant to primaquine than elsewhere [19]. These tolerant strains, however, can be effectively treated with increased doses of primaquine [11]. Although little evidence exists to support primaquine-resistant exo-erythrocytic stages including hypnozoites, several reports have described multiple relapses of P. vivax in military personnel after primaquine treatment [87, 88]. Further well-controlled studies where treatment compliance is known and primaquine is administered in a weight-based dose would help resolve the resistance issue.
3 Tafenoquine
3.1 Historical Development
Originally labeled as WR238605 or SB-252263 and now named tafenoquine, the drug is a new 8-aminoquinoline antimalarial being codeveloped by GlaxoSmithKline Pharmaceuticals and the US Army as a replacement for primaquine for radical cure of P. vivax malaria and as a potential prophylactic agent [89–91]. In an effort to develop less toxic, more active and longer acting 8-aminoquinolines, tafenoquine was first synthesised by the US Army at the Walter Reed Army Institute of Research in 1979. Although tafenoquine is a primaquine analog, it possesses different physicochemical properties, antimalarial potency and toxicological and pharmacokinetic properties compared with primaquine. In in vitro testing and in vivo preclinical animal models tafenoquine is more active than primaquine. To date, it has been evaluated in more than 2,000 human subjects in clinical studies.
On an equimolar basis, in vitro antimalarial susceptibility studies have shown tafenoquine to exhibit equivalent activity (IC50 of 0.7–1.5 μM) to primaquine against culture-adapted chloroquine-sensitive strains, but was considerably more active than primaquine against multidrug-resistant P. falciparum lines, with IC50 values ranging from 0.06 to 0.3 μM [92]. It is conceivable that tafenoquine’s enhanced blood schizontocidal potency compared with primaquine is because it exerts greater oxidative stress on multidrug-resistant parasitised erythrocytes [93]. In contrast to culture-adapted multidrug-resistant P. falciparum lines, tafenoquine was only marginally more active than primaquine against wild isolates of P. falciparum from central, west and east Africa (mean IC50 values of 4.43 μM versus 6.82 μM) [94, 95]. The enantiomers of tafenoquine have similar levels of in vitro antimalarial activity against the drug-sensitive D6 and multidrug-resistant W2, TM90-C2a and TM90-C2b strains of P. falciparum (D. K. Kyle personal communication).
In the rodent–P. berghei Peters 4-day suppressive test, tafenoquine was about 9 times more active as a blood schizontocide than primaquine against the drug-sensitive P. berghei N strain and 4–5 times as active as primaquine against highly resistant chloroquine, mefloquine or halofantrine strains of P. berghei [95]. In addition to developing new schizontocidal drugs, the capacity to interrupt malaria transmission is also of great importance. Tafenoquine possesses significant sporontocidal activity against P. berghei, with a minimum effective dose of 25 mg/kg that prevents mosquitoes from developing sporozoites [96]. Tafenoquine also has gametocytocidal activity, with a significant reduction in the number of gametocytes in the blood of P. berghei-infected mice treated with 25 mg/kg, resulting in a twofold extension of mice survival time [90].
In the rhesus monkey–P. cynomolgi model, tafenoquine was effective as a causal prophylactic agent against pre-erythrocytic tissue stages of sporozoite-induced P. cynomolgi malaria [97]. The causal prophylactic ED50 (50% effective dose) of tafenoquine was 0.125 mg/kg/day or 0.27 μM/kg/day for 3 days, which was 14 times more effective than primaquine, with an ED50 of 1 mg/kg/day or 3.86 μM/kg/day for 3 days. Tafenoquine was also a highly effective agent against liver stages of P. cynomolgi, with an ED50 of 0.172 mg/kg/day or 0.371 μM/kg/day for 7 days and was 7 times more potent than primaquine, with an ED50 of 0.712 mg/kg/day or 2.75 μM/kg/day for 7 days [98].
Although developed primarily as an antirelapse agent, tafenoquine has also been found to possess significant blood schizontocidal activity against trophozoite-induced infections in simian–malaria models. Against P. cynomolgi B and P. fragile, which are recognised as biological counterparts of P. vivax and P. falciparum infections in humans, respectively [99], tafenoquine at a dose of 3.16 mg/kg/day for 7 days led to a cure for established trophozoite induced infections in monkeys with both these parasites [100]. In contrast, primaquine was only partially curative (25% for P. cynomolgi B and 67% for P. fragile) at a dose of 10 mg/kg/day for 7 days. Tafenoquine was also effective against blood-induced vivax malaria infections of the chloroquine-resistant AMRU1 strain in the Aotus monkey–P. vivax model. Parasite clearance of the AMRU1 strain occurred at a dose of 0.3 mg/kg tafenoquine daily for 3 days and cures were achieved at 3 mg/kg daily for 3 days [101].
In addition to tafenoquine’s greater in vitro and in vivo antimalarial activities compared with primaquine in preclinical studies, it is less toxic than primaquine. In acute oral toxicity studies, tafenoquine’s LD50 (50% lethal dose) of 0.78 and 0.64 mM/kg in rats and guinea pigs, respectively, was markedly less toxic than primaquine, with corresponding LD50 values of 0.46 and 0.12 mM/kg [98]. In subchronic and chronic studies of tafenoquine (WR 238605 IND #38503), the compound was also found to be less toxic than primaquine. For example, in dog toxicology studies, 3 and 9 mg/kg/day of primaquine orally for 28 days resulted in muscle necrosis, coma and death, whereas tafenoquine up to a maximum tested dose of 16 mg/kg/day for 28 days did not produce these adverse events [102].
3.2 Chemistry
The chemical name for the racemic tafenoquine is (±)-8-[(4-amino-1-methylbutyl)amino]-2,6-dimethoxy-4-methyl-5-(3-trifluoromethylphenoxy) quinoline succinate. The structural formula for tafenoquine is shown in Fig. 2. Its chemical formula is C24H28N3O3·C4H6O4, with molecular weights of 463 for the base and 581 for the succinate salt. Tafenoquine is an off-white to pink/orange/brown solid powder with a strong phenolic odor. It is poorly soluble in water and stable at room temperature, when stored in amber bottles for at least 10 years. The formulated product of tafenoquine is a hard gelatin capsule containing 250 mg tafenoquine succinate equivalent to 200 mg of the free base. Tafenoquine capsules should be stored below 30°C and protected from light.

Structure of Tafenoquine
3.3 Mechanism of Action and Development of Resistance
As already indicated, the exact mechanism of action of 8-aminoquinolines is not well understood. It has been proposed that the blood-stage activity of 8-aminoquinolines may be derived from an oxidative stress mechanism since it is known that primaquine stimulates the hexose monophosphate shunt, increases hydrogen peroxide and MetHb production and decreases glutathione levels in the erythrocyte [93, 103, 104]. Similar to chloroquine, the blood-stage activity of tafenoquine may be through inhibition of haematin polymerisation. In contrast to the inactive primaquine (IC50 > 2,500 μM), tafenoquine (IC50 of 16 μM) inhibited haematin polymerisation more efficiently than did chloroquine (IC50 of 80 μM) [92]. Other suggested modes of action of tafenoquine include drug-induced mitochondrial dysfunction or inhibition of receptor recycling by endosomes [105, 106].
In vitro studies have also shown a positive correlation between tafenoquine and primaquine (r 2 = 0.61) against seven P. falciparum lines, with different levels of susceptibility to chloroquine and mefloquine [92]. In contrast, no correlation exists between tafenoquine and either chloroquine or mefloquine, suggesting a lack of cross-resistance between tafenoquine and chloroquine or mefloquine.
3.4 Pharmacokinetics and Metabolism
The pharmacokinetics of tafenoquine has been investigated following both single and multiple oral administration of the drug in healthy subjects. Single-dose studies ranging from 4 to 600 mg tafenoquine have been carried out in 48 healthy males (Caucasian [n = 20], African American [n = 12] and Hispanic [n = 16]) in the fasting state [98]. The absorption half-life of tafenoquine was 1.7 h, suggesting rapid absorption of the compound. However, the t max of 13.8 h implied prolonged absorption of tafenoquine from the gut. Plasma tafenoquine concentrations declined in a mono-exponential manner and the drug was slowly cleared, with an elimination half-life of 14 days. The C max and area under the drug concentration curve of tafenoquine were linear over the doses studied. The tafenoquine concentration–time data were best described by a one-compartment model, with first-order absorption and elimination. Tafenoquine had a low oral clearance (CL/F, 5.7 L/h) and a large apparent volume of distribution (V/F, 2,558 L), suggesting extensive tissue binding. Whole blood concentrations of tafenoquine were 1.8-fold higher than corresponding plasma concentrations, reflecting an accumulation of the drug in erythrocytes, which may contribute to the greater potency of tafenoquine compared with primaquine, which does not concentrate in erythrocytes [61].
The population pharmacokinetics of tafenoquine has also been determined in healthy Thai and Australian soldiers after receiving tafenoquine for malaria prophylaxis. A one-compartment model with first-order absorption and elimination was found to best describe the population pharmacokinetics of tafenoquine. In the Thai study, 104 soldiers received a loading dose of 400 mg tafenoquine daily for 3 days followed by 400 mg tafenoquine monthly for 5 consecutive months [107]. Blood samples were randomly collected from each soldier on several occasions each month. The population estimates of the first-order absorption rate constant (K a), CL/F and V/F were 0.69/h, 3.20 L/h and 1,820 L, respectively. The absorption and elimination half-lives were 1.0 h and 16.4 days, respectively. The covariants, age and weight influenced the volume of distribution. The one subject who contracted malaria had a higher plasma clearance, but this was not considered to have sufficient impact to warrant a change in dosing.
In the Australian study, 490 soldiers received a loading dose of 200 mg tafenoquine daily for 3 days followed by a weekly dose of 200 mg tafenoquine for 6 months [108]. Blood samples were collected from each soldier after the last loading dose and then at weeks 4, 8 and 16. Typical values of K a, CL/F and V/F were 0.24/h, 4.37 L/h and 1,901 L, respectively. The V/F was similar to that reported in the Thai soldiers, but the systemic CL/F was greater (4.37 L/h versus 3.20 L/h). The derived elimination half-life of tafenoquine in the Australian soldiers of 12.7 days was slightly shorter than the 14 and 16 days reported previously in healthy Caucasians, African-Americans and Hispanic subjects [98] and in Thai soldiers [107], respectively, which may partly reflect the fact that the last samples were drawn at only up to 1 week post dose and therefore, the presumed “terminal” phase may have included some components of the distribution phase. The mean values for CL/F and V/F obtained in the fed Australian soldiers were 30–35% lower than values derived in the fasted healthy subjects participating in the single dose escalating study of tafenoquine. A possible explanation for the disparity is that a high-fat meal can increase the oral bioavailability (F) of tafenoquine by up to 40% (A. K. Miller personal communication), which when comparing the two studies would bring the respective CL/F and V/F values into closer agreement after correcting for F.
Limited investigations have been carried out on the metabolism of tafenoquine. In vitro rat liver microsomal studies have identified tafenoquine to be metabolised to aminophenolic compounds that undergo air oxidation to a mixture of quinones and quinoneimines [109]. Similar to primaquine, the metabolism of tafenoquine is difficult to study, because its structure contains several metabolically labile constituent groups, and its intermediates are unstable and possess amphoteric properties [74]. So far, no metabolites of tafenoquine have been identified in either human plasma or urine.
3.5 Safety and Tolerability
In single dose escalating pharmacokinetic studies in healthy subjects, only a few GI side effects such as heartburn, flatulence, vomiting and diarrhoea were seen in those subjects who received the higher doses of 300–600 mg tafenoquine [98]. These side effects were few and were not unexpected, based on past experiences with primaquine. Methaemoglobinaemia, haemolytic anaemia, thrombocytopenia, or changes in white blood cell counts or electrocardiograms were not observed in the subjects. Because tafenoquine is related to primaquine, it can cause methaemoglobinaemia and haemolytic anaemia in individuals with deficiency of G6PD. Thus, all individuals who receive an 8-aminoquinoline should undergo laboratory testing for confirmation of a normal G6PD status [110]. This is potentially tafenoquine’s major drawback for use worldwide as G6PD is one of the most common human genetic polymorphisms. Although malaria patients with anemia may be at greater risk, methaemoglobinaemia generally is not a serious concern when <20% of haemoglobin is in the MetHb form and only rarely will testing for methaemoglobinaemia be indicated on clinical grounds, such as the presence of bluish mucous membranes [111].
In individuals with severe G6PD deficiency, such as the Mediterranean variety, tafenoquine or primaquine should not be used. Even individuals with the low-grade deficiency (A-) variant of G6PD, which is most commonly found in Africa, can be at risk of developing haemolysis when exposed to tafenoquine. In a Kenyan field study, two women who were inadvertently given tafenoquine (400 mg daily for 3 days) experienced a haemolytic reaction when their G6PD deficiency status was incorrectly recorded during screening [112]. One woman, who was later found to be heterozygous for the (A-) G6PD variant, developed intravascular haemolysis and required a 2-unit blood transfusion. Haemolysis did not continue after the acute event, no renal compromise was seen in spite of blackwater urine, and she restored and maintained normal haematologic parameters for 6 months after the event. The other woman, who was later found to be homozygous for the (A-) G6PD variant, remained asymptomatic despite an acute 30 g/L decrease in haemoglobin, which was noticed only because of routine blood tests. She restored her haemoglobin level without intervention.
3.6 Clinical Use
3.6.1 Chemoprophylaxis against P. falciparum and P. vivax Malaria
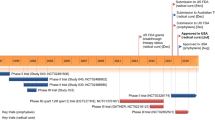
The development and spread of multiple drug-resistant P. falciparum malaria in many parts of the world highlights the need to develop new, safe, well-tolerated and effective chemoprophylactic agents for travellers and in special risk groups such as military personnel. A long-acting drug that acts on all stages of the malaria parasite could be a significant addition to the limited armamentarium for protecting individuals against malaria infections. Tafenoquine is a long-acting antimalarial and, based on preclinical studies acts on all stages of the parasite, including the pre-erythrocytic stages providing causal prophylactic activity. Table 1 summarises the Phase II and III studies on the safety, tolerability and protective efficacy of tafenoquine in its clinical development.
3.6.2 Presumptive Antirelapse Therapy and Radical Cure
Tafenoquine was also developed as a potential replacement of primaquine for presumptive antirelapse therapy and radical cure. Table 2 summarises the clinical development of tafenoquine for antirelapse therapy.
3.7 Future Potential
Tafenoquine is a unique antimalarial drug that is active against all stages of Plasmodium spp. Although clinical studies of tafenoquine have shown the long-acting 8-aminoquinoline to have comparable efficacy to primaquine for radical cure and presumptive antirelapse therapy, the markedly shorter regime of tafenoquine compared with primaquine (3 days versus 14 days) is more convenient and with improved compliance one could expect the number of relapses of P. vivax malaria to decrease markedly. For the treatment of uncomplicated P. falciparum, artemisinin-based combination therapies (ACTs) are now recommended for first-line treatment worldwide. Because of tafenoquine’s long elimination half-life of 14 days, it could be considered as a partner drug with an artemisinin derivative such as artesunate. Today, however, we have very efficacious and well-tolerated ACTs for the treatment of falciparum malaria [125]. Thus, it may be more prudent to limit the use of tafenoquine to treating P. vivax and P. ovale infections, and for selected applications, including prophylaxis (short and long-term) for special risk groups such as military personnel.
Furthermore, since tafenoquine possesses both gametocytocidal and sporontocidal activity it is a promising candidate agent for transmission-blocking public health applications. Because of its long half-life, tafenoquine has enormous potential for malaria control and possibly the elimination of the disease. To test this latter concept will be difficult. Perhaps tafenoquine could be evaluated for transmission blocking in an area of low endemicity, with controlled geographical access such as an island. For malaria elimination, tafenoquine could be used in mass drug administration to eliminate residual parasites in an entire population [112] and, thus, would be an excellent drug for the eradication of malaria under the new initiative by the Bill and Melinda Gates Foundation [126].
Before these possible public health applications of tafenoquine can be implemented, a regimen that can safely be given to G6PD-deficient individuals needs to be developed. Alternatively, a field friendly, rapid and inexpensive G6PD test needs to be produced so that the G6PD status of the individual can be ascertained prior to tafenoquine administration. A clinical dose-escalating study in G6PD-deficient subjects is planned to better quantify and characterise the risk of tafenoquine use in this important risk group [117].
References
Peters W (1999) The evolution of tafenoquine–antimalarial for a new millennium? J R Soc Med 92:345–352
Alving AS, Pullman TN et al (1948) The clinical trial of 18 analogues of pamaquin (plasmochin) in vivax malaria, Chesson strain. J Clin Invest 27:34–45
Arnold J, Alving AS, Hockwald RS, Clayman CB, Dern RJ, Beutler E, Flannagan OL, Jeffery GM (1955) The antimalarial action of primaquine against the blood and tissue stages of falciparum malaria (Panama, P-F-6 strain). J Lab Clin Med 46:391–397
Baird JK, Wiady I, Sutanihardja A, Suradi P, Basri H, Sekartuti AE, Fryauff DJ, Hoffman SL (2002) Short report: therapeutic efficacy of chloroquine combined with primaquine against Plasmodium falciparum in northeastern Papua, Indonesia. Am J Trop Med Hyg 66:659–660
Basco LK, Bickii J, Ringwald P (1999) In-vitro activity of primaquine against the asexual blood stages of Plasmodium falciparum. Ann Trop Med Parasitol 93:179–182
Edgecomb J, Arnold J, Yount E Jr, Alving A, Eichelberger L (1950) Primaquine, SN-13272, a new curative agent in vivax malaria: a preliminary report. Nat Malar Soc 9:285–357
Wilairatana P, Silachamroon U, Krudsood S, Singhasivanon P, Treeprasertsuk S, Bussaratid V, Phumratanaprapin W, Srivilirit S, Looareesuwan S (1999) Efficacy of primaquine regimens for primaquine-resistant Plasmodium vivax malaria in Thailand. Am J Trop Med Hyg 61:973–977
Pukrittayakamee S, Vanijanonta S, Chantra A, Clemens R, White NJ (1994) Blood stage antimalarial efficacy of primaquine in Plasmodium vivax malaria. J Infect Dis 169:932–935
Powell RD, Brewer GJ (1967) Effects of pyrimethamine, chlorguanide, and primaquine against exoerythrocytic forms of a strain of chloroquine-resistant Plasmodium falciparum from Thailand. Am J Trop Med Hyg 16:693–698
Arnold J, Alving AS, Hockwald RS, Clayman CB, Dern RJ, Beutler E, Jeffery GM (1954) The effect of continuous and intermittent primaquine therapy on the relapse rate of Chesson strain vivax malaria. J Lab Clin Med 44:429–438
Hill DR, Baird JK, Parise ME, Lewis LS, Ryan ET, Magill AJ (2006) Primaquine: report from CDC expert meeting on malaria chemoprophylaxis I. Am J Trop Med Hyg 75:402–415
Baird JK, Hoffman SL (2004) Primaquine therapy for malaria. Clin Infect Dis 39:1336–1345
Fryauff D, Baird J, Basri H, Sumawinata I, Purnomo RT, Ohrt C, Mouzin E, Church C, Richards A et al (1995) Randomised placebo-controlled trial of primaquine for prophalaxis of falciparum and vivax malaria. Lancet 346:1190–1193
Baird JK, Lacy MD, Basri H, Barcus MJ, Maguire JD, Bangs MJ, Gramzinski R, Sismadi P, Krisin LJ et al (2001) Randomized, parallel placebo-controlled trial of primaquine for malaria prophylaxis in Papua, Indonesia. Clin Infect Dis 33:1990–1997
Baird JK, Fryauff DJ, Basri H, Bangs MJ, Subianto B, Wiady I, Purnomo LB, Masbar S, Richie TL et al (1995) Primaquine for prophylaxis against malaria among nonimmune transmigrants in Irian Jaya, Indonesia. Am J Trop Med Hyg 52:479–484
Soto J, Toledo J, Rodriquez M, Sanchez J, Herrera R, Padilla J, Berman J (1998) Primaquine prophylaxis against malaria in nonimmune Colombian soldiers: efficacy and toxicity. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 129:241–244
Alving AS, Arnold J, Robinson DH (1952) Mass therapy of subclinical vivax malaria with primaquine. JAMA 149:1558
Jelinek T, Nothdurft HD, Von Sonnenburg F, Loscher T (1995) Long-term efficacy of primaquine in the treatment of vivax malaria in nonimmune travelers. Am J Trop Med Hyg 52:322–324
Baird JK, Rieckmann KH (2003) Can primaquine therapy for vivax malaria be improved? Trends Parasitol 19:115–120
Schwartz E, Regev-Yochay G, Kurnik D (2000) Short report: a consideration of primaquine dose adjustment for radical cure of Plasmodium vivax malaria. Am J Trop Med Hyg 62:393–395
Duarte EC, Pang LW, Ribeiro LC, Fontes CJ (2001) Association of subtherapeutic dosages of a standard drug regimen with failures in preventing relapses of vivax malaria. Am J Trop Med Hyg 65:471–476
Clyde DF, McCarthy VC (1977) Radical cure of Chesson strain vivax malaria in man by 7, not 14, days of treatment with primaquine. Am J Trop Med Hyg 26:562–563
Goller JL, Jolley D, Ringwald P, Biggs BA (2007) Regional differences in the response of Plasmodium vivax malaria to primaquine as anti-relapse therapy. Am J Trop Med Hyg 76:203–207
Dao NV, Cuong BT, Ngoa ND, le Thuy TT, The ND, Duy DN, Dai B, Thanh NX, Chavchich M, Rieckmann KH et al (2007) Vivax malaria: preliminary observations following a shorter course of treatment with artesunate plus primaquine. Trans R Soc Trop Med Hyg 101:534–539
Pukrittayakamee S, Imwong M, Chotivanich K, Singhasivanon P, Day NP, White NJ (2010) A comparison of two short-course primaquine regimens for the treatment and radical cure of Plasmodium vivax malaria in Thailand. Am J Trop Med Hyg 82:542–547
Krudsood S, Tangpukdee N, Wilairatana P, Phophak N, Baird JK, Brittenham GM, Looareesuwan S (2008) High-dose primaquine regimens against relapse of Plasmodium vivax malaria. Am J Trop Med Hyg 78:736–740
Alving AS et al (1955) Potentialtion of the curative action of primaquine in vivax malaria by quinine and chloroquine. J Lab Clin Med 46:301–306
Bray PG, Deed S, Fox E, Kalkanidis M, Mungthin M, Deady LW, Tilley L (2005) Primaquine synergises the activity of chloroquine against chloroquine-resistant P. falciparum. Biochem Pharmacol 70:1158–1166
Galappaththy GN, Omari AA, Tharyan P (2007) Primaquine for preventing relapses in people with Plasmodium vivax malaria. Cochrane Database Syst Rev CD004389
Silachamroon U, Krudsood S, Treeprasertsuk S, Wilairatana P, Chalearmrult K, Mint HY, Maneekan P, White NJ, Gourdeuk VR, Brittenham GM et al (2003) Clinical trial of oral artesunate with or without high-dose primaquine for the treatment of vivax malaria in Thailand. Am J Trop Med Hyg 69:14–18
Rieckmann KH, McNamara JV, Frischer H, Stockert TA, Carson PE, Powell RD (1968) Gametocytocidal and sporontocidal effects of primaquine and of sulfadiazine with pyrimethamine in a chloroquine-resistant strain of Plasmodium falciparum. Bull World Health Organ 38:625–632
Pukrittayakamee S, Chotivanich K, Chantra A, Clemens R, Looareesuwan S, White NJ (2004) Activities of artesunate and primaquine against asexual- and sexual-stage parasites in falciparum malaria. Antimicrob Agents Chemother 48:1329–1334
Lederman ER, Maguire JD, Sumawinata IW, Chand K, Elyazar I, Estiana L, Sismadi P, Bangs MJ, Baird JK (2006) Combined chloroquine, sulfadoxine/pyrimethamine and primaquine against Plasmodium falciparum in Central Java, Indonesia. Malar J 5:108
Shekalaghe S, Drakeley C, Gosling R, Ndaro A, van Meegeren M, Enevold A, Alifrangis M, Mosha F, Sauerwein R, Bousema T (2007) Primaquine clears submicroscopic Plasmodium falciparum gametocytes that persist after treatment with sulphadoxine-pyrimethamine and artesunate. PLoS One 2:e1023
El-Sayed B, El-Zaki SE, Babiker H, Gadalla N, Ageep T, Mansour F, Baraka O, Milligan P, Babiker A (2007) A randomized open-label trial of artesunate- sulfadoxine-pyrimethamine with or without primaquine for elimination of sub-microscopic P. falciparum parasitaemia and gametocyte carriage in eastern Sudan. PLoS One 2:e1311
Suputtamongkol Y, Chindarat S, Silpasakorn S, Chaikachonpatd S, Lim K, Chanthapakajee K, Kaewkaukul N, Thamlikitkul V (2003) The efficacy of combined mefloquine-artesunate versus mefloquine-primaquine on subsequent development of Plasmodium falciparum gametocytemia. Am J Trop Med Hyg 68:620–623
Kumar N, Zheng H (1990) Stage-specific gametocytocidal effect in vitro of the antimalaria drug qinghaosu on Plasmodium falciparum. Parasitol Res 76:214–218
Dunyo S, Milligan P, Edwards T, Sutherland C, Targett G, Pinder M (2006) Gametocytaemia after drug treatment of asymptomatic Plasmodium falciparum. PLoS Clin Trials 1:e20
White NJ (2008) The role of anti-malarial drugs in eliminating malaria. Malar J 7(Suppl 1):S8
Lanners HN (1991) Effect of the 8-aminoquinoline primaquine on culture-derived gametocytes of the malaria parasite Plasmodium falciparum. Parasitol Res 77:478–481
Beaudoin RL, Aikawa M (1968) Primaquine-induced changes in morphology of exoerythrocytic stages of malaria. Science 160:1233–1234
Boulard Y, Landau I, Miltgen F, Ellis DS, Peters W (1983) The chemotherapy of rodent malaria. XXXIV. Causal prophylaxis Part III: Ultrastructural changes induced in exo-erythrocytic schizonts of Plasmodium yoelii yoelii by primaquine. Ann Trop Med Parasitol 77:555–568
Howells RE, Pters W, Fullard J (1970) The chemotherapy of rodent malaria. 13. Fine structural changes observed in the eryhrocytic stages of Plasmodium berghei berghei following exposureto primaquine and menoctone. Ann Trop Med Parasitol 64:203–207
Aikawa M, Beaudoin RL (1970) Plasmodium fallax: high-resolution autoradiography of exoerythrocytic stages treated with Primaquine in vitro. Exp Parasitol 27:454–463
Peters W, Ellis D, Boulard Y, Landau I (1984) The chemotherapy of rodent malaria XXXVI. Part IV. The activity of a new 8-aminoquinoline, WR 225,448 against exo-erythrocytic schizonts of Plasmodium yoelii yoelii. Ann Trop Med Parasitol 78:467–478
Rotman A (1975) Genetics of a primaquin-resistant yeast. J Gen Microbiol 89:1–10
Krungkrai J, Burat D, Kudan S, Krungkrai S, Prapunwattana P (1999) Mitochondrial oxygen consumption in asexual and sexual blood stages of the human malarial parasite, Plasmodium falciparum. Southeast Asian J Trop Med Public Health 30:636–642
Idowu OR, Peggins JO, Brewer TG (1995) Side-chain hydroxylation in the metabolism of 8-aminoquinoline antiparasitic agents. Drug Metab Dispos 23:18–27
Vale N, Moreira R, Gomes P (2009) Primaquine revisited six decades after its discovery. Eur J Med Chem 44:937–953
Grewal RS (1981) Pharmacology of 8-aminoquinolines. Bull World Health Organ 59:397–406
Fry M, Pudney M (1992) Site of action of the antimalarial hydroxynaphthoquinone, 2-[trans-4-(4′-chlorophenyl) cyclohexyl]-3-hydroxy-1,4-naphthoquinone (566 C80). Biochem Pharmacol 43:1545–1553
Fry M, Beesley JE (1991) Mitochondria of mammalian Plasmodium spp. Parasitology 102:17–26
Srivastava IK, Rottenberg H, Vaidya AB (1997) Atovaquone, a broad spectrum antiparasitic drug, collapses mitochondrial membrane potential in a malarial parasite. J Biol Chem 272:3961–3966
Painter HJ, Morrisey JM, Mather MW, Vaidya AB (2007) Specific role of mitochondrial electron transport in blood-stage Plasmodium falciparum. Nature 446:88–91
Vaidya AB, Lashgari MS, Pologe LG, Morrisey J (1993) Structural features of Plasmodium cytochrome b that may underlie susceptibility to 8-aminoquinolines and hydroxynaphthoquinones. Mol Biochem Parasitol 58:33–42
Fletcher KA, Barton PF, Kelly JA (1988) Studies on the mechanisms of oxidation in the erythrocyte by metabolites of primaquine. Biochem Pharmacol 37:2683–2690
Greenberg J, Taylor DJ, Josephson ES (1951) Studies on Plasmodium gallinaceum in vitro II. The effects of some 8-aminoquinolines against the erythrocytic parasites. J Infect Dis 88:163–167
Meshnick SR (1998) Artemisinin antimalarials: mechanisms of action and resistance. Med Trop 58:13–17
McChesney JD (1981) Considerations about the structure-activity relationships of 8- aminoquinoline antimalarial drugs. Bull World Health Organ 59:459–462
Peters W, Irare SG, Ellis DS, Warhurst DC, Robinson BL (1984) The chemotherapy of rodent malaria, XXXVIII. Studies on the activity of three new antimalarials (WR 194,965, WR 228,258 and WR 225,448) against rodent and human malaria parasites (Plasmodium berghei and P. falciparum). Ann Trop Med Parasitol 78:567–579
Mihaly GW, Ward SA, Edwards G, Nicholl DD, Orme ML, Breckenridge AM (1985) Pharmacokinetics of primaquine in man. I. Studies of the absolute bioavailability and effects of dose size. Br J Clin Pharmacol 19:745–750
Ward SA, Mihaly GW, Edwards G, Looareesuwan S, Phillips RE, Chanthavanich P, Warrell DA, Orme ML, Breckenridge AM (1985) Pharmacokinetics of primaquine in man. II. Comparison of acute vs chronic dosage in Thai subjects. Br J Clin Pharmacol 19:751–755
Bangchang KN, Songsaeng W, Thanavibul A, Choroenlarp P, Karbwang J (1994) Pharmacokinetics of primaquine in G6PD deficient and G6PD normal patients with vivax malaria. Trans R Soc Trop Med Hyg 88:220–222
Binh VQ, Chinh NT, Thanh NX, Cuong BT, Quang NN, Dai B, Travers T, Edstein MD (2009) Sex affects the steady-state pharmacokinetics of primaquine but not doxycycline in healthy subjects. Am J Trop Med Hyg 81:747–753
Mihaly GW, Ward SA, Edwards G, Orme ML, Breckenridge AM (1984) Pharmacokinetics of primaquine in man: identification of the carboxylic acid derivative as a major plasma metabolite. Br J Clin Pharmacol 17:441–446
Greaves J, Evans DA, Gilles HM, Fletcher KA, Bunnag D, Harinasuta T (1980) Plasma kinetics and urinary excretion of primaquine in man. Br J Clin Pharmacol 10:399–404
Mayorga P, Deharo E, Landau I, Couarraze G (1997) Preliminary evaluation of primaquine activity on rodent malaria model after transdermal administration. Parasite 4:87–90
Nishi KK, Jayakrishnan A (2007) Self-gelling primaquine-gum arabic conjugate: an injectable controlled delivery system for primaquine. Biomacromolecules 8:84–90
Singh KK, Vingkar SK (2008) Formulation, antimalarial activity and biodistribution of oral lipid nanoemulsion of primaquine. Int J Pharm 347:136–143
Stensrud G, Sande SA, Kristensen S, Smistad G (2000) Formulation and characterisation of primaquine loaded liposomes prepared by a pH gradient using experimental design. Int J Pharm 198:213–228
Vangapandu S, Sachdeva S, Jain M, Singh S, Singh PP, Kaul CL, Jain R (2004) 8-Quinolinamines conjugated with amino acids are exhibiting potent blood-schizontocidal antimalarial activities. Bioorg Med Chem 12:239–247
Rajic Z, Kos G, Zorc B, Singh PP, Singh S (2009) Macromolecular prodrugs. XII. Primaquine conjugates: synthesis and preliminary antimalarial evaluation. Acta Pharm 59:107–115
Borissova R, Lammek B, Stjarnkvist P, Sjoholm I (1995) Biodegradable microspheres. 16. Synthesis of primaquine-peptide spacers for lysosomal release from starch microparticles. J Pharm Sci 84:249–255
Brueckner RP, Ohrt C, Baird JK, Milhous WK (2001) 8-aminoquinolines. In: RP J (eds) Antimalarial chemotherapy: mechanisms of action, resistance and new directions. Humana, Totowa, NJ, pp 123–151
Cappellini MD, Fiorelli G (2008) Glucose-6-phosphate dehydrogenase deficiency. Lancet 371:64–74
Beutler E, Duparc S (2007) Glucose-6-phosphate dehydrogenase deficiency and antimalarial drug development. Am J Trop Med Hyg 77:779–789
Beutler E, Dern RJ, Alving AS (1955) The hemolytic effect of primaquine. VI. An in vitro test for sensitivity of erythrocytes to primaquine. J Lab Clin Med 45:40–50
Beutler E, Dern RJ, Flanagan CL, Alving AS (1955) The hemolytic effect of primaquine. VII. Biochemical studies of drug-sensitive erythrocytes. J Lab Clin Med 45:286–295
Srivastava P, Singh S, Jain GK, Puri SK, Pandey VC (2000) A simple and rapid evaluation of methemoglobin toxicity of 8-aminoquinolines and related compounds. Ecotoxicol Environ Saf 45:236–239
Clayman C, Arnold J, Hockwald R, Yount E Jr, Edgecomb J, Alving A (1952) Toxicity of primaquine in Caucasians. JAMA 149:1563–1568
Clyde DF (1981) Clinical problems associated with the use of primaquine as a tissue schizontocidal and gametocytocidal drug. Bull World Health Organ 59:391–395
Taylor WR, White NJ (2004) Antimalarial drug toxicity: a review. Drug Saf 27:25–61
Prakash S, Chakrabarti AK, Choudhury DS (1961) Studies on Plasmodium berghei Vincke and Lips, 1948. XXXI. Selection of a primaquine resistant strain. Indian J Malariol 15:115–122
Peters W (1966) Drug responses of mepacrine- and primaquine-resistant strains of Plasmodium berghei Vincke and Lips, 1948. Ann Trop Med Parasitol 60:25–30
Arnold J, Alvinig AS, Clayman CB (1961) Induced primaquine resistance in vivax malaria. Trans R Soc Trop Med Hyg 55:345–350
Baird JK (2007) A rare glimpse at the efficacy of primaquine. Am J Trop Med Hyg 76:201–202
Kitchener S (2002) Malaria in the Australian Defence Force associated with the InterFET peacekeeping operation in East Timor. Mil Med 167:iii–iv
Spudick JM, Garcia LS, Graham DM, Haake DA (2005) Diagnostic and therapeutic pitfalls associated with primaquine-tolerant Plasmodium vivax. J Clin Microbiol 43:978–981
Crockett M, Kain KC (2007) Tafenoquine: a promising new antimalarial agent. Expert Opin Investig Drugs 16:705–715
The GlaxoSmithKline (GSK) Clinical Study Register. http://www.gsk-clinicalstudyregister.com. Accessed 23 Apr 2010
Medicines for Malaria Venture Project Portfolio. http://www.mmv.org/research-development/project-portfolio/tafenoquine. Accessed 23 Apr 2010
Vennerstrom JL, Nuzum EO, Miller RE, Dorn A, Gerena L, Dande PA, Ellis WY, Ridley RG, Milhous WK (1999) 8-aminoquinolines active against blood stage Plasmodium falciparum in vitro inhibit hematin polymerization [In Process Citation]. Antimicrob Agents Chemother 43:598–602
Vennerstrom JL, Eaton JW (1988) Oxidants, oxidant drugs, and malaria. J Med Chem 31:1269–1277
Pradines B, Mamfoumbi MM, Tall A, Sokhna C, Koeck JL, Fusai T, Mosnier J, Czarnecki E, Spiegel A, Trape JF et al (2006) In vitro activity of tafenoquine against the asexual blood stages of Plasmodium falciparum isolates from Gabon, Senegal, and Djibouti. Antimicrob Agents Chemother 50:3225–3226
Peters W, Robinson BL, Milhous WK (1993) The chemotherapy of rodent malaria. LI. Studies on a new 8-aminoquinoline, WR 238,605. Ann Trop Med Parasitol 87:547–552
Coleman RE, Clavin AM, Milhous WK (1992) Gametocytocidal and sporontocidal activity of antimalarials against Plasmodium berghei ANKA in ICR Mice and Anopheles stephensi mosquitoes. Am J Trop Med Hyg 46:169–182
Heisy GE, Milhous WK, Hansuklarita P, Theoharides AD, Schuster BG, Davidson DE (1988) Radical curative properties of Tafenoquine (WR 238605, SB252263), Abstr. No. 323. The American Society of Tropical Medicine and Hygiene, Washington DC, p 217
Brueckner RP, Lasseter KC, Lin ET, Schuster BG (1998) First-time-in-humans safety and pharmacokinetics of WR 238605, a new antimalarial. Am J Trop Med Hyg 58:645–649
Coatney GE, Collins WE, Warren M, Contacos PG (1971) Primate malarias. Department of Health and Welfare, US Govt Publication, Washington, DC
Puri SK, Dutta GP (2003) Blood schizontocidal activity of WR 238605 (Tafenoquine) against Plasmodium cynomolgi and Plasmodium fragile infections in rhesus monkeys. Acta Trop 86:35–40
Obaldia N 3rd, Rossan RN, Cooper RD, Kyle DE, Nuzum EO, Rieckmann KH, Shanks GD (1997) WR 238605, chloroquine, and their combinations as blood schizonticides against a chloroquine-resistant strain of Plasmodium vivax in Aotus monkeys. Am J Trop Med Hyg 56:508–510
Lee CC, Kinter LD, Heiffer MH (1981) Subacute toxicity of primaquine in dogs, monkeys, and rats. Bull World Health Organ 59:439–448
Augusto O, Weingrill CL, Schreier S, Amemiya H (1986) Hydroxyl radical formation as a result of the interaction between primaquine and reduced pyridine nucleotides. Catalysis by hemoglobin and microsomes. Arch Biochem Biophys 244:147–155
Baird JK, Davidson DJ, Decker JJ (1986) Oxidative activity of hydroxylated primaquine analogs. Non-toxicity to glucose-6-phosphate dehydrogenase-deficient human red blood cells in vitro. Biochem Pharmacol 35:1091–1098
Hiebsch RR, Raub TJ, Wattenberg BW (1991) Primaquine blocks transport by inhibiting the formation of functional transport vesicles. Studies in a cell-free assay of protein transport through the Golgi apparatus. J Biol Chem 266:20323–20328
van Weert AW, Geuze HJ, Groothuis B, Stoorvogel W (2000) Primaquine interferes with membrane recycling from endosomes to the plasma membrane through a direct interaction with endosomes which does not involve neutralisation of endosomal pH nor osmotic swelling of endosomes. Eur J Cell Biol 79:394–399
Edstein MD, Kocisko DA, Brewer TG, Walsh DS, Eamsila C, Charles BG (2001) Population pharmacokinetics of the new antimalarial agent tafenoquine in Thai soldiers. Br J Clin Pharmacol 52:663–670
Charles BG, Miller AK, Nasveld PE, Reid MG, Harris IE, Edstein MD (2007) Population pharmacokinetics of tafenoquine during malaria prophylaxis in healthy subjects. Antimicrob Agents Chemother 51:2709–2715
Idowu OR, Peggins JO, Brewer TG, Kelley C (1995) Metabolism of a candidate 8-aminoquinoline antimalarial agent, WR 238605, by rat liver microsomes. Drug Metab Dispos 23:1–17
Lell B, Faucher JF, Missinou MA, Borrmann S, Dangelmaier O, Horton J, Kremsner PG (2000) Malaria chemoprophylaxis with tafenoquine: a randomised study. Lancet 355:2041–2045
Shanks GD, Kain KC, Keystone JS (2001) Malaria chemoprophylaxis in the age of drug resistance. II. Drugs that may be available in the future. Clin Infect Dis 33:381–385
Shanks GD, Oloo AJ, Aleman GM, Ohrt C, Klotz FW, Braitman D, Horton J, Brueckner R (2001) A new primaquine analogue, tafenoquine (WR 238605), for prophylaxis against Plasmodium falciparum malaria. Clin Infect Dis 33:1968–1974
Brueckner RP, Coster T, Wesche DL, Shmuklarsky M, Schuster BG (1998) Prophylaxis of Plasmodium falciparum infection in a human challenge model with WR 238605, a new 8-aminoquinoline antimalarial. Antimicrob Agents Chemother 42:1293–1294
Hale BR, Owusu-Agyei S, Fryauff DJ, Koram KA, Adjuik M, Oduro AR, Prescott WR, Baird JK, Nkrumah F, Ritchie TL et al (2003) A randomized, double-blind, placebo-controlled, dose-ranging trial of tafenoquine for weekly prophylaxis against Plasmodium falciparum. Clin Infect Dis 36:541–549
Walsh SD, Eamsila C, Sasiprapha T, Sangkharomya S, Khaewsathien P, Supakalin P, Tang DB, Jarasrumgsichol P, Chuenchitra SC, Edstein MD, et al (2004) Randomized, double-blind, placebo controlled evaluation of monthly tafenoquine (WR 238605) for Plasmodium falciparum and P. vivax malaria in Royal Thai Army soldiers. J Inf Dis 190:1456-1463
Nasveld PE, Edstein MD, Reid M, Brennan L, Harris IE, Kitchener SJ, Leggat PA, Pickford P, Kerr C, Ohrt C et al (2010) Randomized, double-blind study of the safety, tolerability, and efficacy of tafenoquine versus mefloquine for malaria prophylaxis in nonimmune subjects. Antimicrob Agents Chemother 54:792–798
Leary KJ, Riel MA, Roy MJ, Cantilena LR, Bi D, Brater DC, van de Pol C, Pruett K, Kerr C, Veazey JM Jr et al (2009) A randomized, double-blind, safety and tolerability study to assess the ophthalmic and renal effects of tafenoquine 200 mg weekly versus placebo for 6 months in healthy volunteers. Am J Trop Med Hyg 81:356–362
Nasveld P, Kitchener S, Edstein M, Rieckmann K (2002) Comparison of tafenoquine (WR238605) and primaquine in the post-exposure (terminal) prophylaxis of vivax malaria in Australian Defence Force personnel. Trans R Soc Trop Med Hyg 96:683–684
Elmes NJ, Nasveld PE, Kitchener SJ, Kocisko DA, Edstein MD (2008) Comparison of three different dose regimens of tafenoquine versus primaquine for post exposure prophylaxis of vivax malaria in the South West Pacific. Trans Roy Soc Trop Med Hyg 102:1095–1101
Edstein MD, Nasveld PE, Kocisko DA, Kitchener SJ, Gatton ML, Rieckmann KH (2007) Gender differences in gastrointestinal disturbances and plasma concentrations of tafenoquine in healthy volunteers after tafenoquine administration for post-exposure vivax malaria prophylaxis. Trans R Soc Trop Med Hyg 101:226–230
Walsh DS, Looareesuwan S, Wilairatana P, Heppner DG Jr, Tang DB, Brewer TG, Chokejindachai W, Viriyavejakul P, Kyle DE, Milhous WK et al (1999) Randomized dose-ranging study of the safety and efficacy of WR 238605 (Tafenoquine) in the prevention of relapse of Plasmodium vivax malaria in Thailand. J Infect Dis 180:1282–1287
Walsh DS, Wilairatana P, Tang DB, Heppner DG Jr, Brewer TG, Krudsood S, Silachamroon U, Phumratanaprapin W, Siriyanonda D, Looareesuwan S (2004) Randomized trial of 3-dose regimens of tafenoquine (WR238605) versus low-dose primaquine for preventing Plasmodium vivax malaria relapse. Clin Infect Dis 39:1095–1103
Nasveld P, Kitchener S (2005) Treatment of acute vivax malaria with tafenoquine. Trans R Soc Trop Med Hyg 99:2–5
Kitchener S, Nasveld P, Edstein MD (2007) Tafenoquine for the treatment of recurrent Plasmodium vivax malaria. Am J Trop Med Hyg 76:494–496
Nosten F, White NJ (2007) Artemisinin-based combination treatment of falciparum malaria. Am J Trop Med Hyg 77:181–192
Roberts L, Enserink M (2007) Malaria. Did they really say … eradication? Science 318:1544–1545
Acknowledgments
We thank Professor Dennis Shanks for review and helpful discussions with the manuscript. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official, or as reflecting true views of the United States Department of the Army, the Department of Defense or the Australian Defense Force.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer Basel AG
About this chapter
Cite this chapter
Waters, N.C., Edstein, M.D. (2011). 8-Aminoquinolines: Primaquine and Tafenoquine. In: Staines, H., Krishna, S. (eds) Treatment and Prevention of Malaria. Milestones in Drug Therapy. Springer, Basel. https://doi.org/10.1007/978-3-0346-0480-2_4
Download citation
DOI: https://doi.org/10.1007/978-3-0346-0480-2_4
Published:
Publisher Name: Springer, Basel
Print ISBN: 978-3-0346-0479-6
Online ISBN: 978-3-0346-0480-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)