
Abstract
In this chapter, we highlight how recent advances in influenza epidemiology can inform strategies for disease control. Given the challenge of direct measurement, influenza epidemiology has benefited greatly from statistical inference from the analysis of large datasets regarding hospitalization, mortality, and outpatient visits associated with seasonal circulation of influenza viruses. These data have allowed comparison of the impact of influenza in various climates and the evaluation of the direct and indirect benefits of vaccination, the latter through the vaccination of “transmitter populations” such as school children, to achieve herd immunity. Moreover, the resolution of influenza epidemiology has undergone a leap to the molecular level due to the integration of new antigenic and viral genomic data with classical epidemiological indicators. Finally, the new data have led to an infusion of quantitative studies from the fields of evolutionary biology, population genetics, and mathematics. Molecular influenza epidemiology is providing deeper insight into temporal/spatial patterns of viruses, the important role of reassortment in generating genetic novelty, and global diffusion of virus variants – including the role of the tropics, as a source of new variants. Higher resolution, contemporary, and historic epidemiological data provide a more detailed picture of the effect of age and other host characteristics on outcomes, as well as better estimates of the transmissibility of pandemic and seasonal influenza viruses. New epidemiologic and virologic data from the current A/H1N1pdm 2009 pandemic improve our understanding of the emergence and establishment of new viral subtypes in human populations and their mortality and morbidity burden in the first years of circulation. Re-examination of observational studies of vaccine effectiveness in seniors is leading to reconsideration of seasonal and pandemic vaccine priorities, while mathematical modelers have developed tools to explore optimal strategies for mitigating on-going and future pandemics. The field of influenza epidemiology has rapidly progressed in the past decade and become truly multidisciplinary. Progress could be sustained in the next decade by further interdisciplinary studies between virology, evolutionary biology, immunology, and clinical outcomes.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Influenza Virus
- Respiratory Syncytial Virus
- Influenza Vaccine
- Syndromic Surveillance
- Secondary Bacterial Infection
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Influenza viruses evolve continuously, challenging mammalian and avian hosts with new variants and causing complex epidemic patterns with regard to age, place, and time. Human influenza viruses cause disease through a variety of direct and indirect pathological effects. The direct effects include destruction of infected cells, damage to respiratory epithelium, and immunological responses that cause general malaise and pneumonia. Indirect consequences of infection include secondary bacterial infections as a result of tissue damage and exacerbation of underlying comorbid conditions such as cardiovascular disease, renal disease, diabetes, or chronic pulmonary disease [1, 2]. Given the lack of the conduct of laboratory tests, the morbidity and mortality associated with influenza is frequently classified into broad disease categories, such as pneumonia and influenza (P&I), respiratory illness, or all-cause (AC) mortality determined through statistical inference, based on seasonal coincidence of virus circulation and disease outcomes [3–5].
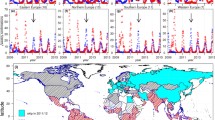
Given the difficulty of directly measuring influenza morbidity and mortality, time series models have been developed to elucidate patterns of disease within various age groups and populations [5–13]. Such models allow for quantification of disease burden by season and severity of circulating strains [9]. Historical data have also elucidated the links between influenza transmission across geographic regions and population movements [14] and allowed comparison of the impact and transmissibility of past pandemics and epidemics in multiple countries [15–24]. Similar models applied to prospective syndromic surveillance data have allowed the study of the epidemiological signature of recurring and reemerging strains of influenza on populations [25]. Mathematical modeling and statistical analyses of influenza activity in tropical countries have rekindled interest into the seasonal drivers of influenza and offered new insights into the circulation patterns of this virus at the global and regional scales [26–28] (Fig. 1).

Comparison of influenza virus seasonal patterns in temperate and tropical countries in the Americas. Pie charts represent the percent distribution of influenza virus isolation by month as compiled from WHO data between 1997 and 2005 (color bar). Note the transition in seasonal patterns from north to south. The latitude of the capital city is indicated for each country in the legend. Adapted from Viboud et al. [27]
The field of influenza epidemiology has recently undergone a quantum leap in resolution due to the increased availability of antigenic and viral genomic data and the integration of these data with classical epidemiological indicators [29–32]. The emerging field of molecular influenza epidemiology and evolution, or “phylodynamics” [29], has provided a much clearer picture of the complex dynamics of global influenza virus circulation and reassortment patterns. The growing number of available influenza genome sequences from specimens collected around the world has started to create a more coherent picture of the global epidemiology of influenza, in particular the interplay between virus evolution, population immunity, and impact.
We highlight how influenza epidemiology through statistical inference tools has helped refine existing strategies for influenza control. We begin by examining the spatial and temporal spread of seasonal influenza, and how old and new analytical tools are reshaping quantitative thinking in influenza epidemiology and control. We examine historical patterns of disease observed during the three pandemics of the twentieth century and discuss the epidemiology of the recent avian A/H5N1 influenza threat and the current A/H1N1pdm 2009 pandemic. We review what is known about the impact of vaccine in older age groups – the group with the greatest influenza-related mortality burden – and a discussion of the implications of influenza epidemiology for pandemic planning. We conclude with a short discussion of the epidemiology of “H1N1pdm,” the virus behind the current pandemic. Readers looking for a more comprehensive treatment of the vast field of influenza epidemiology may consider supplementing this chapter with some of the classical reviews published over the last decades [2, 33–37].
2 Seasonal Influenza: New Insights
The disease burden of annual influenza epidemics varies greatly in terms of hospitalizations and deaths. In the USA, clinical illness affects 5–20% of the population and asymptomatically infects a larger number [36]. Infants, who are exposed to influenza epidemics as a novel antigenic challenge after maternal antibodies decline, may have attack rates as high as 30–50% in their first year of life, depending on the frequency of contacts with older siblings [38]. For reasons not fully understood, influenza viruses cause seasonal epidemics in the northern and southern hemisphere during their respective winters. In the tropics, the timing of activity is less defined, with sometimes year-round circulation or bi-seasonal peaks during the year (Fig. 1) [27, 28, 39–42].
2.1 Methods Used to Estimate the Mortality Burden of Influenza
Estimates of the number of influenza-related deaths are typically inferred through statistical analysis. The syndromic diagnosis “influenza-like illness” is rarely laboratory confirmed and is often caused by non-influenza respiratory viruses. Moreover, influenza may be an inciting factor that brings about death from secondary bacterial pneumonia or an underlying chronic disorder. In these cases, the secondary infection or underlying disorders are typically identified as the cause of death which may occur weeks after the initial viral infection. Because of these ascertainment problems, determining the magnitude of influenza-related deaths requires indirect approaches in which mathematical or statistical models are applied to broad death categories. This approach was first used in 1847 by William Farr to characterize an influenza epidemic in London and was further developed and extensively used throughout the twentieth century. The refinements include Serfling-like cyclical regression models [6, 12, 18, 21, 43–46] and Arima models [7, 8, 47, 48], which are applied to monthly or weekly time series of P&I or AC mortality. Overall, investigators from at least 17 countries have used variants of these Serfling-type models to estimate the mortality burden of influenza. Similar issues and statistical approaches apply to the estimation of the influenza burden on hospitalization [10, 11, 49]. The various statistical approaches all attribute “excess” health outcomes (deaths or hospitalizations) in winter months to influenza. Such seasonal approaches are not suited to studying disease burden of influenza in countries with tropical climates because they require an annual seasonal pattern of viral activity interrupted by influenza-free periods.
More recently, the US Centers for Disease Control and Prevention (CDC) has used an approach to measure hospitalization and mortality burden based on a new generation of seasonal regression models integrating laboratory surveillance data on influenza and respiratory syncytial virus (RSV) [5, 11]. In such models, winter seasonal increases in deaths or hospitalizations are directly proportional to the magnitude of respiratory virus activity. In the USA between 1980 and 2001, Thompson et al. [5, 11] estimated that seasonal influenza epidemics were associated with 17 deaths per 100,000 on average (range 6–28 per 100,000) depending on the severity of the circulating strains. Reassuringly, different model approaches, with and without the quantification of the number of viral isolates, yield similar average estimates of the influenza mortality burden in the USA [13, 50, 51]. Estimates from Europe and Canada are similar to those from the USA [44, 52, 53]. Viral surveillance data with the integration of hospitalization or death indicators are particularly useful for the study of influenza in the tropics where there is less seasonality.
2.2 Age and Time Variability in Influenza-Related Mortality in Temperate Climates
Influenza-related deaths contribute ~5% (range 0–10%) of all winter mortality in persons over 65 years of age in the USA, with similar proportion in Italy and Canada [12, 53, 54]. Seasons dominated by the influenza A/H3N2 subtype are typically associated with 2–3-fold higher mortality than seasons dominated by A/H1N1 and influenza B viruses from the 1980s to 2009. The pattern is not always uniform; there have been influenza A/H3N2-dominated seasons with little excess mortality (e.g., 2005–2006 northern hemisphere season). The age-specific risk of influenza-related (excess) mortality rates rises sharply past age 65 years (Fig. 2). People aged ≥80 years are at approximately 11-fold higher risk than people aged 65–69 years. Moreover, in recent decades about 90% of all influenza-related deaths occurred among seniors ≥65 years, 75% occurred among seniors aged ≥70 years, and 55% occurred among seniors over 80 years [12]. As the population in the USA and other developed countries has aged substantially over the last decades, the crude number of influenza-related deaths has been rising. Because the risk of influenza-related death increases exponentially with age in the later decades of life, it is essential to standardize for age when comparing mortality impact in different countries and over time [12, 54].

Average age-specific rates of influenza-related excess deaths and hospitalizations for ten seasons during 1990–2001 in the USA (estimated from Serfling regression models). Note the characteristic U-shape of severe disease burden by age that characterizes seasonal influenza. Data source: Vital Statistics from the National Center for Health Statistics (NCHS) and hospital discharge data from Agency for Health Care Research and Quality (AHRQ)
2.3 Burden and Circulation Patterns of Influenza in the Tropics
Because most seasonal influenza models (“Serfling approaches”) depend on winter seasonality in the data, they are not generally useful for tropical countries. However, such models can be used for unusually severe epidemics and pandemics, where the excess disease burden is many fold greater than in average years [43]. Integration of viral surveillance data with death or hospitalization indicators is the most useful approach in tropical settings, although long-term historical surveillance data are usually lacking [27]. A series of studies in Hong Kong and Singapore recently found that annual influenza-related hospitalization and mortality rates in wealthy (sub)tropical locations are similar to those in temperate countries [39–42]. In Hong Kong, as in many other countries, the influenza is associated not only with pneumonia outcomes but also with a wide range of chronic health conditions such as diabetes and cardiovascular diseases [42]. In addition, influenza-related hospitalization rates in Hong Kong vary with age as a U-shaped curve [41], in which young infants and elderly people are at highest risk of severe outcomes, reminiscent of the age pattern of epidemic influenza in the USA and other temperate countries.
The spread of influenza in the tropics has also proven to be an enigma. Influenza seasonality in the southernmost temperate regions is 6 months out of phase with the northern hemisphere. A study from Brazil found seasonal influenza activity starting early in remote, less densely populated equatorial regions of the north (March–April) and traveling in ~3 months to the more temperate areas of the south during their winter season (June–July) [28]. This finding was contrary to what was expected, given that the larger, well-connected, densely populated cities are located in the south. If population movements were a driving factor like in the USA [14], then the opposite traveling wave would have been expected. This study has inspired further studies to investigate the circulation of specific influenza virus subtypes during a season based on analysis of viral genomics data. Finding firm evidence of this unusual circulation pattern suggested from analysis of regional mortality data also bears on considerations of use of southern or northern hemisphere vaccine formulation and timing. Because of this study, Brazil is considering changing the timing of vaccination in the north of Brazil to accommodate the early occurrence of influenza in that area.
2.4 The Burden of Influenza in Infants and Young Children
For age groups other than those over 65 years of age, it can be difficult to measure the relatively low seasonal impact of influenza mortality above the expected baseline. However, for occasional severe seasons, a surge in P&I deaths can often be seen in children and young adults. For example, the 2003–2004 season was dominated by a new antigenic variant of A/H3N2 viruses (A/Fujian/2003) and was unusually severe; in the USA, 153 children with documented influenza infections died of primary or secondary pneumonia and sepsis [55]. Surprisingly, 47% of the children who died had no known underlying risk conditions. The reason for this unusual epidemic of pediatric deaths has not been resolved. As a result of this experience, the CDC enhanced their influenza surveillance system with a reporting system for children hospitalized with laboratory-confirmed influenza.
2.5 The Impact of Influenza on Morbidity
Very few quantitative data on mild influenza morbidity with known population denominators are available. The most careful studies using the longest existing time series come from the Royal Network of General Practitioners in the UK, which has reported influenza-like illnesses on a weekly basis since 1966 [52, 56]. Such long-term morbidity records are unique and have allowed the study of the 1968–1969 influenza pandemic transmission patterns based on case data [57]. In addition to the UK, several countries have national sentinel surveillance systems in place (USA, France, Netherlands, Australia, and New Zealand are examples). These are used to detect the onset and peak timing of influenza epidemics, as well as the magnitude of morbidity impact relative to surrounding seasons. In the USA, emergency room visit time series are now being analyzed in the context of biodefense research and have shed light on interannual and age-specific variability in influenza impact [25, 58].
In contrast, quantitative burden studies using samples of national hospital discharge data and estimation approaches similar to those used for excess mortality are more widely available, in particular since the 1970s [11, 49, 59, 60]. The patterns of excess hospitalizations are quite similar to those of excess mortality, with a U-shaped incidence reflecting the highest values in young children and seniors (Fig. 2).
2.6 The Relative Contribution of Influenza and RSV
One controversy in the literature concerns the relative contributions of influenza and RSV to the winter increase in respiratory hospitalizations and deaths, especially among seniors. The current CDC modeling approach simultaneously estimates the influenza and RSV burden by correlating periods of excess mortality with their respective period and magnitude of viral activity [5]. In the overall US population, the CDC investigators estimate that the average seasonal RSV burden is approximately one-third of that of influenza for all seasons during the 1990s. However, the relative contribution of RSV and influenza varies greatly with age.
For US infants of <12 months of age, the RSV contribution to mortality is more than twofold greater than that of influenza (5.5 vs. 2.2 deaths per 100,000) based on the CDC model [5]. Above 5 years of age, mortality due to influenza predominates in the US data, similar to the age pattern of respiratory deaths in the UK [61]. For seniors over age 65, the CDC model estimates the average seasonal RSV burden at ~10,000 deaths, which is approximately one-third the estimated deaths attributed to influenza over the same period. But others disagree; several observational studies set in the UK by Fleming et al. [62, 63] have argued that RSV has replaced influenza as the major cause of respiratory mortality and hospitalization, in particular in the elderly. Further, in a recent laboratory-based study set in a large cohort of seniors hospitalized with pneumonia, twice as many hospitalizations were attributed to RSV as influenza [64]. But because influenza-related pneumonia is most often due to secondary bacterial infections (quite distinct from primary RSV pneumonia) that occur long after the triggering influenza infection has been cleared, it is possible that this study substantially underestimated the influenza burden [65].
Two recent studies carefully delineated the relative burden of influenza and RSV in children, using seasonality in pediatric respiratory hospitalizations and focusing the analysis on seasons when the influenza and RSV epidemics occurred at different times [39, 66]. The authors subtracted hospitalization rates during periods of high influenza circulation from baseline “peri-influenza” winter periods when neither influenza nor RSV was circulating (Fig. 3). Using this approach, the authors attributed a similar number of hospitalizations to RSV and influenza in children under 5 years in the USA [66]. In a parallel study from Hong Kong, investigators attempted to delineate the burden of RSV, influenza, and other respiratory pathogens in various age groups in this subtropical setting with less clear seasonality [39]. Although influenza burden estimates in Hong Kong were similar to those of the USA in most age groups [27], children under 5 years appeared to have approximately tenfold higher rates of hospitalization in Hong Kong than in the USA [39]. Such large discrepancies may reflect true geographical differences in influenza transmission and impact, although they are perhaps more likely to result from differences in access to hospital care. Indeed, young children in Hong Kong tend to be rushed to the hospital when they have respiratory symptoms (Malik Peiris, personal communication).

An analytic approach to estimate influenza-related hospitalization rates in USA and Hong Kong children [39, 66]. This method relies on identifying the precise periods of influenza and RSV viral circulation for each season studied. Influenza-related excess rates were calculated as the difference in observed rates between periods of influenza and RSV circulation and those with low circulation of both influenza and RSV
Finally, there are numerous studies on respiratory virus isolates from children hospitalized with respiratory symptoms in tropical and subtropical settings. A review of these studies attributes a substantial proportion of pediatric respiratory hospitalizations to influenza A and B viruses [67]. Unfortunately, it is difficult to compare findings across studies because they are often carried out using different laboratory techniques and are set in different study years, seasons, and clinical settings. These studies frequently present a systematic age pattern that suggests that RSV is more important in infancy, with a gradual shift to influenza by about 5 years of age as the pathogen more likely to cause severe respiratory illness.
2.7 Observational Transmission Studies
The transmission patterns of influenza were carefully documented in classic virus surveillance studies that meticulously followed all respiratory illness episodes in a large number of families in Cleveland, Ohio, Tecumseh, Michigan, Seattle, and Washington in the 1950s through the 1970s [35, 68, 69]. Unfortunately, such careful studies have not been repeated in contemporary populations, so little is known about the consequences of increasing population movements and changes in intrafamilial interactions. The result is that the existing mathematical models employed to “forecast” the likely patterns and spread of a pandemic influenza virus rely largely on parameter values of transmission and age group dynamics that are decades old and may not reflect current realities.
In parallel to careful family studies tracking the infection status of each individual, time series mortality data aggregated at the scale of cities, regions, or countries can also be used as a proxy to estimate the transmissibility of influenza [16, 19, 20, 23, 24, 70–73]. Two crucial factors, the basic reproductive number, R0, and the effective reproductive number, R, have been estimated for pandemic and epidemic influenza. R0 measures the average number of secondary infections per primary case for a new pathogen invading a fully susceptible population (e.g., a pandemic influenza virus), whereas R measures a similar quantity for a recurrent pathogen re-invading a partially susceptible population (e.g., seasonal influenza virus). Current estimates of R0 and R are in the range of 1.7–5.4 for pandemics and 1.0–2.1 for seasonal influenza epidemics. While these estimates of transmissibility are not as high as for other respiratory viruses (e.g., for measles R is ~15), the generation time for influenza is relatively short, on the order of 2–4 days. Consequently, in a 60-day period, there could be R (60/4) to R (60/2) infections.
Overall, the use of time series of population-level data (hospitalizations, mortality) in large populations has provided a more complete picture of the transmissibility of influenza through space and time. One study correlated mortality peaks in US influenza seasons for the last 30 years with daily transportation data and found that epidemics spread across the country in an average of about 6 weeks and that transmission was correlated with adult work travel patterns [14].
2.8 Syndromic Surveillance and Its Contributions to Influenza Epidemiology
Use of real-time syndromic surveillance data is another area with substantial promise in influenza epidemiology. Information technology now allows for the rapid compilation and analysis of electronic health records from emergency rooms, inpatient hospitals, and outpatient clinics. Syndromic surveillance efforts have already provided a new level of insight into age and geographic patterns of impact of influenza epidemics. In particular, a recent study that combined time series analysis of age-specific emergency room visits with laboratory-confirmed timing of influenza and RSV periods in New York City demonstrated that the burden of a contemporary influenza epidemic varies greatly at the level of age cohorts in children and adults, perhaps as a consequence of different historical exposures to influenza [25].
2.9 Influenza Genomics and Molecular Epidemiology
Phylogenetic and antigenic studies of influenza viruses have increased our understanding of the emergence and spread of new influenza drift variants both locally and globally. Begun in 2004, the Influenza Genome Sequencing Project, as well as an increased number of sequences published by other contributors, has resulted in the publication of over 80,000 influenza genes from isolates around the world isolated from numerous species. These data have led directly to advances in molecular influenza epidemiology [31]. Studies emerging from this project have demonstrated a high frequency of gene segment reassortment in A/H3N2 viruses, perhaps more frequent around the time of transition to new antigenic variants [30]. Specifically, one possible mechanism leading to the emergence of antigenic novelty is reassortment between dominant and subdominant lineages of past seasons. Further, each A/H3N2-dominated season features multiple genetically distinct cocirculating lineages that may or may not have similar antigenic properties [32]. Studies of recent epidemics of A/H3N2 in New York City and New Zealand have shown that next season’s viruses are seeded by importation either from the opposite global hemisphere or from the tropics and that there is no preferred hemisphere leading the circulation of viruses [74]. This rapidly emerging area of molecular influenza epidemiology has increased our understanding of viral circulation patterns around the globe, and the genesis and spread of drift variants.
3 Pandemic Influenza: Lessons from Historical Data and Modeling
Historic experience with influenza pandemics in the twentieth century has been a prelude to the current pandemic with the global spread of novel A/H1N1pdm virus [75]. The three pandemics of the twentieth century – the 1918 A/H1N1 “Spanish influenza,” the 1957 A/H2N2 “Asian influenza,” and 1968 A/H3N2 “Hong Kong influenza” – were highly variable in terms of mortality impact (Table 1). The catastrophic 1918 pandemic resulted in 0.2% to as much as 8% mortality in various countries around the world and an estimated global mortality of ~50 million people [76]. The relatively mild 1968 pandemic, however, was not appreciably worse than other severe seasonal epidemics in terms of total influenza-related deaths, whereas the 1957 A/H2N2 pandemic was moderately severe [15, 18]. As of September 2009, in the northern hemisphere autumn season, the impact of the A/H1N1 pandemic virus appears relatively mild, though it has an uncertain future of mutating to a more virulent strain.
3.1 History Lessons from the Field of Archaeo-Epidemiology
Recent efforts to re-examine the 1918 Spanish influenza pandemic [77], as well as that of later pandemics, have allowed for a more comprehensive view of pandemics and highlighted their diversity in time and space. Historical vital statistics data have been analyzed to provide a quantitative analysis of the last century’s three pandemics. For each of these pandemics, there was a quantitative and qualitative change in the mortality patterns, as compared to seasonal influenza epidemics. The shift of the mortality burden to younger ages has been a “signature” of each pandemic and stands in marked contrast to the low mortality burden among young people during typical influenza epidemics [15, 78]. This age shift was most pronounced in the 1918 pandemic but occurred in all three pandemics for which age group mortality data have been studied (Table 1; Fig. 4). During the initial outbreak of the novel H1N1pdm virus (April 2009), a shift of morbidity and mortality toward younger age groups was observed in Mexico [79] and remains a characteristic of this virus.

Age-specific mortality impact of three historical pandemics contrasted with the average impact of recent A/H3N2 epidemics in the 1990s. Based on a Serfling model applied to US all-cause excess mortality data (and presented on a logarithmic scale)
Sero-archaeology studies of collections of serum from blood donors have been informative about preexisting influenza antibodies and therefore indicate the past circulation of historical pandemic viruses, even in tropical populations. These studies provide interesting pieces of the puzzle but have unfortunately fallen out of fashion lately. For example, one collection of serum gathered before the 1968 pandemic showed that people born before 1892 had antibodies to the hemagglutinin A/H3 antigen; this may partially explain the fact that seniors older than 77 years were only at a decreased risk of death during that pandemic [15, 80]. In another example, a sero-epidemiology study looking at influenza antibodies in a population of women in Ghana following the 1968 pandemic showed that in the tropics, most had become infected 5 years after the emergence of the A/H3N2 subtype [81].
A similar antigen recycling phenomenon may explain the low rates of morbidity and mortality observed in people over the age of 50 years in the early months of A/H1N1pdm virus circulation [79]. For almost all persons born from 1918 to 1957 (~52- to 91-year olds in 2009), the first exposure to an influenza A virus was to the strains containing A(H1); those born from 1957 to 1968 (~41 to ~52) to A(H2); those born since the 1968 pandemic (<41 years of age), most likely first saw A(H3). Indeed, the A(H1) subtype was reintroduced in 1977 but rarely dominates [5], suggesting that most people born after 1977 were first exposed to A(H3) viruses. This is important because the concept of “original antigenic sin” postulates that the first encounter with an influenza virus, likely in childhood, provides the strongest immunity in later years [82]. Therefore, people born before 1957 may have the greatest natural immunity to the currently circulating A/H1N1pdm pandemic virus in 2009 [79].
Looking back to the 1918 A/H1N1 pandemic suggests that antigen recycling may have also played a role and could partly explain the extreme case of mortality age shift associated with this pandemic. In this pandemic, seniors were completely spared, in stark contrast to the extreme mortality impact in the young adults, as shown by age-specific mortality surveillance from New York City (Fig. 5) [17, 78]. This was further confirmed in an additional study of age-detailed mortality time series from Copenhagen [22]. This phenomenon could be explained by immune protection conferred by prior exposure (recycling) of an H1Nx virus in the late nineteenth century. Alternatively, the atypical mortality spike in young adults in the 1918 pandemic may be explained by an unusual immune dysfunction causing a “cytokine storm” [83, 84], which primarily affected young adults. These two possibilities – recycling and immune pathology – cannot be resolved without further experimental and epidemiological studies. This unfortunately leaves us with a great unknown as we attempt to deal with the current pandemic: if the pandemic virus contains a hemagglutinin antigen that has not previously circulated in human populations – such as the current avian A/H5N1 virus in Asia – then the recycling hypothesis would suggest seniors could be at great risk, as suggested by one author [85]. In contrast, the immune pathology hypothesis suggests that immune senescence might mitigate the full impact among seniors, leaving young adults at highest risk of dying.

Comparison of age mortality patterns during the 1918 pandemic and a severe interpandemic season, New York City. (a) Influenza season-attributable excess deaths are plotted for the 1915–1916 interpandemic seasons (○), the pandemic herald wave (epidemic months March and April 1918; ▴), and the main fall pandemic wave (September 1918 to April 1919, ▪). (b) Relative risk of death is plotted by age group on a log10 scale for the herald (▴) and fall pandemic waves (▪), relative to the severe interpandemic season. Adapted from Olson et al. [17]
Comparative studies of pandemic influenza in multiple countries have revealed many interesting insights. For example, a recent study used annual mortality data from multiple countries to estimate the mortality burden of the 1918–1920 influenza pandemic and uncovered substantial geographical differences in influenza-related mortality rates. The percentage of the population that died varied from 0.2% in Scandinavia to 8% in some areas of India, representing a 40-fold difference in mortality risk in these settings [76]. The underlying reasons for this substantial variability are not well understood but might be revealed by additional historical pandemic studies.
In a second example, analysis of excess mortality data from several countries put a surprising spin on the 1968 pandemic [18]. An unexpected pattern of a “smoldering” mortality impact in European and some Asian countries was revealed – a relatively mild first wave of the emerging virus in the 1968–1969 season, followed by a very severe 1969–1970 season. This is different from the classical impression based on the North American experience that most of the impact occurs with the first exposure to pandemic strains. It may be more common than previously thought that the first wave of a pandemic virus results in low mortality, only to be followed by a more dramatic impact a few months later. Indeed, this intriguing pattern was not only observed in some countries during the mild 1968 pandemic but also consistent with the herald wave experience in New York City and Scandinavia during the catastrophic 1918 pandemic [17, 22]. Further, historical mortality data from the less-studied 1889–1892 pandemic in England also suggest a pattern of successive pandemic waves where the first encounter was not the most lethal [86]. The reasons for this “smoldering” (or herald wave) pattern are still unknown and may be partly related to on-going adaptation in newly emerged pandemic viruses and preexisting population immunity.
3.2 Transmission Models Used to Predict Future Pandemic Scenarios
Mathematical transmission models have been employed to simulate in detail the possible spread of a new pandemic virus in a susceptible human population (e.g., [70, 71, 87, 88]). These models seek to predict the spatiotemporal dynamic of a hypothetical pandemic virus and the effectiveness of intervention strategies such as vaccination before an outbreak with a partially matched, low-efficacy vaccine, distribution of antivirals for prophylaxis or treatment, school closure, case isolation, and household quarantine. These models generally agree that a combination of measures, if implemented early and with sufficient compliance, might bring about a meaningful level of mitigation and substantially slow geographic spread. Subsequent studies found that early, targeted, and layered use of nonpharmaceutical interventions could greatly reduce the overall pandemic attack rate, provided the intrinsic transmissibility (basic reproductive number, R0) of the emerging virus is not greater than two [89–91]. Mathematical models can be useful to estimate the potential impact of interventions assuming a wide range of parameters. Furthermore, they can prioritize research by highlighting the most sensitive and uncertain parameters for a desired outcome. Simulation models currently used for pandemic planning still need to be tested against real disease data, and for this we must continue to gather data on influenza morbidity, mortality, and viral genetic sequences in both pandemic and seasonal influenza scenarios [92].
3.3 Predicting the Impact of Pandemics
Until spring 2009, concern has focused on the highly pathogenic variant of A/H5N1 influenza that emerged in Hong Kong in 1997 and remerged in 2003. A/H5N1 has now spread to avian populations in more than 30 countries. It is present endemically in Southeast Asia, causing regular die-offs in poultry and wild birds, and occasionally affects humans. As of August 31, 2007, the World Health Organization (WHO) had counted 327 laboratory-confirmed H5N1 cases and noted a very high case fatality of ~61% (http://www.who.int/topics/avian_influenza/en/ 2007). While H5N1 continues to be an economic problem in Asia, Africa, Europe, and the Middle East, the critical question for public health is whether it will gain the ability to effectively transmit among humans. This could occur in one of the two ways: by gradual mutations of avian H5N1 viruses, or by reassortment with circulating human influenza A viruses (H3N2 or H1N1), in humans or another animal. Several comprehensive discussions of the threat of an avian influenza pandemic have been published (e.g., [85, 93–96]).
There are still many uncertainties about the pandemic potential of the circulating avian H5N1 virus, including its potential to effectively transmit between humans and the evolutionary mechanisms that may concurrently affect its virulence. The classical belief is that extremely pathogenic viruses are not well adapted to their hosts – moribund patients do not transmit viruses as easily as those who remain mobile. Further, the pathogenesis of novel pandemic viruses remains unclear, in particular the proportions of severe disease caused by immune-mediated pathological responses, secondary bacterial infections (for which treatments exist), and exacerbation of chronic illnesses. Modern medicine can mitigate some of the pathological mechanisms and control secondary bacterial infections to a certain extent; however, there is undoubtedly a different proportion of persons living with chronic comorbid conditions now than was the case during previous pandemics. Finally, we do not know the degree of cross-protection afforded by early exposure to other influenza virus antigens [97]. If one simply applies the 1918 mortality experience to today’s population, anywhere from 0.2% to 8% of a country’s population could die, and the highest burden would be suffered by developing countries [76].
The emergence of the H1N1pdm virus poses the threat of a potentially severe pandemic in the months to come. Research efforts have intensified and a vaccine has been developed, but many questions remain unanswered. We do not know whether the H1N1pdm virus will reassort with seasonal influenza viruses. We do not know what proportions of severe disease caused by immune-mediated pathological responses, secondary bacterial infections, and exacerbation of chronic illnesses it will cause nor do we know how well medical interventions will mitigate the impact. In terms of mortality, although age groups with severe disease tend to be under 60 years of age, there are more people living with comorbid conditions than during previous pandemics. Thus, for the moment transmission dynamics, morbidity and mortality impact, and the degree of immunity remain obscure.
4 Epidemiology and the Control of Influenza
Influenza vaccines were originally developed for use by the military and have been shown to be highly effective in preventing infection in healthy adults [98]. Most countries that use seasonal influenza vaccine have adopted a policy of targeting influenza vaccination efforts to those at “high risk” of severe outcomes, including those age 65 years and older, persons with certain chronic diseases and their close contacts. Although current policy continues to emphasize vaccination of seniors, the “gold standard” evidence that this strategy effectively reduces influenza-related mortality in that age group is not strong [99]. It has recently become evident that influenza-related mortality has not decreased in at least some countries despite major gains in vaccination coverage among people at highest risk [5, 12, 54, 100]. Because “gold standard” evidence from randomized clinical trials is scarce, epidemiological tools and studies constitute the vast majority of the evidence base for whether vaccination programs are beneficial. Paradoxically, observational studies have consistently argued that about 50% of all winter deaths in seniors are preventable with influenza vaccination despite the relatively low immune response to vaccine in this population [101].
4.1 The Scarce Evidence from Clinical Trials
Langmuir, who originally formulated the policy of targeting seniors and high-risk population for vaccination, questioned whether the vaccine would really be effective in seniors who respond less vigorously to the vaccine than younger adults [102]. Only a single randomized placebo-controlled clinical trial set in young healthy seniors is available. It showed that vaccination effectively prevents influenza illness in seniors aged 60–69 years but could not document significant benefits in seniors ≥70 years [103]. The authors expressed concern that their nonsignificant finding of 23% efficacy in seniors ≥70 years old indicated immune senescence (a decline in immune response with age), although they also noted limitations on the statistical power of their study to address this question. As both T-cell and B-cell responses are impaired in older individuals, it is plausible that the vaccine antibody response to the drifting influenza viruses and vaccine components is less vigorous in seniors [104]. Consequently, immunologists have long perceived a need for more effective vaccine formulations for this population, including the need for adjuvants and a move back to whole-cell vaccine products. The recent emergence of novel avian strains and development of vaccines against them has reopened many of the discussions of immunogenicity and correlates of protection.
4.2 Evidence from Observational Studies
In the near-absence of randomized clinical trials, these cohort studies have long provided the evidence base that supports influenza vaccine policy. Paradoxically, the concerns about immune senescence and vaccine failure have existed in parallel with cohort studies reporting extraordinarily large mortality benefits in vaccinated seniors [105–107]. In these studies, comparison of vaccinated and unvaccinated seniors indicates that vaccination could prevent fully 50% of all deaths among during winter months, implying that influenza causes half of all winter deaths among seniors. Instead, meta-analyses consolidated the findings and produced estimates with tight confidence intervals. But only about 5% of all winter deaths can be attributed to influenza in an average season according to excess mortality studies [5, 12, 54]. Even in the 1968 A/H3N2 pandemic and in more recent seasons such as 1997–1998, when the vaccine was completely mismatched to the new circulating variant of A/H3N2, the proportion of all deaths attributed to influenza never exceeded 10% of all winter deaths among seniors [12].
A few researchers subsequently addressed this paradox directly and investigated the possibility that unrecognized bias has led the majority of cohort studies to systematically overestimate influenza vaccine benefits. In 2006, two published reports clearly demonstrated that the senior cohort study findings are largely a result of systematic mismeasurements [108, 109]. First, they showed that the greatest mortality reductions occurred in early winter before influenza ever circulated and were not specifically associated with the peak influenza period. Second, they showed that the analytical adjustment techniques typically used in cohort studies actually magnified the mismeasurement rather than reducing it. The authors concluded that the magnitude of the unadjusted bias detected was sufficient to account entirely for the observed benefit of 50% mortality reduction during the entire winter period. This problem in the evidence base was also highlighted in a recent Cochrane review and an editorial [106, 110]. The source of bias may be a subset of frail seniors who are undervaccinated in the fall months for that season and subsequently contribute substantially to mortality in the early winter months [99]. Studies have substantiated that frail elderly are indeed vaccinated less often than their healthy peers [111, 112]. Controlling for these biases yields far more modest estimates of mortality reductions [113].
In summary, the emerging picture is a mixture of that residual selection bias, counter-productive adjustment efforts, and low-specificity endpoints has led to systematic overestimation in virtually all cohort studies published over the last decades. Adjustments for selection bias may be possible, but only if high specificity endpoints are studied. Beyond that, a commonly agreed set of standards for carrying out and reporting observational studies that includes a framework for detection of bias would be helpful. Also, previously published observational studies could undergo reanalysis, guided by such expectations as that vaccine benefits should be highest in peak influenza periods and for well-matched influenza vaccines. We have recently proposed such a framework [99].
4.3 Revisiting the Evidence Base Supporting Strategies for Protecting Populations with Vaccine
If we discount the biased cohort studies, the remaining studies suggest that the benefits of the vaccine are in fact much less than previously thought to be – probably lower than 30% in seniors >70 years of age. This assessment is based on the “gestalt” of results from the randomized placebo-controlled clinical trial described earlier [103], a nested case–control study using laboratory-confirmed endpoints from an RSV study [64, 65], and the excess mortality studies showing little decline in mortality as vaccine coverage rose [12, 54]. None of these studies are conclusive, but if these findings hold up in future studies, then there is ample room for improvement of influenza vaccines, including better vaccine formulations, adjuvants, or higher doses or combinations of live and killed vaccine doses [114–116].
Japan is the only country that has implemented a policy of vaccinating school children, with a strategy of reducing transmission in the community and thereby indirectly protecting high-risk populations. Although Japan abandoned this policy in 1994, an excess mortality study found evidence that it was associated with substantially reduced excess mortality in elderly people for the decades it was in place [117] (Fig. 6). Other studies have examined the value of inducing greater herd immunity based on local community trials or mathematical models [118–121], but unfortunately none have thus far proved conclusive enough to extend the policy of school children vaccination nationally. To fully investigate the indirect benefits of a school children vaccination program, it would be necessary to conduct a large cluster-randomized study across the country; such a study has been proposed but has not yet been undertaken [122].

Herd immunity and influenza vaccination. Encouraging evidence from the Japanese experience of vaccinating school children between 1964 and 1996. The graph compares the different phases of the vaccination program with baseline total death rates, rates of excess deaths from all causes and pneumonia and influenza, in Japan, 1950–1998. Adapted from Reichert et al. [117, 122]
4.4 Vaccines for the Control of Pandemic Influenza
Prior to spring 2009, a great deal of effort had been expended to develop and clinically test several types of vaccines against H5N1 influenza, including inactivated, live-attenuated, and DNA vaccine preparations. Several countries had stockpiled million doses of “prepandemic” inactivated vaccines based on H5N1 strains. During May to August, 2009, a first vaccine against the H1N1pdm virus has been developed with plans to vaccinate populations in the northern hemisphere autumn months. National planning documents have set forth priorities for how to deploy an effective vaccine as it becomes available, and detailed logistical plans have been laid for vaccine distribution. WHO and national pandemic plans are reviewed in Uscher-Pines et al. [123].
But uncertainties abound. We still do not know which age groups will be most at risk, although a shift in mortality toward younger people is very likely. Whether this shift will put young adults at greatest absolute risk (as was the case in 1918–1919), or just higher relative risk (as in 1957–1958 and 1968–1969), cannot be predicted. Although effective vaccines against H1N1pdm have already been developed and are being manufactured in large quantities, just how quickly the billions of doses required to vaccinate a substantial portion of the world’s population will be available is unknown. Resource-poor countries fear that they will be able to obtain vaccine for their populations only after wealthy countries have covered their own – a fear that had already exacerbated tensions over sharing of H5N1 data and samples [124]. For all these reasons, it is not clear that policy makers’ hopes that vaccines will play a major role in limiting the global impact of the next pandemic will be realized.
5 Remaining Questions in Influenza Epidemiology and Considerations About the 2009 Pandemic
Many unsolved questions about influenza epidemiology remain [86, 125–127]. Solving these riddles will depend on the successful integration of many separate fields, including immunology, phylogenetics, virology, and clinical ascertainment. Exciting progress has recently been made in areas where mathematical modelers and phylogenetic researchers have entered the influenza field [29, 31, 128, 129]. This cross-fertilization has, for example, produced useful new findings in molecular influenza epidemiology, which may in turn lead to improved tools for the selection of vaccine strains [130].
Regarding pandemic influenza, for more than a decade the world had been bracing for a pandemic emerging from an avian H5N1 virus. Preparedness efforts anticipated that a pandemic would likely originate in Asia and focused strongly on surveillance of wild and domestic birds. Instead, the pandemic H1N1pdm virus emerged in Mexico, displaying a complex evolutionary lineage drawn from gene segments found in human, avian, and swine populations.
Fortunately, the H1N1pdm pandemic has thus far proved to be relatively mild, and the mortality impact of the summer 2009 northern hemisphere wave was not severe. Unlike seasonal outbreaks, however, the mortality and morbidity patterns of H1N1pdm show the “signature age shift” typical of influenza pandemics. Adults aged 20–50 years are at highest risk of severe morbidity and mortality [79], whereas children experience high rates of illness but relatively few severe outcomes. Seniors are largely spared from both illness and death, perhaps because of childhood exposure to H1N1 viruses circulating during 1918–1956.
Taken together, these features – a mild summer wave with elevated mortality in young adults and sparing of seniors – resemble the first wave pattern of the 1918 pandemic in the USA [17] and Europe [22]. Of note, morbidity impact in the first wave varied a great deal among US cities and regions [131]. For example, about 7% of New Yorkers have experienced influenza-like illness during the early weeks of the epidemic May 1–20, 2009, based on a phone survey [132], whereas other cities experienced little or delayed elevation of influenza-like illness [131]. Such spatial-temporal heterogeneity in timing of local epidemics remains unexplained.
Southern hemisphere countries, however, had the first encounter with the H1N1pdm virus under typical winter conditions. Reports from Argentina, New Zealand, and Australia suggest that pandemic impact is heterogeneous. Argentina experienced an emergency situation with severe overcrowding in hospitals and intensive care units, whereas New Zealand or Australia experienced no more than the equivalent of a severe A/H3N2 seasonal influenza epidemic [133]. Such variability between countries occurred during the 1918–1920 pandemic and was attributed to differences in access to care and overall mortality risk among developing countries [76]. In this on-going outbreak, however, it is still too early to quantify differences in disease burden with precision.
The case fatality rate is a key indicator of the severity of the H1N1pdm pandemic and an important decision parameter for determining pandemic response. But it is difficult to make an accurate estimate early in a pandemic. Because most H1N1pdm cases are not confirmed by laboratory testing and therefore not included in the “confirmed” tally, the case fatality rate tends to be greatly overestimated. In New Zealand, a combined strategy integrating epidemiological surveillance and modeling led to a case fatality rate estimate of 0.005% [134], far lower than earlier estimates based on early data from Mexico [135] and lower than the typical seasonal case fatality rate of ~0.2%. It is important to consider that while the case fatality rate – and perhaps even the total number of H1N1pdm-related deaths – may be lower than in a typical seasonal influenza epidemic, the higher proportion of deaths occurring in young adults results in a much higher burden of life years lost than in a typical influenza season, where 90% of deaths occur in those over 65 years of age [12].
Even though the similarities in the epidemiology of H1N1pdm and the 1918 pandemic are worrisome, as of September 2009, the pandemic is still relatively mild. We simply cannot know whether the virus will cause more severe waves in the coming months and years. A likely challenge will be the constant, dynamic real-time reassessment of benefit/risk of vaccinating atypical target groups during a pandemic. While policy makers plan to target vaccines to various groups, the perceived benefits from individuals will be based on severity of illness and real or temporally associated adverse reactions identified through surveillance and the media. Rapid reassessments of risks and benefits will be crucial for the viability of a vaccination program.
One impending question regarding vaccines, however, is whether the H1N1pdm virus will replace either or both of the influenza A viruses that had been circulating previously, H3N2 and H1N1. If all three cocirculate in the next season, the new H1N1pdm could be added as a component in the seasonal vaccine. But even if the new H1N1pdm thoroughly dominates the 2009–2010 season in one country, the other subtypes should probably still be included until the long-term pattern becomes clear. For example, it is not unusual for influenza A/H3N2 viruses to account for >99% of influenza specimens isolated in a country on a given year, only to become uncommon the next year, when seasonal A/H1N1 or influenza B virus might dominate. To avoid dropping any component too soon, it will be necessary to track subtype distribution globally over at least a few years. If history is a guide, as immunity builds up in younger population, the H1N1pdm virus will cause seasonal epidemics, with a proportionate shift in mortality to the older age groups.
Whatever the scenario, the epidemiological characteristics of a pandemic directly affect the ethical principles that should be invoked when allocating limited vaccine doses [136, 137]. For that reason, it is absolutely essential that real-time surveillance data from the early phase of a pandemic continue to be freely shared and rapidly interpreted to determine who is at risk and where scarce resources such as pandemic vaccine and antivirals could best be used. Moreover, pandemic planners should build sufficient flexibility into their plans to allow rapid shifts in planned control strategies, as key epidemiological insights hopefully become available in the early pandemic phase. Continued influenza surveillance efforts in temperate and tropical regions, combined with international sharing of epidemiological and viral sequence data, are our best hope for limiting the impact of current and future influenza pandemics.
References
Nicholson K, Hay A (1998) Textbook of influenza. Blackwell, Oxford
Schoenbaum S (1996) Impact of influenza in persons and populations. In: Brown L, Hampson A, Webster A (eds) Options for the control of influenza III. Elsevier, Amsterdam, pp 17–25
Reichert TA, Simonsen L, Sharma A, Pardo SA, Fedson DS, Miller MA (2004) Influenza and the winter increase in mortality in the United States, 1959–1999. Am J Epidemiol 160:492–502
Simonsen L (1999) The global impact of influenza on morbidity and mortality. Vaccine 17(Suppl 1):S3–S10
Thompson WW, Shay DK, Weintraub E, Brammer L, Cox N, Anderson LJ, Fukuda K (2003) Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA 289:179–186
Serfling R (1963) Methods for current statistical analysis of excess pneumonia-influenza deaths. Public Health Rep 78:494–506
Choi K, Thacker SB (1981) An evaluation of influenza mortality surveillance, 1962–1979. I. Time series forecasts of expected pneumonia and influenza deaths. Am J Epidemiol 113:215–226
Carrat F, Valleron AJ (1995) Influenza mortality among the elderly in France, 1980–90: how many deaths may have been avoided through vaccination? J Epidemiol Community Health 49:419–425
Simonsen L, Clarke MJ, Williamson GD, Stroup DF, Arden NH, Schonberger LB (1997) The impact of influenza epidemics on mortality: introducing a severity index. Am J Public Health 87:1944–1950
Simonsen L, Fukuda K, Schonberger LB, Cox NJ (2000) The impact of influenza epidemics on hospitalizations. J Infect Dis 181:831–837
Thompson WW, Shay DK, Weintraub E, Brammer L, Bridges CB, Cox NJ, Fukuda K (2004) Influenza-associated hospitalizations in the United States. JAMA 292:1333–1340
Simonsen L, Reichert TA, Viboud C, Blackwelder WC, Taylor RJ, Miller MA (2005) Impact of influenza vaccination on seasonal mortality in the US elderly population. Arch Intern Med 165:265–272
Dushoff J, Plotkin JB, Viboud C, Earn DJ, Simonsen L (2006) Mortality due to influenza in the United States – an annualized regression approach using multiple-cause mortality data. Am J Epidemiol 163:181–187
Viboud C, Bjornstad ON, Smith DL, Simonsen L, Miller MA, Grenfell BT (2006) Synchrony, waves, and spatial hierarchies in the spread of influenza. Science 312:447–451
Simonsen L, Olson D, Viboud C, Miller M (2004) Pandemic influenza and mortality: past evidence and projections for the future. In: Knobler S, Oberholtzer K (eds) Forum on microbial threats. Pandemic influenza: assessing capabilities for prevention and response. Institute of Medicine, The National Academy of Sciences, Washington
Mills CE, Robins JM, Lipsitch M (2004) Transmissibility of 1918 pandemic influenza. Nature 432:904–906
Olson DR, Simonsen L, Edelson PJ, Morse SS (2005) Epidemiological evidence of an early wave of the 1918 influenza pandemic in New York City. Proc Natl Acad Sci USA 102:11059–11063
Viboud C, Grais RF, Lafont BA, Miller MA, Simonsen L (2005) Multinational impact of the 1968 Hong Kong influenza pandemic: evidence for a smoldering pandemic. J Infect Dis 192:233–248
Chowell G, Ammon CE, Hengartner NW, Hyman JM (2006) Transmission dynamics of the great influenza pandemic of 1918 in Geneva, Switzerland: assessing the effects of hypothetical interventions. J Theor Biol 241:193–204
Viboud C, Tam T, Fleming D, Handel A, Miller MA, Simonsen L (2006) Transmissibility and mortality impact of epidemic and pandemic influenza, with emphasis on the unusually deadly 1951 epidemic. Vaccine 24:6701–6707
Viboud C, Tam T, Fleming D, Miller MA, Simonsen L (2006) 1951 influenza epidemic, England and Wales, Canada, and the United States. Emerg Infect Dis 12:661–668
Andreasen V, Viboud C, Simonsen L (2007) Epidemiologic characterization of the summer wave of the 1918 influenza pandemic in Copenhagen: implications for pandemic control strategies. J Infect Dis 197:270–278
Chowell G, Miller MA, Viboud C (2007) Seasonal influenza in the United States, France, and Australia: transmission and prospects for control. Epidemiol Infect 2:1–13
Chowell G, Nishiura H, Bettencourt LM (2007) Comparative estimation of the reproduction number for pandemic influenza from daily case notification data. J R Soc Interface 4:155–166
Olson DR, Heffernan RT, Paladini M, Konty K, Weiss D, Mostashari F (2007) Monitoring the impact of influenza by age: emergency Department fever and respiratory complaint surveillance in New York City. PLoS Med 4:e247
Dushoff J, Plotkin JB, Levin SA, Earn DJ (2004) Dynamical resonance can account for seasonality of influenza epidemics. Proc Natl Acad Sci USA 101:16915–16916
Viboud C, Alonso WJ, Simonsen L (2006) Influenza in tropical regions. PLoS Med 3:e89
Alonso WJ, Viboud C, Simonsen L, Hirano EW, Daufenbach LZ, Miller MA (2007) Seasonality of influenza in Brazil: a traveling wave from the Amazon to the subtropics. Am J Epidemiol 165:1434–1442
Grenfell BT, Pybus OG, Gog JR, Wood JL, Daly JM, Mumford JA, Holmes EC (2004) Unifying the epidemiological and evolutionary dynamics of pathogens. Science 303:327–332
Holmes EC, Ghedin E, Miller N, Taylor J, Bao Y, St George K, Grenfell BT, Salzberg SL, Fraser CM, Lipman DJ, Taubenberger JK (2005) Whole-genome analysis of human influenza A virus reveals multiple persistent lineages and reassortment among recent H3N2 viruses. PLoS Biol 3:e300
Nelson MI, Holmes EC (2007) The evolution of epidemic influenza. Nat Rev Genet 8:196–205
Nelson MI, Simonsen L, Viboud C, Miller MA, Taylor J, George KS, Griesemer SB, Ghedin E, Sengamalay NA, Spiro DJ et al (2006) Stochastic processes are key determinants of short-term evolution in influenza a virus. PLoS Pathog 2:e125
Cox NJ, Subbarao K (2000) Global epidemiology of influenza: past and present. Annu Rev Med 51:407–421
Glezen WP (1982) Serious morbidity and mortality associated with influenza epidemics. Epidemiol Rev 4:25–44
Monto AS (2002) Epidemiology of viral respiratory infections. Am J Med 112(Suppl 6A):4S–12S
Noble G (1982) Epidemiological and clinical aspects of influenza. CRC Press, Boca Raton
Stuart-Harris C (1979) Epidemiology of influenza in man. Br Med Bull 35:3–8
Glezen WP, Taber LH, Frank AL, Gruber WC, Piedra P (1997) Influenza virus infections in infants. Pediatr Infect Dis J 16:1065–1068
Chiu SS, Lau YL, Chan KH, Wong WH, Peiris JS (2002) Influenza-related hospitalizations among children in Hong Kong. N Engl J Med 347:2097–2103
Chow A, Ma S, Ling AE, Chew SK (2006) Influenza-associated deaths in tropical Singapore. Emerg Infect Dis 12:114–121
Wong CM, Yang L, Chan KP, Leung GM, Chan KH, Guan Y, Lam TH, Hedley AJ, Peiris JS (2006) Influenza associated weekly hospitalization in a subtropical city. PLoS Med 3:e89
Wong CM, Chan KP, Hedley AJ, Peiris JS (2004) Influenza-associated mortality in Hong Kong. Clin Infect Dis 39:1611–1617
Assaad F, Cockburn WC, Sundaresan TK (1973) Use of excess mortality from respiratory diseases in the study of influenza. Bull World Health Organ 49:219–233
Rizzo C (2007) Trends for influenza-related deaths during pandemic and epidemic seasons, Italy, 1969–2001. Emerg Infect Dis 13:694–699
Rocchi G, Ragona G, De Felici A, Muzzi A (1974) Epidemiological evaluation of influenza in Italy. Bull World Health Organ 50:401–406
Viboud C, Boelle PY, Pakdaman K, Carrat F, Valleron AJ, Flahault A (2004) Influenza epidemics in the United States, France, and Australia, 1972–1997. Emerg Infect Dis 10:32–39
Imaz MS, Eimann M, Poyard E, Savy V (2006) Influenza associated excess mortality in Argentina: 1992–2002. Rev Chilena Infectol 23:297–306
Stroup DF, Thacker SB, Herndon JL (1988) Application of multiple time series analysis to the estimation of pneumonia and influenza mortality by age 1962–1983. Stat Med 7:1045–1059
Barker WH (1986) Excess pneumonia and influenza associated hospitalization during influenza epidemics in the United States, 1970–78. Am J Public Health 76:761–765
Simonsen L, Taylor R, Viboud C, Dushoff J, Miller M (2006) US flu mortality estimates are based on solid science. Br Med J 332:177–178
Thompson W, Weintraub E, Cheng P et al (2007) Comparing methods for estimating influenza-associated deaths in the United States: 1976/1977 through 2002/2003 respiratory seasons. In: Katz JM (ed) Options for the control of influenza VI, International Medical Press, London
Fleming DM (2000) The contribution of influenza to combined acute respiratory infections, hospital admissions, and deaths in winter. Commun Dis Public Health 3:32–38
Schanzer DL, Tam TW, Langley JM, Winchester BT (2007) Influenza-attributable deaths, Canada 1990–1999. Epidemiol Infect 135:1109–1116
Rizzo C, Viboud C, Montomoli E, Simonsen L, Miller MA (2006) Influenza-related mortality in the Italian elderly: no decline associated with increasing vaccination coverage. Vaccine 24:6468–6475
Bhat N, Wright JG, Broder KR, Murray EL, Greenberg ME, Glover MJ, Likos AM, Posey DL, Klimov A, Lindstrom SE et al (2005) Influenza-associated deaths among children in the United States, 2003–2004. N Engl J Med 353:2559–2567
Elliot AJ, Fleming DM (2006) Surveillance of influenza-like illness in England and Wales during 1966–2006. Euro Surveill 11:249–250
Hall IM, Gani R, Hughes HE, Leach S (2007) Real-time epidemic forecasting for pandemic influenza. Epidemiol Infect 135:372–385
Brownstein JS, Kleinman KP, Mandl KD (2005) Identifying pediatric age groups for influenza vaccination using a real-time regional surveillance system. Am J Epidemiol 162:686–693
Crighton EJ, Elliott SJ, Moineddin R, Kanaroglou P, Upshur RE (2007) An exploratory spatial analysis of pneumonia and influenza hospitalizations in Ontario by age and gender. Epidemiol Infect 135:253–261
Fleming DM, Zambon M, Bartelds AI, de Jong JC (1999) The duration and magnitude of influenza epidemics: a study of surveillance data from sentinel general practices in England, Wales and the Netherlands. Eur J Epidemiol 15:467–473
Fleming DM, Pannell RS, Cross KW (2005) Mortality in children from influenza and respiratory syncytial virus. J Epidemiol Community Health 59:586–590
Fleming DM, Cross KW (1993) Respiratory syncytial virus or influenza? Lancet 342:1507–1510
Fleming DM, Elliott AJ, Cross KW (2007) Is routine seasonal influenza vaccination of elderly people an effective community policy? In: Katz JM (ed) Options for the control of influenza VI, International Medical Press, London
Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE (2005) Respiratory syncytial virus infection in elderly and high-risk adults. N Engl J Med 352:1749–1759
Simonsen L, Viboud C (2005) Respiratory syncytial virus infection in elderly adults. N Engl J Med 353:422–423
Izurieta HS, Thompson WW, Kramarz P, Shay DK, Davis RL, DeStefano F, Black S, Shinefield H, Fukuda K (2000) Influenza and the rates of hospitalization for respiratory disease among infants and young children. N Engl J Med 342:232–239
Weber MW, Mulholland EK, Greenwood BM (1998) Respiratory syncytial virus infection in tropical and developing countries. Trop Med Int Health 3:268–280
Monto AS (1994) Studies of the community and family: acute respiratory illness and infection. Epidemiol Rev 16:351–373
Monto AS, Cavallaro JJ (1971) The Tecumseh study of respiratory illness. II. Patterns of occurrence of infection with respiratory pathogens, 1965–1969. Am J Epidemiol 94:280–289
Ferguson NM, Cummings DA, Fraser C, Cajka JC, Cooley PC, Burke DS (2006) Strategies for mitigating an influenza pandemic. Nature 442:448–452
Ferguson NM, Cummings DAT, Cauchemez S, Fraser C, Riley S, Meeyai A, Iamsirithaworn S, Burke DS (2005) Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature 437:209–214
Spicer CC (1979) The mathematical modelling of influenza epidemics. Br Med Bull 35:23–28
Spicer CC, Lawrence CJ (1984) Epidemic influenza in Greater London. J Hyg (Lond) 93:105–112
Nelson MI, Simonsen L, Viboud C, Miller MA, Holmes EC (2007) Phylogenetic analysis reveals the global migration of seasonal influenza a viruses. PLoS Pathog 3:1220–1228
Kilbourne ED (1997) Perspectives on pandemics: a research agenda. J Infect Dis 176(Suppl 1):S29–S31
Murray CJ, Lopez AD, Chin B, Feehan D, Hill KH (2006) Estimation of potential global pandemic influenza mortality on the basis of vital registry data from the 1918–20 pandemic: a quantitative analysis. Lancet 368:2211–2218
Barry J (2004) The great influenza: the epic story of the deadliest plague in history. Viking Penguin, New York
Simonsen L, Clarke MJ, Schonberger LB, Arden NH, Cox NJ, Fukuda K (1998) Pandemic versus epidemic influenza mortality: a pattern of changing age distribution. J Infect Dis 178:53–60
Chowell G, Bertozzi SM, Colchero MA, Lopez-Gatell H, Alpuche-Aranda C, Hernandez M, Miller MA (2009) Severe respiratory disease concurrent with the circulation of H1N1 influenza. N Engl J Med 361:674–679
Simonsen L, Reichert TA, Miller M (2003) The virtues of antigenic sin: consequences of pandemic recycling on influenza-associated mortality. In: Kawaoka Y (ed) Options for the control of influenza V. International Congress Series, no. 1263. Elsevier, Okinawa, pp 791–794
McGregor IA, Schild GC, Billewicz WZ, Williams K (1979) The epidemiology of influenza in a tropical (Gambian) environment. Br Med Bull 35:15–22
Francis T Jr (1960) On the doctrine of original antigenic sin. Proc Am Philos Soc 104(6):572–578
Kash JC, Tumpey TM, Proll SC, Carter V, Perwitasari O, Thomas MJ, Basler CF, Palese P, Taubenberger JK, García-Sastre A et al (2006) Genomic analysis of increased host immune and cell death responses induced by 1918 influenza virus. Nature 443:578–581
Kobasa D, Jones SM, Shinya K, Kash JC, Copps J, Ebihara H, Hatta Y, Kim JH, Halfmann P, Hatta M et al (2007) Aberrant innate immune response in lethal infection of macaques with the 1918 influenza virus. Nature 445:319–323
Palese P (2004) Influenza: old and new threats. Nat Med 10:S82–S87
Stuart-Harris CH (1970) Pandemic influenza: an unresolved problem in prevention. J Infect Dis 122:108–115
Germann TC, Kadau K, Longini IM Jr, Macken CA (2006) Mitigation strategies for pandemic influenza in the United States. Proc Natl Acad Sci USA 103:5935–5940
Longini IM Jr, Nizam A, Xu S, Ungchusak K, Hanshaoworakul W, Cummings DA, Halloran ME (2005) Containing pandemic influenza at the source. Science 309:1083–1087
Bootsma MC, Ferguson NM (2007) From the cover: the effect of public health measures on the 1918 influenza pandemic in U.S. cities. Proc Natl Acad Sci USA 104:7588–7593
Glass K, Barnes B (2007) How much would closing schools reduce transmission during an influenza pandemic? Epidemiology 18:623–628
Glass RJ, Glass LM, Beyeler WE, Min HJ (2006) Targeted social distancing design for pandemic influenza. Emerg Infect Dis 12:1671–1681
Smith DJ (2006) Predictability and preparedness in influenza control. Science 312:392–394
Peiris JS, de Jong MD, Guan Y (2007) Avian influenza virus (H5N1): a threat to human health. Clin Microbiol Rev 20:243–267
Subbarao K, Luke C (2007) H5N1 viruses and vaccines. PLoS Pathog 3:e40
Taubenberger JK, Morens DM, Fauci AS (2007) The next influenza pandemic: can it be predicted? JAMA 297:2025–2027
Webster RG, Hulse-Post DJ, Sturm-Ramirez KM, Guan Y, Peiris M, Smith G, Chen H (2007) Changing epidemiology and ecology of highly pathogenic avian H5N1 influenza viruses. Avian Dis 51:269–272
Bermejo-Martin JF, Kelvin DJ, Guan Y, Chen H, Perez-Breña P, Casas I, Arranz E, de Lejarazu RO (2007) Neuraminidase antibodies and H5N1: geographic-dependent influenza epidemiology could determine cross-protection against emerging strains. PLoS Med 4:e212
Demicheli V, Rivetti D, Deeks JJ, Jefferson TO (2004) Vaccines for preventing influenza in healthy adults. Cochrane Database Syst Rev 3:CD001269
Simonsen L, Taylor RJ, Viboud C, Miller MA, Jackson LA (2007) Mortality benefits of influenza vaccination in elderly people: an ongoing controversy. Lancet Infect Dis 7:658–666
Reichert TA, Pardo SA, Valleron AJ et al (2007) National vaccination programs and trends in influenza-attributable mortality in four countries. In: Katz JM (ed) Options for the control of influenza VI, International Medical Press, London
Goodwin K, Viboud C, Simonsen L (2005) Antibody response to influenza vaccination in the elderly: a quantitative review. Vaccine 24:1159–1169
Langmuir AD, Henderson DA, Serfling RE (1964) The epidemiological basis for the control of influenza. Am J Public Health Nations Health 54:563–571
Govaert TM, Thijs CT, Masurel N, Sprenger MJ, Dinant GJ, Knottnerus JA (1994) The efficacy of influenza vaccination in elderly individuals. A randomized double-blind placebo-controlled trial. JAMA 272:1661–1665
Vallejo AN (2007) Immune remodeling: lessons from repertoire alterations during chronological aging and in immune-mediated disease. Trends Mol Med 13:94–102
Gross PA, Hermogenes AW, Sacks HS, Lau J, Levandowski RA (1995) The efficacy of influenza vaccine in elderly persons. A meta-analysis and review of the literature. Ann Intern Med 123:518–527
Jefferson T, Rivetti D, Rivetti A, Rudin M, Di Pietrantonj C, Demicheli V (2005) Efficacy and effectiveness of influenza vaccines in elderly people: a systematic review. Lancet 366:1165–1174
Vu T, Farish S, Jenkins M, Kelly H (2002) A meta-analysis of effectiveness of influenza vaccine in persons aged 65 years and over living in the community. Vaccine 20:1831–1836
Jackson LA, Jackson ML, Nelson JC, Neuzil KM, Weiss NS (2006) Evidence of bias in estimates of influenza vaccine effectiveness in seniors. Int J Epidemiol 35:337–344
Jackson LA, Nelson JC, Benson P, Neuzil KM, Reid RJ, Psaty BM, Heckbert SR, Larson EB, Weiss NS (2006) Functional status is a confounder of the association of influenza vaccine and risk of all cause mortality in seniors. Int J Epidemiol 35:345–352
Jefferson T (2006) Influenza vaccination: policy versus evidence. Br Med J 333:912–915
Bratzler DW, Houck PM, Jiang H, Nsa W, Shook C, Moore L, Red L (2002) Failure to vaccinate Medicare inpatients: a missed opportunity. Arch Intern Med 162:2349–2356
Fedson DS, Wajda A, Nicol JP, Roos LL (1992) Disparity between influenza vaccination rates and risks for influenza-associated hospital discharge and death in Manitoba in 1982–1983. Ann Intern Med 116:550–555
Örtqvist Å, Granath F, Askling J, Hedlund J (2007) Influenza vaccination and mortality: prospective cohort study of the elderly in a large geographical area. Eur Respir J 30:414–422
Keitel WA, Atmar RL, Cate TR, Petersen NJ, Greenberg SB, Ruben F, Couch RB (2006) Safety of high doses of influenza vaccine and effect on antibody responses in elderly persons. Arch Intern Med 166:1121–1127
Minutello M, Senatore F, Cecchinelli G, Bianchi M, Andreani T, Podda A, Crovari P (1999) Safety and immunogenicity of an inactivated subunit influenza virus vaccine combined with MF59 adjuvant emulsion in elderly subjects, immunized for three consecutive influenza seasons. Vaccine 17:99–104
Treanor JJ, Mattison HR, Dumyati G, Yinnon A, Erb S, O’Brien D, Dolin R, Betts RF (1992) Protective efficacy of combined live intranasal and inactivated influenza A virus vaccines in the elderly. Ann Intern Med 117:625–633
Reichert TA, Sugaya N, Fedson DS, Glezen WP, Simonsen L, Tashiro M (2001) The Japanese experience with vaccinating school children against influenza. N Engl J Med 344:889–896
Glezen WP (2006) Herd protection against influenza. J Clin Virol 37:237–243
Longini IM Jr, Halloran ME (2005) Strategy for distribution of influenza vaccine to high-risk groups and children. Am J Epidemiol 161:303–306
Monto AS, Davenport FM, Napier JA, Francis T Jr (1970) Modification of an outbreak of influenza in Tecumseh, Michigan by vaccination of school children. J Infect Dis 122:16–25
Halloran ME, Longini IM Jr (2006) Public health. Community studies for vaccinating school children against influenza. Science 311:615–616
Reichert TA, Sugaya N, Fedson DS, Glezen WP, Simonsen L, Tashiro M (2001) Vaccinating Japanese school children against influenza: author reply. N Engl J Med 344:1948
Uscher-Pines L, Omer SB, Barnett DJ, Burke TA, Balicer RD (2006) Priority setting for pandemic influenza: an analysis of national preparedness plans. PLoS Med 3:e436
Enserink M (2007) Data sharing. New Swiss influenza database to test promises of access. Science 315:923
Earn D, Dushoff J, Levin S (2002) Ecology and evolution of the flu. Trends Ecol Evol 37:334–340
Hope-Simpson RE (1992) The transmission of epidemic influenza. Plenum Press, New York
Thacker SB (1986) The persistence of influenza A in human populations. Epidemiol Rev 8:129–142
Ferguson NM, Galvani AP, Bush RM (2003) Ecological and immunological determinants of influenza evolution. Nature 422:428–433
Smith DJ, Lapedes AS, de Jong JC, Bestebroer TM, Rimmelzwaan GF, Osterhaus AD, Fouchier RA (2004) Mapping the antigenic and genetic evolution of influenza virus. Science 305:371–376
Plotkin JB, Dushoff J, Levin SA (2002) Hemagglutinin sequence clusters and the antigenic evolution of influenza A virus. Proc Natl Acad Sci U S A 99:6263–6268
Distribute Network. http://isds.cirg.washington.edu/distribute/index.php
New-York City Department of Health. http://www.nyc.gov/html/doh/downloads/pdf/cd/h1n1_citywide_survey.pdf
New-Zealand influenza surveillance. http://www.moh.govt.nz/moh.nsf/indexmh/influenza-a-h1n1-situation
Baker MG, Wilson N, Huang QS, Paine S, Lopez L, Bandaranayake D, Tobias M, Mason K, Mackereth GF, Jacobs M, Thornley C, Roberts S, McArthur C (2009) Pandemic influenza A(H1N1)v in New Zealand: the experience from April to August 2009. Euro Surveill 14(34):1–6
Fraser C, Donnelly CA, Cauchemez S, Hanage WP, Van Kerkhove MD, Hollingsworth TD, Griffin J, Baggaley RF, Jenkins HE, Lyons EJ, Jombart T, Hinsley WR, Grassly NC, Balloux F, Ghani AC, Ferguson NM, Rambaut A, Pybus OG, Lopez-Gatell H, Alpuche-Aranda CM, Chapela IB, Zavala EP, Guevara DM, Checchi F, Garcia E, Hugonnet S, Roth C, WHO Rapid Pandemic Assessment Collaboration (2009) Pandemic potential of a strain of influenza A (H1N1): early findings. Science 324(5934):1557–1561
Emanuel EJ, Wertheimer A (2006) Public health. Who should get influenza vaccine when not all can? Science 312:854–855
Gostin LO (2006) Medical countermeasures for pandemic influenza: ethics and the law. JAMA 295:554–556
Acknowledgments
We are enormously grateful to our many colleagues – nationally and internationally through the Multinational Influenza Seasonal Mortality Study network – for the many inspiring conversations we have had over the years about the “mysteries” of influenza epidemiology. We thank the Department of Health and Human Services OGHA and the Department of Homeland Security RAPIDD program for funding support. We also thank Marta Balinska who provided editorial assistance to this manuscript.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Birkhäuser Basel
About this chapter
Cite this chapter
Simonsen, L., Viboud, C., Taylor, R.J., Miller, M.A. (2011). The Epidemiology of Influenza and Its Control. In: Rappuoli, R., Del Giudice, G. (eds) Influenza Vaccines for the Future. Birkhäuser Advances in Infectious Diseases. Springer, Basel. https://doi.org/10.1007/978-3-0346-0279-2_2
Download citation
DOI: https://doi.org/10.1007/978-3-0346-0279-2_2
Published:
Publisher Name: Springer, Basel
Print ISBN: 978-3-0346-0278-5
Online ISBN: 978-3-0346-0279-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)