
Abstract
A positive association between dilated cardiomyopathy (DCM) and Lyme disease (LD) has been shown in several small observational studies in Europe but has not been replicated in North America. In previous studies, serological testing has been a limiting factor in establishing a causal link between LD and DCM. Many trials have relied on the more accurate endomyocardial biopsy (EMB) with PCR testing of tissue. Randomized controlled trials are required to determine if there is a benefit of antibiotics in addition to standard goal-directed medial therapy in the treatment of LD-associated DCM.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
When Lyme disease (LD) is not diagnosed or treated effectively with antibiotics during the initial weeks of infection, the bacteria Borrelia burgdorferi may result in manifestations of disseminated infection. In cases of early neurologic disease and LC, consequence of this may be seen in the first several months (Stage 2) following the original untreated infection. Late disseminated LD (Stage 3) may present clinically months or years after initial infection. It has been best documented in the skin (acrodermatitis chronica atrophicans in Europe) and in the joints (Lyme arthritis) [1].
Recently, there has been growing evidence that dilated cardiomyopathy (DCM) may be one of the late consequences of infection with LD and is covered in detail in Chap. 14 [2]. DCM is characterized by left ventricular or biventricular dilation with impaired myocardial contraction that is not explained by abnormal loading conditions such as hypertension, valvular disease, or coronary artery disease. Despite several studies showing a positive association between DCM and LD, and in some cases, improvement in cardiac function following the administration of antibiotics, research in this area has been done exclusively with small observational studies, that are underpowered and subject to confounding [2]. As such, routine testing for LD is not currently recommended in clinical guidelines for patients with idiopathic DCM [3]. There is significant potential for further research in this area to determine the true prevalence of Lyme-associated DCM and to assess whether there is a role for antibiotics in its treatment.
2 Discussion
Studies out of Europe have shown an association between B.burgdorferi and DCM, via endomyocardial biopsy (EMB) (tissue staining, immunohistochemistry, PCR) and serological testing, as well as improvement in cardiac function on echocardiography after antibiotic administration [4,5,6,7,8,9,10]. Based on these studies, the prevalence of LD amongst patients with DCM is estimated to be 20–26% [4,5,6,7,8,9,10]. These findings were not replicated in a single North American study, which failed to show both an association between DCM and LD or any statistically significant improvement in cardiac function on echocardiography, in a small number of patients treated with antibiotics [11]. This study however relied on clinical characteristics and serology rather than EMB used in many of the European studies. The clinical presentation, severity and virulence of LD differ between North American and European species of B.burgdorferi sensu lato, so it is possible that DCM is not a common manifestation of North American species [12]. Unfortunately, there is not enough data to support this hypothesis.
There are many challenges to studying LD in patients with idiopathic DCM. The accuracy of diagnostic tests in late disseminated disease remains uncertain. Early studies used ELISA testing, which has a sensitivity of around 50% in the early phases of disseminated LD and in the post-treatment phase [2, 13]. Many of the studies discussed above have included EMB specimens, which can be used to directly visualize spirochaetes and inflammation [2]. EMB in combination with western blot and qualitative serum PCR has the highest positive predictive value for B.burgdoferi; however EMB is an invasive procedure, not free of complications, and can be limited by sampling error [14].
Serum antibody testing is very sensitive in patients with extracutaneous manifestations, such as LC; therefore, seronegativity to immunoglobulin G (IgG) in untreated patients essentially rules out LD, if there is no humoral immunodeficient state [3]. Current guidelines from the Infectious Disease Society of America (IDSA) recommend a standard 2-tiered testing protocol (STTT), in which an enzyme immunoassay (EIA) or indirect florescent antibody test (IFA) is followed by antibody (IgM, IgG) immunoblots [3]. Alternatively, two different EIAs can be performed without the use of immunoblot testing [3]. One of the challenges with this method is that it can be difficult to determine when the initial infection occurred, as IgM and IgG for B.burgdorferi can persist for years after eradication of the infection [3]. Cross-reactivity can occur with antibodies to other microbes, which can also cause a false positive result [3].
Another consideration is that medial therapy for DCM has improved significantly since the publication of these observational studies on the topic of DCM and LD. Any clinical study performed to assess the benefit of antibiotics in patients with DCM and positive Lyme serology, would need to be a randomized controlled trial to determine if any measured improvement in cardiac function was secondary to the administered antibiotics or due to guideline-directed medical therapy (GDMT) alone. Additionally, there is uncertainty regarding the recommended length of antibiotics in this population. Current guidelines from the IDSA recommend ceftriaxone intravenously for 14–21 days for patients with neurologic LD and refractory Lyme arthritis [3]. Studies that have tried to treat presume Lyme-associated DCM have used a similar course of antibiotics to the IDSA guidelines with mixed results, with two studies administering intravenous ceftriaxone for 14 days and four studies administering intravenous ceftriaxone for 21 days [2]. Longer courses of antibiotics have not been shown to incur benefit and may be associated with an increased risk of side effects [15].
It is worth considering that when there is cardiac colonization, an exaggerated immune response occurs leading to cardiac injury. Animal models have shown transmural inflammation with infiltration of myocytes and lymphocytes, regardless of the presence of spirochaetes, with a predilection for perivascular regions [16]. It is possible therefore that DCM is the result of immune-mediated damage rather than ongoing active infection. In these cases, antibiotics would not be an effective treatment option for these patients.
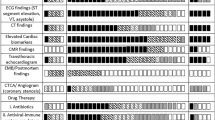
Our lab is in the process of finalizing a research proposal to explore this association in more detail. LD is endemic in our region of southeastern Ontario and therefore, we would be able to facilitate a study with adequate power to measure an association more accurately [2]. In addition to establishing the true prevalence of Lyme-associated DCM, our study will establish whether there is any noticeable improvement in symptoms, echocardiographic parameters and MRI imaging following adequate treatment of Lyme disease in those who have highly suspected or possible Lyme-associated DCM (Fig. 1).

Recommended RCT algorithm for patients presenting with idiopathic DCM
3 Conclusion
The true prevalence of late disseminated LD amongst those presenting with idiopathic DCM in Lyme endemic regions is likely underreported and needs to be further assessed, especially in North America. In addition, randomized controlled trials are necessary to determine whether there is a role for antibiotics in addition to standard GDMT in patients with idiopathic DCM and suspected or possible late disseminated LD.
References
Skar GL, Simonsen KA. Lyme disease. StatPearls [Internet]. 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431066/#_NBK431066_pubdet_.
Motamed M, Liblik K, Miranda-Arboleda AF, Wamboldt R, Wang CN, Cingolani O, Rebman AW, Novak CB, Aucott JN, Farina JM, Baranchuk A. Disseminated Lyme disease and dilated cardiomyopathy: a systematic review. Trends Cardiovascular Med. 2022; [in press] https://doi.org/10.1016/j.tcm.2022.05.010.
Lantos PM, Rumbaugh J, Bockenstedt LK, Falck-Ytter YT, Aguero-Rosenfeld ME, Auwaerter PG, Baldwin K, Bannuru RR, Belani KK, Bowie WR, et al. Clinical practice guidelines by the infectious diseases society of America (IDSA), American academy of neurology (AAN), and American college of rheumatology (ACR): 2020 guidelines for the prevention, diagnosis and treatment of lyme disease. Clin Infect Dis. 2021;72:e1–48.
Gasser R, Fruhwald F, Schumacher M, Seinost G, Reisinger E, Eber B, et al. Reversal of Borrelia burgdorferi associated dilated cardiomyopathy by antibiotic treatment? Cardiovasc Drugs Ther. 1996;10:351–60.
Klein J, Stanek G, Bittner R, Horvat R, Holzinger C, Glogar D. Lyme borreliosis as a cause of myocarditis and heart muscle disease. Eur Heart J. 1991;12(Suppl D):73–5.
Stanek G, Klein J, Bittner R, Glogar D. Borrelia burgdorferi as an etiologic agent in chronic heart failure? Scand J Infect Dis Suppl. 1991;77:85–7.
Karatolios K, Maisch B, Pankuweit S. Suspected inflammatory cardiomyopathy. Prevalence of Borrelia burgdorferi in endomyocardial biopsies with positive serological evidence. Herz. 2015;40 Suppl 1:91–95.
Bartunek P, Gorican K, Veiser T, Táborský M, Hulínská D. Significance of Bor-relia infection in development of dilated cardiomypathy (a pilot study). Prague Med Rep. 2007;108:339–47.
Kuchynka P, Palecek T, Havranek S, Vitkova I, Nemecek E, Trckova R, et al. Re-cent-onset dilated cardiomyopathy associated with Borrelia burgdorferi infec-tion. Herz. 2015;40:892–7.
Palecek T, Kuchynka P, Hulinska D, Schramlova J, Hrbackova H, Vitkova I, et al. Presence of Borrelia burgdorferi in endomyocardial biopsies in patients with new-onset unexplained dilated cardiomyopathy. Med Microbiol Immunol. 2010;199:139–43.
Sonnesyn SW, Diehl SC, Johnson RC, Kubo SH, Goodman JL. A prospective study of the seroprevalence of Borrelia burgdorferi infection in patients with severe heart failure. Am J Cardiol. 1995;76:97–100.
Yeung C, Baranchuk A. Diagnosis and treatment of lyme carditis. J Am Coll Cardiol. 2019;73(6):717–26.
Kubánek M, Šramko M, Berenová D, Hulínská D, Hrbáˇcková H, Malušková J, et al. Detection of Borrelia burgdorferi sensu lato in endomyocardial biopsy specimens in individuals with recent-onset dilated cardiomyopathy. Eur J Heart Fail. 2012;14:588–96.
Cooper, LT, Baughman, KL, Feldman, AM. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, American College of Cardiology, and European Society of Cardiology. Endorsed by the heart failure society of America and heart failure association of the European society of cardiology. J Am Coll Cardiol. 2007;50:1914–31.
Krause PJ, Bockenstedt LK. Lyme disease and the heart. Circulation. 2013;127:e451–4.
Cadavid D, Bai Y, Hodzic E, Narayan K, Barthold SW, Pachner AR. Cardiac involvement in non-human primates infected with the Lyme disease spirochete Borrelia burgdorferi. Lab Investig. 2004;84:1439–50.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Wamboldt, R., Aucott, J., Cingolani, O., Baranchuk, A. (2023). Into the Future: Research Prospects for Late Disseminated Lyme Carditis. In: Baranchuk, A., Wamboldt, R., Wang, C.N. (eds) Lyme Carditis. Springer, Cham. https://doi.org/10.1007/978-3-031-41169-4_17
Download citation
DOI: https://doi.org/10.1007/978-3-031-41169-4_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-41168-7
Online ISBN: 978-3-031-41169-4
eBook Packages: MedicineMedicine (R0)