
Abstract
Retinal laser is an essential tool in the treatment and prevention of retinal detachment (RD). Laser retinopexy to fuse the retina to the underlying retinal pigment epithelium and choroid by photocoagulation (PC) can prevent progression of retinal breaks to prevent rhegmatogenous RD (RRD), contain and confine smaller and slowly progressive RDs by laser PC demarcation of the advancing edge of the RD to prevent spread and preclude the need for major surgery. It also, serves as an essential tool for sealing retinal breaks during scleral buckling (SB) and/or pars plana vitrectomy (PPV), and can be used to create thermal choroidal perforations to facilitate external drainage of subretinal fluid during RD repair.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Retinal laser is an essential tool in the treatment and prevention of retinal detachment (RD). Laser retinopexy to fuse the retina to the underlying retinal pigment epithelium and choroid by photocoagulation (PC) can prevent progression of retinal breaks to prevent rhegmatogenous RD (RRD), contain and confine smaller and slowly progressive RDs by laser PC demarcation of the advancing edge of the RD to prevent spread and preclude the need for major surgery. It also, serves as an essential tool for sealing retinal breaks during scleral buckling (SB) and/or pars plana vitrectomy (PPV), and can be used to create thermal choroidal perforations to facilitate external drainage of subretinal fluid during RD repair. Laser retinopexy works only if the etiology of retinal detachment is rhegmatogenous. Alternative types of laser mechanisms have been used in exudative retinal detachments which are described in other chapters of this book. This chapter will describe processes and risk factors leading to rhegmatogenous retinal detachment formation and report published success rates in using laser retinopexy for rhegmatogenous RD.
The formation of retinal break leading to retinal detachment is usually preceded by the posterior vitreous detachment (PVD)—a separation of the posterior vitreous cortex from the internal limiting membrane of the retina which may be complete or partial [1]. The formation of vitreous traction at areas of significant vitreoretinal adhesion is responsible for most retinal breaks that lead to retinal detachment. Nearly 70% of the population develop a posterior vitreous detachment, but only about 4% of the population have retinal breaks [2]. Typical onset of PVD is between the ages of 45 and 65, however, the risk factors leading to earlier onset could be trauma and myopia. Other risk factors include aphakia, pseudophakia, cataract surgery, lattice retinal degeneration, uveitis, retinitis and hereditary vitreoretinopathies [3]. During the acute onset of PVD patients typically report the light flashes mainly in the dark. As the vitreous separates from the retina, photopsias are the result of vitreoretinal tractions. The vitreous opacities or floaters may be due to condensations of vitreous collagen, release the epipapillary glial tissues (Weiss ring) from the optic nerve head or blood from a damaged retinal vessel. At the time of the first examination about 8–22% patients with acute PVD symptoms will have a retinal tear [4,5,6]. If no retinal tears appear upon presentation of acute, symptomatic PVD, there is a 2–5% chance of a retinal tear in the subsequent weeks [5].
Retinal tears are full-thickness discontinuities in the neurosensory retina. Asymptomatic operculated holes and atrophic round holes have a very low risk of retinal detachment [7]. In eyes with symptoms of acute PVD, atrophic retinal breaks with clinical features have been found suggesting that they are unrelated to this acute condition. The literature provides little evidence of necessity for further laser treatment [8].
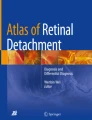
In symptomatic PVD, retinal tears associated with symptoms of floaters and/or photopsias are more likely to cause rhegmatogenous retinal detachment. A symptomatic retinal break is caused by vitreoretinal traction in eyes with an acute onset of PVD [9]. Untreated, symptomatic horseshoe tears are reported to lead to retinal detachment in 30–50% of cases. Retinal break features that are particularly high risk for progression to RD include breaks of acute onset, superior location, large size and surrounding subretinal fluid [10] (Fig. 9.1). Some breaks are associated with subclinical RD, which is defined as an extension of subretinal fluid at least 1 disc diameter away from the break but not more than 2 disc diameters posterior to the equator. Operculated retinal breaks have a low risk of progression to RD because the operculum represents relief of the vitreoretinal traction.

(Source Dr. Igor Kozak, Abu Dhabi, U.A.E.)
Ultra wide-field color fundus image of barrier laser surrounding a large peripheral retinal tear (white arrow). The condition has been stable for several years.
Retinal laser photocoagulation to surround a retinal break reduces progression to RD (Figs. 9.2 and 9.3). Laser treatment creates adhesions between the retina and retinal pigment epithelium and prevents migration of subretinal fluid [11, 12]. American Academy of Ophthalmology recommends prophylactic treatment of acute symptomatic horseshoe tears and dialyses, while leaving management options for acute symptomatic operculated holes, traumatic retinal breaks or asymptomatic retinal breaks to the treating physician’s decisions [9].

(Source Dr. Per Heuvels, Stade, Germany)
Laser retinopexy using navigated retinal photocoagulation. 2A—Peripheral fundus view showing a horseshoe tear with laser application pre-planning (blue dots, yellow circles represent protective zones). 2B—The same horseshoe tear following laser photocoagulation.

(Source Dr. Igor Kozak, Abu Dhabi, U.A.E.)
Ultra wide-field color fundus image of barrier laser surrounding a symptomatic operculated retinal break. The condition has been stable for one year.
Retinal detachment occurs in about 5% of eyes with symptomatic retinal breaks despite laser retinopexy. This can be caused by inadequate treatment to all margins of the break, subretinal fluid accumulation before chorioretinal adhesion from retinopexy is complete or because of missed or new breaks [2, 7, 8]. Subsequent retinal breaks occur after treatment of the first retinal break in 5–14% of eyes. Despite apparently adequate prophylactic treatment of retinal breaks, RD is diagnosed in 2–8.8% eyes [11, 12]. Nearly half of subsequent breaks occur within four to six weeks, but new breaks may occur months or even years later [13].
Lattice degeneration is a peripheral vitreoretinal degeneration characterized by retinal thinning, overlying vitreous liquefaction, and firm vitreoretinal adhesions at the margins of thinning. The incidence is about 6–8% of general populations and up to 30% of retinal detachments occur in these eyes; bilateral cases are seen in 45% [9]. Most lattice degenerations are ovoid, with the long axes of lattice running parallel to the ora serrata. Lattice lesions are usually localized between 11–1 o’clock and 5–7 o’clock meridians anterior to the equator [14]. Atrophic retinal holes can be localized in a lattice as a result of progressive retinal thinning [7]. Subsequently, retinal holes without posterior vitreous detachment, may develop in as many as 35% of these lesions and tends to occur in young myopic patients. Localized retinal detachments occur only in 2% of cases and, if they do become clinical, expand relatively slowly. The data from studies reported that the incidence of progression of lattice degenerations with or without round retinal holes to retinal detachment is very low in eyes without previous retinal detachment in fellow eye. Treatment is only recommended in cases of progressive retinal detachments [15].
Lattice can be associated with tractional retinal tears and treatment depends of the careful examination and patient history. In asymptomatic cases, prophylactic retinopexy is indicated in aphakic eyes, fellow eyes of patients with retinal detachment, eyes of patients with family history of retinal detachment. In symptomatic cases preventive treatment is indicated due to relatively high risk of progression to retinal detachment [16]. Bilateral incidence is reported in 45% of cases which open the debate whether to treat asymptomatic lattice prophylactically in the contralateral eye of a patient with history of lattice associated retinal detachment. The risk of retinal detachment in the contralateral eye is 5% (up to 25% in high myopic eyes with extensive lattice). To perform prophylactic retinopexy of lattice degeneration in fellow eyes may reduce the risk of RD two—to threefold, although this has been under discussion because new retinal breaks often develop in untreated areas or may occur at the edge of retinopexy scars if a posterior vitreous detachment occurs or extends [17, 18].
Degenerative (atrophic, senile) retinoschisis is generally benign and sometimes vision—threating. The schisis is characterized by smooth dome—shaped elevation of the retinal inner layers in the retinal periphery. The incidence is about 1% of the population and usually are bilateral located in inferotemporal quadrant. Outer wall breaks are usually large (greater than 3 disc diameters), round, located posteriorly, often with rolled edges [19]. If chronic, a ring of pigmentation can be found at the edge of subretinal fluid accumulation. In contrast, inner wall breaks are typically small and round [20]. Outer layer holes occur in approximately 17% and inner layer holes in less than 4% of cases. The large size and posterior location of outer wall breaks increase the amenability to laser prophylaxis, however, studies suggest that outer wall breaks usually remain stable [19, 20]. To develop progressive retinal detachment, (less than 2.5%), breaks should be found in both the inner and outer retinal layers. Prophylactic therapy (laser retinopexy) may not be beneficial, since the schisis may progress through the treated area or may develop in new areas. Treatment is indicated if patients have symptomatic, progressive RD [19,20,21].
Another risk factor leading to retinal detachment is a giant retinal tear, defined as a full-thickness neurosensory retinal break that extends 3 clock hours (90°) or more around the circumference of the globe and has rolled edges. Its incidence in large population—based studies has been estimated in 1.5% of rhegmatogenous retinal detachments, bilateral in 12.8% of cases. Most giant retinal tears are idiopathic—trauma, hereditary vitreoretinopathies and high myopia are less frequent causative factors. Non-traumatic giant retinal tears are often associated with a high rate of vitreoretinal pathology in the fellow eye. The incidence of retinal tears of fellow eyes is 59%, and the progression to retinal detachment is reported in nearly 18% [22]. Prophylactic treatment under these circumstances may be considered but there is no firm evidence of its efficacy at the present time. Similarly, a strong evidence is lacking whether prophylactic laser in infectious retinitis leads to prevention of retinal detachment and containment of retinitis spread.
Laser retinopexy is an outpatient procedure performed under local anesthesia with usually three rows of moderately visible laser spots surrounding the break (Figs. 9.1, 9.2 and 9.3). Follow-up examination takes place at an estimated formation of chorioretinal scarring (7–14 days) or earlier if visual symptoms worsen. Additional laser can be added with extension of the retinal tear or subretinal fluid increase. Laser retinopexy can be done using either slit-lamp delivery via contact lens or via indirect ophthalmoscope laser delivery. Intraoperative laser is performed at the time of pars plana vitrectomy surgery where both drainage retinotomy and peripheral retinal tears are surrounded by laser applications followed by intraocular endotamponade.
References
Johnson MW. Posterior vitreous detachment: evolution and role in macular disease. Retina. 2012;32(Suppl 2):S174–178.
Combs J, Welch R. Retinal breaks without detachment: natural history, management, and long-term follow-up. Trans Am Ophthalmol Soc. 1982;80:64–97.
Snead MP, Snead DR, James S, Richards AJ. Clinicopathological changes at the vitreoretinal junction: posterior vitreous detachment. Eye (Lond). 2008;22(10):1257–62.
Tani P, Robertson DM, Langworthy A. Rhegmatogenous retinal detachment without macular involvement treated with scleral buckling. Am J Ophthalmol. 1980;90(4):503–8.
Coffee RE, Westfall AC, Davis GH, Mieler WF, Holz ER. Symptomatic posterior vitreous detachment and the incidence of delayed retinal breaks: case series and meta-analysis. Am J Ophthalmol. 2007;144(3):409–13.
Benson WE, Grand MG, Okun E. Aphakic retinal detachment. Management of the fellow eye. Arch Ophthalmol. 1975;93(4):245–49.
Byer NE. Natural history of posterior vitreous detachment with early management as the premier line of defense against retinal detachment. Ophthalmology. 1994;101:1503–13.
Wilkinson CP. Interventions for asymptomatic retinal breaks and lattice degeneration for preventing retinal detachment. Cochrane Database Syst Rev. 2014(9):CD003170
Posterior vitreous detachment, retinal breaks, and lattice degeneration PPP—2019. American Academy of Ophthalmology. Updated October 2019. https://www.aao.org/preferred-practice-pattern/posterior-vitreous-detachment-retinal-breaks-latti Accessed 25 Feb 2022.
Mitry D, Singh J, Yorston D, et al. The fellow eye in retinal detachment: findings from the Scottish retinal detachment study. Br J Ophthalmol. 2012;96:110–3.
Smiddy WE, Flynn HW, Nicholson JR, et al. Results and complications in treated retinal breaks. Am J Ophthalmol. 1991;112:623–31.
Blindbaek S, Grausland J. Prophylactic treatment of retinal breaks - a systemic review. Acta Ophthalmol. 2015;93:3–8.
Goh YW, Ehrlich R, Stewart J, et al. The incidence of retinal breaks in the presenting and fellow eyes in patients with acute symptomatic posterior vitreous detachment and their associated risk factors. Asia Pac J Ophthalmol (Phila.) 2015;4:5–8.6.
Foos RY, Simons KB. Vitreous in lattice degeneration of retina. Ophthalmology. 1984;91:452–7.
Byer NE. Long-term natural history of lattice degenerations of the retina. Ophthalmology. 1989;96:1396–401.
Silva RE, Blumenkraz MS. Prophylaxis for retinal detachment. American Academy of Ophthalmology. https://www.aao.org/munnerlyn-laser-surgery-center/prophylaxis-retinal-detachments. Accessed March 2022.
Chauhan DS, Downie JA, Eckstein M, et al. Failure of prophylactic retinopexy in fellow eyes without a posterior vitreous detachment. Arch Ophthalmol. 2006;124:968–71.
Robertson DM, Norton EW. Long-term follow-up of treated retinal breaks. Am J Ophthalmol. 1973;75:395–404.
Byer NE. Long-term natural history study of senile retinoschisis with implications for management. Ophthalmology. 1986;93:1127–36.
Reed DC, Gupta OP, Garg SJ. Managing complications of retinoschisis. Retin Today. 2014;November/December:32–39.
Okun E, Cibis PA. The role of photocoagulation in the management of retinoschisis. Arch Ophthalmol. 1964;72:309–14.
Freeman HM. Fellow eyes of non-traumatic giant retinal breaks. In: Ryan SJ, editors. Retina, vol. 3. St. Louis: Mosby;2001. p. 2366–70.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Stefaničková, J., Kozak, I. (2023). Laser Treatment in Rhegmatogenous Retinal Detachment. In: Grzybowski, A., Luttrull, J.K., Kozak, I. (eds) Retina Lasers in Ophthalmology. Springer, Cham. https://doi.org/10.1007/978-3-031-25779-7_9
Download citation
DOI: https://doi.org/10.1007/978-3-031-25779-7_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-25778-0
Online ISBN: 978-3-031-25779-7
eBook Packages: MedicineMedicine (R0)