
Abstract
The recent 11th revision of the International Classification of Diseases and Related Health Problems (ICD-11) has met with great interest around the world. As the most widely used classification system globally, as approved by the World Health Organization, the changes will have direct implications for clinicians and researchers in the field of child psychology. This chapter focuses on the history and development of the ICD, and the changes made in this most recent revision, with a specific focus on the Mental, Behavioural, and Neurodevelopmental Disorders chapter. It also describes some of the key debates and commentary around the classification system and its revisions. The ICD-11 has a strong emphasis on clinical utility and is designed for use globally in multiple settings and by non-specialist health workers. Its development over many years, with large field trials involving practitioners from around the world, has resulted in a fit-for-purpose, dynamic, and comprehensive tool. The ICD-11 reflects the latest advances in psychiatric classification. It has been well-received by practitioners and is likely to play a significant role in the field of child psychology and the advancement of mental health worldwide.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- International Classification of Diseases (ICD-11)
- Psychiatric classification
- Clinical utility
- Global applicability
- Cultural sensitivity
- Mental health
Introduction
The International Classification of Diseases and Related Health Problems (ICD) is the foundation for the identification of health trends and statistics globally and the international standard for reporting diseases and health conditions (WHO, 2021). The 11th Revision of the ICD (ICD-11) has been approved by the World Health Organization (WHO) and has important implications for practice and research. The update and specifically the chapter on Mental, Behavioural and Neurodevelopmental Disorders is of great interest around the world (Reed et al., 2019).
The ICD has played a major role in modern psychiatric research and practice (Clark et al., 2017). Its unique vision and aim of developing a psychiatric nosology that has clinical utility and can be used globally in multiple settings and by non-specialist health workers is in line with the broader aims of WHO (Clark et al., 2017). The majority of the world’s population live in low and middle income countries (LMIC), and there is a strong emphasis on reducing the global burden of disease, particularly mental health which makes up 14% of that burden (MhGAP, 2021; Murray et al., 2020). The WHO Sustainable Development Goals and the WHO Mental Health Gap Action Programme (mhGAP) demonstrate the commitment of the global community and have been endorsed by all United Nations Member States (Patel et al., 2018). The ICD-11 is aligned with these efforts and represents the latest changes and advancements in the field of psychiatric classification with the aim of improving the delivery of primary health services globally.
This chapter is divided into four broad sections. The first will look at the origins, development, and future directions of ICD, and in particular, the chapter on MBND. This sets the ICD in context, noting its original development as a medical taxonomy under the instruction of the WHO. The classification system’s development and progress, from including psychiatric categories to its shift towards global applicability and accessibility, will be detailed. The extensive development process that brought about the ICD-11 and specifically the chapter on mental disorders, including carefully coordinated working groups and large, global field trials, are also described. The second section will outline the overall structure of the ICD-11, with an emphasis on the MBND chapter. With 28 chapters and around 55,000 categories, the ICD-11 has a particular focus on utility and application which is emphasized. The third section gives an overview of the key changes related to mental, behavioural, and neurodevelopmental disorders. Given the global aims of the ICD-11, it also explores cultural considerations in this latest iteration of ICD. The final section will explore the clinical utility of the ICD-11 in more detail and some of the key debates surrounding the MBND chapter. Considerations of the broad status of psychiatric nosology, as well as criticisms relating to the lack of etiological focus, overpathologizing of problems in living, reification, arbitrary thresholds, overlap with DSM-5, and artefactual comorbidity will be covered. The specific inclusion of gaming disorder in the ICD-11 will be used to demonstrate the challenges of including new classification categories because of its relevance to adolescent mental health. There will be a particular emphasis throughout the chapter on the features and diagnostic categories of interest to clinical child psychology.
ICD-11: Origins, Development, and Future Directions
The ICD-11 emerges from a history of nomenclature, nosology, and medical taxonomy. Under the instruction of the World Health Organization (WHO), the development process was extensive, with a lifespan of more than a decade. Issues of mental health have been routinely acknowledged in the ICD, with a designated chapter since the 1940s. Its development is best understood against the broader historical context of the ICD as a medical classification system. Its lineage is traced back to the sixteenth century (WHO, 2004), and the current working version is considered a dynamic and comprehensive tool which may be utilized across health disciplines, emphasizing clinical utility and global applicability.
This section outlines the origins of medical statistics as they are related to the overall development of the ICD, as well as the ICD’s multiple revisions throughout the twentieth century, with reference to considerations of mental health. The principal vision, development, processes, and implementation of the current revision, ICD-11, are provided. Development procedures and findings specifically related to the advancement of the current Mental, Behavioural and Neurodevelopmental Disorders (MBND) chapter are discussed, and consideration is given to future directions. This serves to situate the MBND chapter within the broader context of global health, an essential frame of reference when considering the psychological health of children.
Classifying Mortality: The Beginnings of the ICD
The first known statistical records of death originated in sixteenth century England, where deaths “from distinctly medieval purposes” were recorded on a weekly basis by the London Bills of Mortality (ICD-11, 2019, p. 2273). Pioneered by John Graunt, the bills were reported to have been collected and collated by parish clerks who had not necessarily been exposed to the practice of medicine, or statistics (Chute, 2000). Regarding medical classification, very little else was recorded until the mid-nineteenth century (WHO, 2004). Formal use of statistics is evidenced by reports and papers issued by the London Statistical Society from 1838, and the International Statistical Institute in 1853. This was indicative of the increasingly widespread use of statistics at that time, as well as the emergence of more precise data-gathering.
Considered to be the first medical statistician, William Farr, associated with the General Register Office of England and Wales, advocated for a uniform nosology based on statistical principles. His reports were influential, and at the first International Statistical Congress in 1853, he was tasked – alongside Marc d’Espine – with preparing a classification of death with international applicability. The anatomical basis of categories and general arrangement suggested by Farr and d’Espine influenced the ICD architecture.
A major development in the emerging field of medical statistics involved the International Statistical Institute’s collaboration with the Statistical Works for the City of Paris in 1891. Jacques Bertillon, a French statistician and social scientist, was tasked with the preparation of a comprehensive classification system to capture causes of death, with applicability to public health. The outcome of Bertillon’s efforts, known as the Bertillon International Classification of Causes of Death, was formally adopted by the International Statistical Institute in 1893 and was soon recognized by other countries. Under the jurisdiction of the International Statistical Institute, international revision conferences saw the first three iterations of the ICD developed in 1900, 1909, and 1920, respectively, each reflecting advances in medicine and involving an increasing number of international collaborators. Each version took on the standard title of the International Classification of Death (ICD). The brief involvement of the Health Organization of the League of Nations (post-World War I) contributed to the use of tabulation in the ICD, which reflected global developments in the field of statistics. The ICD-4 and -5 were published in 1929 and 1938, respectively.
From Death to Disease
In response to growing public health demands, the Fifth Decennial Revision Conference of the ICD in 1938 acknowledged the potential utility of classification beyond records of mortality. As a result, a resolution to develop a corresponding list of diseases was instated. The need to include morbidity had been identified through the administration of multinational surveys and so it became standard practice to formally engage an internationally representative committee, a gesture suggestive of the inclusive processes that remain today.
The notion that a list of diseases would be beneficial within the health professions was considered by Farr in the early nineteenth century. Further, in parallel to the globally accepted International Classification of Death, a Parisian classification of diseases had been in use since 1900. While there were some attempts to integrate non-fatal diseases into the ICD-4 in 1929, these categories were generally omitted in administrative practice due to the existence of localized morbidity lists.
The major turning point in the ICD’s implementation and development took place after World War II. The World Health Organization (WHO), founded under the jurisdiction of the United Nations in 1948, was granted responsibility for developing and maintaining the ICD; The recommendation to incorporate disease classifications into the ICD led to the International Classification of Diseases, Injuries, and Causes of Death, which was circulated to national governments. This was accepted at the first World Health Assembly in 1948, with the ICD-6, in the same year. The 6th revision comprised two volumes and included a chapter on psychiatric disorders. At this inaugural meeting, members were encouraged to establish national committees which would, in the future, contribute to the ongoing development and revision of the newly titled ICD.
ICD Revisions Under the Guidance of the WHO
The WHO released the ICD-7 in 1957, and the ICD-8 in 1968, setting a precedent for decennial revision (Janssen & Kunst, 2004). Between these revisions, the WHO’s Nomenclature Regulations, an international treaty instated in 1967, were endorsed. The Nomenclature Regulations mandated all WHO Member States to instate the most current version of the ICD (WHO, 2021). The implementation of the treaty secured the ICD’s status and function as a global communication tool which facilitates the collection of comparable health information (Clark et al., 2017).
The newly formed network of WHO member states, now committed to implementing the ICD, began to level criticism at the ICD, targeting its structure and utility. While the 9th revision (released in 1978) did not initiate structural changes, discussions regarding the future utility of the ICD were ongoing at the time of publication. The standard decennial revision of the ICD was determined to have an insufficient time period to facilitate adequate evaluation processes, leading to the decision to increase the preparation period leading up to the release of the ICD-10.
The ICD-10 was endorsed in 1990, and approved in 1992, but implementation was slow and inconsistent. The ICD-10 was updated almost yearly post-2000, with the most recent version released in 2019 (WHO, 2021). Initial work focused on remodelling the structure of the ICD and led to the WHO Family of International Classifications [FIC]. The ‘family’ is inclusive of several WHO-developed health and health-care system classification products, which may each be used independently or in conjunction with one another.
Mental Health Classification in the ICD
The ICD-6 chapter “Mental, Psychoneurotic, and Personality Disorders” (Clark et al., 2017) had a total of 26 categories that were put forward with suggested inclusion and exclusion terms. While the categories were broadly grouped into three clusters, no definitions or diagnostic guidelines were provided. As with the other sections of the ICD manual, the changes to this chapter between ICD-6 and ICD-7 were minimal.
Discussions regarding the inclusion of mental health within the ICD often invite comparison to the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM). This is due in part to the extensive collaboration between the WHO and American Psychiatric Association (APA) which led to a high level of consistency between the ICD-8 and the DSM-II, both of which identified psychoses, neuroses (including personality disorders), and “mental retardation” as the major categories for mental disorders. DSM-III included diagnostic criteria, and although these were included in ICD-10, DSM-III became more widely used for research and academic training purposes.
Following the release of the ICD-8, the WHO issued a glossary in which recognition of nosological problems within the psychiatric profession emerged. This was subsequently incorporated into the main statistical body in the ICD-9 (Clark et al., 2017; First et al., 2015). The glossary represented an important step towards the diagnostic guidelines included in later editions. DSM-III and DSM-III-R were developed independently of the WHO and ICD and reflected substantial changes with regard to disorder classification, namely a trend towards more thorough description. A more methodological approach was used to develop the DSM-IV and, apart from additional content, the edition was known for explicitly documenting its use of literature reviews, analysis, and field trials.
The publication of the ICD-10 marked an important step forward with the concurrent release of the ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines (CDDG), also known as “the blue book” (First et al., 2015). The CDDG expanded on the previous ICD glossary for mental disorders and was meant to provide diagnostic guidance to clinicians. However, the guidelines provided in the CDDG were often inconsistent in their level of detail, which impacted the CDDG’s utility in clinical practice – while it allowed for flexibility, this came at the cost of consistency and therefore, potential global validity (First et al., 2015). This aspect of the CDDG was identified as one of the main areas for revision in the ICD-11 and was informed by work on and discussion of the DSM-5.
For example, an important addition to the CDDG in the ICD-11 expands the previously named ‘mental retardation’ subdivision (now named ‘disorders of intellectual development’ and included under the Neurodevelopmental Disorders section) via the provision of guidelines which outline both intellectual and adaptive domains. Children are uniquely considered within the diagnostic guidelines for this category, distinct from adolescents and adults, reflective of the developmental approach adopted by the ICD-11 (Reed et al., 2019). The recognition of the differences in presentation of mental disorders across the lifespan – in which the mental health of children is carefully contemplated – is an important result of the extensive, decade-long development process outlined below.
ICD-11: Vision, Development, and Process
Vision
The current version of the ICD was built with the primary objective of overall utility, applicability, and accessibility. The final product needed to be user-friendly and appropriate for integration into the public health sector, while retaining statistical integrity and scientific credibility (Ustun & Jakob, 2009). The key settings identified for implementation included primary care, clinical care, research, and public health.
Development
At the outset of development, three broad phases were outlined (Ustun & Jakob, 2009). The first phase, labelled “ICD-10-Plus”, consolidated criticisms of the ICD-10, first combining all national modifications and other adaptations before inviting structured proposals for potential changes. The second phase saw the compilation of an “ICD-11 alpha draft”. This was compiled by WHO assigned editors and Topic Advisory Groups, who reviewed taxonomic rules, definitions, and diagnostic criteria. Upon completion, the third phase involved the use of a “ICD-11 beta draft” as a field-trial version. This early version of the ICD was tested for feasibility, reliability, and utility through the Global Clinical Practice Network (GCPN) and allowed for direct comparison with the ICD-10.
Process
To facilitate the revision of the ICD, the WHO established a comprehensive organizational structure which linked WHO headquarters to WHO’s member states. This included a Revision Steering Group, which oversaw the many Topic Advisory Groups (TAGs), each consisting of field experts aligned to each major domain of the classification (e.g., a TAG was responsible for Chapter 5). Each TAG established Working Groups as needed; the working groups were tasked with assessing diagnostic issues within their domain, through a process of review of published literature, revision of the ICD-10 diagnostic categories, and the address of public comments. Following this process, the revised category was then submitted for testing in field trials via the GCPN – an innovative and collaborative web-based platform where members of the WHO-FIC network, NGOs, and interested health professionals with relevant experience participated in quarterly surveys. The GCPN used surveys to collect data which captured how clinicians understood and used diagnostic codes and categories. These data informed the revision of diagnostic criteria, and subsequently became the platform through which systematic field trials which allowed comparison between ICD-10 and proposed ICD-11 diagnoses were implemented. This allowed for reliability, validity, and clinical utility to be tested.
Mental Health Classification: The Approach of ICD-11
Major changes in the MBND chapter included a review of chapter structure, the addition and relocation of diagnostic categories, and the standardization of the format of diagnostic guidelines (Gaebel et al., 2020). Part of the restructuring process involved the adoption of a developmental and ‘lifespan’ approach. Where previously the ICD structure had aligned itself with the one presented in Kraeplin’s seminal psychiatry textbook, the current version orders disorder categories from a developmental perspective, beginning with disorders most often diagnosed in childhood, and closing with disorders most often diagnosed in elderly populations (neurocognitive disorders) (Reed et al., 2018a, b). The official use of the term ‘neurodevelopmental’ is new to the ICD system, significant in its recognition of a group of chronic disorders which have a distinctly early onset and are characterized by lasting difficulties in both cognitive and social-communicate domains (Stein et al., 2020).
Regarding the clinical utility overall, both the core statistical chapter and the CDDG were revisited with a particular aim of enhancing clinical utility (IAG for Revision, 2011). The need for greater clinical utility was highlighted in two provisional surveys, in which only ~60% of mental health clinicians indicated routine use of classification systems, with practical references to the ICD-10 used predominantly for administration purposes (Evans et al., 2013; First et al., 2018). Other considerations identified by the IAG included the definition of mental disorders, the universality of categories, and the application of the system across contexts. The MBND chapter needed to be relevant to three stakeholder groups: governments and administrative bodies, mental health clinicians, and mental health service users and their families. The development process was based on the recommended ICD revisionary process, held the same organizational structure (namely TAGs and working groups), and included systematic literature reviews, country-level analysis, as well as international surveys of mental health professionals. An important function of the working groups was to use uniform ‘content forms’ in order to standardize the development of diagnostic descriptions for the CDDG (First et al., 2015).
Global collaboration for these processes was ensured through the creation of The Global Clinical Practice Network (GCPN) for mental health. The GCPN is considered the largest practice-based research network in global mental health. It is composed mostly of individual mental health practitioners, who are appropriately diverse and represent different professions (psychiatrists, psychologists, nurses, social workers, and occupational therapists), countries, years of experience, and professional contexts (Reed et al., 2015). As of February 2021, it included over 16,000 members from 160 countries (Socially Responsive Mental Health, 2021). Importantly, 40% of practitioners represent LMIC countries, 92% currently see patients, and a further 58% supervise others. This reflects the diversity of WHO member states, as well as the ICD’s global relevance. Registration for the web-based platform was made available in nine different languages.
The primary function of the GCPN so far has been the facilitation of various field trials, which have been utilized throughout all three major phases of development. The field trials included both internet studies and clinic-based studies and were internationally inclusive. The internet-based field studies (surveys) were administered via the Global Clinical Practice Network (GCPN) web platform and were helpful in understanding accuracy, consistency, and clinician diagnostic judgement of the ICD-10 criteria, and formative in revising the overall architecture of mental disorder classification (Reed et al., 2015). One of the major applications of the web-based studies was the review of the newly proposed diagnostic descriptions for implantation in the CDDG. In addition, clinic-based studies used the revised criteria to assess reliability, and clinical utility and applicability (see Reed et al., 2018a, b).
Noteworthy studies included an early project in which over 500 mental health professionals provided input regarding the ‘natural’ taxonomical use of mental health classification (see Reed et al., 2013). Data from experienced clinicians – representing the diversity of WHO member states – indicated a high level of consistency in taxonomical application, suggesting a surprising level of utility in both the ICD-10 and DSM-IV. In support of this finding, a larger study, the product of a collaboration between the WHO and the International Union of Psychological Science (IUPsyS), which exclusively examined the views of psychologists, went on to highlight specific diagnostic areas requiring attention, as well as issues regarding cross-cultural applicability (Evans et al., 2013). For example, controversies regarding what is currently reflected as autism spectrum disorder, as well as the then ‘hyperkinetic disorder’ (now attention deficit/hyperactivity disorder in both the ICD and DSM), were identified by psychologists as disorders which were problematic in both validity and utility (Evans et al., 2013).
ICD-11 Field Trials: Relevance for Children and Adolescents
The implementation of ICD-11 field trials was a protracted process which took place over several years. The initial published results have focused on disorders more commonly diagnosed in adulthood, including schizophrenia and schizoaffective disorders (Luciano et al., 2020; Petersen et al., 2019), personality disorders (Kim et al., 2014), gender identity diagnosis (Robles et al., 2016) as well as mood disorders, anxiety disorders, and disorders specifically related to stress (see Keely et al., 2016; Reed et al., 2018a, b). Clinical presentations of relational problems in adults have also been evaluated by mental health clinicians (Heyman et al., 2018).
The disorder categories listed above have received adequate yet limited attention in relation to childhood and adolescence. Relevant commentary has focused on gender incongruence in childhood (see Drescher et al., 2016) as well as early life complex post-traumatic stress disorder and the restructuring of oppositional defiant disorder. Issues related to gaming disorder are also addressed in this chapter.
Regarding ICD-11 specific field trials, an initial child and adolescent study examined diagnoses related to childhood chronic irritability and oppositionality (Evans et al., 2021). In this comprehensive study, the vignette methodology described by Evans et al. (2015) required clinicians to differentiate between chronic irritability and non-irritable oppositionality, episodic bipolar disorder, dysthymic depression, and ‘normative’ irritability in children. The results were formative in the decision to exclude the DSM-5’s DMDD and the reconfiguration of child oppositional and conduct disorders in the ICD-11. The impact of this field trial represents an important step forward in the nosology of this area of child functioning and highlights the utility of the field-trial methodology outlined in the ICD-11’s overall vision.
A number of independent studies which reference disorders in children also exist, but ultimately highlight the need for further field trials. For example, regarding trauma and stress disorders, the works of La Greca et al. (2017), Murphy et al. (2016), Perkonigg and colleagues (2016), as well as others provide helpful information regarding clinical utility of PTSD and the newly included Complex-PTSD. Yet nosologically, there are still limitations regarding these diagnoses (see Vasileva et al., 2018). Data from completed ICD-11 global field trials, including those that are relevant to disorders impacting on children and adolescents, continue to be processed and analysed. It is expected that results from these trials will be published and provide continued opportunity for refinement and increased understanding of these disorders.
Future Directions
Reception of the ICD-11 MBND chapter has been mostly positive, though not without criticism (Stein et al., 2020). The inclusivity of the revision process has integrated the many demands made of the ICD system, reflecting the aims of clinical utility and global applicability, yet ensuring scientific validity. Ongoing commentary and advances in psychiatric classification and nosology will continue to inform future revisions of the ICD, with hopes that models based on dimensional – rather than categorical – approaches will inform both structure and diagnostic description (Gaebel et al., 2020).
The ICD’s vision for the future is that it will remain a work in progress and always provide a global clinical utility which adequately reflects the most current knowledge base and advancements in the health professions. More immediately, issues of distribution, implementation, and adequate training will be prioritized, a process which is expected to be ongoing for several years. The WHO’s International Advisory Group will oversee this process: its role is to identify practical next steps and to facilitate operational management, as well to provide consultation for the development of additional resources (such as case books, primary care versions, and assessment tools). This includes mechanisms for evaluating the effectiveness of the MBND chapter and monitoring of implementation progress.
Training in the use of the ICD-11 MBND chapter is crucial in ensuring ongoing utility and is expected to take place both in-person and online. Due to the extent of the current network, this is expected to be a resource intensive project which may have difficulties in scaling. Also, concerns have been raised regarding accessibility. In response, a web-based training academy is currently being both developed and piloted. Development of the online training platform, Global Mental Health Academy – informed by experts – aims to utilize best practices in medical training and is based on the empirical data collected in the field studies referenced above. Upon its completion, it will be available to practitioners, who will receive certificates of completion for each module. The content of the online training is planned to be iterative and will reflect revisions to the ICD-11 as it continues to be developed and updated.
ICD-11: Overall Structure
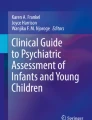
The ICD-11 consists of chapters, blocks, and categories arranged in a hierarchical manner which allows for different levels of detail to be communicated. This corresponds with the overall purpose of the ICD-11 – to classify diseases in a manner that is practical and clinically useful, while allowing statistical presentation of mortality and morbidity data for research, legislative, and other purposes. ICD-11 chapters are the top-level entities consisting of several categories which are arranged in a hierarchical manner within each chapter. A block is a group of related categories (World Health Organization, 2021) (Fig. 4.1).

A schematic representation of the ICD-11 showing the increase of detail in each level from the most general (chapter) to the most detailed (category) level
Categories included in the ICD-11 are mutually exclusive and cover the complete range of diseases or morbid conditions. Every disease or condition has a specific and well-defined place, or category, within the ICD-11 framework.
A health condition that meets classification criteria for a specific category is classified under that primary category (known as its primary parent). A unique feature of the ICD-11 is that it allows health conditions to be classified under secondary and even tertiary categories in different ICD-11 chapters. For example, Tourette’s syndrome’s primary classification is under Chapter 8 (Diseases of the Nervous System – Movement Disorders Grouping); it is however also classified under Chapter 6 (Mental, Behavioural and Neurodevelopmental Disorders – Obsessive-Compulsive Disorders Grouping and the Neurodevelopmental Disorders Grouping). Conditions that cannot be allocated to the specific categories are categorized in residual categories. Every category has a unique, alphanumeric code referred to as an ICD-11 code. Chapters and blocks do not have ICD-11 codes, and are therefore descriptive, and cannot be used for diagnostic purposes. For an entity to qualify as a category, certain criteria were considered during the development of the ICD-11. These include epidemiological evidence, clinical evidence, granularity (the level of detail reported and useful for a specific condition), continuity (relating to previous versions of the ICD), and parsimony (the need to describe and classify a condition in enough, but not excessive, detail) (World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health, 2021).
ICD-11 codes can be combined to describe a clinical condition in as much detail as needed. Additionally, unique identifiers can be assigned to category codes if a high level of granularity is necessary, or an ICD-11 category code can be used without identifiers to classify a condition in cases where detail is limited or not needed. The ICD-11 has 28 chapters and roughly 55,000 categories. Chapter 6 – Mental, Behavioural or Neurodevelopmental Disorders will be described in more detail.
The 23 groupings classified under the MNDB Chapter of the ICD-11 (Gaebel et al., 2017; Gozi, 2019; WHO, 2021) are as follows:
-
Neurodevelopmental Disorders. This grouping refers to disorders that arise during the developmental period and involve challenges with acquisition and performance of specific intellectual, language, motor, and social functions. Examples include autism spectrum disorders, disorders of intellectual development (previously mental retardation and disorders of psychological development), and attention deficit hyperactivity disorder (previously hyperkinetic disorder). This grouping considers presentation across the lifespan and includes indicators for different age groups (early childhood, childhood/adolescence, and adulthood), levels of severity, and adaptive functioning domains (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Schizophrenia and Other Primary Psychotic Disorders. This grouping includes conditions where psychosis is the primary or core feature. Disorders where psychosis are induced or affective (e.g. mood disorders or psychosis due to substance use) are classified elsewhere. Positive and negative symptoms should occur with sufficient intensity and frequency. Cultural norms are considered. Examples of Schizophrenia and Other Primary Psychotic Disorders include schizoaffective disorder, schizotypal disorder, and delusional disorder (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Catatonia is a condition of psychomotor disturbances such as mutism, stupor, posturing, negativism, and psychomotor agitation to name a few. Catatonia may occur in the context of other disorders such as mood disorders, schizophrenia, or neurodevelopmental disorders (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Mood Disorders, Including bipolar disorders and depressive disorders. The ICD-11 emphasizes the importance of a longitudinal pattern of a particular type of mood episodes over time. Examples of mood disorders include Bipolar or related disorder and Depressive disorder (Gaebel et al., 2017; Gozi, 2019; WHO, 2021)
-
Anxiety and Fear-Related Disorders are characterized by excessive fear and anxiety that results in significant functional impairment. Although fear and anxiety are closely related, they can be clearly differentiated. Fear can be described as a reaction resulting from an impending threat. Anxiety is more future-orientated and relates to a perceived rather than imminent threat. Examples are generalized anxiety disorder, panic disorder, and agoraphobia (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Obsessive-Compulsive and Related Disorders are characterized by repetitive thoughts and behaviours. Some disorders in the Obsessive-Compulsive and Related Disorders grouping include a cognitive component in the form of obsessions, intrusive thoughts, and preoccupations that is central to the condition. Examples are obsessive-compulsive disorder, body dysmorphic disorder, hypochondriasis, and olfactory reference disorder. Body-focused disorders lack a cognitive aspect and are characterized by recurring and habitual actions. Examples of body-focused disorders included are hair-pulling (trichotillomania) or skin-picking (excoriation disorder) (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Disorders Specifically Associated with Stress are related to exposure to traumatic or stressful events. An identifiable, causal stressor is necessary for each disorder categorized under this grouping. Examples are post-traumatic stress disorder, prolonged grief disorder, and adjustment disorder (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Dissociative Disorders, examples include dissociative neurological symptom disorder, trances disorder, and dissociative amnesia. These conditions are characterized by involuntary disruption or discontinuity of identity, sensations, perceptions, affects, thoughts, memories, control over bodily movements, or behaviour (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Feeding and Eating Disorders involve abnormal eating behaviours that are not developmentally appropriate and cannot be explained by an individual’s cultural context. Eating disorders involve preoccupations with food relating to body weight and body shape. Feeding disorders are not concerned with body shape and weight, for example eating non-food substances. Examples of eating disorders are anorexia nervosa, bulimia nervosa, and binge eating disorder. Pica and rumination-regurgitation disorder are examples of feeding disorders (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Elimination Disorders refer to repeated urination or defecation in inappropriate places after a developmental age when continence is expected. Enuresis after 5 years and encopresis after 4 years old are considered atypical. Elimination disorders may be present from birth or occur following acquired continence (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Bodily Distress Disorder involve disturbances in a person’s experience of their body. Examples are body integrity dysphoria and bodily distress disorder (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Disorders Due to Substance Use and Addictive Behaviours result because of substance use.
-
Impulse Control Disorders refer to disorders where an individual repeatedly fails to resist an impulse to perform an act that is harmful to either themselves or others. Examples are kleptomania and compulsive sexual behaviour disorder (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Disruptive Behaviour and Dissocial Disorders are characterized by persistent defiant, disobedient, provocative, or disruptive behaviours. These behaviours violate the rights of others and are not in line with societal norms, rules, or even laws. Examples include oppositional defiant disorder and conduct-dissocial disorder. The onset of these disorders is most often, but not always, during childhood (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Personality Disorders and Related Traits are characterized by dysfunctional patterns of behaviour relating to the self (e.g. identify, self-worth, or self-view) and/or interpersonal dysfunction (e.g. ability to form and maintain interpersonal relationships). The trait domain includes codes that can be assigned to describe prominent personality characteristic of an individual (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Paraphilic Disorders refer to persistent and intense patterns of atypical sexual arousal involving others who are not able or willing to consent. Examples are exhibitionistic disorder, voyeuristic disorder, or paedophilic disorder (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Factitious Disorders are characterized by intentionally feigning, falsifying, inducing, or aggravating medical, psychological, or behavioural signs and symptoms or injury in oneself or in another person (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Neurocognitive Disorders involve deficits in cognitive functioning that are not developmental but arise later in life and involve a decline in cognitive ability and function. Examples include delirium and dementia (Gaebel et al., 2017; Gozi, 2019; WHO, 2021).
-
Mental or Behavioural Disorders Associated with Pregnancy, Childbirth, or the Puerperium. These conditions develop following pregnancy, childbirth or the period after delivery, and can occur with or without psychosis. This category can be assigned with another mental disorder if symptoms meet diagnostic criteria for both categories.
-
Psychological and Behavioural Factors Affecting Disorders or Diseases Classified Elsewhere. This category pertains to psychological and behavioural factors affecting health conditions classified in another chapter. The psychological or behavioural factor should adversely affect the health condition classified elsewhere by, for example, influencing treatment and posing additional risk or exacerbating symptoms. This code should always be assigned with a code from another chapter/diagnosis.
-
Mental and Behavioural Disorders Associated with Disorders or Diseases Classified Elsewhere. Psychological or behavioural symptoms that are resulting from a health condition not classified under mental and behavioural disorders should be coded here. This category should be used with the diagnostic category for the underlying condition.
-
Other specified mental, behavioural or neurodevelopmental disorders.
-
Mental, behavioural or neurodevelopmental disorders unspecified.
Each grouping consists of categories arranged in a hierarchical manner. Table 4.1 illustrates the hierarchal categorization of two conditions, autism spectrum disorder and attention deficit hyperactivity disorder, that are categorized under the Neurodevelopmental Disorders grouping.
ICD-11: Overall Application
The ICD-11 is designed to be a versatile, user-friendly tool that can be used across a range of settings and speciality areas by a variety of people. An improvement that adds to the practical feasibility of the ICD-11 is the fact that it is completely digitalized and accessible free of charge online (WHO, 2021). This allows the ICD-11 to be used for many different purposes, including documenting causes of death, recording the incidence and prevalence of diseases, and documenting external causes of disease. The systematic, comprehensive design of the ICD-11 also allows for comparison of health data across different time frames and settings (countries, regions, cities, hospitals). Data gathered using the ICD-11 can be used by researchers, policy makers, clinicians, and financial decision-makers to identify health trends, make financing decisions, identify relevant research areas, and plan intervention strategies (Jones et al., 2018).
Clinical Descriptions and Diagnostic Guidelines for ICD-11 Mental, Behavioural, and Neurodevelopmental Disorders
To provide comprehensive guidelines for implementation in clinical practice, the WHO developed Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD-11 Mental, Behavioural and Neurodevelopmental Disorders. The CDDG version of the chapter contains detailed diagnostic guidelines for clinical application and is unique to the ICD-11 (Socially Responsive Mental Health, 2021; First et al., 2015; World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health, 2021). The format includes uniform categories of description in order to comprehensively comment on various features found across the presentation of health disorders.
The Clinical Descriptions and Diagnostic Guidelines for Mental, Behavioural and Neurodevelopmental Disorders contain the following eight sections for each disorder:
-
1.
Essential or Required Features are characteristics that a clinician could expect to see in all cases of a disorder. These are listed as a bulleted list of symptoms or characteristics in the CDDG. Although this bulleted list of essential or required features may appear like diagnostic criteria, it is used in a different manner and for a different purpose than diagnostic criteria found in the DSM-5 for example. Essential or required features are intended to provide clinicians with guidance when making a diagnosis. They do not include symptom counts or precise durations and therefore allow for more flexible clinical judgement regarding the presentation of an individual case (First et al., 2015; Socially Responsive Mental Health, 2021; World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health, 2021).
-
2.
Additional Clinical Features are clinical characteristics that are important and relevant to a specific health condition, but not necessary for diagnosis. This includes features and presentations of a disorder that are commonly associated with the specific disorder, but may or may not be present in a clinical case. These features are necessary to consider as they assist recognition of a condition when it can present in a variety of manners. Additional clinical features also need to be considered for clinical management and may assist in making a differential diagnosis (First et al., 2015; Socially Responsive Mental Health, 2021; World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health, 2021).
-
3.
The Boundary with Normality (threshold) section intends to help clinicians differentiate between symptoms that are clinically relevant and can be described as a disorder and subclinical symptoms that can be more accurately described as a variation of normal functioning, as opposed to a disorder. Different criteria apply to different health conditions. For example, in some cases the level of functional impairment or distress is used to distinguish disorder from non-disorder (First et al., 2015; Socially Responsive Mental Health, 2021; World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health, 2021).
-
4.
Course Features contain guidance on the typical prognosis or course the health condition is expected to run. This can include information about typical age of onset; whether the condition is persistent or episodic; duration of the condition; disorder progression or remission over time; and the relationship of the condition to life stressors and other disorders (First et al., 2015; Socially Responsive Mental Health, 2021; World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health, 2021).
-
5.
Developmental Presentation. Many mental, behavioural, and developmental disorders present somewhat differently in different developmental stages. The developmental presentation section describes how symptom presentation may differ across the lifespan and provides guidance on recognizing health conditions based on their presentation across developmental stages (First et al., 2015; Socially Responsive Mental Health, 2021; World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health, 2021).
-
6.
Culture-Related Features consider how features of a disorder may manifest in ways that are culturally specific. Taking culture-related features into consideration assists clinicians in making culturally informed and sensitive diagnosis (First et al., 2015; Socially Responsive Mental Health, 2021; World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health, 2021).
-
7.
The Gender-Related Features Section provides information about gender differences in symptom presentation; base rates of disorders; and in help-seeking behaviours.
-
8.
Boundaries with Other Disorders and Conditions (or Differential Diagnosis) describe characteristics that differentiate a specific disorder from a condition with similar features. In some cases, guidance is given regarding comorbidity and whether an additional diagnosis can be considered (First et al., 2015; Socially Responsive Mental Health, 2021; World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health, 2021).
The ICD-11 provides a common language and systematic classification system. The simplified coding structure of the MBND chapter adds to the clinical utility of the instrument.
Overview of Changes Related to Mental, Behavioural, and Neurodevelopmental Disorders in the ICD-11
The ICD-11 has received attention from mental health professionals across the globe. The chapter related to mental health in the ICD-11 was among the first truly global participatory processes in the area of mental health, as well as child and adolescent mental health more broadly (Gaebel et al., 2020). The inclusion of both mental health providers and users throughout the entire process of developing the classifications related to child and adolescent mental health made provision for applicability across the globe, scientific validity, and clinical utility (Gaebel et al., 2017, 2020).
The MBND chapter has broadly seen a number of changes (outlined in Table 4.2). One of the broad, overarching changes has been the extensive inclusion of 23 groupings related to mental health in the recent iteration of the ICD (see ICD-11: overall structure above), compared with the 11 groupings which were examined in the ICD-10 (Gaebel et al., 2017). The chapter structure of the ICD-11 has attempted to compliment the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), which was done through a collaborative process between the World Health Organization and the American Psychiatric Association (Gaebel et al., 2017; Reed et al., 2019). In addition to the chapter structure, diagnostic and disorder classification has been grouped according to common aetiology, pathophysiology, and phenomenology (Gaebel et al., 2017).
Discussions and Debates Related to Changes in the ICD-11
The updated version of the ICD-11 has seen numerous changes, particularly in the section related to the classification of mental and behavioural disorders for children and adolescents. Some of these are briefly outlined:
Neurodevelopmental Disorders
The ICD-11 introduced a new grouping on neurodevelopmental disorders, replacing this grouping where the ICD-10 made use of classifications such as ‘disorders of psychological development’ and ‘mental retardation’. Another key development and change seen within this specific grouping is that the ICD-11 recognizes that autism spectrum disorder and attention deficit hyperactivity disorder may co-occur in the same individual. This becomes important for treatment as children and adolescents with a diagnosis of autism spectrum disorder can benefit from treatment with the co-occurrence of attention deficit hyperactivity disorder, such as stimulant medication (Stein et al., 2020; Sturman et al., 2017). The recent ICD iteration also sees the amalgamation of diagnoses such as childhood autism, atypical autism, and Asperger syndrome as being categorized as autism spectrum disorder (Silleresi et al., 2020; Stein et al., 2020).
Disorders of Addictive Behaviours
The ICD-11 presents many clinically relevant changes related to addictive behaviours. The recent iteration of the ICD brings together substance use disorders under the category of addictive behaviours through the grouping of disorders due to substance use or addictive behaviours; mental health professionals have applauded the change in the recent iteration of the ICD as it resembles similar changes as seen in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, highlighting alignment between the two systems (DSM-5) (American Psychiatric Association, 2013). The ICD-11 also contributes to the conceptualization of disorders of addiction by recognizing a group of ‘disorders due to addictive behaviours’. These are associated with distress/dysfunction surfacing from repetitive rewarding behaviours rather than from the use of dependence-producing substances (Stein et al., 2020). An advance to this grouping is the inclusion of gambling disorder as well as gaming disorder that may be relevant to child and adolescent mental health, which is a new addition to the ICD-11 classification and can be considered as being related to both online and offline behaviour (Rumpf et al., 2018).
Highlighting New Additions to Mental Health in ICD-11
The MBND chapter has seen new additions to the diagnostic characteristics and guidelines in terms of the revised classification interaction. These new additions included the incorporation of Catatonia as an independent syndrome, as well as the inclusion of gaming disorder and complex post-traumatic stress disorder in the ICD-11. The 15 new additions to diagnosis and disorders related to mental health in the ICD-11 have been outlined by Gozi (2019) and Gaebel et al. (2017) and are outlined in Table 4.3.
Cultural Considerations
The latest iteration of the ICD-11 has brought about a number of new changes, developments, and advances which have prompted numerous debates and discussion. One area is cultural considerations related to the classification system. While it has given an opportunity for global engagement in its development, it is essential to note that child and adolescent mental health and psychopathology takes place within a particular environment that can act as a protective or a contributory factor to mental health disorders. Coupled with the environment is the importance of culture and cultural considerations, particularly related to mental health (Gureje et al., 2020).
Mood, anxiety, and stress-related disorders, for both child and adult mental health alike, are among the most common presentations in mental health services and among the disorders commonly impacted by cultural factors (El Khourv et al., 2020). To account for culture and promote cultural sensitivity in the ICD-11, field studies were conducted in multiple countries to ensure global utility and cultural awareness of child and adolescent mental health. These field studies included diverse settings, including countries such as South Africa, Mexico, Japan, Russia, and Brazil (El Khourv et al., 2020).
The ICD-11 provides an international classification framework for child and adolescent mental health practitioners which can aid in addressing the treatment gap between the need for and access to services but remains culturally sensitive as indicated by the global field studies. While the ICD-11 makes some provision for cultural consideration and sensitivity, having an international classification system which promotes clinical utility and considers all cultural factors in mental health decision-making may be difficult. Gureje et al. (2020) have alluded to the cultural considerations of the ICD-11, noting child and adolescent mental health practitioners have been provided guidance for considering contextual and cultural considerations. This aims to strike a balance between global classification of mental health and the pertinent clinical information which should be geographically and culturally relevant. Striving for cultural consideration and sensitivity is a daunting task for a global classification system; however, clinicians and practitioners should be aware of the complexity of these areas when acting in the best interest of both children and adolescents as users of mental health treatment and services.
Clinical Utility of ICD-11
Clinical utility is regarded as an important priority of the WHO ICD-11 (Clark et al., 2017; Reed et al., 2018a, b). Improving the clinical utility of the ICD-10 is regarded as a major orientating principle in its revision (Reed, 2010).
The WHO has provided a detailed definition of a classification system’s clinical utility based on earlier descriptions of the concept (First et al., 2004). In relation to the ICD classification of mental disorders, the clinical utility of a classification system, construct, or category depends on: (a) its value communicating (e.g. among practitioners, patients, administrators, families); (b) its implementation characteristics in clinical practice, which includes its goodness of fit (accuracy of description), its ease of use, and feasibility (e.g. how much time is required to use it); and (c) its usefulness in selecting interventions and in making clinical management decisions (Keeley et al., 2016; Reed et al., 2018a, b).
One of the critical objectives of the ICD-11 is to reduce the disease burden of mental and behavioural disorders by serving WHO Member States. This is emphasized by the International Advisory Group for the Revision of the ICD-10 Mental and Behavioural Disorders (2011) who state, ‘People are only likely to have access to the most appropriate mental health services with the conditions that define eligibility and treatment selection are supported by a precise, valid, and clinically useful classification system’ (p. 90).
ICD-11 revisions have sought to improve clinical utility with the understanding that this could improve public health (Keeley et al., 2016). If a system is not implemented or used extensively because it is not viewed as clinically useful by practitioners, this can impact in a number of ways. It will not generate valid data that can be used for health statistics; outcome evaluation at the individual level will be limited, resource allocation and needs assessment at the system level will be compromised, as will public health decision-making at many levels, including national and global (Keeley et al., 2016).
The ICD-11’s emphasis on clinical utility is based on the challenges faced in this area by previous classification systems. As described by multiple authors, including those involved in the development of the systems (e.g. DSM and ICD), there are several problems with clinical utility (Andreasen, 2007). Reed et al. (2013) describe four primary concerns based on the literature. First, many people with mental health needs meet criteria for more than one disorder (Kessler et al., 2005; Kreuger & Bezdjian, 2009; Krueger et al., 2003). This may indicate that current classification systems are not efficiently capturing the core elements of mental disorders as they present in clinical settings (Reed et al., 2013). Second, a large proportion of mental disorders are recorded as either ‘Not Otherwise Specified’ (DSM terminology) or ‘Unspecified’ (ICD). This could indicate that current diagnostic categories are not easily understood by professionals or not accurately descriptive of patients. It may also reflect that the finer descriptions of diagnoses are not regarded as clinically useful by clinicians. Third, diagnostic categories are often poor predictors of treatment needs, particularly for those with severe forms of mental disorders. This is despite specific diagnoses often being used to define service eligibility. Existing diagnostic systems do not assist with the efficient use of often limited treatment resources, at either a clinical or country level (Reed et al., 2013). Finally, certain psychological and pharmacological treatments are effective over a range of mental disorders (e.g. Barlow et al., 2004; Harvey & Gumport, 2015). This suggests that several diagnostic distinctions currently made have limited relevance for clinical practice. In other instances, some disorders are significantly heterogenous, for example, the DSM-5 criteria for conduct disorder require only 3 of 15 possible criteria. Thus, for some disorders, it is possible that individuals with the same diagnosis will not share overlapping clinical features which have direct implications for treatment. These significant challenges in previous classification systems raise concerns about their increasing complexity and clinical utility. The ICD-11 revision has aimed to directly address these challenges.
As described in earlier sections of this chapter, the WHO Department of Mental Health and Substance Abuse conducted major field studies for ICD-11 which focused on improving clinical utility (Reed et al., 2018a, b). The subsequent substantive changes to the Clinical Description of Diagnostic Guidelines (CDDG) for ICD-11 Mental, Behavioural and Neurodevelopmental Disorder are intended for use by mental health professionals in clinical settings. Three main changes sought to improve clinical utility. First, providing consistent and uniform diagnostic information across categories (First et al., 2015). Second, allowing for appropriate clinical judgement and reducing arbitrary cut-offs when not strongly supported by evidence. And finally, the groupings and categories are intended to be more consistent with how mental disorders are conceptualized by clinicians (Reed et al., 2013; Roberts et al., 2012).
There is good evidence that these changes have been favourably received by clinicians. In a paper by Reed and colleagues (2018a, b), the clinical utility of the ICD-11 mental, behavioural and neurodevelopmental disorders diagnostic guidelines was assessed by 339 clinicians in 1806 patients in 28 mental health settings in 13 countries. They found very positive overall clinician ratings for the proposed ICD-11 diagnostic guidelines. The guidelines were regarded as easy to use, corresponded closely to patients’ presentations (i.e. ‘goodness of fit’), were clear and understandable, gave an appropriate level of detail, took a reasonable amount of time (i.e. about the same or less the clinicians’ usual practice), and gave useful guidance in distinguishing normality from disorder. While clinicians rated the guidelines as less useful for assessing prognosis and treatment selection than for communicating with other professionals, all the ratings were nonetheless positive. Though every effort has been made to improve the clinical utility of the ICD-11, and early indications are positive that they have done so, it remains to be seen how the revisions will be taken up as the classification system is implemented globally.
Criticisms and Commentary on ICD-11
While some of the criticisms of ICD-11 relate to the larger status of nosology in psychiatry, others relate to more specific elements of the ICD-11, including the MBND chapter (Stein et al., 2015, 2020; Stein & Reed, 2019). This section will cover seven broad criticisms and attempts by ICD-11 to mitigate them. The status of psychiatric nosology, aetiology, overpathologizing of problems in living, reification, arbitrary thresholds overlap with DSM-5, and artefactual comorbidity will be covered in more detail. Finally, the specific case of gaming disorder will be used as an exemplar for controversies that can arise with the introduction of new disorders into classification system.
First, there are multiple classification systems, for example, ICD, DSM, Research Domain Criteria, and there is some debate regarding the need for more than one (Clark et al., 2017). Stein et al. (2020) argue that different systems are needed for differing purposes. For example, the ICD-11’s emphasis on clinical utility and global applicability is designed to ensure it would result in a classification system that is of value for global mental health, ultimately reducing the mental health treatment gap and burden of mental disorder globally.
Second, ICD-11 and DSM-5 have been criticized for not being etiologically based (Gitlin & Miklowitz, 2014); this reflects uncertainty about the psychobiological underpinnings of psychiatric disorders (Clark et al., 2017; Gitlin & Miklowitz, 2014; Drabrik & Kendall, 2010). Not only is there a growing awareness that mental disorders are multicausal, but they are also incompletely understood (Clark et al., 2017; Stein et al., 2020). The ICD-11, and specifically the chapter on Mental, Behavioural or Neurodevelopmental Disorders, acknowledges this complexity and includes aetiology in certain groupings that have similar underlying mechanisms (e.g. addictive behaviours). It further details some diagnoses based on specified causes (e.g. anxiety disorder due to a medical disorder or substance use). Finally, certain causal factors can be classified though they aren’t defined as disorders (e.g. chapter on Factors Influencing Health Status and Contact with Health Services) (Stein et al., 2020). Despite these efforts, the ICD-11 emphasizes the continuous need of careful individualized assessment that shows awareness of the multiple causal factors in mental illness and the consequent divergent range of interventions (Stein et al., 2020).
Another challenge for diagnostic systems is the difficulty of setting a proper balance between not overpathologizing human problems and being inclusive enough to ensure the treatment of suffering individuals (Frances, 2014; Gitlin & Miklowitz, 2014). There is a large literature on how nosologies have medicalized problems of daily life (Frances, 2014). On the other hand, it is key for disorders to be listed in ICD-11 to ensure clinical and public health attention.
A further consideration for diagnostic classification systems is that complex symptom profiles of individuals often do not fit neatly into diagnoses (Hyman, 2010). There is a danger that the reification of diagnostic categories may impede our deeper understanding of them (Hyman, 2010). Similarly, there is the temptation to inappropriately regard mental disorders as natural kinds (Stein et al., 2013). The ICD-11 (and the DSM-5) are fundamentally categorical in design in order to achieve the purposes for which they were developed: clinical communication, allocation of mental health resources, compilation of health statistics, etc. (Clark et al., 2017). To mitigate the potential for reification, ICD-11 uses clinical guidelines rather than pseudospecific criteria sets. In addition, ICD-11 has a more dimensional approach to a range of conditions, for example, personality disorders, schizophrenia, and other primary disorders. In disorders of intellectual development, ICD-11 also moved away from using cut off scores based on standardized tests of intellectual impairment. To determine the appropriate severity-based subcategory in the updated system, clinicians must make judgements on multiple dimensions, considering intellectual functioning and adaptive behaviour across domains of social, conceptual, and practical skills (Clark et al., 2017; ICD-11). While dimensions may have some disadvantages for clinicians, field studies of the ICD-11 indicate that clinicians do find the guidelines acceptable and at least as easy to use as more categorical systems (Keeley et al., 2016; Luciano et al., 2020; Volpe, 2017; Reed et al., 2018a, b). How these revisions are taken up and used more broadly and on a global scale will be determined as the classification system is more widely implemented.
The problem of drawing thresholds is a fraught issue in mental disorders, particularly given the concerns described of inappropriate over-medicalization (Stein et al., 2020). Thresholds in this case relate to both between mental disorders and between disorders and normality. Setting thresholds in mental health disorders is difficult for three primary reasons: (1) the definition of mental disorder is under debate, (2) mental disorders are multidimensional, and (3) there are significant clinical and social ramifications for thresholds of mental disorders (Clark et al., 2017). To manage the potential pitfalls of thresholds and in keeping with its primary goals, the ICD-11 describes the essential features of each disorder, providing guidance about the symptoms that clinicians can reasonably expect to find in cases of the disorder (First et al., 2015). This approach enables more flexible applications of clinical judgement while also allowing for cultural variation in symptom presentation. Unlike the DSM-5 criteria, the ICD-11 guidelines don’t contain precise symptoms counts, duration thresholds, or polythetic counts (e.g. a patient must have four of a list of seven symptoms). This puts particular emphasis on that distress and impairment that are associated with symptoms (Stein et al., 2020). Through these changes, the ICD-11 aims to support clinicians in identifying the diagnostic formulation that will be most useful in making treatment and management decisions (Clark et al., 2017). There may still be a temptation to reify the particular boundaries set, potentially overlooking the impact of subclinical presentations or underestimating the resilience of individuals meeting clinical thresholds (Stein et al., 2020).
There is a perennial challenge of comorbidity in the classification of mental disorders. As the current classification systems are not completely based on causality, there is the potential for artefactual comorbidity. Multiple diagnoses in an individual may be the result of an underlying dysfunction rather than an actual range of separate disorders with underlying psychological processes involved (Stein et al., 2020). The ICD-11 CDDG has taken a pragmatic approach to comorbidity and uses the term ‘co-occurrence’. It has viewed the assignment of multiple diagnostic codes as sometimes necessary to accurately describe complex clinical conditions (Clark et al., 2017). The ICD-11 also has significantly fewer exclusions rules, although it does note some. For example, developmental language disorder with impairment of pragmatic language should not be diagnosed in the presence of ASD (WHO, 2021). This clinically focused approach by the ICD-11 has the clear advantage of addressing an individual’s most prominent concerns. This is consistent with Wilk et al.’s (2006) findings that practicing clinicians often focus on the more problematic aspects of a symptom picture and tend not to document all possible comorbid disorders of an individual patient. On the other hand, it has been argued that the ICD-11 emphasis on primary conditions and utility does have the disadvantage that clinically important comorbid conditions could be overlooked (Clark et al., 2017).
Similarities and Differences with DSM-5
By design, there are many similarities between the DSM-5 and ICD-11. The broad groupings they contain and the order of these groupings resulted from a series of meetings between the APA (who oversee the DSM) and the WHO (Clark et al., 2017). Both systems used a model of working groups to oversee revisions and the ICD-11 working groups, which were developed later, typically included one or more members from parallel DSM-5 groups to facilitate harmonization. Despite their revisions, both remain categorical classification systems and are fundamentally descriptive in nature (Clark et al., 2017).
While there are many similarities, there are a number of distinct differences which are notable. ICD-11 coding is mandated globally and ICD guidelines are therefore used by clinicians around the world. By contrast, DSM is more widely used by researchers, because of its more specific operational criteria. A survey of close to 5000 international psychiatrists in 44 countries reported that 70% used the ICD-10 system in their everyday work, with only 23% using DSM-IV (Reed et al., 2011). Many countries, and WHO member states, have integrated ICD in policies and clinical processes relating to social services, care coverage, and disability benefits (International Advisory Group for the Revision of ICD-10 Mental and Behavioural Disorders, 2011). In addition, WHO member states are now responsible for reporting health statistics (e.g. prevalence, causes of mortality and morbidity) based on ICD to WHO.
Relating to more specific differences in classification between DSM and ICD, the ICD-11 gender identity disorders are substantially revised and renamed to ‘gender incongruence’ (see Reed et al., 2016 for further discussion). Particularly in relation to children, disruptive behavioural and dissocial disorders and impulsive control disorders are grouped in separate chapters, but combined in DSM-5. Complex-PTSD and prolonged grief disorder were recommended for inclusion in ICD-11, but not included in DSM-5. Conversely, DSM-5 has included disruptive mood dysregulation disorder while this is not in ICD-11. Finally, in relation to approaches to comorbidity, there is substantial similarity between the two systems, though the more specified criteria of DSM-5 can perhaps lead more individuals to have multiple diagnoses (Clark et al. 2017; First et al., 2021).
Gaming Disorder
Gaming disorder is a new addition to the ICD-11 and provides a useful exemplar for controversies that can arise with new diagnostic categories. A widely cited article in a peer reviewed journal by a group of authors in the field (Aarseth et al., 2017) reflected their concerns about including gaming disorder. Five main concerns were, (1) that there is low quality of research supporting its inclusion, (2) the operationalization leans heavily on the criteria of other, traditional addictive disorders, (3) there is little consensus among scholars on the symptomatology and assessment of the problem behaviours, (4) concerns around the stigmatization and potentially forced treatment of healthy ‘gamers’, and that (5) such false-positive cases would hinder research needed to better understand the phenomenology of problematic gaming.
A response paper by Kirӑly and Demetrovics (2017) reviewed the concerns raised by Aarseth and colleagues and submitted that on balance there were more advantages than disadvantages to the inclusion of Gaming Disorder (Billieux et al., 2021). The authors address all five of the original paper’s concerns; for brevity, only three will be reviewed here. Kirӑly and Demetrovics agreed that while the overall quality of research in the field requires improvement (e.g. there are few clinical and longitudinal studies, and survey studies are overrepresented), the qualitative studies there clearly demonstrate that a minority of gamers experience significant functional and psychological impairment related to their excessive gaming. This, they conclude, establishes with certainty that the problematic behaviour exists (King et al., 2019).
In reference to the suggestion that there is little consensus among scholars on the symptomatology, the authors argue that the gaming disorder criteria comprise only the less-debated criteria (behavioural salience, losing interest in, and reducing other recreational activities) and those with strong general support (loss of control continuation of the playing behaviour despite negative consequences, and risking relationships and opportunities). However, work on the ICD-11 revision has given impetus to review the evidence and obtain consensus (Castro-Calvo et al., 2021).
Finally, Kirӑly and Demetrovics (2017) address concerns that the inclusion of gaming disorder may stigmatize millions of healthy gamers and could contribute to treatment of many false-positive casers. They contend that moral panic and stigmatization is more likely to originate from media scaremongering and generation gaps (e.g. mentality of younger and older generations) than the existence of a formal diagnosis. They conclude that a formal diagnosis might decrease stigmatization by regarding problematic gaming not as a personal weakness or bad character but rather as a disorder in the same way depression is considered a disorder rather than laziness. However, others have emphasized the public health benefits of including gaming disorder in the ICD-11 (Stein et al., 2018).
The inclusion of gaming disorder is one of several new disorders in the MBND chapter of ICD-11. Each has met with differing amounts of controversy and critique as might be expected. As Kirӑly and Demetrovics conclude, ‘the definitions of mental disorders are the products of temporary consensuses among professionals and as such they are dynamically changing entities, there will be the possibility to smoothen or modify the criteria in the future based on new empirical results.’ (Kirӑly & Demetrovics, 2017; Stein et al., 2021).
Conclusion
The ICD-11 represents an important advance in psychiatric nosology and global mental health. While there are clear debates around psychiatric nosology broadly and some of the specific revisions in ICD-11, it nonetheless reflects a step forward for psychiatric classification and is likely to impact widely on clinical practice. Three critical advancements are raised by Stein and Reed (2019). First, the ICD-11 has drawn on key strengths of the DSM and other classification systems like the Research Domain Criteria Project. In particular, ICD-11 emphasizes that nosological decision-making should be underpinned by evidence. Close collaboration between DSM-5 developers and ICD-11 Working Groups ensured neuroscience influenced decisions around the structure of the classification systems and that broadly similar structures were adopted (Clark et al., 2017; Stein & Reed, 2019). Second, ICD is available freely across the globe, making it more likely that it will be used in a range of settings, improving diagnosis and treatment (Stein & Reed, 2019). Its emphasis on clinical utility and efforts to ensure it is user-friendly and suited for adoption by non-specialists in primary care settings globally further increases the likelihood it will assist in efforts to reduce the global burden of disease. There are significant implications for clinical child psychology practitioners with the introduction of new diagnoses (e.g. gaming disorder, complex post-traumatic stress disorder) and an emphasis on guidelines and clinical judgement rather than fixed criteria. Finally, despite its revisions, the ICD-11 has maintained its unique identity and vision as a fit-for-purpose instrument (Stein, 2013; Stein & Reed, 2019). Its focus on providing flexible guidance in an acceptable and feasible manner for clinicians in multiple settings makes it more likely to be implemented on a broad scale. While it is too soon to determine the impact ICD-11 may have on global health and its efforts to reduce burden of disease, it is likely to play a significant role in psychiatry, psychology, and the advancement of mental health worldwide.
Notes
- 1.
Much of this section has been adopted directly from the World Health Organization’s 2nd edition of the ICD-10 manual, which provides a comprehensive narrative of the ICD’s historical development. References to other sources are provided.
References
Andreasen, N. C. (2007). DSM and the death of phenomenology in america: an example of unintended consequences. Schizophr Bull, 33(1), 108–112.
Aarseth, E., Bean, A. M., Boonen, H., Colder Carras, M., Coulson, M., Das, D., Deleuze, J., Dunkels, E., Edman, J., Ferguson, C. J., Haagsma, M. C., Helmersson Bergmark, K., Hussain, Z., Jansz, J., Kardefelt-Winther, D., Kutner, L., Markey, P., Nielsen, R. K. L., Prause, N., Przybylski, A., Quandt, T., Schimmenti, A., Starcevic, V., Stutman, G., Van Looy, J., & Van Rooij, A. J. (2017). Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal. Journal of Behavioural Addictions, 6(3), 267–270.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing.
Barlow, D. H., Allen, L. B., & Choate, M. L. (2004). Toward a unified treatment for emotional disorders. Behavior Therapy, 35(2), 205–230.
Billieux, J., Stein, D. J., Castro-Calvo, J., Higushi, S., & King, D. L. (2021). Rationale for and usefulness of the inclusion of gaming disorder in the ICD-11. World Psychiatry, 20(2), 198–199.
Brewin, C. (2020). Complex post-traumatic stress disorder: A new diagnosis in ICD-11. BJPsych Advances, 26(3), 145–152.
Castro-Calvo, J., King, D. L., Stein, D. J., Brand, M., Carmi, L., Chamberlain, S. R., Demetrovics, Z., Fineberg, N. A., Rumpf, H., Yucel, M., Achab, S., Ambekar, A., Bahar, N., Blaszczynski, A., Bowen-Jones, H., Carbonell, X., et al. (2021). Expert appraisal of criteria for assessing gaming disorder: an international Delphi study. Addiction. https://doi.org/10.1111/add/15411
Chute, C. G. (2000). Clinical classification and terminology: Some history and current observations. Journal of the American Medical Informatics Association, 7(3), 298–303.
Clark, L. A., Cuthbert, B., Lewis-Fernández, R., Narrow, W. E., & Reed, G. M. (2017). Three approaches to understanding and classifying mental disorder: ICD-11, DSM-5, and the National Institute of Mental Health’s Research Domain Criteria (RDoC). Psychological Science in the Public Interest, 18(2), 72–145.
Drabick, D. A., & Kendall, P. C. (2010). Developmental psychopathology and the diagnosis of mental health problems among youth. Clinical Psychology: A Publication of the Division of Clinical Psychology of the American Psychological Association, 17(4), 272–280.
Drescher, J., Cohen-Kettenis, P. T., & Reed, G. M. (2016). Gender incongruence of childhood in the ICD-11: Controversies, proposal, and rationale. The Lancet Psychiatry, 3(3), 297–304.
El Khoury, J. R., Baroud, E. A., & Khoury, B. A. (2020). The revision of the categories of mood, anxiety and stress-related disorders in the ICD-11: A perspective from the Arab region. Middle East Current Psychiatry, 27, 7.
Evans, S. C., Reed, G. M., Roberts, M. C., Esparza, P., Watts, A. D., Correia, J. M., Ritchie, P., Maj, M., & Saxena, S. (2013). Psychologists’ perspectives on the diagnostic classification of mental disorders: Results from the WHO-IUPsyS global survey. International Journal of Psychology, 48(3), 177–193.
Evans, S. C., Roberts, M. C., Keeley, J. W., Blossom, J. B., Amaro, C. M., Garcia, A. M., et al. (2015). Vignette methodologies for studying clinicians’ decision-making: Validity, utility, and application in ICD-11 field studies. International Journal of Clinical and Health Psychology, 15(2), 160–170.
Evans, S. C., Roberts, M. C., Keeley, J. W., Rebello, T. J., de la Peña, F., Lochman, J. E., et al. (2021). Diagnostic classification of irritability and oppositionality in youth: A global field study comparing ICD-11 with ICD-10 and DSM-5. Journal of Child Psychology and Psychiatry, 62(3), 303–312.
First, M. B., Pincus, H. A., & Levine, J. B. (2004). Clinical utility as a criterion for revising psychiatric diagnoses. American Journal of Psychiatry, 161, 946–954.
First, M. B., Reed, G. M., Hyman, S. E., & Saxena, S. (2015). The development of the ICD-11 clinical descriptions and diagnostic guidelines for mental and behavioural disorders. World Psychiatry, 14(1), 82–90.
First, M. B., Rebello, T. J., Keeley, J. W., Bhargava, R., Dai, Y., Kulygina, M., Matsumoto, C., Robles, R., Stona, A., & Reed, G. M. (2018). Do mental health professionals use diagnostic classifications the way we think they do? A global survey. World Psychiatry, 17(2), 187–195.
First, M. B., Gaebel, W., Maj, M., Stein, D. J., Kogan, C. S., Saunders, J. B., Poznyak, V. B., Gureje, O., Lewis-Fernandez, R., Maercker, A., Brewin, C. R., Cloitre, M., Claudino, A., Pike, K. M., Baird, G., Skuse, D., Krueger, R. B., Briken, P., Burke, J. D., Lochman, J. E., Evans, S. C., Woods, D. W., & Reed, G. M. (2021). An organisation and category level comparison of diagnostic requirements for mental disorders in ICd-11 and DSM-5. World Psychiatry, 20(1), 34–51.
Frances, A. (2014). Saving normal: An insiders revolt against out-of-control psychiatric diagnosis, DSM-5, big pharma, and the medicalization of ordinary life. Harper Collins Publishers.
Gaebel, W., Zielasek, J., & Reed, G. M. (2017). Mental and behavioural disorders in the ICD-11: Concepts, methodologies, and current status. Psychiatria Polska, 51(2), 169–195.
Gaebel, W., Stricker, J., & Kerst, A. (2020). Changes from ICD-10 to ICD-11 and future directions in psychiatric classification. Dialogues in Clinical Neuroscience, 22(1), 7–15.
Gitlin, M. J., & Miklowitz, D. J. (2014). Psychiatric diagnosis in ICD-11: Lessons learned (or not) from the mood disorders section in DSM-5. The Australian and New Zealand Journal of Psychiatry, 48(1), 89–90.
Gozi, A. (2019). Highlights of ICD-11 classification of mental, behavioural and neurodevelopmental disorders. Indian Journal of Private Psychiatry, 13(1), 11–17.
Gureje, O., Lewis-Fernandez, R., Hall, B. J., & Reed, G. M. (2020). Cultural considerations in the classification of mental disorders: Why and how in ICD-11. BMC Medicine, 18, 25.
Harvey, A. G., & Gumport, N. B. (2015). Evidence-based psychological treatments for mental disorders: modifiable barriers to access and possible solutions. Behaviour Research and Therapy, 68, 1–12.
Heyman, R. E., Kogan, C. S., Foran, H. M., Burns, S. C., Slep, A. M. S., Wojda, A. K., et al. (2018). A case-controlled field study evaluating ICD-11 proposals for relational problems and intimate partner violence. International Journal of Clinical and Health Psychology, 18(2), 113–123.
Hyman, S. E. (2010). The diagnosis of mental disorders: The problem of reification. Annual Review of Clinical Psychology, 6, 155–179.
ICD-11. (2019, June 8). The Lancet, 393, 2275.
International Advisory Group for the Revision of ICD-10 Mental and Behavioural Disorders. (2011). A conceptual framework for the revision of the ICD-10 classification of mental and behavioural disorders. World Psychiatry, 10(2), 86–92.
Janssen, F., & Kunst, A. E. (2004). ICD coding changes and discontinuities in trends in cause-specific mortality in six European countries, 1950–99. Bulletin of the World Health Organization, 82, 904–913.
Jones, L. K., Pulk, R., Gionfriddo, M. R., Evans, M. A., & Parry, D. (2018). Utilizing big data to provide better health at lower cost. American Journal of Health-System Pharmacy: AJHP: Official Journal of the American Society of Health-System Pharmacists, 75(7), 427–435.
Keeley, J. W., Reed, G. M., & Roberts, M. C. (2016). Developing a science of clinical utility in diagnostic classification systems: field study strategies for ICD-11 mental and behavioural disorders. American Psychology, 71, 3–16.
Kessler, R. C., Chiu, W. T., Demler, O., Merikangas, K. R., & Walters, E. E. (2005). Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archive of General Psychiatry, 62(6), 617–627.
Kim, Y. R., Blashfield, R., Tyrer, P., Hwang, S. T., & Lee, H. S. (2014). Field trial of a putative research algorithm for diagnosing ICD-11 personality disorders in psychiatric patients: 1. Severity of personality disturbance. Personality and Mental Health, 8(1), 67–78.
King, D. L., & Potenza, M. N. (2019). Not playing around: Gaming disorder in the International Classification of Diseases (ICD-11). Journal of Adolescent Health, 64(1), 5–7.
King, D. L., Delfabbro, P. H., Deleuze, J., Perales, J. C., Kiraly, O., Krossbakken, E., & Billieux, J. (2019). Maladaptive player-game relationships in problematic gaming and gaming disorder: A systematic review. Clinical Psychology Review, 73, 101777.
Király, O., & Demetrovics, Z. (2017). Inclusion of Gaming Disorder in ICD has more advantages than disadvantages. Journal of Behavioral Addictions, 6(3), 280–284.
Krueger, R. F., & Bezdjian, S. (2009). Enhancing research and treatment of mental disorders with dimensional concepts: Toward DSM-V and ICD-11. World Psychiatry, 8(1), 3–6.
Krueger, R. F., Chentsova-Dutton, Y. E., Markon, K. E., Goldberg, D. P., & Ormel, J. (2003). A cross-cultural study of the structure of comorbidity among common psychopathological syndromes in the general health care setting. Journal of Abnormal Psychology, 107, 216–227.
La Greca, A. M., Danzi, B. A., & Chan, S. F. (2017). DSM-5 and ICD-11 as competing models of PTSD in preadolescent children exposed to a natural disaster: assessing validity and co-occurring symptomatology. European journal of psychotraumatology, 8(1), 1310591.
Luciano, M., Sampogna, G., & Del Vecchio, V. (2020). The Italian ICD-11 field trial: Clinical utility of diagnostic guidelines for schizophrenia and related disorders. International Journal of Mental Health Systems, 14, 4.
Mental Health Gap Action Programme (mhGAP). World Health Organisation. https://www.who.int/teams/mental-health-and-substance-use/mental-health-gap-action-programme. Accessed 10 Apr 2021.
Murphy, S., Elklit, A., Dokkedahl, S., & Shevlin, M. (2016). Testing the validity of the proposed ICD-11 PTSD and complex PTSD criteria using a sample from Northern Uganda. European Journal of Psychotraumatology, 7(1), 32678.
Murray, C., & GBD 2019 Risk Factors Collaborators. (2020). Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet, 396(10258), 1223–1249.
Patel, V., Saxena, S., Lund, C., Thornicroft, G., Baingana, F., Bolton, P., Chisholm, D., Collins, P. Y., Cooper, J. L., Herrman, H., Herzallah, M. M., Huang, Y., Jordans, M. J., et al. (2018). The Lancet Commission on global mental health and sustainable development. The Lancet, 392(10157), 1553–1598.
Perkonigg, A., Höfler, M., Cloitre, M., Wittchen, H. U., Trautmann, S., & Maercker, A. (2016). Evidence for two different ICD-11 posttraumatic stress disorders in a community sample of adolescents and young adults. European archives of psychiatry and clinical neuroscience, 266(4), 317–328.
Peterson, D. L., Webb, C. A., Keeley, J. W., Gaebel, W., Zielasek, J., Rebello, T. J., et al. (2019). The reliability and clinical utility of ICD-11 schizoaffective disorder: A field trial. Schizophrenia Research, 208, 235–241.
Reed, G. M. (2010). Toward ICD-11: Improving the clinical utility of WHO’s international classification of mental disorders. Professional Psychology: Research and Practice, 41, 457–464.
Reed, G. M., Correia, J., Esparza, P., Saxena, S., & Maj, M. (2011). The WPA-WHO global survey of psychiatrists’ attitudes towards mental disorders classification. World Psychiatry, 10, 118–131.
Reed, G. M., Roberts, M. C., Keeley, J., Hooppell, C., Matsumoto, C., Sharan, P., et al. (2013). Mental health professionals’ natural taxonomies of mental disorders: Implications for the clinical utility of the ICD-11 and the DSM-5. Journal of Clinical Psychology, 69, 1191–1212.
Reed, G. M., Rebello, T. J., Pike, K. M., Medina-Mora, M. E., Gureje, O., Zhao, M., Dai, Y., Roberts, M. C., Maruta, T., Matsumato, C., Krasnov, V. N., Kulygina, M., Lovell, A. M., Stona, A., Sharan, P., Robles, R., Gaebel, W., Ziesalsek, J., Khoury, B., De Jesus Mari, J., et al. (2015). WHO’s Global Clinical Practice Network for mental health. The Lancet Psychiatry, 2(5), 379–380.
Reed, G. M., Drescher, J., Krueger, R. B., Atalla, E., Cochran, S. D., First, M. B., et al. (2016). Disorders related to sexuality and gender identity in the ICD-11: Revising the ICD-10 classification based on current scientific evidence, best clinical practices, and human rights considerations. World Psychiatry, 15, 205–221.
Reed, G. M., Keeley, J. W., Rebello, T. J., First, M. B., Gureje, O., Ayuso-Mateos, J. L., Kanba, S., Khoury, B., Kogan, C. S., Krasnow, V. N., Maj, M., Jair de Jesus, M., Sharan, P., Stein, D. J., Zhao, M. Z., Akiyama, T., Andrews, H. F., Asevedo, E., Cheour, M., et al. (2018a). Clinical utility of ICD-11 diagnostic guidelines for high-burden mental disorders: Results from mental health settings in 13 countries. World Psychiatry, 17(3), 306–315.
Reed, G. M., Sharan, P., Rebello, T. J., Keeley, J. W., Elena Medina-Mora, M., Gureje, O., et al. (2018b). The ICD-11 developmental field study of reliability of diagnoses of high-burden mental disorders: Results among adult patients in mental health settings of 13 countries. World Psychiatry, 17(2), 174–186.
Reed, G. M., First, M. B., Kogan, C. S., et al. (2019). Innovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disorders. World Psychiatry, 18(1), 3–19.
Remberk, B., Szostakiewicz, L., Kalwa, A., Bogucka-Bonikowska, A., Borowska, A., & Racicka-Pawlukiewicz, E. (2020). What exactly is catatonia in children and adolescents. Psychiatria Polska, 54(4), 759–775.
Roberts, M. C., Reed, G. M., Medina-Mora, M. E., Keeley, J. W., Sharan, P., Johnson, D. K., Mari Jde, J., Ayuso-Mateos, J. L., Gureje, O., Xiao, Z., Maruta, T., Khoury, B., Robles, R., & Saxena, S. (2012). A global clinicians’ map of mental disorders to improve ICD-11: Analysing meta-structure to enhance clinical utility. International Review of Psychiatry, 24(6), 578–590.
Robles, R., Fresán, A., Vega-Ramírez, H., Cruz-Islas, J., Rodríguez-Pérez, V., Domínguez-Martínez, T., & Reed, G. M. (2016). Removing transgender identity from the classification of mental disorders: A Mexican field study for ICD-11. The Lancet Psychiatry, 3(9), 850–859.
Rumpf, H. J., Achab, S., Billieux, J., Bowden-Jones, H., Carragher, N., Demetrovics, Z., Higuchi, S., King, D. L., Mann, K., Potenza, M., Saunders, J. B., Abbott, M., Ambekar, A., Aricak, O. T., Assanangkornchai, S., Bahar, N., Borges, G., Brand, M., Chan, E. M., Chung, T., et al. (2018). Including gaming disorder in the ICD-11: The need to do so from a clinical and public health perspective. Journal of Behavioral Addictions, 7(3), 556–561.
Silleresi, S., Prevost, P., Zebib, R., Bonnet-Brihault, F., Conte, D., & Tuller, L. (2020). Identifying language and cognitive profiles in children with ASD via a cluster analysis exploration: Implications for the new ICD-11. Autism Research, 13(7), 1155–1167.
Socially Responsive Mental Health. (2021, March 13). Engagement and training of global mental health professionals in WHO’s ICD-11. Dr Tahilia J. Rebello [Video]. YouTube https://www.youtube.com/watch?v=NBoA_w3XzFA. Accessed 9 Apr 2021.
Stein, D. J., Lund, C., & Nesse, R. M. (2013). Classification systems in psychiatry: diagnosis and global mental health in the era of DSM-5 and ICD-11. Current opinion in psychiatry, 26(5), 493–497.
Stein, D. J., Billieux, J., Bowden-Jones, H., et al. (2018). Balancing validity, utility and public health considerations in disorders due to addictive behaviours. World Psychiatry, 17(3), 363–364.
Stein, D. J., & Reed, G. M. (2019). Global mental health and psychiatric nosology: DSM-5, ICD-11, and RDoC. Brazilian Journal of Psychiatry, 41(1), 3–4.
Stein, D. J., He, Y., Phillips, A., Sahakian, B. J., Williams, J., & Patel, V. (2015). Global mental health and neuroscience: Potential synergies. Lancet Psychiatry, 2, 78–85.
Stein, D. J., Szatmari, P., Gaebel, W., Berk, M., Vieta, E., Maj, M., de Vries, Y. A., Roest, A. M., de Jonger, P., Maercker, A., Brewin, C. R., Pike, K. M., Grilo, C. M., Fineberg, N. A., Briken, P., Cohen-Kettenis, P. T., & Reed, G. M. (2020). Mental, behavioral and neurodevelopmental disorders in the ICD-11: An international perspective on key changes and controversies. BMC Medicine, 18(1), 1–24.
Stein, D. J., Palk, A. C., & Kendler, K. S. (2021). What is a mental disorder? An exemplar-focused approach. Psychological Medicine, 51(6), 894–901.
Sturman, N., Deckx, L., & van Driel, M. L. (2017). Methylphenidate for children and adolescents with autism spectrum disorder. Cochrane Database of Systematic Reviews, 11, CD011144.
Ustun, T. B., & Jakob, R. (2009). The overall development of ICD-11. Psychiatric Diagnosis: Challenges and Prospects, 8, 233–246.
Vasileva, M., Haag, A. C., Landolt, M. A., & Petermann, F. (2018). Posttraumatic stress disorder in very young children: Diagnostic agreement between ICD-11 and DSM-5. Journal of Traumatic Stress, 31(4), 529–539.
Veale, D., Gledhill, L. J., Christodoulou, P., & Hodsoll, J. (2016). Body dysmorphic disorder in different settings: A systematic review and estimated weighted prevalence. Body image, 18, 168–186.
Volpe, U. (2017). The development of the ICD-11 chapter on mental disorders. South African Journal of Psychiatry, 23, a1105.
Wilk, J. E., West, J. C., Narrow, W. E., Marcus, S., Rubio-Stipec, M., Rae, D. S., et al. (2006). Comorbidity patterns in routine psychiatric practice: Is there evidence of under-detection and under-diagnosis? Comprehensive Psychiatry, 47, 258–264.
World Health Organization. (2004). ICD-10: International statistical classification of diseases and related health problems: tenth revision (2nd ed.).
World Health Organization. (2021). International statistical classification of diseases and related health problems (ICD). https://www.who.int/standards/classifications/classification-of-diseases
World Health Organization & WHO collaborating Centre for Capacity Building and Training in Global Mental Health. (2021). Training course on ICD-11 guidelines for mental, behavioural, and neurodevelopmental disorders. https://gmhacademy.dialogedu.com/icd11
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Dawson-Squibb, JJ., Davids, E.L., Viljoen, M., Rice, K., Stein, D.J. (2023). The WHO International Classification of Diseases 11th Revision (ICD-11). In: Matson, J.L. (eds) Handbook of Clinical Child Psychology. Autism and Child Psychopathology Series. Springer, Cham. https://doi.org/10.1007/978-3-031-24926-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-031-24926-6_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-24925-9
Online ISBN: 978-3-031-24926-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)