
Abstract
Muscle injuries are very frequent in athletes, and despite their high incidence, advances in clinical diagnostic criteria, imaging, management, and rehabilitation strategies are still debated in literature. The diagnosis of muscle injury is mainly based on history and clinical examination. The examiner should start with a precise history of the circumstances surrounding the injury, before reviewing the player’s symptoms and identifying any previous related injury problems. When making a diagnosis, the first step is to differentiate between injury categories, indirect or direct muscle injuries. In a contusive injury, pain onset is usually immediate, the insult is direct, and symptoms increase in association with size and entity of the hematoma. The active range of motion is reduced, and the athlete cannot continue to train and compete. When functional disability appears early, a new assessment is recommended after 24 h to better define the injury. In nonstructural injuries, athletes complain of soreness, heaviness, and stiffness of the muscle, usually increasing with exercise, at times present at rest. On palpation, it is possible to appreciate stiffness of some bundles. It is important to distinguish these injury types because they have different prognoses, causing different absences. This chapter discusses the main principles of the physical evaluation of muscle injuries, including relevant imaging modalities in context.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Muscle injuries are among the most frequent injuries in sport, accounting for up to one-third of all sports-related injuries; they are responsible for 25% of days of absence away from training and competition [1]. Despite their considerable impact, there is still a lack of high-quality studies evaluating their specific control [2]. This entity is common, often occurring during sports practice, affecting the athlete’s functional capacity and ability to continue [3].
Athlete’s return to competition and injury prevention are the physician’s main goal. The clinical evaluation and imaging information is crucial to dictate prognosis [3]. Since the 1980s, availability of ultrasound (US) and magnetic resonance imaging (MRI) has been permitting direct visualization of muscle tears, resulting in appreciable tools to confirm and address the extent of muscle injuries helping to lead the management [2].
Despite the recognition of many risk factors and prevention protocols, muscle injuries have been increasing over the last 12 years. Therefore, it is necessary to enhance our knowledge based on clinical experiences and supported by scientific evidence about this issue [4].
2 Epidemiology
Muscle injuries are frequent in high-demand sports, accounting for 10–55% of all acute sports injuries [5]. In view of all damaging consequences, this current scenario causes a necessity for better comprehension of muscle tears and specially their prevention has turned a considerable challenge to the sports medicine centers all over the world [4].
Regarding professional soccer players, muscle injuries represent 31% of all injuries and are responsible for 25% of days of absence from training and competition [5]. The majority of muscle injuries (92%) affect the lower extremity involving the four major muscle groups: hamstrings, adductors, quadriceps, and calves, with the hamstring injuries being the most common single type, representing 12–37% of all [2, 4]. In addition, the incidence risk of muscle tears in this population is six times higher during match play compared to training. Age represents another attribute involved with muscle injuries; the increase occurs in players aged over 30, emphasizing the sural triceps [4, 5].
In other modalities, the incidence of muscle injuries is variable: 16% in running sports, 11% in rugby, and 18% in basketball. In all these sports, the main affected muscles are the hamstrings, quadriceps, and adductors [5].
3 Etiology
The main function of skeletal muscle is to perform as the “motor” driving the muscle-tendon-bone unit, producing movement and locomotion. This unit is an extraordinarily organized complex of tissues consisting of the following: the muscle; the myotendinous junction, where muscle fibers interdigitate with collagen, allowing force to be transferred from the muscle to the tendon; the tendon, which may be at the ends of and/or within the muscle; the enthesis, where the tendon attaches to the bone; and the bone [3].
The injury therefore depends on the impact intensity, state of contraction of the muscle, traumatic moment, and muscle injured. Muscle injuries usually occur in the eccentric phase of the muscle contraction after an indirect insult, more common in noncontact sports, and after direct trauma, as in contact sports.
Trauma mechanisms can be divided into direct and indirect forms. The former indicates that the muscle is damaged directly by an externally applied force, such as contusion or penetration. In contrast, the indirect form refers to muscle trauma that occurs secondary to a nonphysiologically or abrupt elongation. Whereas the direct type of injury typically results in hemorrhage, hematoma, and/or laceration of the target muscle, the indirect type commonly results in muscle strains or tears. The direct injury mostly occurs where the maximal external force is exerted, whereas the indirect type frequently takes place across the myotendinous junction of the affected muscles [5].
Direct muscle injuries are a commonplace in sports that involve frequent body contact, such as rugby, basketball, and soccer. However, indirect muscle injuries more often occur during activities in which the contracted muscles undergo excessive traction [6]. Muscle strain is the most common presentation of an indirect-type injury resulting from extravagant stretching of a shortened muscle.
The most prevalent location for muscle strain is the myotendinous junction, where the distal tendons are interwoven with the muscle fibers to relay contraction forces. The myotendinous junction (MTJ) reveals less capacity for energy absorption than muscle and tendon. In animal models, the average tension leading to MTJ failure is only 20% greater than the maximum isometric tension normally produced during activity [3, 6].
The MTJ is situated at a variable distance from the bone, and the tendinous portion located between the bone and the MTJ is named as the “free tendon.” Therefore, muscles with short free tendons, such as the deltoid and gluteus maximus, appear to insert virtually directly on the bone, whereas muscles such as the biceps brachii, rectus femoris, and plantaris have free tendons varying in length [3].
4 Physical Exam
Physical examination routine includes the inspection and palpation of the injured area and also function tests of the suspicious injured muscles both with and without resistance. The main objectives are to determine the precise location (region, muscle(s), tendon, or fascia involvement) and presume the severity of the injury. The diagnostic accuracy of the tests is quite variable; therefore, a bilateral comparison should always be performed to help the exam accuracy (Table 51.1) [4].
In the past, the earliest efforts to grade the severity of muscle injuries were based on the symptoms and signs present on physical exam and this evaluation composed the basis for grading a given injury as “mild,” “moderate,” or “severe” [7].
Many authors, since 1966, tried to better identify the severity of the injury considering diverse attributes such as the degree of pain, disability, swelling, ecchymosis, presence of a palpable defect or other features of the clinical history such as the type of trauma, ability to continue activity after the injury, and, not least of all, range-of-motion limitation and anatomic location of the tear in the muscle unit [1, 7].
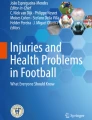
Generally, a grade I or “mild” muscle injury has been considered to correspond to stretching or minimal disruption of muscle fibers and a clinical presentation marked by minimal, well-localized pain, contracture and hemorrhage, minor disability, a full pain-free range of motion (or <10° ROM deficit), and ability to continue the sporting activity immediately after the injury. Grade II or “moderate” injury has been considered as a tear of a considerable number of muscle fibers but no complete muscle rupture; a more severe clinical presentation occurs when compared with the previous grade, represented by moderate pain, disability, painful range of motion (or 10–25° ROM deficit), and inability to continue the sporting activity. Grade III or “severe” injury has been defined to be a complete muscle rupture, with the worst clinical scenario, recognized by the athlete’s fall in pain immediately after the injury, more than 50% loss of motion (or <25° ROM), a rapid muscle circumference decrease of more than 12 mm when compared to the healthy contralateral muscle, diffuse pain, and hemorrhage (Figs. 51.1, 51.2, and 51.3) [7].

A 45-year-old male presenting with enlarging areas of ecchymosis over inner and posterior aspects of the right thigh after a long head biceps femoris injury; (a) clinical inspection (posterior view) of a large bruising on the inner and posterior aspects of the right thigh; (b) lateral view

Presence of a gap detected at physical examination in the place where the patient reports pain, featuring a more severe quadriceps muscle injury

A 32-year-old male soccer player presenting a distally retracted muscle belly after a subtotal muscle tear of the rectus femoris; (a) relax muscle; (b) active contraction for right-leg raises
All these clinical presentations and physician’s findings about the muscle injury described since the 1960s are estimated tools for an initial evaluation, mainly because of their reproducibility and simplicity, resulting in a quick approach. However, they were based only on specialist opinion and did not have a validated prognostic value [7].
Although the diagnosis is usually clinical, many physicians have an ultrasound in their office and this is especially important when the diagnosis is unclear, when recovery is taking longer than expected and when interventional or surgical management may be necessary [4]. It has advantages such as non-radiation, portability, excellent resolution of neuromuscular structures, and possibility for the examiner to perform dynamic examinations [6].
5 Classification
Over the last decade, the “Munich Muscle Injury Classification” was established by an international group of experts in sports medicine, establishing an alliance with the International Olympic Committee (IOC) and the Union of European Football Associations (UEFA) (Table 51.2) [7,8,9]. Magnetic resonance imaging (MRI) is a crucial exam to assess the degree of muscle injury.
This classification is characterized by two main branches according to the nature of the muscle trauma: direct or indirect. Additionally, indirect muscle injuries are subdivided into four types according to MRI appearance where types 1 and 2 represent MRI-negative functional disease, and types 3 and 4 represent structural injuries that can be classified as minimal (type 3a), moderate (type 3b), or complete (type 4) [7,8,9].
Key Points
-
Muscle injuries are among the most common injuries in sports and remain a notable issue since it causes competition time loss and a relatively high recurrence rate, despite all technological advances of science in this field.
-
Indirect muscle tear is related to muscle strain/stretching; the most common area injured is the myotendinous junction.
-
Direct muscle tear or muscle contusion is caused by a direct blow; the severity is determined by the force of impact, size of the striking body, and muscle’s state of contraction.
-
The examiner should start with a precise history of the circumstances surrounding the injury, before reviewing the symptoms and identifying any previous related injury problems.
-
The next step in diagnosis is a careful clinical examination of the injured area. This should include an inspection, palpation, a comparison with the contralateral side, and functional testing of the muscles.
-
The main purpose of the physical examination is to determine injury location and try to define severity. Acute injuries’ evaluation is often limited by pain, and accuracy of the tests is quite variable.
-
Diagnosis is based on history and meticulous clinical examination. Crucial imaging exams for evaluation are US and MRI. US is fast and cost effective, can offer a dynamic muscle assessment, and represents a good tool for serial evaluation to follow healing. MRI imaging is considered the gold standard method to assess the muscular architecture and to evaluate the extent of muscle injuries.
-
Classifications and grading systems are currently going through a continuous progression. Additional studies may help validate new grading systems to develop a universally applicable terminology with more clinical relevance.
References
Guermazi A, Roemer FW, Robinson P, Tol JL, Regatte RR, Crema MD. Imaging of muscle injuries in sports medicine: sports imaging series. Radiology. 2017;282(3):646–63.
Hamilton B, Valle X, Rodas G, Til L, Grive RP, Rincon JAG, et al. Classification and grading of muscle injuries: a narrative review. Br J Sports Med. 2015;49(5):306.
Flores DV, Gómez CM, Estrada-Castrillón M, Smitaman E, Pathria MN. MR imaging of muscle trauma: anatomy, biomechanics, pathophysiology, and imaging appearance. Radiographics. 2018;38(1):124–48.
Til L, Tol H, Bruce Hamilton E. Muscle injuries clinical guide 3.0. In: Muscle Injuries Clinical Guide 30; 2015. p. 1–60.
Buono D, Via G. Muscle injuries: a brief guide to classification and management. Transl Med UniSa. 2015;12(4):14–8.
Chang KV, Wu WT, Özçakar L. Ultrasound imaging and rehabilitation of muscle disorders: part 1. Traumatic injuries. Am J Phys Med Rehabil. 2019;98(12):1133–41.
Grassi A, Quaglia A, Canata G, Zaffagnini S. An update on the grading of muscle injuries. Joints. 2016;4(1):39–46.
Patel A, Chakraverty J, Pollock N, Chakraverty R, Suokas AK, James SL. British athletics muscle injury classification: a reliability study for a new grading system. Clin Radiol. 2015;70(12):1414–20. https://doi.org/10.1016/j.crad.2015.08.009.
Mueller-Wohlfahrt HW, Haensel L, Mithoefer K, Ekstrand J, English B, McNally S, et al. Terminology and classification of muscle injuries in sport: the Munich consensus statement. Br J Sports Med. 2013;47(6):342–50.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 ISAKOS
About this chapter

Cite this chapter
Kaleka, C.C., Andrade, P.H.C., Debieux, P., Yamada, A.F., Cohen, M. (2023). Evaluation of Muscle Injuries. In: Lane, J.G., Gobbi, A., Espregueira-Mendes, J., Kaleka, C.C., Adachi, N. (eds) The Art of the Musculoskeletal Physical Exam. Springer, Cham. https://doi.org/10.1007/978-3-031-24404-9_51
Download citation
DOI: https://doi.org/10.1007/978-3-031-24404-9_51
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-24403-2
Online ISBN: 978-3-031-24404-9
eBook Packages: MedicineMedicine (R0)