
Abstract
Perioperative management of the acute care surgical patient can present a complicated array of management decisions. Incorporating the principles of Advanced Trauma Life Support provides the surgeon with a consistent systematic approach for treatment. Identification of the different shock states and their management is key to caring for this often critically ill population. Utilization of current guidelines and protocols such as the Surviving Sepsis Campaign, Acute Respiratory Distress Syndrome Network, and massive transfusion protocols is crucial to optimize outcomes as well. Endpoints of resuscitation can help to guide the surgeon’s management and provide goals in the pre- and postoperative setting. These endpoints may require invasive procedures, and all have limitations that should be recognized.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The acute care surgeon will often face complex management decisions during the initial 72 h of treatment. The role of the surgeon remains undoubtedly central to navigating the patient through all phases of care into excellent outcomes. Through the process of surgical care, the patient’s physiology is taxed to tolerate the surgical insult and to heal the operative site. Optimization of the physiologic baseline thus becomes imperative to achieve successful outcomes. Preparing a patient for surgery and the immediate postoperative management can present a daunting array of physiologic and metabolic derangements. This endeavor can be overwhelming and circumstances may not allow for the immediate assistance of critical care consultants or other subspecialists. The emergent surgical and trauma patient requires attention to additional physiologic and biologic factors that must be addressed. Preoperative risk stratification and risk factor modification, while useful in elective surgery, may be of limited utility to the surgeon embarking on emergent intervention. However, several well-established guidelines, i.e., balanced resuscitation with massive transfusion protocol (MTP), Surviving Sepsis Campaign (SSC), and Acute Respiratory Distress Syndrome Network (ARDSnet), can be readily incorporated into this framework and assist the surgeon in preparation and resuscitation.
There are multiple approaches to the management and care of complex and critically ill patients. We have found that assessment mirroring that of the traumatically injured patient can be utilized in any patient, is pragmatic, and allows the surgeon to institute a thorough care plan throughout the perioperative timeframe.
A primary survey is performed, followed by a secondary survey where each body system is assessed, incorporating the physical exam, laboratory, and radiologic findings pertinent to that system. The management plan then follows to address any abnormalities of that system. This sequential approach allows for the assimilation of large amounts of data while minimizing the risk of missing critical information. What follows is a brief review of the shock states that may be encountered by the practicing general surgeon. Next is a summary of some of the common endpoints of resuscitation. These endpoints can be utilized throughout the perioperative course and serve to minimize injury to key organ systems. The challenge of this chapter is to provide a practical framework from which to assess and manage these most complex patients.
Learning Goals
-
Recognition and treatment of the common types of perioperative shock whenever present
-
Recognition and treatment of the multiple perioperative abnormalities that the emergency general surgeon and trauma surgeon may encounter
-
Early identification of physiological derangements of the different organ systems and their timely correction
-
Awareness of endocrine emergencies and appropriate corrective therapies
2 Shock Etiology
In the many scenarios facing the surgeon, none is more demanding than that dominated by the core physiological instability of the shock states. The ultimate recovery of the surgical patient hinges as much on the appropriate and timely interventions apt at restoring the physiologic integrity in the ICU as it does on appropriately planned and expeditiously performed procedures in the operating room. Cuthbertson in 1942 was the first to describe two distinct phases of the metabolic shift that occurs after major trauma and later recognized this to be a common denominator of all shock states [1]. He characterized “ebb” and “flow” phases of posttraumatic metabolic alterations. The “ebb” phase, early and shorter in nature, is associated with reduced total body expenditure and increased urinary nitrogen wasting in addition to a surge in the release of neuroendocrine hormones and an increased sympathetic flow response. In contrast, the “flow” phase occurs after resuscitation from a state of shock. This leads to increased metabolic turnover, activation of the innate immune system, and induction of the hepatic acute phase response.
Shock is defined as inadequate delivery of oxygen at the cell level with a secondary metabolic shutdown and eventual multiorgan dysfunction syndrome. Prompt recognition is the paramount first step in affording intervention towards mitigation and its early reversal. The acute care surgeon may encounter several types of shock, with septic and hemorrhagic as the most common. Lawrence categorizes shock as follows: [2].
Hypovolemic shock (hemorrhagic, nonhemorrhagic) results from reduced intravascular volume, leading to reduced preload and cardiac output (CO).
Distributive shock (septic, neurogenic, anaphylactic, adrenal crisis) results from excessive vasodilatation of the peripheral vasculature, leading to impaired distribution of blood flow.
Cardiogenic shock results from sudden failure of the cardiac pump function as seen in acute MI, valve rupture, or arrhythmias.
Obstructive shock results from impaired blood flow in the cardiopulmonary circuit. Common causes include tension pneumothorax, pericardial tamponade, and massive pulmonary emboli.
Structured scores and quality initiatives have been created to facilitate early recognition. Resuscitative endpoints, especially for the hemorrhagic and septic categories most crucial to the acute care and trauma surgeon, will be emphasized in this chapter.
3 Priorities and Endpoints of Resuscitation
No single endpoint exists to gauge successful physiologic resuscitation of the acutely ill. A complete discussion of the many parameters used as endpoints is beyond the scope of this chapter. Trending endpoints, as often as every 1–2 h, can guide titration of therapies for optimal outcome. Successful achievement is marked by elimination of acidosis with restoration of aerobic metabolism. Lactate and base deficit have both been shown to be useful in the initial quantification of the shock state and as a gauge to ongoing resuscitative efforts. Decreases in elevated lactate levels during treatment are universally associated with improved outcome in critically ill patients and can provide an early and objective assessment of the response to therapy [3]. Failure to decrease elevated lactate within 48 h correlates with increased mortality [4]. Persistent elevation in the base deficit (up to 96 h) is a marker for ongoing resuscitation requirements and can be present despite normalized vital signs and urine output. Of note, lactate levels can remain elevated in patients with impaired clearance such as liver dysfunction, cardiac surgery, and sepsis. Patients positive for alcohol and drugs may demonstrate elevations in both markers. Urine output as a marker of end organ perfusion remains one of the clinically reliable endpoints, though variable based on patient’s preexisting conditions. A urinary output of 0.5 cc/kg/h is a general threshold in the adult patient. Cardiac indices such as right ventricular end diastolic volume index (RVEDI) correlate best with cardiac preload, but requires placement of a pulmonary artery catheter. Evidence shows that interventions to increase RVEDI result in improved gut perfusion restoration and decreased rate of organ failure. The FloTrac™ device attaches to the arterial line to provide advanced hemodynamic parameters, including stroke volume (SV), stroke volume variance (SVV), mean arterial pressure (MAP), systemic vascular resistance (SVR), and continuous cardiac output (CCO). These parameters update every 20 s and do not require central venous catheterization, although the patient must be intubated. Point of care ultrasound (POCUS) has rapidly expanded our bedside diagnostic capability. It allows for noninvasive determination of preload through visualization of inferior vena cava diameter and right ventricular filling. This modality is subject to patient size, anatomy, and user expertise.
4 Primary Survey
History and physical exam are paramount in the initial evaluation of the acutely ill surgical patient. The “AMPLE” history as outlined in Advanced Trauma Life Support (ATLS) can identify key components essential to further management. Allergies with attention to anaphylactic reactions, IV contrasts, and antibiotic problems are most pertinent [5]. Medications with a focus on anticoagulants, cardiac, diabetic, and steroids are salient. Past medical and surgical history provides surgical context and helps to assess risk. Last oral intake relates to aspiration risk for intubation or possibly sedation if further diagnostic workup is contemplated, such as interventional radiologic procedures. Events in these patients would focus on the presentation, duration, onset, and severity of the illness.
4.1 Pulmonary
Assessment of the patient in need of intubation must be determined promptly. Usually, emergent endotracheal intubation is indicated in the following scenarios:
-
Hypoxemic respiratory failure despite maximum maneuvers such as noninvasive positive pressure support.
-
Hypercapnic ventilatory respiratory failure leading to respiratory acidosis and increased work of breathing.
-
Upper airway obstruction of the pharynx by the tongue or foreign body, or secretions or edema from massive resuscitation (i.e., burns).
-
Shock or hemodynamic instability associated with altered mental status and increased work of breathing.
-
Clinical conditions with risk for airway compromise such as stroke, Glascow Coma Scale (GCS) less than 8, drug overdose, or severe agitation preventing medical intervention.
Asking the patient to speak, auscultating the neck and chest, noting respiratory rate, and use of accessory muscles of breathing are fast and effective. Evaluation of pulse oximetry, CXR and arterial blood gases augment the exam. Once the decision is made to proceed with a definitive airway, defined as intubation of the trachea by either the nasal or the oral route, preparation is immediate. Preoxygenation by nasal cannula or mask is maintained, suction and intubating equipment gathered. Rapid sequence intubation is the technique that induces immediate unresponsiveness with an induction agent and muscular relaxation with a neuromuscular blocking agent. Commonly used induction agents include Etomidate, Ketamine, and Propofol. Neuromuscular blocking agents (NMBAs) must always be preceded by sedatives to ensure the patient is not aware of the paralysis. NMBAs include Succinylcholine, a depolarizing agent, and Vecuronium and Rocuronium, which are non-depolarizing agents.
Ventilator settings will vary based on the patient’s altered physiology and underlying disease states. However, specific parameters are recommended by ARDSnet [6] (Table 12.1).
4.2 Cardiovascular
Perhaps the most intimidating perioperative scenario facing the emergency surgeon is the patient in shock. The cardiovascular system plays a central role in the initial evaluation and ongoing resuscitation of patients suffering from shock. No single marker or test exists to direct therapy in these complex scenarios. The clinician must incorporate clinical exam findings, resuscitative endpoints, physiologic parameters, and imaging techniques to guide intervention.
Clinical assessment of vital signs, mental status, capillary refill, jugular vein distention, breath sounds, skin temperature, and pallor can provide useful clues as to potential etiology of the shock state. Early intervention is crucial and resuscitation measures can start at this point without the delay of more complex diagnostic studies. One must recognize that compensatory mechanisms, age, medications, and overall health complicate the diagnosis. Hypotension does not necessarily equal shock. Similarly, normotension does not mean that all tissue beds are adequately perfused, and the patient is not at risk.
The classification of hemorrhagic shock incorporated into (ATLS) has proved to be essential in caring for this patient population. This classification offers the ability to recognize early or late phases of hemorrhagic shock by allowing an estimation of losses, identifying traits of stability, and prompting corrective action [5] (Table 12.2).
Patients in Class I or II shock may respond to crystalloid resuscitation. If ongoing blood loss has been controlled, blood products may not be required. Patients in Class III and IV shock should be resuscitated with a balanced component blood product regimen where packed red cells, plasma, and platelets are provided in a 1:1:1 ratio [7]. This regimen coupled with damage control surgery and a goal systolic blood pressure of 90 mmHg until hemorrhage is controlled is the basis for the current damage control resuscitation. This regimen can be tailored to the patient’s coagulation profile utilizing the viscoelastic assays thromboelastography (TEG) or thromboelastometry (ROTEM). End points of resuscitation are followed to guide fluid and blood product administration as care progresses into the critical care unit postsurgical or radiologic intervention.
4.3 Renal
Perioperative acute kidney injury (AKI) is defined as sudden and often unanticipated decline in renal function that occurs within hours to days of surgery. It is associated with up to a tenfold increase in mortality, reduced long-term survival, and increased development of chronic kidney disease with subsequent need for hemodialysis. Most commonly, this is due to renal hypoperfusion or systemic inflammation that occurs as a direct response to surgery, although multiple factors may contribute [8]. The Acute Kidney Injury Network (AKIN) defines AKI as any of the following within 48 h: increased serumCr × 1.5, serumCr increase 0.3 mg/dL or more, or urine output less than 0.5 mL/kg/h for more than 6 h [9].
Goal-directed therapy is recommended when AKI develops. Utilization and optimization of endpoints of resuscitation should be instituted; this may require transfer to a critical care unit and possible invasive procedures. Early consultation with nephrology has been shown to lessen chronic kidney disease. Renal replacement therapy may be instituted in cases of refractory fluid overload, severe hyperkalemia (K+ >6.5 mEq/L), signs of uremia, and severe metabolic acidosis (pH < 7.1).
4.4 Gastrointestinal
Use of nasogastric decompression tubes preoperatively in the emergent general surgery patient is selective. Patients with bowel obstruction, high-grade ileus, or at high risk for emesis with aspiration require decompression. These tubes may facilitate early institution of enteral feeding as well. Routine use of nasogastric tubes after abdominal surgery to hasten resolution of postoperative ileus, diminish aspiration risk from gastric contents, improve patient comfort, protect intestinal anastomoses, or shorten hospital stay is not recommended [10].
Surgical patients at severe risk for stress ulceration are those on mechanical ventilation for more than 48 hours and coagulopathy. Additional high risk factors include traumatic brain injury, spinal cord injury, burns, greater than one week in the ICU, steroid use, and past history of gastrointestinal (GI) bleeding [11]. Multiple prophylactic regimens exist for stress ulceration. When compared to histamine 2 blockers, proton pump inhibitors were shown to be more protective against GI bleeding [12].
Early enteral nutrition in the postoperative phase of care is highly beneficial. Advantages include better glycemic control, improved anastomotic integrity, and reduced infectious morbidity [13]. While several systematic reviews have favored post-pyloric feeding over gastric feeding, a large multicenter randomized control study by Davies failed to show a preferential route [14].
4.5 Endocrine
In both the diabetic and nondiabetic populations, hyperglycemia in the perioperative period is an independent marker of poor surgical outcomes such as delayed wound healing, increased infection rates, increased hospital length of stay, and increased hospital mortality. Van den Berghe demonstrated that an intensive insulin therapy (IIT) regimen targeting a blood glucose (BG) of 80–110 mg/dL reduced in-hospital mortality by 34% compared to a standard therapy target of 180–200 mg/dL in surgical ICU patients [15]. Due to concerns for hypoglycemia utilizing IIT, several societies now support moderating the target BG. The Society for Critical Care Medicine (SCCM) recommends BG < 150 mg/dL [16], and the American College of Physicians recommends BG 140–200 mg/dL [17].
Acute adrenal insufficiency may require attention in the emergent surgical patient. Preoperatively, any patient who is taking more than 20 mg/day of prednisone or its equivalent, or any patient on glucocorticoids who has clinical Cushing’s syndrome should be considered adrenal insufficient due to decreased function of the hypothalamic-pituitary-adrenal axis (HPA). For minor procedures, patients should take their usual morning dose with no extra supplementation. For moderate stress procedures, the morning dose should be supplemented with hydrocortisone 50 mg IV immediately pre-op and 25 mg of hydrocortisone every 8 h for 24 h. Return to usual dose thereafter. For major operative procedures, the usual morning dose is supplemented with hydrocortisone 100 mg IV preinduction of anesthesia and 50 mg every 8 h for 24 h. The dose should then be tapered by half per day to maintenance dose [18].
Adrenal insufficient critically ill patients can be difficult to identify due to lack of specific signs and symptoms. Of particular concern is the patient with refractory shock (systolic BP <90 mmHg), despite adequate fluid resuscitation and vasopressor therapy. The decision to utilize steroid therapy is usually made clinically, as testing for HPA function is of limited value in critically ill patients. Current recommendations are for hydrocortisone 200–400 mg/day in divided doses [19].
4.6 Hematologic
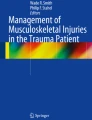
Bleeding in the acute care and trauma patient can present overtly or subtly. The etiology of perioperative hemorrhage is often multifactorial and can include blood loss, hemodilution, acquired platelet dysfunction, coagulation factor consumption, hypothermia, activation of fibrinolytic pathways, and prescribed oral anticoagulants [20]. An awareness of the more common coagulopathies, their assessment, and treatment is indispensable in managing these patients. Thromboelastography (TEG) and thromboelastometry (ROTEM) are both point of care assays that are rapid and measure the complex interactions of different coagulation elements not appreciated by the slower, isolated coagulation parameters such as the prothrombin time (PT), activated partial thromboplastin time (aPTT), or the international normalized ratio (INR) [21]. An example of a TEG assay curve is illustrated in Fig. 12.1.

TEG Assay Curve Demonstrating Normal Coagulation Profile [22]. (TEG® hemostasis analyzer tracing image used by permission of Haemonetics Corporation. TEG® and Thrombelastograph® are registered trademarks of Haemonetics Corporation in the US, other countries or both)
Acute traumatic coagulopathy (ATC) is an impairment in hemostasis with self-sustaining activation of the fibrinolytic system independent of hypothermia, acidosis, and hemodilution [23]. Management of major bleeding requires repair of the underlying cause after surgery or trauma, volume resuscitation with blood products, and diagnosis and management of ongoing coagulopathy.
Disseminated Intravascular Coagulopathy (DIC) is the systemic activation of the coagulative pathways, leading to generation and deposition of fibrin and microvascular thrombi. There is potential for end organ damage and can occur with trauma, sepsis, or amniotic fluid emboli. If not corrected, an additional consumptive state with compounding consumptive coagulopathy features will lead to exhaustion of platelets, coagulation proteins, and accelerated fibrinolysis with continued or worsening bleeding. The hallmark of DIC is fibrinolysis; regardless of other parameters, there will be evidence of breakdown products of fibrinogen [24].
A multitude of therapies have recently emerged with new indications for anticoagulant therapy. The risk of bleeding versus thromboembolism must be balanced in the acute care setting and trauma. High-risk patients such as those with a mechanical mitral valve, atrial fibrillation with mitral valve disease, or history of thromboembolism should be placed on intravenous heparin therapy while off warfarin. Prothrombin complex (PCC) provides the benefit of reversal while limiting volume administration that is associated with plasma reversal. This has been especially advantageous in high-risk reversal situations such as intracranial hemorrhage and intra-abdominal bleeding. The direct oral anticoagulants (DOACs) reversibly inhibit coagulation factors. There are multiple agents available on the market, some of which have specific reversal agents, but not always readily available. Early consultation with pharmacy services is essential.
4.7 Infectious
The Surviving Sepsis Campaign defines sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis with circulatory and cellular or metabolic dysfunction, associated with a higher risk of mortality. Patients with sepsis face a mortality rate of 25–30% and patients with septic shock face a 40–60% mortality rate. Surgical patients make up one third of all sepsis cases, and the incidence of sepsis among patients undergoing emergency surgery is twice that of patients undergoing elective operations. Risk factors include male gender, age greater than 50 years, pancreatic or small intestine procedures, American Society of Anesthesiologists (ASA) physical status class 3–5, and a partially or a totally dependent functional status [25, 26].
Treatment and fluid resuscitation should begin immediately. The goal is to increase cardiac output and improve end organ perfusion [27] (Fig. 12.2).

Surviving Sepsis Campaign Guidelines for Management of Sepsis and Septic Shock [28] (Reproduced with permission from survivingsepsis.org. Copyright©2019 the Society of Critical Care Medicine and the European Society of Intensive Care Medicine)
Obtain blood cultures and lactate levels, begin fluid resuscitation immediately and complete within 3 h. Empiric broad-spectrum antibiotics are started immediately to cover all potential pathogens. At least two sets of blood cultures (aerobic and anaerobic) should be taken prior to antibiotic therapy, but therapy should not be delayed in order to obtain cultures. Antimicrobial therapy should be narrowed once the pathogen and its sensitivities are identified or discontinued if no infection is established. Vasopressors should be started within the first hour to achieve a MAP of greater than 65 mmHg if blood pressure is not restored after initial fluid therapy. The SCCM recommends hydrocortisone 50 mg IV every 6 h, only in the case of vasopressor resistant shock [19].
Dos and Don’ts
Dos
-
Early establishment of definitive airway if indicated
-
Early attention to heart rate, blood pressure, respiratory rate, and mental status
-
Prompt assessment of lactic acid, base deficit, pH, and TEG parameters
-
Timely blood cultures and antibiotic therapy where applicable
Don’ts
-
Delay in evaluation and care
-
Over or under resuscitate as guided by trends in the endpoints of resuscitation
-
Overlook adrenal insufficiency and blood glucose levels
Take-Home Messages
-
Follow the ABC’s of resuscitation
-
Early treatment of hemorrhagic shock with a balanced ratio of blood products
-
Early implementation of Surviving Sepsis Campaign Bundle
-
Timely implementation of the ARDS Network protocol
Multiple Choice Questions
-
1.
Which of the following sedative agents has the adverse effect of hypotension and should not be used in patients with hemodynamic instability?
-
A.
Ketamine
-
B.
Etomidate
-
C.
Propofol
-
D.
Rocuronium
-
A.
-
2.
Which of the following sedative agents causes adrenal insufficiency and should not be administered as a continuous infusion?
-
A.
Propofol
-
B.
Ketamine
-
C.
Midazolam
-
D.
Etomidate
-
A.
-
3.
Renal replacement therapy is indicated in which of the following cases?
-
A.
Severe hypokalemia
-
B.
Severe metabolic alkalosis
-
C.
Severe metabolic acidosis
-
D.
Urine output <0.5 cc/kg/h
-
A.
-
4.
Despite its variability, based on the patient’s preexisting conditions, urine output can serve as a clinical marker of end organ perfusion. The urinary output of the adult being resuscitated should reach:
-
A.
0.5 cc/kg/h
-
B.
1.0 cc/kg/h
-
C.
0.75 cc/kg/h
-
D.
0.25 cc/kg/h
-
A.
-
5.
A 62 year old female recently diagnosed with breast cancer underwent port placement 3 days ago. The incision is erythematous and indurated. Her blood pressure is 90/60 mmHg, temperature 100.5 °F, heart rate 95 bpm, respirations 22. Fluid resuscitation should begin with:
-
A.
50 cc/kg normal saline in the first 5 h
-
B.
30 cc/kg normal saline in the first 5 h
-
C.
30 cc/kg lactated ringers in the first 3 h
-
D.
30 cc/kg colloid in the first 3 h
-
A.
-
6.
An ICU patient requires fluid resuscitation and shows little improvement after 48 h. Which of the following parameters suggests increased mortality?
-
A.
Increased urine output after resuscitation
-
B.
Elevated lactate levels
-
C.
Increased right ventricular end diastolic volume index
-
D.
Base deficit of −4 mEq/L
-
A.
-
7.
A 42 year old male involved in a motor vehicle collision is brought to the ED via ambulance. Over the course of the exam, you see increasing work of breathing and accessory muscle use. His temperature is 98.6 °F, heart rate 110 bpm, respirations 23, and oxygen saturation 90%. Which of the following next steps in management is most appropriate at this time?
-
A.
Begin empiric antibiotic therapy
-
B.
Perform imaging studies
-
C.
Start 30 cc/kg lactated ringers
-
D.
Consider endotracheal intubation
-
A.
-
8.
A surgical ICU patient with a blood glucose of 195 does not have a medical history of diabetes mellitus. In order to reduce in-hospital mortality, postoperative management:
-
A.
Should incorporate insulin therapy to achieve a blood glucose of <150 mg/dL
-
B.
Is already controlling his blood glucose within the target range of 180–200 mg/dL
-
C.
Does not require insulin therapy because the patient is not diabetic
-
D.
Should incorporate insulin therapy to achieve a blood glucose of <190 mg/dL
-
A.
-
9.
Which of the following is not a risk factor for sepsis?
-
A.
Male gender
-
B.
ASA PS class 3–5
-
C.
Gallbladder procedures
-
D.
Totally dependent functional status
-
A.
-
10.
Patients in Class III and Class IV hypovolemic shock should be resuscitated with which of the following regimens?
-
A.
PRBCs, plasma, and platelets in a 2:1:1 ratio
-
B.
PRBCs, plasma, and platelets in a 1:1:1 ratio
-
C.
Crystalloid IVFs only
-
D.
Crystalloid IVF and PRBCs
-
A.
References
Cuthbertson DP. Post-shock metabolic response. Lancet. 1942;239(6189):433–7.
Evans C, Bauman ZM, Cooper C, Capella JM. Surgical shock. In: Essentials of general surgery and surgical specialties. 6th ed. Philadelphia: Wolters Kluwer; 2019.
Vincent JL, Silva AQE, Couto L Jr, Taccone FS. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit Care. 2016;20(1):257.
Mikulaschek A, Henry SM, Donovan R, Scalea TM. Serum lactate is not predicted by anion gap or base excess after trauma resuscitation. J Trauma. 1996;40(2):218–22.
ATLS®. Advanced trauma life support student course manual, 10th ed. American College of Surgeons; 2018.
National Heart, Lung and Blood Institute, Acute Respiratory Distress Syndrome Network (NHLBI ARDS Network). http://www.ardsnet.org.
Holcomb JB, Tilley BC, Baraniuk S, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs. a 1:1:2 ratio and mortality of patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471–81.
Rodriguez JD, Hilthe CC. Perioperative acute kidney injury. StatPearls [Internet] 2020. Treasure Island: StatPearls Publishing; 2021. PMID: 32491609.
Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, Levin A. Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31. https://doi.org/10.1186/cc5713.
Verma R, Nelson RL. Prophylactic nasogastric decompression after abdominal surgery. Cochrane Database Syst Rev. 2007;2007(3):CD004929. https://doi.org/10.1002/14651858.CD004929.
Cook DJ, Fuller HD, Guyatt GH, Marshall JC, Leasa D, Hall R, Winton TL, Rutledge F, Todd TJR, Roy P, Lacroix J, Griffith L, Willan A. Risk factors for gastrointestinal bleeding in critically ill patients. JAMA. 1994;330(6):377–81.
Barkun AN, Bardou M, Pham CQD, Martel M. Proton pump inhibitors vs. histamine 2 receptor antagonists for stress-related mucosal bleeding prophylaxis in critically ill patients: a meta-analysis. Am J Gastroenterol. 2012;107(4):507–20.
Cresci GAM, MacGregor JM, Harbison SP. Surgical nutrition. In: Essentials of general surgery and surgical specialties. 6th ed. Philadelphia: Wolters Kluwer; 2019.
Davies AR, Morrison SS, Bailey MJ, Bellomo R, Cooper DJ, Doig GS, Finfer SR, Heyland DK. A multicenter, randomized controlled trial comparing early nasojejeunal with nasogastric nutrition in critical illness. Crit Care Med. 2012;40(8):2342–8.
Van den Berghe G, Wouters P, Weekers F, Verwaest C, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345(19):1359–67.
Jacobi J, Bircher N, Krinsley J, Agus M, Braithwaite S, Deutschman C, Freire A, Geehan D, Kohl B, Nasraway SA, Rigby M, Sands K, Schallom L, Taylor B, Umpierrez G, Mazuski J, Schenemann H. Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit Care Med. 2012;40(12):3251–76.
Qaseem A, Humphrey LL, Chou R, Snow V, Shekelle P. Use of intensive insulin therapy for the management of glycemic control in hospitalized patients: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2011;154(4):260–7.
Hamrahian AH, Roman S, Milan S. The management of the surgical patient taking glucosteroids. In: UpToDate, Post TW (editor). Waltham; 2021. Accessed 29 Apr 2021.
Kaufman DA. Glucocorticoid therapy in septic shock in adults. In: UpToDate, Post TW (editor). Waltham; 2021. Accessed 29 Apr 2021.
Ghadimi K, Levy JH, Welsby IJ. Perioperative management of the bleeding patient. Br J Anaesth. 2016;117(suppl 3):iii18–30.
Tanaka KA, Bader SO, Gorlinger K. Novel approaches in management of perioperative coagulopathy. Curr Opin Anesthesiol. 2014;27(1):72–80.
TEG® hemostasis analyzer tracing image used by permission of Haemonetics Corporation. TEG® and Thrombelastrograph® are registered trademarks of Haemonetics Corporation in the US, other countries or both.
Brohi K, Singh J, Heron M, Coats T. Acute trauma coagulopathy. J Trauma. 2003;54(6):1127–30.
Levi M, Toh CH, Thacil J, Watson HG. Guidelines for the diagnosis and management of disseminated intravascular coagulation. Br J Haematol. 2009;145(1):24–33.
Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2016. Crit Care Med. 2017;45(3):486–552.
Gabriel V, Grigorian G, Nahmias J, Pejcinovska M, Smith M, Sun B, Won E, Bernal N, Barrios C, Schubl SD. Risk factors for post-operative sepsis and septic shock in patients undergoing emergency surgery. Surg Infect (Larchmt). 2019;20(5):367–72.
Levy MM, Evans LE, Rhodes A. The surviving sepsis campaign bundle: 2018 update. Crit Care Med. 2018;46(6):997–1000.
Copyright©2019 the Society of Critical Care Medicine and the European Society of Intensive Care Medicine. Reproduced with permission from survivingsepsis.org.
Further Reading
ATLS®. Advanced trauma life support student course manual, 10th ed. American College of Surgeons; 2018.
Hamrahian AH, Roman S, Milan S. The management of the surgical patient taking glucosteroids. In: UpToDate, Post TW (editor). Waltham; 2021. Accessed 29 Apr 2021.
Holcomb JB, Tilley BC, Baraniuk S, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs. a 1:1:2 ratio and mortality of patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471–81.
Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2016. Crit Care Med. 2017;45(3):486–552.
Soni NJ, Arntfield R, Kory P. Point-of-care ultrasound. 2nd ed. Philadelphia: Elsevier; 2020.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Romeo, O., Davidson, T.A., Davidson, S.B. (2023). Principles of Perioperative Management in Acute Care Surgery. In: Coccolini, F., Catena, F. (eds) Textbook of Emergency General Surgery. Springer, Cham. https://doi.org/10.1007/978-3-031-22599-4_12
Download citation
DOI: https://doi.org/10.1007/978-3-031-22599-4_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-22598-7
Online ISBN: 978-3-031-22599-4
eBook Packages: MedicineMedicine (R0)