
Abstract
Central Centrifugal Cicatricial Alopecia (CCCA) is a primary, scarring, lymphocytic, alopecia that mostly occurs in middle-aged females of African descent. The hair loss pattern seen in CCCA usually begins at the vertex of the scalp and progresses in a symmetric centrifugal, or circular, pattern, resulting in irreversible scarring and loss of follicular pores. The pathogenesis is unknown but recent evidence suggests that it is a multifactorial condition influenced by genetics, grooming habits, and environmental factors which trigger an inflammatory response that ultimately leads to scarring. Diagnosis can be made through clinical presentation and characteristic dermatoscopic findings with possible use of biopsy. Laboratory values such as nutritional markers, CBC, and androgen levels can aid in ruling out other forms of alopecia. Typical dermatoscopic findings show peripilar white or gray halos, honeycomb patterns, perifollicular and/or interfollicular erythema, broken hairs, and pinpoint white dots. CCCA can be differentiated from LPP histologically but may also require the use of an elastin stain, which shows differences in fibrosis morphology. Patient management should include a progressive multifactorial approach focusing on early intervention with medications, patient education on additional preventative measures and disease course, as well as psychosocial support and counseling. Topical medical treatments include those that reduce scalp inflammation and provide symptomatic relief for patients, such as corticosteroids, tetracyclines, minocycline, calcineurin inhibitors, anti-seborrheic shampoos, and minoxidil. Treatment can progress to the concurrent administration of intralesional corticosteroid injections, and oral immunomodulatory medications. Medications currently being explored for treatment include apremilast, gabapentin, clobetasol propionate, and JAK inhibitors. Invasive procedures, such as hair transplants, are considered last-line therapy. Additional techniques, including non-pharmacological methods such as camouflaging with hair pieces, wigs, and scalp micropigmentation have been beneficial for patients. These in conjunction with psychological support can be beneficial to patient satisfaction.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
A 50-year-old female reported burning on her scalp and hair loss centrally that was present for about 18 months. She treated the area with tea tree oil with no improvement. She reported using a hot comb to style her hair in the past but stopped due to hair breakage. She also used extensions in the past but now wears her hair loose and does not have it braided.
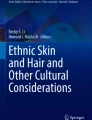
On physical examination, there was a smooth, shiny patch of alopecia with few sparse hairs on the vertex of the scalp extending outward (Fig. 11.1). The eyelashes and eyebrows were intact. She had normal fingernails.

Smooth, shiny, patch of scarring alopecia present on the vertex of the scalp extending centrifugally. Image courtesy of Dr. Melissa Piliang and Janine Sot, MBA medical photographer
Based on the clinical case description, what is the most likely diagnosis?
-
1.
Lichen planopilaris
-
2.
Traction alopecia
-
3.
Central centrifugal cicatricial alopecia
-
4.
Lichen planopilaris, frontal fibrosing variant
Diagnosis
Central centrifugal cicatricial alopecia.
Discussion
Central centrifugal cicatricial alopecia (CCCA) is the most common scarring lymphocytic mediated alopecia that can cause permanent hair loss. It primarily affects young to middle-aged women of African descent with a varying prevalence between 3%–6% [1, 2]. However, there have been no population studies to date so the true prevalence may be unknown [3]. The etiology and pathogenesis are unknown but recent evidence suggests genetics, grooming habits, and environmental factors could trigger an inflammatory response [2, 4]. It is important to note that scarring, not inflammation, is a significant clinical observation [5]. Aggravating factors include heat, traction-inducing hairstyles, chemical relaxers, and texturizers [3]. However, the lack of statistically significant data as well as the presence of CCCA in women who do not practice the aforementioned hair routines, guided researchers to consider broader etiologies such as infection, autoimmune disease, and specific genetic factors [1].
Genetic factors may include familial inheritance. One pedigree study (n = 14 families) suggested CCCA can be inherited in an autosomal dominant pattern with partial penetrance [6]. A study concluded a variant of the PAD13 gene may be responsible for malformed hair shafts associated with CCCA [3, 7]. PADI3 is a peptide enzyme that post-translationally modifies other proteins that are essential for hair-shaft formation. Missense mutations that can occur within this gene affect highly conserved sequences, ultimately resulting in protein misfolding and decreased enzymatic activity [7].
Dysregulation of lipid metabolism may also play an important role in the disruption of hair follicle homeostasis. One gene expression study (n = 5) found a decreased expression of genes related to lipid metabolism and fatty acid synthesis in CCCA. The study also showed an increased expression of genes related to fibroblast regulation in CCCA. The increased expression is also present in uterine fibroid development and other fibroproliferative disorders, suggesting scar formation in CCCA occurs through a similar mechanism [5].
It is thought that disruption of balance or failure of communication between the epithelium regeneration and surrounding dermal papilla mesenchyme could result in hair loss [8]. This could occur secondarily to PPAR-γ downregulation disrupting lipid homeostasis and subsequent inflammation and fibrosis, as previously stated. However, more research is needed to explore the interaction of PPAR-γ and TGF-β in the wound healing pathway [8]. Once there is a better understanding of the pathogenesis, more targeted treatment options will follow [8].
The clinical presentation of CCCA is that of patterned progressive hair thinning. Thinning typically begins at the central vertex and spreads in a symmetric centrifugal pattern to the rest of the scalp [4, 5]. The subsequent scarring is irreversible and leads to the loss of follicular pores resulting in shiny affected areas [4, 5]. The periphery of these shiny affected areas can blend with surrounding, normal-appearing areas leading to no demarcation between affected areas and normal scalp. It is this periphery that is considered to be the most active for disease [1, 2]. Dermoscopic and histological analyses show that evidence of CCCA can be seen beyond the vertex scalp, extending into the normal-appearing tissue that lack clinically evident disease [9]. Presenting symptoms can range from asymptomatic hair thinning to burning, pruritus, scaling, erythema, tenderness, and follicular pustules on the crown.
Diagnosis can be made through clinical presentation and judgment but can also be aided by a biopsy [5]. Clinical judgment largely relies on negative findings for other disorders such as performing KOH prep and obtaining laboratory values such as nutritional markers, a complete blood count, and androgen levels [1]. Typical dermoscopic findings are peripilar white or gray halos, honeycomb patterns, perifollicular and/or interfollicular erythema, broken hairs, and pinpoint white dots [9]. Histologically, CCCA, like other primary scarring alopecia disorders, shows premature desquamation of the inner root sheath [1]. CCCA needs to be differentiated from lichen planopilaris (LPP), which presents with superficial perifollicular fibrosis, infundibular inflammation, and destruction that leads to free hair shafts in the dermis, similar to CCCA. However, it is differentiated by the presence of vacuolar lichenoid dermatitis with epidermal cytoid bodies and peri-infundibular hypergranulosis on histological evaluation [1]. CCCA may also present with a normal follicular pattern and preserved sebaceous glands. Clinicians may also consider using elastin stain to differentiate CCCA from LPP when the two appear identical on histopathology [10]. On elastin stain, CCCA will demonstrate tree trunk fibrosis, while LPP shows narrow wedge-shaped fibrosis [10]. This is used in conjunction with other clinical clues, such as the pattern of alopecia for diagnosis and treatment instead of relying solely on the pathology report.
Treatment
Treatment for CCCA should be multifactorial in its approach, with special attention paid to preventative measures such as topical medications, immunosuppressive therapies, psychosocial support, and patient education, including disease course and grooming education. There are invasive procedures that can be performed but these are not considered first-line therapy. It is crucial to discuss prognosis and limited treatment options to manage patient expectations [1]. Since scarring causes permanent hair loss, management largely relies on prevention, with early intervention preferred, and patient education. Patients are advised to avoid relaxers and chemical treatments, heat, occlusive greasy moisturizers, and traction-inducing hairstyles like braiding [2]. It is important to screen family members for CCCA and encourage natural hairstyles for these patients [3]. These preventative recommendations are empiric at best and not substantiated by sufficient evidence.
No randomized controlled studies have addressed CCCA treatment. The main goal of treatment is to stabilize the condition to slow or halt hair loss. The least invasive treatment options include topical medications, such as corticosteroids, tetracyclines, minocycline, calcineurin inhibitors, anti-seborrheic shampoos, and minoxidil, to reduce inflammation and provide symptomatic relief [3, 4]. For disease not relieved with daily topical treatments, concurrent 5–10 mg intralesional corticosteroid injections at the leading edge can be performed at monthly intervals for 6–8 months [3, 4]. For active disease states, a short course of oral steroids may be considered. If improvement is seen after 2–6 months, a slow one-year taper of topical treatments can be discussed [1]. Persistently resistant disease may require administration of systemic medications like tetracyclines, hydroxychloroquine, antiandrogens, and immunosuppressives (mycophenolate mofetil and cyclosporine) for up to 1 year [3, 4]. Hair transplants can be considered in advanced, stable disease states where inflammation has been absent for 1 year. A test section should be performed first, due to concerns of graft survival on existing scar tissue. Additionally, non-pharmacological techniques such as camouflaging with hairpieces, wigs, scalp micropigmentation, and psychological support can be beneficial to patient satisfaction [3].
Due to the evolving understanding of the disease pathogenesis, new treatment considerations are being explored. Recently, JAK inhibitors have shown to be effective in treating alopecia areata. As a result, trials have begun to study their effectiveness for primary cicatricial alopecia patients [1]. An open label study concluded clobetasol propionate 0.05% emollient foam was a safe and effective treatment to decrease inflammation and provide symptomatic relief [11]. Currently, there are ongoing trials for therapies including apremilast, topical 6% gabapentin, gentle wounding to stimulate follicle growth, and biocellular regenerative treatment [12,13,14,15,16].
Key Points
-
Central centrifugal cicatricial alopecia (CCCA) is a primary scarring lymphocytic alopecia that mostly occurs in middle-aged females of African descent and can cause permanent hair loss.
-
CCCA usually presents as asymptomatic hair thinning that begins on the vertex scalp and progresses in a symmetric centrifugal pattern, resulting in irreversible scarring and loss of follicular pores.
-
Pathogenesis is unknown but recent evidence suggests that multiple factors, such as genetics, grooming habits, and environment, could trigger an inflammatory response that ultimately leads to scarring.
-
Treatment should be a progressive multifactorial approach focused on prevention through early intervention.
References
Gabros S, Masood S. Central centrifugal cicatricial alopecia. In StatPearls Publishing; 2021.
Ogunleye TA, McMichael A, Olsen EA. Central centrifugal cicatricial alopecia: what has been achieved, current clues for future research. Dermatol Clin. 2014;32(2):173–81.
Dlova NC, Salkey KS, Callender VD, McMichael AJ. Central centrifugal cicatricial alopecia: new insights and a call for action. J Investig Dermatol Symp Proc. 2017;18(2):S54–6.
Herskovitz I, Miteva M. Central centrifugal cicatricial alopecia: challenges and solutions. Clin Cosmet Investig Dermatol. 2016;9:175–81.
Aguh C, Dina Y, Talbot CC Jr, Garza L. Fibroproliferative genes are preferentially expressed in central centrifugal cicatricial alopecia. J Am Acad Dermatol. 2018;79(5):904–12.e1
Dlova NC, Jordaan FH, Sarig O, Sprecher E. Autosomal dominant inheritance of central centrifugal cicatricial alopecia in black South Africans. J Am Acad Dermatol. 2014;70(4):679–82.e1
Malki L, Sarig O, Romano M-T, Méchin M-C, Peled A, Pavlovsky M, et al. Variant PADI3 in central centrifugal cicatricial alopecia. N Engl J Med. 2019;380(9):833–41.
Subash J, Alexander T, Beamer V, McMichael A. A proposed mechanism for central centrifugal cicatricial alopecia. Exp Dermatol. 2020;29(2):190–5.
Felix K, De Souza B, Portilla N, Hogue L, Ahn CS, Sangueza O, et al. Dermatoscopic evaluation of central centrifugal cicatricial alopecia beyond the vertex scalp. JAMA Dermatol. 2020;156(8):916–8.
Sun CW, Motaparthi K, Hsu S. Central centrifugal cicatricial alopecia and lichen planopilaris can look identical on histopathology. Skinmed. 2020;18(6):365–6.
Callender VD, Kazemi A, Young CM, Chappell JA, Sperling LC. Safety and efficacy of clobetasol propionate 0.05% emollient foam for the treatment of central centrifugal cicatricial alopecia. J Drugs Dermatol. 2020;19(7):719–24.
ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2016, January – 2021, October. Identifier NCT03346668. Role of Neurogenic Inflammation and Topical 6% Gabapentin Therapy in Symptomatic Scarring Alopecia. [cited 2021 Oct 12]. https://clinicaltrials.gov/ct2/show/NCT03346668.
ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2018, November- 2021, February. Identifier NCT03521687. Apremilast in the Treatment of Central Centrifugal Cicatricial Alopecia (CCCA) [cited 2021 Oct 12]. https://clinicaltrials.gov/ct2/show/record/NCT03521687.
ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2017, February - . Identifier NCT03078686. Biocellular-Cellular Regenerative Treatment Scarring Alopecia and Alopecia Areata. [cited 2021 Oct 12]. https://clinicaltrials.gov/ct2/show/NCT03078686.
ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2018, November- 2021, February. Identifier NCT03521687. Apremilast in the Treatment of Central Centrifugal Cicatricial Alopecia (CCCA) [cited 2021 Oct 12]. https://clinicaltrials.gov/ct2/show/NCT03521687.
ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2018, January - . Identifier NCT03491267. Study to Determine Effect of Gentle Wounding to Stimulate Hair Follicle Neogenesis [cited 2021 Oct 12]. https://clinicaltrials.gov/ct2/show/NCT03491267.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Viola, J., Lawless, M., Sampath, S., Trotter, S.C. (2022). 50-Year-Old Female with a Burning Scalp and Hair Loss. In: Trotter, S.C., Sampath, S. (eds) Clinical Cases in Alopecia. Clinical Cases in Dermatology. Springer, Cham. https://doi.org/10.1007/978-3-031-15820-9_11
Download citation
DOI: https://doi.org/10.1007/978-3-031-15820-9_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-15819-3
Online ISBN: 978-3-031-15820-9
eBook Packages: MedicineMedicine (R0)