
Abstract
Lichen planopilaris (LPP) is a type of cicatricial alopecia that results in permanent hair loss commonly occurring in Caucasian and Indian women. LPP is considered a subtype of lichen planus whose characteristic skin findings may or may not be observed in patients diagnosed with LPP. There are several subtypes of LPP including classic, frontal fibrosing, and Graham-Little-Piccardi-Lasseur, each of which targets different areas of the body. The classic type usually occurs on the vertex and parietal scalp while frontal fibrosing alopecia targets the frontotemporal scalp. Graham-Little-Piccardi-Lasseur subtype presents with a cicatricial spreading pattern. The pathogenesis of LPP is not well understood, though there are several proposed mechanisms. One possible mechanism involves the upregulation of cell-mediated immunity pathways which lead to the targeting of follicular antigens and thus the permanent hair loss that can occur. Other affected pathways include upregulation of JAK expression which also results in the upregulation of proinflammatory cytokines and thus the destruction of the hair follicles. Treatment involves halting the scarring hair loss process before it occurs. First-line treatments typically include topical and intralesional corticosteroids. Novel treatments, based primarily on case studies, which target some of the primary pathogenic pathways include pioglitazone and tofacitinib. Treatment expectations should be discussed with patients before initiation as regrowth of previously destroyed hair follicles may not be possible. It is also important to consider the effect of LPP on patients’ mental health as this may affect the treatment goals and plan.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
A 66-year-old female reported itching in her scalp and occasional flaking for about a year. She also noticed hair loss, more concentrated in the frontal scalp over the past few years, but assumed it was age-related. She stated that she was not bothered by the hair loss but was more annoyed with the pruritus. She had not treated the itching before but stopped using sunscreen in the area because she thought she might be allergic.
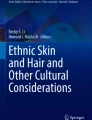
On physical examination, she had a smooth patch of alopecia lacking follicular openings along the frontal scalp line. The amount of recession was evident due to the lack of photodamaged skin in the area of hair loss that was present on the forehead. On further inspection, there was perifollicular erythema and scale noted in the scalp. She had mild thinning of the lateral portion of the eyebrows. Eyelashes were intact (Fig. 10.1). No fingernail changes were present, and her oral mucosa was normal.

Smooth patch of alopecia lacking follicular openings along the frontal scalp. Perifollicular erythema and scale are present on the scalp along with thinning of the lateral eyebrows. Note the demarcation of photodamage present on the forehead and not evident in the area of hair loss
Based on the clinical case description, what is the most likely diagnosis?
-
1.
Folliculitis
-
2.
Traction alopecia
-
3.
Androgenetic alopecia
-
4.
Lichen planopilaris, frontal fibrosing variant
Diagnosis
Lichen planopilaris, frontal fibrosing variant.
Discussion
Lichen planopilaris (LPP) is a chronic, primary, lymphocytic cicatricial alopecia that results in permanent, irreversible hair loss most commonly involving the vertex and parietal scalp [1]. Symptoms may include perifollicular erythema, pruritus, scaling, burning, and scalp tenderness [1, 2]. LPP is thought to be a follicular subtype of lichen planus where skin and mucous membrane manifestations may or may not be present in patients with this condition. Typically, this disorder affects middle-aged Caucasian and Indian women [1]. There is one classic type and two distinct clinical subtypes of LPP each with their own symptoms and characteristic patterns of hair loss. One subtype is frontal fibrosing alopecia which targets the frontotemporal hairline specifically in postmenopausal women. The other type is known as Graham-Little–Piccardi–Lasseur syndrome, which can present with cicatricial alopecia of the scalp, non-cicatricial hair loss in several different areas of the body, and keratotic follicular papules [2]. Other differentials for LPP include central centrifugal cicatricial alopecia, seborrheic dermatitis, discoid lupus, and pseudopelade of brocq. LPP can be diagnosed both clinically and histopathologically. Dermoscopy typically shows perifollicular scaling surrounding the proximal portion of the hair shaft [3]. Histologically, it is common to see subepidermal lymphocytic infiltrate, mucinous perifollicular fibroplasia, and wedge-shaped fibrosis that typically does not affect the deeper part of the follicle [3].
Classic symptoms of LPP can worsen when the skin is exposed to irritation, UV light, stress, and harsh chemical hair products which can result in triggering the pathways related to the overall pathogenesis of this disease [1]. Although not well understood, there are several proposed mechanisms for the pathogenesis of LPP, but the most widely accepted theory points to a possible autoimmune component [4]. Individuals with coexisting autoimmune conditions such as vitiligo and autoimmune thyroiditis have a higher likelihood of developing LPP. Cell-mediated immunity is thought to play a key role in the pathway to the development of LPP through T cell mediated targeting of follicular antigens [1]. This results in inflammation and destruction of the hair follicle stem cells, which explains the previously described symptomatology and ultimately results in permanent scarring [3]. Other proposed pathways contributing to inflammation include upregulation of IFNγ which subsequently increases the number of activated cytotoxic CD8+ cells and thus an increase in JAK expression [5]. Furthermore, decreased expression of peroxisome proliferator-activated receptor (PPAR) γ has been shown to be related to LPP. When PPARγ expression is decreased, this results in lipid accumulation and can lead to the destruction of the pilosebaceous unit through the recruitment of proinflammatory cytokines [6]. In mice models, when the PPARγ transcription factor is deleted, mice can develop symptoms of LPP including scarring alopecia [6]. While the exact pathogenesis of this disease is not well known, treatment options utilizing these pathways have been developed and shown promise in patients with LPP.
Treatment
Since hair loss is usually permanent due to scarring, regrowth may not be possible. As a result, treatment is typically focused on decreasing disease progression, controlling symptoms, and stopping the scarring process before permanent hair loss occurs. First-line treatments typically include high potency topical corticosteroids, intralesional corticosteroids, and oral hydroxychloroquine [1, 3, 4]. First-line treatments may be used in combination with each other or with other second- or third-line treatments to achieve the best treatment outcome. These first line therapies are typically initiated when the disease is more localized and not widespread as they target and are applied to specific areas of the body. Second and third-line treatments include disease-modifying antirheumatic drugs such as methotrexate and mycophenolate mofetil [3, 4]. It is important to note that the efficacy of these treatments is based mainly on case reports making it difficult to find treatments that work for each patient. There are also side effects that should be considered when initiating these medications including their effect on the immune system. If the extent of the LPP disease is refractory to all other treatments, cyclosporine and oral steroids can be used; however, their relapse rates are high and also come with significant side effect profiles [3]. Since relapse is common and hair growth is not possible, it is also important to assess the psychological consequence that this disease may have on individuals. Stress can contribute to disease pathogenesis, so managing a patient’s stress can have a significant impact on disease progression. Furthermore, managing patient expectations is key as stabilizing the disease may take at least 6 months and relapse can occur.
Several novel medications can be used if a patient is not experiencing improvement in symptoms and other first-line treatments have failed. Novel treatments used to treat LPP include pioglitazone and tofacitinib. Pioglitazone is typically used to treat diabetes because of its effect on PPARγ which can result in lower blood sugars. PPARγ has also been shown to play a role in the pathogenesis of LPP [3]. The absence, or downregulation, of PPARγ leads to the destruction of the pilosebaceous unit [6]. Therefore, increasing or upregulating this pathway helps to decrease the infiltration of inflammatory cells and thus diminish the amount of scarring hair loss that is seen in this disease. Secondly, oral tofacitinib, a JAK inhibitor, has shown to be effective in treating alopecia disorders. When this pathway is inhibited, IFN gene expression is also inhibited which results in decreased activation of T cells and thus less scarring and inflammation [5]. In one study, using tofacitinib as a monotherapy or adjunctive therapy against LPP resulted in 80% of individuals involved in the study experiencing an improvement in symptoms [5]. It is also important to note the mild side effect profile that participants in this study experienced [5]. Furthermore, an early phase one clinical trial studying the safety and efficacy of ixekizumab, an IL-17A inhibitor, as a treatment for LP and LPP is currently underway [7].
Key Points
-
Lichen planopilaris (LPP) is a chronic type of scarring alopecia that has an association with several other autoimmune conditions.
-
The pathogenesis of LPP is not well understood, but autoimmunity and pathways that trigger inflammatory cytokine activation have been proposed.
-
Treatment of LPP involves halting the scarring hair loss before it occurs, and patient expectations should be discussed prior to the initiation of treatment.
References
Weston G, Payette M. Update on lichen planus and its clinical variants. Int J Womens Dermatol [Internet]. 2015;1(3):140–9. Available from: https://www.sciencedirect.com/science/article/pii/S2352647515000301
Babahosseini H, Tavakolpour S, Mahmoudi H, Balighi K, Teimourpour A, Ghodsi S-Z, et al. Lichen planopilaris: retrospective study on the characteristics and treatment of 291 patients. J Dermatolog Treat [Internet]. 2019;30(6):598–604. https://doi.org/10.1080/09546634.2018.1542480.
Errichetti E, Figini M, Croatto M, Stinco G. Therapeutic management of classic lichen planopilaris: a systematic review. Clin Cosmet Investig Dermatol [Internet]. 2018;11:91–102. [cited 2022 Feb 28]. Available from: https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC5833781/
Assouly P, Reygagne P. Lichen planopilaris: update on diagnosis and treatment. Semin Cutan Med Surg [Internet]. 2009;28(1):3–10. [cited 2022 Feb 28]. Available from: https://pubmed.ncbi.nlm.nih.gov/19341936/
Yang CC, Khanna T, Sallee B, Christiano AM, Bordone LA. Tofacitinib for the treatment of lichen planopilaris: a case series. Dermatol Ther [Internet]. 2018;31(6):e12656. [cited 2022 Feb 28]; Available from: https://pubmed.ncbi.nlm.nih.gov/30264512/
Karnik P, Tekeste Z, McCormick TS, Gilliam AC, Price VH, Cooper KD, et al. Hair follicle stem cell-specific PPARgamma deletion causes scarring alopecia. J Invest Dermatol [Internet]. 2009;129(5):1243–57. [cited 2022 Feb 28] Available from: https://www.jidonline.org/article/S0022-202X(15)34335-9/fulltext
Ixekizumab in Adult Patients With Lichen Planus and Lichen Planopilaris [Internet]. Clinicaltrials.gov. [cited 2022 Feb 28]. Available from: https://clinicaltrials.gov/ct2/show/NCT05030415.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ernst, M., Viola, J., Sampath, S., Trotter, S.C. (2022). 66-Year-Old Female with Itchy Scalp and Hair Loss. In: Trotter, S.C., Sampath, S. (eds) Clinical Cases in Alopecia. Clinical Cases in Dermatology. Springer, Cham. https://doi.org/10.1007/978-3-031-15820-9_10
Download citation
DOI: https://doi.org/10.1007/978-3-031-15820-9_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-15819-3
Online ISBN: 978-3-031-15820-9
eBook Packages: MedicineMedicine (R0)