
Abstract
Dialectical behavior therapy (DBT) is built on a rich foundation of behavior therapy traditions and, through its innovative blend of dialectical philosophy, Zen Buddhism, and radical behaviorism, extends and enriches these traditions. Ultimately, DBT is a therapy that rests heavily on precise case formulation and the treatment plans that follow from it. Such case formulations are developed through the rigorous assessment procedures that were developed by radical behaviorists throughout the history of behavioral therapy. Similarly, many of the interventions that follow from these formulations have been developed and refined by many behavioral predecessors of DBT. For DBT clinicians, it is behavioral precision, devotion to assessing rather than inferring, and a commitment to precisely targeting controlling variables, paired with acceptance principles espoused by Zen Buddhism, that helps clients build lives worth living. Although DBT may differ from other behavioral therapies in its integration of acceptance-based philosophies, principles over protocols, and a range of assumptions that are central to the treatment, the underpinning emphasis on precision in formulating and targeting behaviors is a shared feature that lives in the “DNA” of DBT, along with its behavioral therapy family members.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Dialectical Behavior Therapy (DBT) was developed by Marsha Linehan throughout the 1970s and 1980s originally as a treatment for chronically suicidal and self-harming adults with borderline personality disorder (BPD). Since its conception, DBT and DBT-informed interventions have been developed for a number of populations, including forensic groups such as individuals in state prisons (Shelton et al., 2009), suicidal adolescents (McCauley et al., 2018), and people who have substance use problems (e.g., Linehan et al., 1999, 2002), major depressive disorder (e.g., Lynch et al., 2003), bipolar disorder (Van Dijk et al., 2013), attention deficit and hyperactivity disorder (Fleming et al., 2015), and eating disorders (e.g., Safer et al., 2010; Telch et al., 2001). DBT is predicated upon three core tenets: radical behaviorism as a technology of change, Zen Buddhism as a technology of acceptance, and dialectical philosophy as an underlying framework that unites and influences the two.
The Development of DBT
Early prototypes of DBT involved applying radical behaviorist principles (e.g., contingency management, skills training) to the treatment of suicidal behavior. However, as detailed in Linehan and Wilks (2018), such a “change-heavy” intervention proved difficult to tolerate for individuals with BPD, possibly due to their high levels of sensitivity, emotional reactivity, and their extensive histories of invalidation by caregivers and other clinical providers (e.g., Austin et al., 2007; Bennett et al., 2019; Staebler et al., 2011). Consequently, Dr. Linehan radically re-oriented DBT development through the creation of an intervention derived from Zen Buddhism and the principles of acceptance and mindfulness (Linehan & Wilks, 2018). Although acceptance and empathy were germane to this new approach, it too produced suboptimal outcomes, as clients expressed frustration at the clinician’s lack of attempts to help them solve their problems in meaningful ways (Linehan & Wilks, 2018). Based on these initial attempts, it was clear that Dr. Linehan’s clients required change, derived from radical behavioral interventions, and acceptance, derived from Zen Buddhism. This realization led Linehan to dialectical philosophy, espoused by philosopher Georg Wilhelm Friedrich Hegel, as a way to unite these two apparently opposing polarities (Linehan & Wilks, 2018).
Within dialectical philosophy, reality is reflected by two seemingly oppositional polarities, both of which contain truth or wisdom. A “synthesis”, then, reflects the unity of these two polarities– holding both sides as true–which allows individuals to progress with a new, multifaceted understanding (Linehan, 1993). Hence, DBT: wherein the fundamental dialectic underpinning therapy is that clients need to simultaneously change (i.e., behavioral interventions) and accept themselves and reality as it is (i.e., Zen Buddhist-informed interventions; Linehan, 1993) in order to build a life worth living.
The Biosocial Model
DBT is predicated on an overarching theory of BPD etiology and maintenance (Linehan, 1993; Crowell et al., 2009). The Biosocial Model (Linehan, 1993; Crowell et al., 2009) posits that the core deficit in BPD is one of emotion dysregulation. Accordingly, all diagnostic criteria contained in the DSM-5 (American Psychiatric Association, 2013) for BPD are theorized to be direct consequences of, or maladaptive attempts to cope with, emotion dysregulation. As implied by the model name, the origin of emotion dysregulation itself entails “Bio” and “Social” elements. Individuals with BPD are theorized to have a biological vulnerability to emotion dysregulation, which involves heightened emotional sensitivity (i.e., a reduced threshold for responding to emotional stimuli), emotional reactivity (i.e., a larger increase in emotion from baseline once provoked), and a slow return to baseline (i.e., prolonged emotional responses following termination of an emotional stimuli), coupled with difficulties modulating those processes (i.e., emotion regulation deficits; Linehan, 1993). Emotion dysregulation is theorized to develop from a transaction between this biological vulnerability and an early invalidating social environment (Linehan, 1993). Invalidating environments are defined as ones that punish emotional displays (e.g., a parent telling a child to “stop making such a fuss” or “don’t be sad”), intermittently reinforce emotional escalations (e.g., meeting a child’s needs only in response to a tantrum and not in response to lower intensity communications), and/or oversimplify the ease of problem solving (e.g., “Nobody else has trouble with this. It’s not that hard – just do it!”). Such invalidation is proposed to be provoked by, and further provokes, the intense, reactive, and prolonged emotional responses that individuals with BPD experience, transacting over time to eventually culminate in emotion dysregulation (Crowell et al., 2009; Linehan, 1993). Although there are no published longitudinal studies that study this transactional relationship exactly as specified in this model, longitudinal research suggests that interactions between tempermental characteristics (e.g., fearful, shyness) in adolescence and potentially invalidating parenting (i.e., maternal overprotection) predict BPD risk over a 5 year time course (Arens et al., 2011). Consequently, DBT assumes that a central skill deficit for those with BPD involves regulating and tolerating painful emotional states (Linehan, 1993).
The DBT Treatment Structure
The development of the underlying treatment philosophy substantively advanced Linehan’s efforts of producing an efficacious treatment for chronically suicidal and self-harming people with BPD. However, the high levels of chaos, multiple problems, and ongoing crises that this client population presented with required consideration of which problems to treat and when. The DBT treatment frame was developed in order to provide such structure and guidance, and holds that DBT has five treatment phases (pre-treatment, then Stages 1–4). Pre-treatment is typically 1–4 sessions long and involves collaboration between the therapist and client to identify therapy goals, gauge their motivation to work together, and obtain and strengthen the client’s commitment to pursue DBT and develop a life worth living. The vast majority of applications and research has been conducted with Stage 1 DBT and thus we describe it below in more detail.
Stage 1
Stage 1 is focused on a goal of achieving behavioral stability. DBT clients often present to therapy with high levels of chaos, changing clinical presentations, low motivation, and the emergence of new and ongoing crises. DBT in Stage 1 therefore has the following functions: (1) enhance capabilities (i.e., teach the client skills to more effectively regulate emotions, tolerate distress, navigate interpersonal interactions, and increase mindful awareness, among other skills necessary to learn new effective behaviors) (2) increase motivation in clients (to practice such skills, engage in effective patterns of behavior, refrain from ineffective patterns of behavior, and structure their lives more effectively) while also helping to remove barriers to effective behavior; (3) generalize skills to the client’s natural environments (i.e., not just the therapy office); and (4) structure the client’s environment to promote new, effective learning. An example of such an environmental structure could be helping the client find stable housing and employment, or teaching how to effectively end destructive relationships and make more supportive ones. DBT clinicians, in turn, often experienced high levels of burn out and emotion, and low levels of motivation, all of which interfered with their capacity to effectively administer DBT (Linehan, 1993). Clinicians thus (5) require a way to maintain their own capabilities, efficacy, and motivation. Standard DBT consequently has four components which address one or more of these five functions. Individual therapy is designed to increase client motivation to and enhance capabilities in whichever capabilities are required to help clients achieve their goals (e.g., emotion regulation, distress tolerance, structuring their environment). Clients also attend weekly DBT skills training sessions, usually in group format, which are predominantly designed to enhance capabilities by providing didactic education on DBT skills in four key areas: emotion regulation, distress tolerance, interpersonal effectiveness, and mindfulness. For example, topics covered include what “essential ingredients” comprise mindfulness and how to practice it (mindfulness skills), skills for decreasing painful emotions (emotion regulation), skills for accepting and tolerating emotions (distress tolerance), and skills to have effective interpersonal interactions (interpersonal effectiveness). In order to ensure that skills generalize to clients’ natural environments, standard DBT involves phone consultation from clinicians outside of sessions, wherein individual therapists coach clients to use skills in their daily lives, manage emerging crises, and work with clients to repair the therapeutic relationship (if ruptured). Finally, DBT therapists operate on a team in which they meet regularly (i.e., DBT consultation team). DBT consultation team involves the application of DBT strategies to hold clinicians within the treatment frame and promote their capabilities, effectiveness, and motivation.
Clinical Targets
The complex, multi-problem nature of the client population in DBT required a method of determining which clinical targets should be prioritized within the DBT treatment modes. In the individual therapy mode, clinical targets are hierarchically organized, and the first priority in treatment is the elimination of life-threatening behavior such as suicidal and self-harming behaviour (Linehan, 1993). Thus, in Stage 1, if clients exhibit life-threatening behavior, then targeting and intervening on these behaviors is the top priority of the treatment session. The second-highest priority in Stage 1 involves targeting and intervening upon behaviors of the client or therapist that interfere with the functioning of therapy (i.e., therapy-interfering behavior), including nonattendance, low adherence to the treatment tasks, and behaviors that promote burnout in therapists (e.g., yelling at therapists, calling too frequently). If neither life-threatening nor therapy-interfering behaviors are present, then the remaining targets of Stage 1 are behaviors that generally interfere with the client having a reasonable quality of life. These “quality of life-interfering behaviors” can include other psychological problems (e.g., depression, anxiety), vocational issues, or other social or economic stressors (e.g., repairing relationships, acquiring work, going back to school). This target hierarchy differs within DBT skills training, where the predominant targets are to teach new skills and to decrease group-destroying behavior (i.e., behavior that would destroy the functioning of the group, such as threatening other group members). Unlike in individual therapy, lower level therapy-interfering behaviors that emerge in group are not prioritized over skills training and may instead be addressed within individual therapy.
Stages 2–4
Clients transition from Stage 1 to Stage 2 following the achievement of behavioral control and stability (Linehan, 1993). However, DBT research has heavily focused on Stage 1 of treatment, and thus interventions for Stages 2–4 are less clearly articulated and documented. Theoretically, the primary target of Stage 2 is to treat what Linehan (1993) termed “quiet desperation.” Comorbid disorders of moderate severity, particularly posttraumatic stress disorder, are targeted in this stage. Other evidence-based treatments for these disorders may be incorporated during this stage, and recent adaptations of DBT that blend Stage 1 DBT with evidence-based PTSD treatments have been developed (e.g., Bohus & Pirebe, 2018; Harned et al., 2012). Ultimately, clinicians strive to help clients experience emotions in the absence of profound anguish within Stage 2. Stage 3 is focused on “ordinary happiness”, wherein typical problems in living are addressed. This stage may involve the application of other treatments to mild comorbid disorders, as well as problem solving general vocational or psychosocial stressors. Finally, Stage 4 is focused on building joy and freedom, wherein spiritual fulfillment, decreased emptiness, and a lack of fulfillment are targeted (Koons, 2021; Linehan, 1993).
Research Evidence
Several randomized controlled trials examining the efficacy of DBT have been conducted across several independent research groups in both adolescent and adult samples (e.g., Carter et al., 2010; Clarkin et al., 2007; Goldstein et al., 2015; Linehan et al., 1991, 1993, 1999, 2002, 2006, 2008, 2015; McCauley et al., 2018; McMain et al., 2009; Mehlum et al., 2014, 2016; van den Bosch et al., 2002; Verheul et al., 2003), with a handful of effectiveness trials (e.g., Barnicot et al., 2014; Feigenbaum et al., 2012; Goodman et al., 2016; Koons et al., 2001; Pistorello et al., 2012). The most common outcome studied in DBT trials is the reduction of suicidal and self-harming behavior. Extensive research suggests that DBT results in significant reductions in suicidal and non-suicidal self-injury compared to treatment as usual (e.g., Pistorello et al., 2012; Verheul et al., 2003), and active control conditions such as community treatment by experts (Linehan et al., 2006), individual and group supportive therapy (McCauley et al., 2018), and enhanced usual care (Melhum et al., 2016). Effectiveness studies also suggest that DBT outperforms treatment as usual in reducing suicidal behavior or non-suicidal self-injury (e.g., Priebe et al., 2012). However, it is notable that some trials suggest that DBT results in comparable reductions in suicidal behavior or non-suicidal self-injury compared to control conditions including general psychiatric management (McMain et al., 2009) and treatment as usual (Carter et al., 2010).
Evidence for DBT also has been culminated in multiple meta-analyses, the most recent of which examined the efficacy of DBT in reducing suicidal behavior and non-suicidal self-injury compared to control conditions across 18 controlled trials. This meta-analysis revealed a small effect sized difference for suicidal behavior and non-suicidal self-injury (d = −.324) and use of crisis services (d = −.379) between DBT and control conditions in favor of DBT. However, this meta-analysis also indicated that DBT did not outperform control conditions in reducing suicidal ideation, suggesting that DBT could be refined to improve its capacity to target this variable (DeCou et al., 2019).
Researchers have also examined the efficacy of DBT skills training alone for a range of populations (e.g., Lynch et al., 2003; McMain et al., 2017; Neacsiu et al., 2014; Soler et al., 2009; Telch et al., 2001). McMain et al. (2017) compared 20 weeks of DBT skills training for those with BPD to a waitlist control and showed that the individuals who received skills training exhibited greater reductions in suicidal and self-harming behaviors than those on the waitlist. Similarly, Soler et al. (2009) compared 12 weeks of DBT skills training or standard group therapy for people with BPD. Suicidal and non-suicidal self-injury outcomes were not measured in this trial, but DBT skills training outperformed the control condition in terms of drop out, anger depression, anxiety, and emotional instability. Studies have also examined the efficacy of DBT skills training for non-BPD populations. One study compared DBT skills groups alone for individuals who had an anxiety or depression disorder with high emotion dysregulation (but not BPD) to an activities-based support group. DBT skills training outperformed the activities-based support group in reducing emotion dysregulation and anxiety, but not depression (Neasciu et al., 2014). These studies suggest that DBT skills training alone may be an efficacious intervention for BPD and related problems.
In a landmark dismantling trial, Linehan et al. (2015) randomized suicidal or self-injuring people with BPD to either standard DBT, individual DBT without DBT skills training but with an activities group (DBT-I), or DBT skills training without individual therapy but with individual case management (DBT-S). Conditions were comparable in the extent to which they decreased suicide attempts, suicidal ideation, and the use of crisis services. However, individuals who engaged in non-suicidal self-injury exhibited lower frequencies of non-suicidal self-injury in standard DBT and DBT-S than in DBT-I during the treatment year, but not at the x month follow-up period. These findings suggest that DBT skills training may be a particularly “active ingredient” of DBT interventions, and that pairing it with other types of individual therapy/case management may be efficacious. However, future research in this area is needed in order to replicate and extend these findings.
The Role of Assessment in DBT
As a primarily behavioral treatment, assessment plays a critical and constant role in the delivery of DBT (Linehan, 1993). The behavioral stance encourages the therapist to regularly engage in rigorous assessment, rather than rely on inferences, and to avoid pejorative descriptions of clients and their behavior such as “manipulative” or “attention-seeking”. The guiding principle of “assess, don’t assume” begins in the first pre-treatment session and remains just as relevant as treatment progresses. It is important to note that self-report and physiological assessments of BPD are frequently discrepant (e.g., Rosenthal et al., 2008), and evidence suggests that there is low agreement between individuals with BPD and informant reporters on BPD symptoms (Balsis et al., 2018). Inclusion of informant reports may therefore generally enhance the comprehensiveness of assessment.
In the first session (or even before the first session in an intake process or over the phone), goodness of fit between the individual client and the treatment needs to be determined through careful assessment. Since DBT was originally developed as a treatment for BPD (and has the most supportive evidence for this disorder), determining whether the person meets DSM criteria (APA, 2013) for BPD may be indicated. However, as has been noted elsewhere (e.g., Biskin & Paris, 2012; Kopala-Sibley et al., 2012), BPD is a highly heterogenous disorder. Case in point: there are 256 different ways to meet criteria for BPD (Biskin & Paris, 2012). Moreover, since a person need meet only five of the nine DSM criteria, it is possible for two people with a BPD diagnosis to only overlap on one diagnostic criterion. Ultimately, then, a diagnosis of BPD may provide less information about goodness of fit than a more careful assessment of areas of dysregulation within the client that DBT can address. A reconceptualization of the BPD criteria initially proposed by Linehan (1993) highlights that the DSM criteria for BPD can be summarized into five categories, and this reorganization may be a more useful tool for assessment with individuals presenting to treatment:
-
1.
Emotion Dysregulation: individuals with BPD typically experience intense emotions, have difficulty regulating emotions when they occur, and experience emotions as lasting a long time (i.e., have slow return to baseline). Questions to assess emotion dysregulation domain: What changes in your body, thoughts, and behavior do you notice when you’re experiencing strong emotions? Do your emotions feel more intense than other people you know? What emotions cause the most problems for you? How long do your emotions seem to last? How frequently do these emotional changes occur?
-
2.
Interpersonal Dysregulation: individuals with BPD tend to have intense and chaotic relationships with others (Bouchard et al., 2009; Hill et al., 2011). These relationships can be romantic, friendships, and/or familial. While not every single relationship is necessarily problematic, individuals frequently experience their relationships as unstable and fragile, and thus never feel completely comfortable with the status of their relationships. Questions to assess interpersonal dysregulation domain: What are your close relationships like? How often do you experience conflict in your close relationships? What happens when you have conflict with loved ones? What kinds of things do you do when you feel that relationships are under threat or are vulnerable?
-
3.
Behavioral Dysregulation: individuals with BPD typically engage in a range of impulsive behaviors (which frequently function to reduce intense emotions) that cause problems for them, including self-injury and suicidal behavior, but also substance use, sexual behavior, binge eating, etc. Questions to assess behavioral dysregulation domain: Do you engage in any behaviors that cause problems for you when you experience intense emotions? Do you ever intentionally hurt yourself? Have you ever attempted to kill yourself? How many times?
-
4.
Cognitive Dysregulation: many times, individuals with BPD have experiences with thought dysregulation, including transient paranoia, dissociation, and depersonalization. Questions to assess cognitive dysregulation domain: Do you ever feel especially “spacey” or “checked out” when you’re under a great deal of stress? Do you ever think people are out to get you? Does this specifically happen in response to stress or intense emotions, or does it occur more generally? Are you sober when these things are occurring?
-
5.
Self Dysregulation: finally, individuals with BPD frequently report not knowing who they are as people, confusion about their identity, and chronic feelings of emptiness. Questions to assess self dysregulation domain: Have your thoughts about who you are as a person changed a lot over time? Do you have a sense of who you are as a person? Do you find that you act very different in one situation versus another? Have others noticed this? Do you ever feel a sense of emptiness? How often?
Identifying which domains of dysregulation are problematic in BPD may yield early foundations of a case formulation that indicates which areas may require greatest clinical attention. For example, individuals who exhibit problems in emotion and behavioral dysregulation domains may be especially likely to benefit from learning skills to tolerate distress, survive crises without making them worse, and regulate emotions. On the other hand, those who suffer extensively from interpersonal dysregulation may require greater emphasis on skills designed to promote communication, healthy relationships, and decrease isolation. However, it is important to note that such domains are not mutually exclusive. For example, careful assessment and case formulation may indicate that interpersonal dysregulation occurs as a result of emotion dysregulation (e.g., intense emotions accompanied by sense of loss of control prompts an individual to engage in behaviors that threaten the integrity of their relationships such as yelling, attacking, or withdrawing). In such a circumstance, enhancing emotion regulation skills will be essential to improving interpersonal dysregulation. Thus, as we discuss below, further assessment beyond the domains of dysregulation to what maintains them is imperative.
In addition to the five areas of dysregulation, it is critical at the start of, and throughout, treatment to conduct a careful assessment of life-threatening behaviors, including nonsuicidal self-injury. Individuals who meet criteria for BPD are at heightened risk for suicide, with studies reporting 8–10% dying by suicide (American Psychiatric Association, 2013; Leichsenring et al., 2011). In addition, many clients who are referred for DBT have a history of engaging in self-injury even if they don’t meet criteria for BPD. A history of non-suicidal self-injury is a strong risk factor for eventual suicide (Franklin et al., 2017). Thus, understanding the client’s risk factors for suicide, as well as protective factors, is necessary in order to fulfill the first goal of DBT treatment – keeping the client alive (in order to help them develop a life worth living).
The Linehan Risk Assessment and Management Protocol (L-RAMP; Linehan et al., 2012) is a commonly used tool in DBT to assess suicide risk. The L-RAMP includes assessment of acute risk and protective factors for suicide as well as strategies for the assessor or clinician to use based on risk level. When confronted with a suicide risk situation, it is easy for a clinician to be overwhelmed or frightened and therefore forget to assess critical information. The measure then can serve as an important tool that reminds the clinician to assess important domains (e.g., access to lethal means, intoxication, insomnia) and also guide decision making. In DBT, therapists are instructed to have access to the L-RAMP at all times whether it be paper copies in one’s office or online versions so that they can use it throughout treatment as needed. However, beyond knowing the risk factors, it is important to develop a case conceptualizing that indicates why these behaviors are occurring in the first place. In this way, case conceptualization, and the treatment plan that follows from it, form a critical backbone of DBT.
Case Conceptualization in DBT
The information provided by chain analyses (described below), along with other forms of assessment, lead to a precise case conceptualization in DBT. This assessment-driven approach to case formulation begins in the first pre-treatment session and continues throughout therapy wherein the case formulation constantly evolves in response to new information. Given the complex clinical presentations of individuals in DBT, it is imperative that therapists have a roadmap for assessment. Rizvi and Sayrs (2020) have described this case formulation approach at length and provided such a roadmap; it is summarized here.
The first step is to determine the stage of treatment the client is to be provided. As previously discussed, the marker of Stage 1 DBT is behavioral dyscontrol and most clients who are referred to DBT initially engage in out-of-control behaviors, such as suicide attempts, non-suicidal self-injury, substance use, risky sexual behaviors, etc. However, if it is not clear to the therapist, an assessment of the problems that brought the client to therapy as well as the behaviors that they wish to change, or that cause problems for them, is necessary. The second step is to assess the client’s goals: both for treatment (i.e., what she hopes to achieve by the end of treatment) and for life (i.e., “life worth living goals”). Understanding these goals is important for many reasons, not least of which is to develop a better awareness of the client’s experiences and hopes. However, knowing the client’s goals becomes an important tool for the therapist as they begin to link treatment activities to these goals. For example, a DBT therapist might (irreverently) say “the way you’re going to find someone with whom you want to settle down and have children is to first stop trying to kill yourself. You can’t have that relationship if you’re dead.”
The third step in case formulation, which is frequently an iterative process that develops over many sessions, is to create a preliminary target hierarchy. As described above, in Stage 1 DBT, the target hierarchy is to: (1) decrease (eliminate) life-threatening behaviors, (2) decrease therapy-interfering behaviors, and (3) decrease quality-of-life interfering behaviors. The DBT therapist must assess the presence of behaviors in each of these domains and, in the first few sessions of DBT, begin to organize them hierarchically. For example, if a client engages in both non-suicidal self-injury and substance use, the DBT therapist would know (and describe back to the client) that non-suicidal self-injury would be conceptualized as the most important target of treatment. This hierarchy does not mean that substance use would be completely ignored- it is often the case that the therapist can make strides on multiple behaviors at the same time, especially if they are functionally linked. However, the therapist is clear that non-suicidal self-injury takes priority as a behavior to be changed and organizes sessions and treatment tasks accordingly.
Organizing such a treatment hierarchy is somewhat clear when a client exhibits behavior that fall discretely into the categories of life-threatening behaviors and therapy-interfering behaviors. It becomes less clear, however, when the client’s engages in multiple quality-of-life interfering target behaviors. Which target is the therapist to prioritize, for example, when the client exhibits binge eating, problematic alcohol use, and shop lifting, but does not exhibit life-threatening behaviors or therapy-interfering behaviors? To this end, Persons (2008) has delineated several key factors to consider when determining target priorities including whether some problems interfere with solving others (e.g., substance use, housing instability), and which problems clients are most motivated to change. Such considerations may be useful when therapists find themselves in the fortunate circumstances of having no life-threatening behaviors or therapy-interfering behaviors to target.
Once developed, the target hierarchy may change as new information is gathered or new behavior occurs. For example, a therapist and client may be working systematically on reducing non-suicidal self-injury when the client suddenly reports a significant increase in urges to kill herself. This suicide risk then takes precedence and needs to be addressed. Alternatively, the therapist may have developed a target hierarchy based on careful assessment in the first couple of sessions but, as therapy progresses, a number of therapy interfering behaviors may appear (e.g., chronic lateness to session, not doing assigned tasks) that weren’t known at the beginning of treatment. The therapist then reformulates her target hierarchy to incorporate this new information.
Once the target hierarchy is established, the next step in the case formulation plan is to assess and treat the highest-order target. Assessment is done via one or many chain analyses of instances of the target behavior in order to identify controlling variables (described more below) and identify points of intervention (i.e., solutions).
Chain Analysis
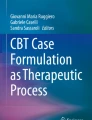
The primary method of assessment in DBT is the chain analysis. Chain analysis is a form of behavioral analysis that zeroes in on one specific instance of behavior and assesses all the variables (internal and external) immediately leading up to the behavior as well as the consequences (Koerner, 2012; Linehan, 1993; Rizvi & Ritschel, 2014; Rizvi, 2019). Figure 1 shows an example of a chain analysis of a suicide attempt. As a behavior therapy, DBT focuses on understanding a behavior with precision in order to be able to change it effectively. Accordingly, a chain analysis – which focuses on what often seems like an excruciating level of detail to the client – allows for the therapist to understand the controlling variables, develop an accurate case formulation, and then be more likely to propose and implement solutions that will actually work.

Example chain analysis of a suicide attempt
Chain analysis is described in detail elsewhere (Rizvi, 2019). However, in short: chain analysis involves a moment-by-moment examination of the variables that led to and followed a problem behavior, and groups them into five categories. The target behavior is, as it sounds, the behavior being analyzed. Once the target behavior has been established, therapists work to identify its prompting event, which is the event that precipitates the target behavior. In other words, had the prompting event not occurred, the target behavior would likely not have occurred. Prompting events provide essential information regarding what variables control target behaviors and need to be addressed in therapy. In Fig. 1, the prompting event is a critical comment from the client’s mother. Links in the chain include the events, emotions, thoughts, and actions that link the prompting event to the target behavior. Establishing links is critical because it provides the therapist with information regarding what clients could do at various points to “get off the chain” that leads to a target behavior, and onto a new chain of behaviors that is more aligned with their goals. Vulnerability factors are variables that are more distal from the target behavior, and “give the prompting event power” by increasing client’s vulnerability to be adversely impacted by it. Lack of sleep, substance use, hunger, a conflictual history with another individual, and already having a “bad day” are common vulnerability factors reported by clients in DBT. Finally, consequences provide key information regarding whether target behaviors may be reinforced or maintained through operant conditioning principles in some way (Rizvi, 2019). In Fig. 1, a client’s suicide attempt may be negatively reinforced by the decreased shame and anger, as well as positively reinforced by the increase in care from her mother, that followed after it.
Based on the backbone of case formulation provided through detailed chain analyses, the solution analysis that follows involves clients and therapists discussing potential solutions to various components of the chain that, if implemented in the future, could prevent a similar chain of behaviors from occurring. For example, in Fig. 1, potential solutions could occur early in the chain by reducing vulnerability factors (e.g., sleeping earlier, having regular meals), and using DBT skills designed to modify unhelpful cognitions (e.g., working to alter unhelpful cognitions such as “she thinks I’m a waste of space”). If the client did not implement these solutions, or they were ineffective, they may intervene at later points including using a range of emotion regulation skills to down-regulate shame or avoid acting on anger-related urges (e.g., preventing throwing a mug into the sink). Another solution may involve the client using interpersonal effectiveness skills to communicate with her mother in a way that is more effective than throwing a mug into the sink which elicited subsequent escalations. Finally, additional solutions may be relevant to points in the chain that are quite proximal to the target behavior, such as calling one’s therapist or using crisis survival skills to resist suicide urges or decrease emotional intensity (e.g., splashing cold water on one’s face, intense exercise, paced breathing). This solution analysis informs the crux of the DBT therapist’s broader treatment plan. For example, based on their chain analysis, the therapist of the client whose chain is displayed in Fig. 1 now knows that emotion regulation skills training, crisis survival skills training, and targeting negative cognitions that follow from other’s criticism may be essential to treating suicidal behavior.
Once solutions are identified, assessment continues by monitoring outcomes (did the solution work?) and making adjustments as needed. If a solution based on a chain analysis does not have the intended effect, then the therapist assesses what went wrong. The solution may have been based on an incomplete assessment and therefore the therapist needs to look for what was missing from his initial assessment. This careful re-examination can represent the “dialectical assessment” strategy in DBT which is the practice of looking for “what is being left out” of our conceptualization that contributes to lack of understanding of the problem. Following resolution of the target behavior, chain analyses and solution implementation steps are repeated for the next target behavior. In this way, DBT reflects an ongoing cycle of assessment, formulation, solution generation, solution implementation, and solution evaluation.
The same focus on careful assessment also extends to other target behaviors beyond life-threatening behaviors. Chain analyses is used throughout treatment to assess target behaviors until a thorough understanding is achieved (Rizvi, 2019) and solutions based on assessment are effective at changing the behavior. For example, a chain analysis might be used to address lateness to session, an episode of risky sexual behavior, or substance use. Chain analysis is not a tool used to assess life-threatening behaviors per se but rather a method of generating a particularly precise behavioral case formulation to inform an equally precise treatment plan. Thus, chain analysis strategies are virtually unchanged regardless of the topography of the behavior being analyzed and whether it is life-threatening in nature or not.
Similarities and Differences Between DBT and Other Therapies
Similarities
DBT is drawn from the long and rich tradition of behavior therapy. As such, it owes many of its core features to the earlier forms of behavioral therapy from which it came. All “change-focused” strategies in DBT are derived from what are now termed “first” and “second wave” behavior therapy interventions. Problem assessment derived from older behavior therapy traditions (e.g., Kanfer & Saslow, 1965), such as macro-level behavioral assessments (e.g., examining antecedents, behaviors, and consequences), are frequently used in DBT to guide case formulation and subsequent intervention efforts. DBT expands on these behavioral assessment approaches with chain analyses to provide more granular levels of detail regarding the controlling variables of client behavior (see description of chain analysis, above).
One of the most pertinent pieces of information gleaned from behavioral or chain analyses is identification of the controlling variables influencing problematic behaviors. Four types of controlling variables are theorized to be potentially involved in clients’ problem behaviors: skills deficits, problematic conditioned emotional reactions, problematic cognitions, or problematic contingencies (see Koerner, 2012). All of these controlling variables can be targeted using standard technologies provided by first and second waves of behavior therapies. Skills deficits are frequently addressed by training clients in the skills that they are deficient in through an iterative process of skills acquisition, strengthening, and generalization. Problematic conditioned emotional responses may be targeted through the use of exposure to extinguish relationships between unconditioned and conditioned stimuli. For example, clients who have developed a problematic response of shame whenever they hear a particular song because it reminds them of a highly critical parent who played it may listen to the song repeatedly in therapy in order to extinguish the relationship between the song, the abusive parent, and the associated shame response. Such an approach is highly consistent with those evident in contemporary exposure-based therapies (e.g., Abramowitz et al., 2019). Furthermore, problematic cognitions may be targeted through cognitive intervention approaches derived from second wave behavior therapies such as Beck’s Cognitive Behavioral Therapy and Ellis’ Rational Emotive Behavior Therapy (Beck et al., 1979; Ellis, 1962, 1973).
DBT also draws heavily on contingency management approaches to target problematic contingencies, including the use of reinforcement, extinction, and, where appropriate, punishment. Adaptive, desirable behaviors are reinforced, while maladaptive, problematic behaviors are extinguished or punished. Clinicians are also vigilant for signs that they are reinforcing problematic behaviors and adjust their own behavior accordingly. For example, a behavioral analysis might reveal that a client’s yelling behavior is prompted by the clinician raising an uncomfortable subject, such as an ongoing pattern of disordered eating. The clinician may inadvertently reinforce the yelling behavior by withdrawing the aversive stimulus (i.e., the discussion of disordered eating) in response to it. Given such a formulation, a DBT clinician might therefore work to hold the aversive cue in response to the yelling behavior (i.e., continue to discuss disordered eating), perhaps only removing it when the client engages in alternative and adaptive behaviors (i.e., discussing the issue calmly). Such an approach is directly aligned with contingency management interventions.
Akin to some behavioral approaches (i.e., Functional Analytic Therapy, FAP; Kohlenberg & Tsai, 1991), DBT emphasizes that behavioral principles such as contingency management and observational learning shape and inform the therapeutic relationship. Thus, just as the therapist’s behaviors can reinforce or punish the client’s, the client’s behaviors can reinforce or punish that of the therapist’s. DBT clinicians are thus attentive to psychotherapy process through a behavioral lens, and are advised to elicit and reinforce target adaptive behaviors and avoid reinforcing target maladaptive behaviors (Kohlenberg & Tsai, 1991). For example, when the same client exhibits a willingness to discuss disordered eating without yelling, a clinician may respond with natural reinforcers such as leaning forward, increasing warmth, and sharing expressions of caring. This emphasis on behavioral principles within the therapy process itself aligns DBT with Functional Analytic Approaches (Kohlenberg & Tsai, 1991), and distinguishes it from other behavioral approaches (e.g., exposure; Abramowitz et al., 2019), where it is relatively de-emphasized.
Differences
Although DBT arguably has more points of overlap than divergence with other behavior therapies, there are some key differences.
Dialectics: Integration of Acceptance and Change
Most notably, the integration of Zen Buddhism (Masuda & O’Donohue, 2017) into behavioral therapy is a substantive point of departure between DBT and other forms of behavior therapy that have been called “first” and “second” wave interventions (Hayes et al., 2004). Indeed, the integration of acceptance-based approaches was fomented by Linehan’s failed initial attempts at the application of standard behavior therapy to individuals with BPD.
It is notable that other modalities – often grouped under the heading of “third wave approaches” – have similarly integrated mindfulness and acceptance into behavioral therapy interventions (e.g., Acceptance and Commitment Therapy; Hayes, 2004; Hayes et al., 2004). DBT is therefore not entirely unique in the synthesis of acceptance and change. Where DBT is unique, however, is its use of dialectical philosophy to unite and underpin the two. The dialectical philosophy underpins virtually every element of DBT, because DBT is premised upon a dialectical worldview which assumes that reality is always changing, in transaction, and responding to itself. According to the dialectical worldview, all things are interrelated and in polarity with one another, and the interplay of these polarities and consequent syntheses that arise from them allow truth to evolve in a continually changing fashion. For example, a client may acknowledge both grief and relief at the death of an abusive parent. From a dialectical perspective, the client may need to recognize the inherent truth and validity at both ends of such a dialectic to allow their understanding to evolve and give way to a new series of dialectical polarizations.
The dialectical philosophy permeates DBT in a number of tangible ways. First, any specific strategy applied by a DBT clinician in a particular moment in time is informed by a dialectical approach that seeks to balance acceptance with change. Clinicians thus regularly interrogate whether they have become overly committed to change (e.g., pushing a client to stop self-harming, resulting in increasing refusal from the client (polarization)) or acceptance (e.g., giving up pursuing the client’s self-harm behavior). Second, clinicians, clients, and DBT teams are prompted to search for “what is missing” from their understanding in order to ensure that their perception of reality has not become rigidly attached to one end of a polarity or another. Third, clinicians also help their clients to alter their thinking from non-dialectical, mutually exclusive absolutes (e.g., “You say you care for me but you’re telling me you won’t talk to me on the phone tonight”) to ones that are dialectical in nature (e.g., “You care for me and you won’t talk to me on the phone tonight”). Indeed, even DBT consultation teams attend to potential such polarizations within themselves and their teams and encourage each other to search for what is missing in order to illuminate more dialectical truths.
Principles Versus Protocols
Another key difference between DBT and other behavioral therapies reflects the use of treatment protocols. Several cognitive and cognitive behavioral therapies involve the administration of fixed protocols that progress in a pre-specified order (e.g., Barlow et al., 2011; Hope et al., 2019; Resick et al., 2016). Administration of such fixed protocols are challenging in the context of BPD because high levels of chaos, multiple problems, and rapidly changing clinical presentations associated demand rapidly changing interventions and can quickly derail a protocol. Rather than a protocol-based therapy, DBT contains protocols (e.g., for managing suicidal, crisis, or therapy-interfering behaviors) which are flexibly utilized based on a set of principles that inform what protocols and DBT strategies to draw on and when. The target hierarchy in Stage 1 of DBT is an example of one such principle. Similarly, the use of chain analysis is used to build a case formulation, which guides the selection and implementation of DBT strategies throughout the treatment, is another such example. Accordingly, the strategies observed within an “adherent” DBT session may vary widely across clients and sessions.
DBT Assumptions
Finally, working with suicidal or self-harming people with BPD can be frightening, frustrating, and exhausting for clinicians. When burned out, clinicians run the risk of becoming rigid, judgmental, or interpreting client behaviors in unhelpful or therapy-interfering ways (e.g., assuming clients are “seeking attention” or “do not want” to get better). In order to avoid this and maintain an effective, compassionate, and non-judgemental stance, DBT clinicians agree to hold to specific “assumptions” about their clients and the therapy itself. For example, DBT clients are assumed to be doing the best they can and that they want to change. However, dialectically, an additional assumption is that they “need to do better, try harder, and be more motivated to change” (pp. 106, Linehan, 1993). These assumptions are part of the foundation of DBT and are in place to guide case formulations and clinical decision-making throughout treatment. In this way, the DBT assumptions may serve as something of a “lighthouse,” guiding clinicians away from judgments and conjecture and back to clarity and openness to new information. These assumptions are unique to DBT and capture its individual “ethos.”
Training and Certification in DBT
As has been made clear in this chapter, DBT is a complex treatment for a complex population. Learning to conduct DBT according to all the principles and using all the strategies can take significant training, especially if one comes to DBT from a non-behavioral background. Currently the “gold standard” approach to learning DBT is to participate in an “intensive” training sequence with a team of fellow clinicians (that transitions to form a consultation team). An intensive training can take different forms; a common version involves two 5-day trainings spaced about 6 months apart. During the months between the two trainings, therapists are expected to do a number of homework assignments and begin implementing DBT with individual and skills group clients. Increasingly, DBT training programs have been established in graduate training clinics in psychology and social work (see Lungu et al., 2012; Rizvi et al., 2017) thus creating more opportunities to learn the treatment earlier in one’s developmental training.
In 2014, Linehan established the DBT- Linehan Board of Certification (DBT-LBC; dbt-lbc.org). The board certification process in DBT was developed in order to identify clinicians and programs that reliably offered DBT in a manner that conforms to the evidence-based research for the treatment. The prerequisites for certification include, among others, a minimum of 40 h of didactic training, 12-months of participation on a DBT consultation team, at least three clients treated through Stage 1 of DBT, experience teaching all the skills, and a regular ongoing mindfulness practice. Although this process may appear arduous to the aspiring DBT clinician, we proffer that the impact this treatment can make in client’s lives is well worth the effort.
Conclusion
DBT is built on a rich foundation of behavior therapy traditions and, through its innovative blend of dialectical philosophy, Zen Buddhism, and radical behaviorism, extends and enriches these foundations. Ultimately, DBT is a therapy that rests heavily on precise case formulation and the treatment plans that follow from it. Such case formulations are developed through the rigorous assessment procedures that were developed by radical behaviorists throughout the history of behavioral therapy. Similarly, many of the interventions that follow from these formulations have been developed and refined by many behavioral predecessors of DBT. For DBT clinicians, it is behavioral precision, devotion to assessing rather than inferring, and a commitment to precisely targeting controlling variables, paired with acceptance principles espoused by Zen Buddhism, that helps clients build lives worth living. Although DBT may differ from other behavioral therapies in its integration of acceptance-based philosophies, principles over protocols, and a range of assumptions that are central to the treatment, the underpinning emphasis on precision in formulating and targeting behaviors is a shared feature that lives in the “DNA” of DBT, along with its behavioral therapy family members.
References
Abramowitz, J. S., Beacon, B. L., & Whiteside, S. P. H. (2019). Exposure therapy for anxiety: Principles and practice (2nd ed.). Guilford Press.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association.
Arens, E. A., Grabe, H., Spitzer, C., & Barnow, S. (2011). Testing the biosocial model of borderline personality disorder: Results of a prospective 5-year longitudinal study. Personality and Mental Health, 5, 29–42.
Austin, M. A., Rinolio, T. C., & Porges, S. W. (2007). Borderline personality disorder and emotion regulation: Insights from the Polyvagal Theory. Brain and Cognition, 65, 69–76.
Balsis, S., Loehle-Conger, E., Busch, A. J., Ungredda, T., & Oltmanns, T. F. (2018). Self and informant report across the borderline personality disorder spectrum. Personality Disorders, Theory, Research, and Treatment, 9, 429–436. https://doi.org/10.1037/per0000259
Barlow, D. H., Farchione, T. J., Fairholme, C. P., Ellard, K. K., Boisseau, C. L., Allen, L. B., & Ehrenreich-May, J. (2011). Treatments that work. Unified protocol for transdiagnostic treatment of emotional disorders: Therapist guide. Oxford University Press.
Barnicot, K., Savill, M., Bhatti, N., & Priebe, S. (2014). A pragmatic randomised controlled trial of dialectical behaviour therapy: Effects on hospitalisation and post-treatment follow-up. Psychotherapy and Psychosomatics, 83, 192–193. https://doi.org/10.1159/000357365
Beck, A., Rush, J. T. A., Shaw, B., & Emery, G. (1979). Cognitive therapy of depression. Guilford Press.
Bennet, C., Melvin, G. A., Quek, J., Saeedi, N., Gordon, M. S., & Newman, L. K. (2019). Perceived invalidation in adolescent borderline personality disorder: An investigation of parallel reports of caregiver resposnes to negative emotions. Child Psychiatry and Human Development, 50, 209–221.
Biskin, R. S., & Paris, J. (2012). Diagnosing borderline personality disorder. CMAJ, 184, 1789–1794. https://doi.org/10.1503/cmaj.090618
Bohus, M., & Priebe, K. (2018). DBT-PTSD: A treatment programme for complex PTSD after childhood abuse. In M. A. Swales (Ed.), The Oxford handbook of dialectical behaviour therapy. Oxford Univeristy Press.
Bouchard, S., Sabourin, S., Lussier, Y., & Villeneuve, E. (2009). Relationship quality and stability in couples when one partner suffers from borderline personality disorder. Journal of Marital and Family Therapy, 35, 446–455.
Carter, G. L., Willcox, C. H., Lewin, T. J., Conrad, A. M., & Bendit, N. (2010). Hunter DBT project: Randomized controlled trial of dialectical behaviour therapy in women with borderline personality disorder. Australian and New Zealand Journal of Psychiatry, 44, 162–173. https://doi.org/10.3109/00048670903393621
Clarkin, J. F., Levy, K. N., Lenzenweger, M. F., & Kernberg, O. F. (2007). Evaluating three treatments for borderline personality disorder: A multiwave study. American Journal of Psychiatry, 164, 922–928. https://doi.org/10.1176/ajp.2007.164.6.922
Crowell, S. E., Beauchaine, T. P., & Linehan, M. M. (2009). A biosocial developmental model of borderline personality: Elaborating and extending Linehan’s theory. Psychological Bulletin, 135, 495–510. https://doi.org/10.1037/a0015616
DeCou, C. R., Comtois, K. A., & Landes, S. J. (2019). Dialectical behavior therapy is effective for the treatment of suicidal behavior: A meta-analysis. Behavior Therapy, 50, 60–72. https://doi.org/10.1016/j.beth.2018.03.009
Ellis, A. (1962). Reason and emotion in psychotherapy. Citadel.
Ellis, A. (1973). Humanistic psychotherapy: The rational-emotive approach. McGraw-Hill.
Feigenbaum, J. D., Fonagy, P., Pilling, S., Jones, A., Wildgoose, A., & Bebbington, P. E. (2012). A real-world study of the effectiveness of DBT in the UK National Health Service. British Journal of Clinical Psychology, 51, 121–141. https://doi.org/10.1111/j.2044-8260.2011.02017.x
Fleming, A. P., McMahon, R. J., Moran, L. R., Peterson, A. P., & Dreessen, A. (2015). Pilot randomized controlled trial of dialectical behavior therapy group skills training for ADHD among college students. Journal of Attention Disorders, 19, 260–271. https://doi.org/10.1177/1087054714535951
Franklin, J. C., Ribeiro, J. D., Fox, K. R., Bentley, K. H., Kleiman, E. M., Huan, X., et al. (2017). Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychological Bulletin, 143, 187–232. https://doi.org/10.1037/bul0000084
Goldstein, T. R., Fersch-Podrat, R. K., Rivera, M., Axelson, D. A., Merranko, J., Yu, H., Brent, D. A., & Birmaher, B. (2015). Dialectical Behavior Therapy for adolescents with bipolar disorder: Results from a pilot randomized trial. Journal of Child and Adolescent Psychopharmacology, 25, 140–149. https://doi.org/10.1089/cap.2013.0145
Goodman, M., Banthin, D., Blair, N. J., Mascitelli, K. A., Wilsnack, J., Chen, J., Messenger, J. W., Perez-Rodriguez, M. M., Triebwasser, J., Koenigsberg, H. W., Goetz, R. R., Hazlett, E. A., & New, A. S. (2016). A randomized trial of dialectical behavior therapy in high-risk suicidal veterans. The Journal of Clinical Psychiatry, 77, e1591–e1600. https://doi.org/10.4088/JCP.15m10235
Harned, M. S., Korslund, K. E., Foa, E. B., & Linehan, M. M. (2012). Treating PTSD in suicidal and self-injuring women with borderline personality disorder: Development and preliminary evaluation of a dialectical behavior therapy prolonged exposure protocol. Behaviour Research and Therapy, 50, 381–386.
Hayes, S. C. (2004). Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behavior Therapy, 35, 639–665. https://doi.org/10.1016/S0005-7894(04)80013-3
Hayes, S. C., Follette, V. M., & Linehan, M. M. (2004). Mindfulness and acceptance: Expanding the cognitive-behavioural tradition (pp. 1–29). Guilford Press.
Hill, J., Stepp, S., Wan, M., Hope, H., Morse, J., Steele, M., et al. (2011). Attachment, borderline personality, and romantic relationship dysfunction. Journal of Personality Disorders, 25, 789–805.
Hope, D. A., Heimberg, R. G., & Turk, C. L. (2019). Managing social anxiety, therapist guide: A cognitive-behavioral therapy approach. Oxford University Press.
Kanfer, F. H., & Saslow, G. (1965). Behavioral analysis: An alternative to diagnostic classification. Archives of General Psychiatry, 12, 529–538. https://doi.org/10.1001/archpsyc.1965.01720360001001
Koerner, K. (2012). Doing dialectical behavior therapy: A practical guide. Guilford Press.
Kohlenberg, R. J., & Tsai, M. (1991). Functional analytic psychotherapy: Creating intense and curative therapeutic relationships. Springer.
Koons, C. R., Robins, C. J., Lindsey Tweed, J., Lynch, T. R., Gonzalez, A. M., Morse, J. Q., Bishop, G. K., Butterfield, M. I., & Bastian, L. A. (2001). Efficacy of dialectical behavior therapy in women veterans with borderline personality disorder. Behavior Therapy, 32, 371–390. https://doi.org/10.1016/S0005-7894(01)80009-5
Koons, C. R. (2021). DBT beyond Stage 1: An overview of Stages 2, 3, and 4. In L. A. Dimeff, S. L.Rizvi, & K. Koerner (Eds.), Dialectical behavior therapy in clinical practice: Applications across disorders andsettings (pp. 306–326). The Guilford Press.
Kopala-Sibley, D. C., Zuroff, D. C., Russell, J. J., Moskowitz, D. S., & Paris, J. (2012). Understanding heterogeneity in borderline personality disorder: Differences in affective reactivity explained by the traits of dependency and self-criticism. Journal of Abnormal Psychology, 121, 680–691. https://doi.org/10.1037/a0028513
Leichsenring, F., Leibing, E., Kruse, J., New, A. S., & Leweke,F. (2011). Borderline personality disorder. Lancet (London, England), 377(9759), 74–84. https://doi.org/10.1016/S0140-6736(10)61422-5
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. Guilford Press.
Linehan, M. M., & Wilks, C. R. (2018). The course and evoluation of dialectical behavior therapy. The American Journal of Psychotherapy, 69, 97–110. https://doi.org/10.1176/appi.psychotherapy.2015.69.2.97
Linehan, M. M., Armstrong, H. E., Suarez, A., Allmon, D., & Heard, H. L. (1991). Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Archives of General Psychiatry, 48, 1060–1064. https://doi.org/10.1001/archpsyc.1991.01810360024003
Linehan, M. M., Heard, H. L., & Armstrong, H. E. (1993). Naturalistic follow-up of a behavioral treatment for chronicallyparasuicidal borderline patients. Archives of General Psychiatry, 50, 971–974. https://doi.org/10.1001/archpsyc.1993.01820240055007
Linehan, M. M., Schmidt, H., Dimeff, L. A., Craft, J. C., Kanter, J., & Comtois, K. A. (1999). Dialectical behavior therapy for patients with borderline personality disorder and drug-dependence. American Journal on Addictions, 8, 279–292. https://doi.org/10.1080/105504999305686
Linehan, M. M., Dimeff, L. A., Reynolds, S. K., Comtois, K. A., Welch, S. S., Heagerty, P., & Kivlahan, D. R. (2002). Dialectical behavior therapy versus Comprehensive Validation Therapy plus 12-step for the treatment of opioid dependent women meeting criteria for borderline personality disorder. Drug and Alcohol Dependence, 67, 13–26. https://doi.org/10.1016/S0376-8716(02)00011-X
Linehan, M. M., Comtois, K. A., & Ward-Ciesielski, E. F. (2012). Assessing and managing risk with suicidal individuals. Cognitive and Behavioral Practice,19(2), 218–232.
Linehan, M. M., Comtois, K. A., Murray, A. M., Brown, M. Z., Gallop, R. J., Heard, H. L., Korslund, K. E., Tutek, D. A., Reynolds, S. K., & Lindenboim, N. (2006). Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Archives of General Psychiatry, 63, 757–766. https://doi.org/10.1001/archpsyc.63.7.757
Linehan, M. M., McDavid, J. P., Brown, M. Z., Sayrs, J. H. R., & Gallop, R. J. (2008). Olanzapine plus dialectical behavior therapy for women with high irritability who meet criteria for borderline personality disorder: A double-blind, placebo-controlled pilot study. Journal of Clinical Psychiatry, 69, 999–1005. https://doi.org/10.4088/JCP.v69n0617
Linehan, M. M., Korslund, K. E., Harned, M. S., Gallop, R. J., Lungu, A., Neacsiu, A. D., McDavid, J., Comtois, K. A., & Murray-Gregory, A. M. (2015). Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: A randomized clinical trial and component analysis. JAMA Psychiatry, 72(5), 475–482. https://doi.org/10.1001/jamapsychiatry.2014.3039
Lungu, A., Gonzalez, M. R., & Linehan, M. M. (2012). Implementing a dialectical behavior therapy training program for graduate students. The Behavior Therapist, 35, 4–11.
Lynch, T. R., Morse, J. Q., Mendelson, T., & Robins, C. J. (2003). Dialectical behavior therapy for depressed older adults: A randomized pilot study. American Journal of Geriatric Psychiatry, 11, 33–45. https://doi.org/10.1097/00019442-200301000-00006
Masuda, A., & O’Donohue, W. T. (2017). Handbook of Zen, mindfulness, and behavioral health. Springer.
McCauley, E., Berk, M. S., Asarnow, J. R., Adrian, M., Cohen, J., Korslund, K., Avina, C., Hughes, J., Harned, M., Gallop, R., & Linehan, M. M. (2018). Efficacy of dialectical behavior therapy for adolescents at high risk for suicide a randomized clinical trial. JAMA Psychiatry, 75, 777–785. https://doi.org/10.1001/jamapsychiatry.2018.1109
McMain, S. F., Links, P. S., Gnam, W. H., Guimond, T., Cardish, R. J., Korman, L., & Streiner, D. L. (2009). A randomized trial of dialectical behavior therapy versus general psychiatric management for borderline personality disorder. American Journal of Psychiatry, 166, 1365–1374. https://doi.org/10.1176/appi.ajp.2009.09010039
McMain, S. F., Guimond, T., Barnhart, R., Habinski, L., & Streiner, D. L. (2017). A randomized trial of brief dialectical behaviour therapy skills training in suicidal patients suffering from borderline disorder. Acta Psychiatrica Scandinavica, 135, 138–148. https://doi.org/10.1111/acps.12664
Mehlum, L., Tørmoen, A. J., Ramberg, M., Haga, E., Diep, L. M., Laberg, S., Larsson, B. S., Stanley, B. H., Miller, A. L., Sund, A. M., & Grøholt, B. (2014). Dialectical behavior therapy for adolescents with repeated suicidal and self-harming behavior: A randomized trial. Journal of American Academy of Child and Adolescent Psychiatry, 53, 1082–1091. https://doi.org/10.1016/j.jaac.2014.07.003
Mehlum, L., Ramberg, M., Tørmoen, A. J., Haga, E., Diep, L. M., Stanley, B. H., Miller, A. L., Sund, A. M., & Grøholt, B. (2016). Dialectical behavior therapy compared with enhanced usual care for adolescents with repeated suicidal and self-harming behavior: Outcomes over a one-year follow-up. Journal of the American Academy of Child and Adolescent Psychiatry, 55, 295–300. https://doi.org/10.1016/j.jaac.2016.01.005
Neacsiu, A. D., Eberle, J. W., Kramer, R., Wiesmann, T., & Linehan, M. M. (2014). Dialectical behavior therapy skills for transdiagnostic emotion dysregulation: A pilot randomized controlled trial. Behaviour Research and Therapy, 59, 40–51. https://doi.org/10.1016/j.brat.2014.05.005
Persons, J. B. (2008). Developing an initial case formulation and setting treatment goals. In The case formulation approach to cognitive-behavior therapy (pp. 126–149). Guilford Press.
Pistorello, J., Fruzzetti, A. E., MacLane, C., Gallop, R., & Iverson, K. M. (2012). Dialectical behavior therapy (DBT) applied to college students: A randomized clinical trial. Journal of Consulting and Clinical Psychology, 80, 982–994. https://doi.org/10.1037/a0029096
Priebe, S., Bhatti, N., Barnicot, K., Bremner, S., Gaglia, A., Katsakou, C., Molosankwe, I., McCrone, P., & Zinkler, M. (2012). Effectiveness and cost-effectiveness of dialectical behaviour therapy for self-harming patients with personality disorder: A pragmatic randomised controlled trial. Psychotherapy and Psychosomatics, 81, 356–365. https://doi.org/10.1159/000338897
Resick, P. A., Monson, C. M., & Chard, K. M. (2016). Cognitive processing therapy for PTSD: A comprehensive manual. Guilford.
Rizvi, S. L. (2019). Chain analysis in dialectical behavior therapy. The Guilford Press.
Rizvi, S. L., Hughes, C. D., Hittman, A. D., & Vieira Oliveira, P. (2017). Can trainees effectively deliver dialectical behavior therapy for individuals with borderline personality disorder? Outcomes from a training clinic. Journal of Clinical Psychology, 73, 1599–1611.
Rizvi, S. L., & Ritschel, L. A. (2014). Mastering the art of chain analysis in dialectical behavior therapy. Cognitiveand Behavioral Practice, 21(3), 335–349. https://doi.org/10.1016/j.cbpra.2013.09.002
Rizvi, S. L., & Sayrs, J. H. R. (2020). Assessment-driven case formulation and treatment planning in dialectical behaviour therapy: Using principles to guide effective treamtent. Cognitive and Behavioral Practice, 27, 2–17. https://doi.org/10.1016/j.cbpra.2017.06.002
Rosenthal, M. Z., Gratz, K. L., Kosson, D. S., Cheavens, J. S., Lejuez, C. W., & Lynch, T. R. (2008). Borderline personality disorder and emotional responding: A review of the research literature. Clinical Psychology Review, 28, 75–91. https://doi.org/10.1016/j.cpr.2007.04.001
Safer, D. L., Robinson, A. H., & Jo, B. (2010). Outcome from a randomized controlled trial of group therapy for binge eating disorder: Comparing dialectical behavior therapy adapted for binge eating to an active comparison group therapy. Behavior Therapy, 41, 106–120. https://doi.org/10.1016/j.beth.2009.01.006
Shelton, D., Sampl, S., Kesten, K. L., Zhang, W., & Trestman, R. L. (2009). Treatment of impulsive aggression in correctional settings. Behavioral Sciences & the Law, 27, 787–800. https://doi.org/10.1002/bsl.889
Soler, J., Pascual, J. C., Tiana, T., Cebrià, A., Barrachina, J., Campins, M. J., Gich, I., Alvarez, E., & Pérez, V. (2009). Dialectical behaviour therapy skills training compared to standard group therapy in borderline personality disorder: A 3-month randomised controlled clinical trial. Behaviour Research and Therapy, 47, 353–358. https://doi.org/10.1016/j.brat.2009.01.013
Staebler, K., Helbing, E., Rosenbach, C., & Renneberg, B. (2011). Rejection sensitivity and borderline personality disorder. Clinical Psychology & Psychotherapy, 18, 275–283.
Telch, C. F., Agras, W. S., & Linehan, M. M. (2001). Dialectical behavior therapy for binge eating disorder. Journal of Consulting and Clinical Psychology, 69, 1061–1065. https://doi.org/10.1037/0022-006X.69.6.1061
Van Den Bosch, L. M. C., Verheul, R., Schippers, G. M., & Van Den Brink, W. (2002). Dialectical Behavior Therapy of borderline patients with and without substance use problems: Implementation and long-term effects. Addictive Behaviors, 27, 911–923. https://doi.org/10.1016/S0306-4603(02)00293-9
Van Dijk, S., Jeffrey, J., & Katz, M. R. (2013). A randomized, controlled, pilot study of dialectical behavior therapy skills in a psychoeducational group for individuals with bipolar disorder. Journal of Affective Disorders, 145, 386–393. https://doi.org/10.1016/j.jad.2012.05.054
Verheul, R., Van Den Bosch, L. M. C., Koeter, M. W. J., De Ridder, M. A. J., Stijnen, T., & Van Den Brink, W. (2003). Dialectical behaviour therapy for women with borderline personality disorder: 12-month, randomised clinical trial in The Netherlands. British Journal of Psychiatry, 182, 135–140. https://doi.org/10.1192/bjp.182.2.135
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Fitzpatrick, S., Rizvi, S.L. (2022). Dialectical Behavior Therapy: Assessment and Case Conceptualization. In: O'Donohue, W., Masuda, A. (eds) Behavior Therapy. Springer, Cham. https://doi.org/10.1007/978-3-031-11677-3_8
Download citation
DOI: https://doi.org/10.1007/978-3-031-11677-3_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-11676-6
Online ISBN: 978-3-031-11677-3
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)