
Abstract
Immune costimulatory checkpoints are crucial in regulating both lymphocyte activation and function. They also serve a major role in foreign antigen specificity and self-tolerance. The two major families of checkpoint inhibitors target the CTLA-4/B7s and the PD-1/PD-L1 axis. Inhibition of either of these two pathways intends to enhance the antitumor activity of lymphocytes. The risk of infections associated with checkpoint inhibition can be explained by two major mechanisms: the use of corticosteroids for the treatment of autoimmune inflammatory reactions and immune-mediated cytopenia. The overall risk of infections with immune checkpoint inhibitors is considered to be low, with bacterial infections being most frequent. For this reason, no prophylaxis is recommended with the use of checkpoint inhibitors. Recent research suggests that these drugs may be efficacious in treating specific infectious syndromes (such as sepsis, HIV infection, progressive multifocal leukoencephalopathy, hepatitis B, fungal infections, and COVID-19) but more data is needed to recommend its use.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction to Immune Checkpoint Blockade
Appropriate and effective functioning of the immune system requires a delicate balance between activation against foreign antigens and tolerance to self-molecules. The disruption of this balance is evident in immunosuppressed or immunocompromised individuals who have significantly increased susceptibility to infectious agents or reactivation of immunologically suppressed pathogens. A prime example of this phenomenon is observed in human immunodeficiency virus (HIV)-acquired immunodeficiency syndrome (AIDS) patients who are prone to opportunistic fungal infections such as cryptococcal meningitis. On the other hand, the lack of an appropriate self-antigen tolerance can manifest into severe autoimmune diseases such as type I diabetes mellitus.
The defining characteristics of foreign antigen specificity and self-tolerance are mediated by the adaptive immunity and their main cellular effectors – lymphocytes. An essential component in the maintenance of the immunological balance of specificity and tolerance is the immune costimulatory checkpoints that are crucial in regulating lymphocyte activation and function. Cytotoxic T-lymphocyte antigen (CTLA)-4 and the programmed cell death (PD)-1/PD-L1 axes are two well-characterized immune checkpoints which are foundational as immunotherapeutic targets and will be discussed in further detail.
CTLA-4 Immune Checkpoint
Activation and subsequent regulation of T-lymphocytes are determined through a combination of stimulatory and/or inhibitory signals. One such regulatory checkpoint is dependent on the CD28 receptor, which is important in the antigen priming and activation of naïve T cells. These immune cells utilize T-cell receptors (TCR) for recognition of a specific antigen presented on the appropriate major histocompatibility complex (MHC) molecule, which provides an initial activating signal (i.e., signal 1). However, signal 1 alone is insufficient for T-lymphocyte activation, and additional costimulatory interactions between the lymphocyte and antigen presentation cells (APC) are required. More specifically, the CD28 molecule present on the cell surface of naïve T cells can interact with B7-1 (CD80) and/or B7-2 (CD86) located on the APCs (Fig. 13.1a). These interactions serve as additional activation signals (i.e., signal 2) that subsequently induce naïve T-cell activation and differentiation against the presenting antigen.

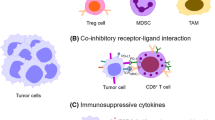
Immune checkpoints fundamental for immunotherapeutic targeting using checkpoint inhibitors. (a) CTLA-4/B7s axis is characterized by the interaction of CTLA-4 with B7-1 and/or B7-2. Activation of T cells arises with signal 1 (TCR + MHC) in combination with costimulatory signal 2 (CD28 + B7-1/B7-2) present on antigen-presenting cells. However, CTLA-4 serves to outcompete CD28 for interactions with B7s thereby inducing T-cell tolerance and inactivity. (b) PD-1/PD-L1 checkpoint is primarily associated with peripheral tolerance (e.g., tumor tissues). PD-1 on activated T cells interacts with PD-L1 expressed by a variety of cells including tumor cells and immunosuppressive cells. This association results in inhibition of T-cell activity, proliferation, and function thereby inducing T-cell exhaustion or anergy. In addition, peripheral Treg cells are induced which further suppress peripheral T-cell responses. (Figure prepared using Biorender.com)
Shortly after T cell activation via TCR binding to MHC, CTLA-4 expression is induced. CTLA-4 serves as an inhibitory signal receptor that can bind selectively to the B7-1 and B7-2 ligands (Fig. 13.1a). Through interactions with these ligands, CTLA-4 utilizes a combination of cell-intrinsic and cell-extrinsic mechanisms for immune regulation. CTLA-4 expression on cells can directly outcompete the costimulatory receptor CD28, thereby blocking activation signals to subsequently dampen T lymphocytes. Furthermore, CTLA-4 ligation to B7-1 and B7-2 also modulates intracellular signaling pathways which prevent appropriate activation via TCR signal transduction [1].
CTLA-4 also possesses cell-extrinsic immune modulatory mechanisms. A particular feature of CTLA-4 is the capability of inducing trans-endocytosis of the B7–1 and B7–2 ligands. In brief, CTLA-4 can essentially remove the B7 ligands from APCs thereby effectively reducing the presence and levels of the B7 ligands required for T-cell activation [2]. An important subset of cellular immune mediators is the regulatory T (Treg) cells that may utilize B7 trans-endocytosis as an aspect of their immunosuppressive activities [1, 3]. Indeed, CTLA-4 function and expression have been shown to contribute toward Treg cell-mediated suppression of host immune responses and the induction of immune tolerance.
However, it is important to highlight the essential physiological role of CTLA-4 in immunological balance. Indeed, the appropriate function of CTLA-4 is best demonstrated by murine models lacking functional copies of this gene (CTLA-4−/−). These CTLA-4 double knockout mice would succumb to extensive lymphoproliferation that invades multiple organ systems shortly after birth [4]. Similarly, autoimmune diseases in humans such as type I diabetes mellitus have been associated with dysfunctional or mutated CTLA-4 [1, 5].
PD-1/PD-L1 Immune Checkpoint
The second prototypical immune checkpoint is the interaction of PD-1 with endogenous ligands, mainly PD-L1 and to a lesser extent PD-L2. The PD-1/PD-L1 axis serves as a potent negative feedback loop in which pro-inflammatory cytokines can induce the expression of PD-L1 in both immune cells and nonimmune tissues/cells. Although PD-1 is constitutively expressed in naïve T lymphocytes, both PD-1 and PD-L1 expression can be upregulated upon their activation [6]. The ligation of PD-1 with PD-L1 inhibits T-lymphocyte activation and function through disruption of TCR signaling pathways, metabolic activity, cytokine production, as well as cellular proliferation and survival (Fig. 13.1b) [6, 7].
With the variety of different tissue expression patterns in both immune and nonimmune cells, the PD-1/PD-L1 immune checkpoint is primarily focused upon the peripheral tissues and tolerance. Indeed, PD-1/PD-L1 interaction can also induce the differentiation of naïve T cells into a particular subset of Treg cells that are induced peripherally (Fig. 13.1b) [6]. Another feature contributing to peripheral tolerance is the presence of exhausted or anergic T cells. Extensive expression of PD-1 is characteristic of this unique subset of cells with reduced immune activity and function [6, 7]. Similar to CTLA-4, it is important to note the significance of PD-1 toward appropriate immunological balance as demonstrated by murine models that develop autoimmune conditions when PD-1 is dysfunction or deficient [7].
Brief History of Immune Checkpoint Inhibitors
Unfortunately, a variety of infectious agents and neoplastic diseases have developed mechanisms that exploit these immune checkpoints to evade the immune system, thereby advancing their replication, proliferation, and growth. Chronic infections from viral pathogens including HIV and hepatitis B virus often induce immune tolerance and anergy to facilitate their persistence. Long-term exposure to viral antigens such as HBV surface protein is associated with the sustained expression of PD-1 and creation of exhausted or anergic T cells [6]. Similarly, a variety of malignant cancers frequently recruit and foster immune cells in their tumor microenvironment that expresses high levels of PD-1 or PD-L1 [6]. Often, the tumor cells themselves overexpress or amplify PD-L1 to attenuate antitumor T-cell responses in order to evade immune-mediated destruction [6, 7].
To counteract the ineffective antitumor effects observed within malignant diseases, immune checkpoint inhibitors (ICI) were developed and have made significant progress within the field of cancer therapeutics. Indeed, this progress resulted in the 2018 Nobel Prize in Medicine which recognized the immense clinical potential and impact of these anticancer immunotherapies. The conceptualization of using inhibitors specifically targeting of CTLA-4 and PD-1 originated in the 1990s.
Shortly after the discovery of CTLA-4 as an inhibitor of T-cell activation, Allsion and his colleagues hypothesized that CTLA-4 might be hindering effective endogenous antitumor immunity [8]. Indeed, the seminal publications from their group demonstrated the powerful antitumor effects and potential of antibodies targeting CTLA-4 [8]. Successful studies in preclinical models of anti-CTLA-4 in a variety of cancers eventually led to human clinical trials, the first of which began in 2003 with ipilimumab (Bristol-Myers Squibb’s Yervoy®). In 2011, ipilimumab was the first ICI approved by the FDA for use in unresectable or metastatic melanoma (Table 13.1) [9]. Subsequent clinical trials with ipilimumab have been completed which now has expanded uses beyond advanced melanoma, as well as combination therapies with anti-PD-1 therapy (i.e., nivolumab) [9]. Building off the success in melanoma, ipilimumab (and other anti-CTLA-4 agents) are being explored in other malignancies either as monotherapy or in a combination therapy with other immunotherapies or chemotherapies (www.clinicaltrials.gov). Aside from ipilimumab, the other notable anti-CTLA-4 agent thus far with some clinical success is tremelimumab (by AstraZeneca) which is undergoing continual research in a variety of trials as a monotherapy or combination therapy. A more comprehensive description of clinical indications of anti-CTLA-4 agents will be discussed in Sect. 3.1 and 3.2.
Discovery of PD-1 itself and its immune modulatory function was spearheaded by the work of Honjo and his colleagues in the 1990s. Subsequent identification of PD-L1 and PD-L2 as ligands of PD-1 was achieved in 2000 and 2001, respectively. These important findings led to the creation of anti-PD-1 and anti-PD-L1 antibodies which were tested in murine models of cancer. The remarkable preclinical results quickly led to human clinical trials which began in 2006 with nivolumab (marketed as Opdivo® by Bristol-Myers Squibb), an anti-PD-1-based immunotherapy. Nivolumab was eventually approved in 2014 by the FDA for use as therapy for advanced melanoma (Table 13.1, Sect. 3.4) [9]. Due to a combination of improved therapeutic efficiency, range of activity, and reduced drug-related adverse effects, anti-PD-1 and anti-PD-L1 therapeutic candidates have surpassed that of anti-CTLA-4 [9]. Indeed, nivolumab was approved shortly after pembrolizumab (Keytruda® by Merck) which received recognition as the first ICI targeting PD-1 for clinical use (see Sect. 3.3). Since 2018, a third anti-PD-1 monoclonal antibody cemiplimab (Libtayo® by Regeneron) is now clinically available (Table 13.1, Sect. 3.5). Furthermore, atezolizumab (Roche’s Tecentriq®), avelumab (Bavenio® by EMD Serono/Pfizer), and durvalumab (Imfinzi® by AstraZeneca) were FDA approved as human therapeutics in 2016, 2017, and 2017, respectively. These three anti-PD-L1-based immunotherapies are recognized for their utility against a growing list of malignant diseases (Table 13.1, Sect. 3.6–3.8).
Considering the different immune pathways targeted by anti-CTLA-4 and anti-PD-1 agents, combination therapy of the two was explored beginning with ipilimumab and nivolumab. The simultaneous targeting of these separate pathways has been successful in terms of enhancing the antitumor efficacy observed with monotherapy use [3, 9]. Indeed, ipilimumab and nivolumab are now clinically indicated for use in a variety of non-melanoma malignancies (Table 13.1, Sect. 3). The success of ipilimumab and nivolumab opened the doorway for additional research into combinatory therapies with other immunotherapy agents. For example, pembrolizumab and ipilimumab are currently within a phase III clinical trial as first-line therapy for non-small cell lung cancer (NCT03302234). These developments in combination therapies allow for further expansion of the clinical uses of ICIs to improve cancer immunotherapies.
Although the clinical advancements of ICIs thus far have primarily been focused upon malignant neoplastic diseases, it is important to highlight that ICIs are also being explored for use in chronic viral infections (see Sect. 5). With the immunosuppressive similarities between persistent viral infections and cancer, a number of studies in chronic diseases such as HIV or HBV have been initiated (www.clinicaltrials.gov; example search terms: HIV or HBV with PD-1, CTLA-4, PD-L1, ipilimumab, nivolumab, etc.).
The field of ICIs is exceptionally promising with an explosion of therapeutic options with an increasing range of activity against malignant diseases. Since the discoveries of CTLA-4 and PD-1/PD-L1 immune checkpoints, additional inhibitory regulators of T-cell function and markers of exhausted T-cells have been identified. Some of the more prominent contenders include but are not limited to LAG-3, TIGIT, and B7-H3 [10]. Moving forward, additional research into these molecules and checkpoints will likely produce an increasing variety of different therapeutic possibilities for the next generation of immunotherapies and the prospect of combination therapies. Indeed, a variety of clinical trials including phase II and III trials are currently underway for antibodies targeting LAG3, TIGIT, and B7-H3 as either monotherapies or combination therapies [10]. Appropriately understanding the clinical outcomes and risks of ICI use will be of utmost importance as this field of immune-modulating therapies rapidly expands.
Mechanism of Action of Immune Checkpoint Inhibitors
All ICIs currently approved for clinical use are biologic agents, namely, monoclonal antibodies, that specifically interfere with CTLA-4, PD-1, or PD-L1 signaling. Overall, the blockade of these checkpoints aims to reinvigorate the immune system by removing the brakes to the antitumor responses. Recognizing the mechanism of action of these monoclonal antibody therapies is essential to understand the potential adverse effects as well as inform the development of improved ICIs.
Ipilimumab, the anti-CTLA-4 biologic, functions through a combination of two main mechanisms. The binding of the monoclonal antibody to CTLA-4 introduces a direct block that prevents interactions of this receptor to the endogenous ligands B7-1 and B7-2 [1, 3]. As a result, CTLA-4 can no longer serve as a competitive inhibitor for the costimulatory CD28 nor induce intracellular signaling changes that prevent T-cell activation. Through this interaction, ipilimumab functions to allow activation and priming of T cells toward tumor antigens (Fig. 13.2a). In addition, a secondary effect of anti-CTLA-4 is Treg cell depletion. The specific binding of ipilimumab can induce antibody-dependent cellular cytotoxicity (ADCC) of Tregs, which generally express CTLA-4, thereby reducing their immunosuppressive effects on antitumor immunity (Fig. 13.2a) [3]. This secondary mechanism of action is important to note as the lack of ADCC activity might be responsible for the reduced efficacy of tremelimumab, an additional anti-CTLA-4 agent that has yet to receive approval for clinical use [1, 3].

Mechanism of action of immune checkpoint inhibitors targeting the CTLA-4/B7s and PD-1/PD-L1 axes. (a) Monoclonal antibodies targeting CTLA-4 (e.g., ipilimumab) serve to sterically hinder interaction with B7s thus eliminating the competition with the costimulatory CD28. In addition, ipilimumab serves to identify CTLA-4+ T cells which are targeted by antibody-dependent cellular cytotoxicity (ADCC) mediated by binding of the anti-CTLA-4 Fc. (b) PD-1/PD-L1 checkpoint is inhibited with the use of either anti-PD-1 (e.g., pembrolizumab) or anti-PD-L1 (e.g., atezolizumab). Attenuating PD-1/PD-L1 interactions allows for restoration of T-cell function and activity. Anti-PD-L1 agents are also associated with the induction of ADCC thereby directly removing PD-L1-expressing malignant cells. (Figure prepared using Biorender.com)
The basis of anti-PD-1 immunotherapy is to disrupt the PD-1/PD-L1 immune checkpoint axis. By preventing the interaction of these two cell surface molecules, their inhibitory effects on T cells can be attenuated. An important aspect of anti-PD-1 therapy is the targeting of exhausted T cells which are characterized, at least in part, with sustained elevated expression of PD-1 [3]. By inhibiting the signals transduced through PD-1 and PD-L1, exhausted T cells can regain their function and proliferative capabilities (Fig. 13.2b). Thus, T cells previously exposed to tumor antigens that were subsequently rendered anergic or tolerant can be restored into antitumor effectors. It is noteworthy to mention that the three currently approved anti-PD-1 therapies (nivolumab, pembrolizumab, and cemiplimab) are IgG4 antibodies which lack effective cytotoxic capabilities (i.e., ADCC and complement dependent cytotoxicity) [1]. As the endogenous ligand for PD-1, biologic therapies targeting PD-L1 have similar mechanisms of action. However, an additional feature of anti-PD-L1 biologic agents is the benefit of ADCC which also directly induces cell death in tumor cells that express PD-L1 (Fig. 13.2b).
Indications
Outside of experiment settings, checkpoint inhibitors are currently being used for the treatment of advanced malignancies, often in conjunction with other therapies, or after more conventional therapy fails. All are given intravenously, typically every 2–4 weeks, though sometimes at longer intervals. As more data is collected and studies are performed, their frequency of use and list of indicated conditions will undoubtably increase.
CTLA-4 Inhibitors: Ipilimumab (Yervoy®)
Ipilimumab was the first checkpoint inhibitor approved for clinical use. It was first approved in 2011 for single agent use in unresectable or metastatic melanoma. With the advent of nivolumab and the development of ipilimumab/nivolumab combination therapy, its list of approved uses has increased substantially. Combination therapy is currently FDA-approved for RCC, metastatic NSCLC, and malignant pleural mesothelioma. Under the FDA’s accelerated approval process (all conditions marked by * are included in the accelerated approval process in which approval is contingent on verification and confirmatory trials), this combination is also conditionally approved for several other cancers including HCC and MSI-H or mismatch repair deficient metastatic CRC.
Tremelimumab
Tremelimumab has been tested as mono- or part of combination therapy for several cancers such as NSCLC, SCLC, and UC. Unfortunately, none of these trials have found success and lead to FDA approval. Despite this, research continues, and promising results for a phase II trial in advanced HCC have been reported recently (NCT02519348).
PD-1 Inhibitors: Pembrolizumab (Keytruda®)
When pembrolizumab was approved for use in 2014, it was the first of the PD-1 inhibitor class. Like ipilimumab, it was first indicated for the treatment of unresectable melanoma. In 2017, it would make history when studies showed it could treat microsatellite instability-high (MSI-H) or mismatch repair-deficient malignancies. Microsatellite instability is the measure of the number of genetic mutations in a tumor cell’s microsatellite DNA sequences, used a marker of prognosis. Pembrolizumab’s approval for MSI-H malignancies marked the first time a medication could be used for a cancer based on a biomarker, rather than the origin location in the body. Later in 2020, pembrolizumab would receive its second biomarker-based approval from the FDA. This time, it was for unresectable or metastatic tumors with a high tumor mutational burden (TMB-H), defined as >10 mutations/megabase. While some indications for Pembrolizumab are based on biomarkers, others are based on location of the cancer or the location in addition to a biomarker such as tumor proportion score (TPS), the percentage of tumor cells that express PD-L1. Typically, the medication is indicated if either conventional treatment has failed or biomarker requirements are met. Pembrolizumab is also currently approved for NSCLC, SCLC, HNSCC, HL, PMLBCL, UC, GC*, ESCC, CC* HCC*, MCC*, RCC, ENC*, and cSCC.
Nivolumab (Opdivo®)
Nivolumab was approved shortly after Pembrolizumab. Like the earlier ICIs, it was originally approved for use in advanced melanoma. It would later have its approval expanded to NSCLC and then SCLC. As monotherapy, it can also be used for HNSCC and ESCC. Together with ipilimumab, it is approved for use in malignant pleural mesothelioma, metastatic NSCLC, and RCC. Accelerated approval has been granted by the FDA for use in UC, cHL, MSI-H, or mismatch repair-deficient CRC and HCC.
Cemiplimab (Libtayo®)
Cemiplimab, the latest PD-1 inhibitor, was approved for use in 2018. Being a newer medication, it has fewer indicated uses than other ICIs. Currently, it is only approved for metastatic cSCC or locally advanced cutaneous SCC in patients who are not candidates for surgery or radiation.
PD-L1 Inhibitors: Atezolizumab (Tecentriq®)
Atezolizumab was approved for use in 2016, the first of the PD-L1 inhibitor class. Its initial indication was for use in UC*, and it has since been approved for NSCLC, triple-negative BC*, SCLC, HCC, and melanoma. Atezolizumab is often used as part of a cancer regimen alongside chemotherapy agents carboplatin and etoposide, in addition to newer agents such as bevacizumab, cobimetinib, and vemurafenib.
Avelumab (Bavencio®)
Avelumab’s first indicated use was in metastatic MCC in 2017*. This made it the first ICI not originally approved for use in advanced skin cancer (either melanoma or cSCC). Other approved indications include UC and advanced RCC.
Durvalumab (Imfinzi®)
Like atezolizumab, durvalumab is currently approved for use in UC*. NSCLC and SCLC were later added to its list of indications.
Checkpoint Inhibitors and Infections
Mechanisms Predisposing to Infection
There are several possible mechanisms through which immune checkpoint inhibitors can predispose individuals to infection, each with their own level of evidence to support them.
The first, and most common mechanism, is through immune-related adverse events (irAEs). By “boosting” the immune system, ICIs can cause autoimmune inflammatory reactions. Due to the ubiquitous nature of the immune system, any organ system can be involved, though most commonly are the gastrointestinal tract (colitis, diarrhea, pancreatitis, and hepatitis), lungs (pneumonitis and sarcoidosis), endocrine glands (hypo−/hyperthyroidism, thyroiditis, hypophysitis, diabetes mellitus, Addison’s disease, and adrenal insufficiency), skin (rash and vitiligo) [11]. The exact mechanism behind these adverse events is unclear, but these autoimmune events make sense from a mechanistic perspective. The healthy immune system is constantly trying to find equilibrium between detecting intruders (microbes, cancer) and not reacting to the host. A balance that most of the time is carefully struck. Checkpoint molecules are part of this crucial balancing act, by “deactivating” immune cells when they are no longer needed. However, when a host develops a malignancy, the scales can be tipped toward inactivation. Studies have shown that tumor cells are able to upregulate checkpoint molecules [6], an adaptation that likely helps avoid an immune-mediated demise. When we use ICIs, we are shifting the balance toward immune-system activation, which can lead to the collateral damage of autoimmune events. These events usually occur several weeks-months after starting an ICI; however, they can occur at any point, even after discontinuation [12]. Treatment for irAEs typically involves the use of corticosteroids, and if corticosteroids are ineffective, then another immunosuppressive therapy may be required. In this mechanism, it is the treatment of the side effects (irAEs) rather than the ICI itself that predisposes to infection. Interestingly, the different classes of ICIs do not seem to have identical side effect profiles. CTLA-4 inhibitors tend to cause more GI symptoms or hypophysitis, whereas the PD-1 inhibitors cause more pneumonitis and arthralgias.
The second way that ICIs can predispose to infection is through immune-mediated cytopenia. Like other irAEs, the exact mechanism is unclear. The frequency of these hematopoietic immune events has been found to be around 0.5% [13], and they can present in a wide spectrum of conditions such as immune thrombocytopenia, autoimmune hemolytic anemia, neutropenia, aplastic anemia, and hemophagocytic syndrome. Not only do these events usually warrant immune suppression on their own, but neutropenia can also predispose patients to opportunistic infections. One review found that of 11 cases of ICI-induced neutropenia, 6 were complicated by severe infection [13]. These immune-mediated cytopenia’s were typically reversible and usually treated with some combination of granulocyte-colony stimulating factor, corticosteroids, IVIG, or other immunosuppressants.
Lastly, it has been suggested that ICIs can lead to the development/reactivation of tuberculosis (TB) independent of immune suppression for irAEs. Several cases have been published on patients, not on immunosuppressants, who develop acute pulmonary TB after taking ICIs for metastatic malignancies. There are many confounding factors to consider when looking at TB infection in patients on ICIs. For one, patients are often started on ICIs after first undergoing many cycles of chemotherapy. Second, cancer itself is a risk factor for infection. Diagnosis can also be difficult as TB and lung cancer share many symptoms and pneumonitis is a documented side effect of the PD-1/PD-L1 inhibitors. There are some preclinical trials to support this notion as studies in mice have suggested that PD-1/PD-L1 play a protective role against the reactivation of TB [14]. One theory is that ICIs activate mycobacterium-specific T cells, leading to an immune reconstitution syndrome. Looking beyond case reports, the data suggests that TB reactivation is very rare in patients on ICIs. One retrospective study observed 1144 patients taking ICIs over a 4-year period and found that only three patients developed tuberculosis, and two of them were taking immunosuppressants prior to their diagnosis [15]. Another retrospective study looked at 908 patients on PD-1/PD-L1 inhibitors and found two cases of TB, neither had been on immunosuppressants [16].
Risk of Infection
Assessing the absolute risk of infection with ICIs is difficult for several reasons. Rates of infection are typically secondary outcomes in trials, often lacking detail in the types of infections or how they were diagnosed. The patients on these medications commonly have many comorbidities, are usually seriously ill, and may have completed several cycles of chemotherapy.
Initial studies were done on ipilimumab, as it was the first ICI approved for human use. The phase 2 trials for ipilimumab in melanoma patients did not show an increased risk of infection [17]. A head-to-head trial of ipilimumab plus dacarbazine versus placebo plus dacarbazine also found no increased risk of infections, though there were significantly more adverse events [18].
The largest study, a retrospective study done by Castillo et al. [19], looked at 740 patients receiving ICIs for melanoma and found that 54 (7.3%) developed serious infections (defined as requiring hospital admission or parenteral antibiotics). The risk factors identified for a serious infection were corticosteroid use (OR 7.71), infliximab use (OR 4.74), or the use of ipilimumab and nivolumab together. Pembrolizumab was inversely associated with the risk of serious infections. These different infection rates are likely attributable to the variable risk of irAEs as 69% of patients treated with ipilimumab plus nivolumab received corticosteroids compared to only 6% of the patients who received pembrolizumab alone. Bacterial infections were the most common (pneumonia, bacteremia, C. difficile-associated diarrhea and intra-abdominal infections), but there were also cases of fungal (invasive pulmonary aspergillosis, pneumocystis pneumonia, and candidemia), viral (herpes zoster, CMV colitis, and EBV), and parasitic (single case of Strongyloides) infections.
Komodo et al. [20] did a retrospective analysis on 111 patients taking either nivolumab, pembrolizumab, or ipilimumab and found that 14% developed a serious infection. Patients who were on steroids had a much higher risk of developing a serious infection. Bacterial infections were the most common cause of serious infections (pneumonia, genitourinary infections, SSTIs, and bacteremia), and there were only a few cases of viral infections (enterovirus and rhinovirus).
Another study, done by Fujita et al. [21], reviewed 167 patients with NSCLC who had been treated with nivolumab. They found that 19.2% of the patients developed an infection that required the use of antimicrobials. Of these infections, most were bacterial, but there were some viral and fungal infections as well. This study found that only type 2 diabetes, and not steroid use, was associated with an increased risk of infection. Several limitations to this study were brought up by the authors themselves. The main limitation is that it was difficult to distinguish pneumonia for pneumonitis, and their definition of infection included patients who were empirically given antibiotics. This could explain the higher incidence of infection and why there was no association found with immunosuppressant use.
Current Guidelines
Due to the minor risk of infection associated with ICIs, society guidelines such as the European Society of Medical Oncology [22] and the American Society of Clinical Oncology [23] do not recommend treating patients with infectious prophylactic mediations (either antiviral or anti-pneumocystis). However, prophylaxis is still recommended in patients who are being treated with prolonged immune suppression for ICI-induced irAEs, that same as for any individual on prolonged immunosuppressants. Along with this, some guidelines suggest testing for latent TB, in addition to hepatitis B and C, in case immune suppression is required in the future.
Using Checkpoint Inhibitors to Treat Infections
Not only do cancer cells upregulate checkpoint molecules, but checkpoint molecule expression is also increased on lymphocytes in many infectious disease states. This phenomenon is often referred to as immune exhaustion, and given that ICIs can be used to boost the immune system to help detect and fight cancer, a reasonable proposition would be that they could also treat infections. The mechanism for this makes sense, but most, if not all, of the pivotal trials used to investigate efficacy and safety had active infections as an exclusion criterion. To date, there have been no large-scale RCTs for this, but there have been some promising preclinical and phase 1 trials.
Sepsis
Sepsis is an active area of investigation for checkpoint inhibitors. Checkpoint molecule expression is known to be increased in septic patients [24]. The idea is that ICIs would boost the immune system’s response and enhance clearance of bacterial or even fungal infections. Several animal models have shown that ICIs improve survival when provoked with a bacterial or lipopolysaccharide challenge. A meta-analysis by Busch et al. [25] looked at mouse models of sepsis and found that ICIs significantly increased the OR of survival in 10/19 of the studies (OR = 3.37 [1.55–7.31]). Of note was that ten of the studies were from the same lab group, and all the studies had a high risk of bias. Due to the somewhat promising preclinical data, two phase I trials were conducted in 2019. One with nivolumab [26] and another with BMS-936559 [27], a PD-L1 inhibitor. Both trials showed that the medication was well tolerated, with no evidence of worsening symptoms or cytokine storm. However, being phase I trials, there were no comparison or placebo arms, so definitive conclusions cannot be drawn about their efficacy at this point.
HIV
Research with HIV and ICIs has been done looking into two main categories, the safety and efficacy of ICIs in treating cancers in HIV+ individuals, and whether ICIs can be used to treat HIV itself. In answering the first question, a meta-analysis done in 2019 looked at 73 patients and concluded that there was no association with adverse changes in HIV viral load or CD4 count [28]. It was also found that the checkpoint inhibitors remained effective against their respective malignancies. The answer to the second question is more nuanced and is still an area of active research.
While antiretroviral therapy can effectively suppress HIV and prevent the development of AIDS, it remains an incurable infection. One of the mechanisms through which HIV is able to persist in its host and remain latent is through T-cell exhaustion and checkpoint inhibitor upregulation [29]. In addition to downregulating T-cell proliferation, in vitro studies have shown that PD-1 activation in CD4+ T cells inhibits HIV viral replication. Studies have also shown that overexpression of checkpoint molecules partially regresses with antiretroviral treatment. It is thought that the use of ICIs would not only activate HIV-specific CD8 T cells, but it would also increase the production of the HIV virus from reservoir cells, shifting the disease state away from latency. A meta-analysis by Baptiste et al. [29] evaluated 176 HIV+ individuals taking ICIs and found that in 92%, the viral load remained stable, and it increased in 6% and decreased in 2%. It was found that CD4 counts remained stable in 61%, and they increased in 24% and decreased in 15%. In 2017, a phase I study was conducted on HIV patients, comparing BMS-936559 (a PD-L1 inhibitor) and placebo [30]. They found that there was an increase in HIV-1-specific CD8 T cells in two out of six of the patients, though the results were not significant when the whole treatment arm was analyzed. Overall ICIs have shown some benefit in decreasing the HIV reservoir, though it is unlikely that their use alone will be substantial enough.
JC Virus
Currently the only treatment available for progressive multifocal leukoencephalopathy (PML) is immune reconstitution. This can come with its own risks, depending on the initial reason for immune suppression, and is not always an option for everyone. In 2019, a case report was published about a patient with Hodgkin lymphoma, on nivolumab, who developed PML and then went into remission [31]. This was followed shortly by a small trial in which eight patients with PML were given three doses of pembrolizumab as an experimental treatment [32]. Five of the eight patients had clinical improvement or stabilization of their symptoms. Of these five patients, four of them had a persistently decreased JC viral load in the CSF, with the other being a temporary decrease. A possible confounder was that the studies could not rule out the possibility of pembrolizumab assisting in the treatment of the underlying malignancies. Unfortunately, this study was followed by several case reports of PML developing in patients being treated with nivolumab [33], and more research will be required in this area.
Hepatitis B
Due to hepatitis B virus’s (HBV) causative relationship with hepatocellular carcinoma (HCC), the use of ICIs has been studied in patients with chronic HBV. Metanalysis has shown that ICIs, while they can cause reversible hepatic injury, are safe for use in patients with either chronic HBV or HCV [34]. Like in other chronic infections discussed earlier, HBV is associated with increased checkpoint molecule expression on T lymphocytes. Ex vivo studies have shown that checkpoint inhibition increases HBV-specific T-cell proliferation and the production of protective antibodies [35]. Given this relation, it is thought that HBV clearance could be enhanced with the use of ICIs. A phase I study done in 2019 gave patients with chronic HBV low-dose nivolumab and found that it caused a decreased in HBsAg titers in 91% of the subjects, with one patient seroconverting [36].
Invasive Fungal Infections
Mucormycosis is a serious life-threatening fungal infection caused by fungi in the order Mucorales. These infections are typically seen in the immunosuppressed or the critically ill where they can be challenging to treat. In 2017, the first report of mucormycosis being treated with an ICI was published [37]. The case involved a young woman who survived a terrorist bombing, only to develop invasive intra-abdominal mucormycosis that was nonresponsive to standard treatment. Investigations showed lymphopenia, low monocyte HLA-DR (a T-cell ligand) expression, and increased PD-1 expression on T cells. For this, her treating team gave her interferon-γ and a single dose of nivolumab. The patient made a full recovery, and subsequent investigation showed a reversal of the aforementioned abnormalities. Since then, another case has been described in a woman with AML who developed an invasive infection with aspergillus and lichtheimia [38]. She was treated similarly with interferon-γ and nivolumab. There were signs of recovery, but eventually the patient declined medical treatment due to AML progression. These cases show that under the right circumstances, invasive fungal diseases can be treated with ICIs, though large-scale investigation is still required.
COVID-19
With the COVID-19 pandemic changing almost every aspect of people’s lives, it is no wonder that that researchers are investigating the use of ICIs in this viral illness. One large difference between the SARS-CoV-2 virus and other viral infections discussed in this chapter is that rather than remaining latent in its host, COVID-19 causes mortality through a cytokine storm. This is caused by an exaggerated response of the immune system, leading to systemic inflammation which can cause acute respiratory distress syndrome (ARDS) among other complications. Like the other infections in the chapter, COVID has been associated with T-cell exhaustion [39]. Lymphopenia, another complication associated with COVID, is thought due to T-cell exhaustion and abnormal cytokine production. Like all aspects of COVID-19, this is an area of active research. Retrospective analyses on COVID patients who were previously taking ICIs are mixed, and some have shown no difference in severity [40, 41] while others found the opposite [42]. As of writing, there are several registered trials that are assessing the effectiveness of treating COVID-19 with ICIs such as nivolumab (NCT04343144) and pembrolizumab (NCT04335305), though none have been published. Some researchers have suggested that the best benefit from ICIs in COVID-19 might be when paired with an immunosuppressant like tocilizumab (IL-6 inhibitor). This would allow the ICI to prevent T-cell exhaustion, and an IL-6 inhibitor could manage the cytokine storm. A phase II trial has recently been registered to test this hypothesis (NCT04335305). With the incredible resources and speed of COVID research, it is inevitable that we will soon have more answers.
Mouse Models of Infection
In addition to the potential applications of ICIs in human infections, there are several promising uses that have been demonstrated in mice. In a mouse model of infection with Histoplasma capsulatum, Lázár-Molnár et al. found that PD-1-deficient mice all survived while wild-type mice died from disseminated infection [43]. Their study also found that most of the wild-type mice survived when given a PD-1 inhibitor. Similarly, for mice with persistent Cryptococcus neoformans infections, using a PD-1 inhibitor significantly improved fungal clearance [44]. In mice infected with Echinococcus multilocularis (the causative organism of alveolar echinococcosis, which causes cyst formation in the liver, among other organs), PD-1 blockade was associated with a decreased parasite load and fewer liver lesions [45]. These models all showed impressive response to treatment and, given that the side effect profile of ICIs is well known, look for human case reports in the future.
Summary
Checkpoint molecules are cell ligands or receptors that are expressed on lymphocytes, the main cellular component of the adaptive immune system. Activation of checkpoint molecules (PD-1/PD-L1 and CTLA-4) shifts the immune system away from activation and toward tolerance or dormancy. Various cancers and infections have adapted to take advantage of this by causing the upregulation of checkpoint molecules, thereby decreasing lymphocyte function. The medication class of checkpoint inhibitors (ICIs) consists of monoclonal antibodies against checkpoint molecules or their receptors. The use of these antibodies has been shown to prolong survival in many cancers, with much more tolerable side effects compared to traditional chemotherapies. The main complications of ICIs are immune-related adverse events (irAEs). These autoimmune side effects are caused by the shift of the immune system away from self-tolerance, and they can affect almost any organ system. While ICIs by themselves rarely increase infection risk, the treatment of these irAEs (typically with immunosuppressants) is a significant risk factor for various types of infection. In addition to their ever-increasing role in cancer treatment, ICIs have recently shown promise in treating various types of infection, including but not limited to sepsis, HIV, JC virus, and mucormycosis. With the list of potential uses in oncology and infectious diseases growing exponentially, it is important for researchers and clinicians to know and understand this interesting class of medications.
References
Lee HT, Lee SH, Heo YS. Molecular interactions of antibody drugs targeting PD-1, PD-L1, and CTLA-4 in immuno-oncology. Molecules. 2019;24(6):1190. https://doi.org/10.3390/molecules24061190.
Qureshi OS, Zheng Y, Nakamura K, et al. Trans-endocytosis of CD80 and CD86: a molecular basis for the cell-extrinsic function of CTLA-4. Science. 2011;332(6029):600–3. https://doi.org/10.1126/science.1202947.
Wei SC, Duffy CR, Allison JP. Fundamental mechanisms of immune checkpoint blockade therapy. Cancer Discov. 2018;8(9):1069–86. https://doi.org/10.1158/2159-8290.CD-18-0367.
Waterhouse P, Penninger JM, Timms E, et al. Lymphoproliferative disorders with early lethality in mice deficient in Ctla-4. Science. 1995;270(5238):985–8. https://doi.org/10.1126/science.270.5238.985.
Chen Z, Fei M, Fu D, et al. Association between cytotoxic T lymphocyte antigen-4 polymorphism and type 1 diabetes: a meta-analysis. Gene. 2013;516(2):263–70. https://doi.org/10.1016/j.gene.2012.12.030.
Bardhan K, Anagnostou T, Boussiotis VA. The PD1: PD-L1/2 pathway from discovery to clinical implementation. Front Immunol. 2016;7:550. https://doi.org/10.3389/fimmu.2016.00550.
Sun C, Mezzadra R, Schumacher TN. Regulation and function of the PD-L1 checkpoint. Immunity. 2018;48(3):434–52. https://doi.org/10.1016/j.immuni.2018.03.014.
Leach DR, Krummel MF, Allison JP. Enhancement of antitumor immunity by CTLA-4 blockade. Science. 1996;271(5256):1734–6. https://doi.org/10.1126/science.271.5256.1734.
Hargadon KM, Johnson CE, Williams CJ. Immune checkpoint blockade therapy for cancer: an overview of FDA-approved immune checkpoint inhibitors. Int Immunopharmacol. 2018;62:29–39. https://doi.org/10.1016/j.intimp.2018.06.001.
Pant A, Medikonda R, Lim M. Alternative checkpoints as targets for immunotherapy. Curr Oncol Rep. 2020;22(12) https://doi.org/10.1007/s11912-020-00983-y.
Man J, Ritchie G, Links M, Lord S, Lee CK. Treatment-related toxicities of immune checkpoint inhibitors in advanced cancers: a meta-analysis. Asia Pac J Clin Oncol. 2018;14(3):141–52. https://doi.org/10.1111/ajco.12838.
Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. 2018;378(2):158–68. https://doi.org/10.1056/nejmra1703481.
Michot JM, Lazarovici J, Tieu A, et al. Haematological immune-related adverse events with immune checkpoint inhibitors, how to manage? Eur J Cancer. 2019;122:72–90. https://doi.org/10.1016/j.ejca.2019.07.014.
Barber DL, Mayer-Barber KD, Feng CG, Sharpe AH, Sher A. CD4 T cells promote rather than control tuberculosis in the absence of PD-1–mediated inhibition. J Immunol. 2011;186(3):1598–607. https://doi.org/10.4049/jimmunol.1003304.
Im Y, Lee J, Kim SJ, Koh WJ, Jhun BW, Lee SH. Development of tuberculosis in cancer patients receiving immune checkpoint inhibitors. Respir Med. 2020;161:105853. https://doi.org/10.1016/j.rmed.2019.105853.
Picchi H, Mateus C, Chouaid C, et al. Infectious complications associated with the use of immune checkpoint inhibitors in oncology: reactivation of tuberculosis after anti PD-1 treatment. Clin Microbiol Infect. 2018;24(3):216–8. https://doi.org/10.1016/j.cmi.2017.12.003.
Redelman-Sidi G, Michielin O, Cervera C, et al. ESCMID study Group for Infections in compromised hosts (ESGICH) consensus document on the safety of targeted and biological therapies: an infectious diseases perspective (immune checkpoint inhibitors, cell adhesion inhibitors, sphingosine-1-phosphate receptor modulators and proteasome inhibitors). Clin Microbiol Infect. 2018;24:S95–S107. https://doi.org/10.1016/j.cmi.2018.01.030.
Robert C, Thomas L, Bondarenko I, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364(26):2517–26. https://doi.org/10.1056/nejmoa1104621.
Del Castillo M, Romero FA, Argüello E, Kyi C, Postow MA, Redelman-Sidi G. The spectrum of serious infections among patients receiving immune checkpoint blockade for the treatment of melanoma. Clin Infect Dis. 2016;63(11):1490–3. https://doi.org/10.1093/cid/ciw539.
Komoda K, Ross JA, Margolin K, et al. 1556 Infectious disease complications with use of checkpoint inhibitors in solid organ malignancies. Open forum. Infect Dis. 2018;5(suppl_1):S484. https://doi.org/10.1093/ofid/ofy210.1384.
Fujita K, Kim YH, Kanai O, Yoshida H, Mio T, Hirai T. Emerging concerns of infectious diseases in lung cancer patients receiving immune checkpoint inhibitor therapy. Respir Med. 2019;146:66–70. https://doi.org/10.1016/j.rmed.2018.11.021.
Haanen JBAG, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28:iv119–42. https://doi.org/10.1093/annonc/mdx225.
Brahmer JR, Lacchetti C, Schneider BJ, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American society of clinical oncology clinical practice guideline. J Clin Oncol. 2018;36(17):1714–68. https://doi.org/10.1200/JCO.2017.77.6385.
Patil NK, Guo Y, Luan L, Sherwood ER. Targeting immune cell checkpoints during sepsis. Int J Mol Sci. 2017;18(11):2413. https://doi.org/10.3390/ijms18112413.
Busch LM, Sun J, Cui X, Eichacker PQ, Torabi-Parizi P. Checkpoint inhibitor therapy in preclinical sepsis models: a systematic review and meta-analysis. Intensive Care Med Exp. 2020;8(1):1–19. https://doi.org/10.1186/s40635-019-0290-x.
Hotchkiss RS, Colston E, Yende S, et al. Immune checkpoint inhibition in sepsis: a phase 1b randomized study to evaluate the safety, tolerability, pharmacokinetics, and pharmacodynamics of nivolumab. Intensive Care Med. 2019;45(10):1360–71. https://doi.org/10.1007/s00134-019-05704-z.
Hotchkiss RS, Colston E, Yende S, et al. Immune checkpoint inhibition in sepsis: a phase 1b randomized, placebo-controlled, single ascending dose study of Antiprogrammed cell death-ligand 1 antibody (BMS-936559). Crit Care Med. 2019;47(5):632–42. https://doi.org/10.1097/CCM.0000000000003685.
Kim C, Cook MR. Safety and efficacy of immune checkpoint inhibitor therapy in patients with HIV infection and advanced-stage cancer: a systematic review. JAMA Oncol. 2019;5(7):1049–53. https://doi.org/10.1001/jamaoncol.2018.6737.
Abbar B, Baron M, Katlama C, et al. Immune checkpoint inhibitors in people living with HIV: what about anti-HIV effects? AIDS. 2020;34(2):167–75. https://doi.org/10.1097/QAD.0000000000002397.
Gay CL, Bosch RJ, Ritz J, et al. Clinical trial of the anti-PD-L1 antibody BMS-936559 in HIV-1 infected participants on suppressive antiretroviral therapy. J Infect Dis. 2017;215(11):1725–33. https://doi.org/10.1093/infdis/jix191.
Hoang E, Bartlett NL, Goyal MS, Schmidt RE, Clifford DB. Progressive multifocal leukoencephalopathy treated with nivolumab. J Neurovirol. 2019;25(2):284–7. https://doi.org/10.1007/s13365-019-00738-x.
Cortese I, Muranski P, Enose-Akahata Y, et al. Pembrolizumab treatment for progressive multifocal leukoencephalopathy. N Engl J Med. 2019;380(17):1597–605. https://doi.org/10.1056/nejmoa1815039.
Martinot M, Ahle G, Petrosyan I, et al. Progressive multifocal leukoencephalopathy after treatment with nivolumab. Emerg Infect Dis. 2018;24(8):1594–6. https://doi.org/10.3201/eid2408.180460.
Pu D, Yin L, Zhou Y, et al. Safety and efficacy of immune checkpoint inhibitors in patients with HBV/HCV infection and advanced-stage cancer: a systematic review. Medicine (Baltimore). 2020;99(5):e19013. https://doi.org/10.1097/MD.0000000000019013.
Salimzadeh L, Le Bert N, Dutertre CA, et al. PD-1 blockade partially recovers dysfunctional virus-specific B cells in chronic hepatitis B infection. J Clin Invest. 2018;128(10):4573–87. https://doi.org/10.1172/JCI121957.
Gane E, Verdon DJ, Brooks AE, et al. Anti-PD-1 blockade with nivolumab with and without therapeutic vaccination for virally suppressed chronic hepatitis B: a pilot study. J Hepatol. 2019;71(5):900–7. https://doi.org/10.1016/j.jhep.2019.06.028.
Grimaldi D, Pradier O, Hotchkiss RS, Vincent JL. Nivolumab plus interferon-γ in the treatment of intractable mucormycosis. Lancet Infect Dis. 2017;17(1):18. https://doi.org/10.1016/S1473-3099(16)30541-2.
Mueller N, Banck J, Mellinghoff S, et al. P09.09 PD-1 checkpoint blockade for treatment of mucormycosis and invasive aspergillosis in a stem cell transplant recipient. J Immunother Cancer. 2020;8(Suppl 2):A56–7. https://doi.org/10.1136/jitc-2020-itoc7.109.
Diao B, Wang C, Tan Y, et al. Reduction and functional exhaustion of T cells in patients with coronavirus disease 2019 (COVID-19). Front Immunol. 2020;11:827. https://doi.org/10.3389/fimmu.2020.00827.
Luo J, Rizvi H, Egger JV, Preeshagul IR, Wolchok JD, Hellmann MD. Impact of PD-1 blockade on severity of COVID-19 in patients with lung cancers. Cancer Discov. 2020;10(8):1121–8. https://doi.org/10.1158/2159-8290.CD-20-0596.
Rogiers A, Tondini C, Grimes JM, et al. Abstract S02-01: clinical characteristics and outcomes of coronavirus 2019 disease (COVID-19) in cancer patients treated with immune checkpoint inhibitors (ICI). Clin Cancer Res. 2020;26(18 Supplement):S02-01. https://doi.org/10.1158/1557-3265.COVID-19-S02-01.
Robilotti EV, Babady NE, Mead PA, et al. Determinants of COVID-19 disease severity in patients with cancer. Nat Med. 2020;26(8):1218–23. https://doi.org/10.1038/s41591-020-0979-0.
Lázár-Molnár E, Gácser A, Freeman GJ, Almo SC, Nathenson SG, Nosanchuk JD. The PD-1/PD-L costimulatory pathway critically affects host resistance to the pathogenic fungus histoplasma capsulatum. Proc Natl Acad Sci U S A. 2008;105(7):2658–63. https://doi.org/10.1073/pnas.0711918105.
Roussey JA, Viglianti SP, Teitz-Tennenbaum S, Olszewski MA, Osterholzer JJ. Anti–PD-1 antibody treatment promotes clearance of persistent cryptococcal lung infection in mice. J Immunol. 2017;199(10):3535–46. https://doi.org/10.4049/jimmunol.1700840.
Wang J, Jebbawi F, Bellanger A-P, Beldi G, Millon L, Gottstein B. Immunotherapy of alveolar echinococcosis via PD-1/PD-L1 immune checkpoint blockade in mice. Parasite Immunol. 2018;40(12):e12596. https://doi.org/10.1111/pim.12596.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Lau, K.C.K., Weyant, B., Cervera, C. (2022). Immune Checkpoint Inhibitors. In: Cervera, C., Aguado, J.M. (eds) Infectious Complications in Biologic and Targeted Therapies. Springer, Cham. https://doi.org/10.1007/978-3-031-11363-5_13
Download citation
DOI: https://doi.org/10.1007/978-3-031-11363-5_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-11362-8
Online ISBN: 978-3-031-11363-5
eBook Packages: MedicineMedicine (R0)