
Abstract
There are a variety of conditions that lead to the requirement of total hip arthroplasty (THA), which is performed to ultimately achieve the reduction of the perceived pain and the subsequent improvement of the range of motion of the affected individuals. The following article analyzes some of the aforementioned conditions, giving a thorough examination of each disease from a biological perspective, and providing data regarding the outcomes of the surgical procedures on the patients. The analyzed conditions we cover throughout this work include sickle cell disease, hereditary multiple exostosis (HME), lumbar spinal disorders, developmental hip dysplasia (DDH), renal transplant and hemodialysis, osteoarthritis (OA), and human immunodeficiency virus (HIV).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

1 Introduction
Total hip arthroplasty constitutes a suitable solution for the treatment of conditions that include but are not limited to osteoarthritis of the hip joint. In fact, there are a wide variety of conditions that would significantly benefit from the performance of the orthopedic procedure, particularly in terms of pain relief, and increased functionality. In this article, we review the literature to cover some of the aforementioned conditions, providing a thorough examination of the causes leading to the development of each disease, and some of the reasons for the performance of THA to be beneficial for the affected individuals. Such conditions include sickle cell disease, hereditary multiple exostosis, lumbar spinal disorder, developmental hip dysplasia, end-stage renal failure leading to renal transplant and hemodialysis, and human immunodeficiency virus.
2 Sickle Cell Disease
Sickle cell disease is a recessive disorder derived from the inheritance of hemoglobin S and caused by a point mutation on the 17th nucleotide (in which adenine replaced the thymine present in healthy individuals) on the β-globulin gene located on exon I of both homologs of chromosome 11. It results in the production of red blood cells presenting a sickle shape that eventually causes the blockage of blood vessels, ultimately leading to conditions such as ischemia or breach of the compromised tissue which substantially decrease life expectancy [2].
Avascular necrosis is one of the most common impairments caused by the disease, mainly due to the effects that the blockage of the normal blood flow has on the bone connective tissue.
The head of the femur is the most common site affected by avascular necrosis in patients diagnosed with sickle cell disease, thus impacting operational capacity and leading to osteoarthritis of the hip joint, already presenting previous abnormalities in the morphology of the metaphysis of the femur (characterized by unusually thin trabeculae and cortices) alongside low bone mineral density, which could potentially lead to discrepancies between the joint surfaces of the hip and subsequent collapse of the femoral canal [3]. Therefore, total hip replacement constitutes the most effective and safe procedure to ultimately restore the functional ability of the affected patients, as well as decrease the unbearable pain experienced by the latter [4, 5]. Figure 1 shows the magnification of the red blood cells in patients affected by sickle cell disease. The “sickle”-shaped cells are indicated by the arrows [62].

Red blood cells of individuals with sickle cell disease
2.1 Total Hip Replacement Surgery in Patients with Avascular Necrosis Suffering from Sickle Cell Disease
The objective of the study undertaken in [1] was to analyze the operational outcomes in patients affected by sickle cell disease presenting avascular necrosis, either with or without congruency of the hip.
Throughout the study, the participants were divided into two groups. Group A consisted of 19 patients with optimal congruency of the hip but presenting an infarct area of over 30%, whereas group B comprised 17 patients presenting joint incongruency with arthritic changes. The entirety of the participants was subjected to THR through a lateral approach, performed after reaching a concentration of hemoglobin of a minimum of 10 g/dl and a hemoglobin S concentration below 30% (in order to avoid the incidence of sickle cell crisis postoperatively). The procedure was performed via an incision realized approximately 5 cm proximal to the extremity of the greater trochanter and extending for 8 cm down the femoral bone, which split the tensor fascia lata to expose the tendon of the gluteus medius [1].
After a comparison of the Harris Hip Score results, it was possible to determine that both groups showed substantial progress in their functionality, particularly group B, which presented a superior improvement throughout the first year following the surgery, potentially attributed to the more severe pain experienced before the THR procedure. The rate of survival 5 years postoperatively corresponded to 94.29%, and the observed deaths were caused by factors unrelated to THR. The incidence of superficial infections amounted to 14.2%, successfully treated with administration of antibiotics, whereas it was significantly lower for deep infections, 2.8%. Moreover, only 2.8% of the analyzed cases experienced aseptic loosening of the stem of the femur, whereas no dislocations were observed [1].
3 Hereditary Multiple Exostosis
Hereditary multiple exostosis (HME), also called denominated hereditary multiple osteochondromas, is a rare congenital disease caused by loss-of-function mutations occurring at the EXT1 and EXT2 genes, which are linked to the synthesis of heparan sulfate and result, according to several studies, in alterations at the molecular and cellular levels [6]. The disease induces the thickening and subsequent distortion of the bone during development, ultimately causing the formation of osteomata – benign formation of new bone connective tissue – around areas characterized by active osteogenesis. The bones implicated in this detrimental process are usually less developed in terms of length, thus causing deformities in the skeletal structure of the majority of the affected individuals, such as structural asymmetry in the os coxae and pectoral girdle, abnormal growth of the ulnar and radial bones leading to the subluxation of the glenohumeral articulation, and distortion of the knee caused by similar abnormalities regarding the tibia and the fibula [8]. In particular, about 25% of HME patients present an anomalous increase in the surface area of the metaphysis and valgus hip caused by deformities occurring at the neck of the femur or in the area between the trochanters, ultimately resulting in a decreased space between the lesser trochanter and the ischial tuberosity, which increases the incidence of femoroacetabular impingement and early arthritis of the joint up to 62% [9, 10]. The population affected by this disease usually presents various clinical manifestations, among which chronic pain syndrome, limited range of motion, deformities – especially regarding the limbs – and alterations of the neurovascular system [6].
No medical treatment has been currently identified for HME [6]; therefore, THA has been indicated as the most favorable alternative for patients affected by this condition and by acute osteoarthritis, to ultimately restore the range of motion and provide relief from pain. Figure 2 depicts the radiograph of a patient affected by hereditary multiple exostosis, in which acetabular dysplasia is visible in both hips [63].

Radiograph of an individual with HME
3.1 Total Hip Arthroplasty in Patients Affected by Hereditary Multiple Exostosis
The retrospective review performed in [7] included seven patients affected by HME, three of which suffered from bilateral arthritis of the os coxa and femur, therefore requiring bilateral THA. The surgery was performed through the direct lateral approach in eight instances, whereas only two were performed using the posterior approach; moreover, the patients suffering from bilateral exostosis of the hip underwent two surgeries, with the second one performed 12 months after the first procedure. The components of the acetabulum were successfully press-fitted into the acetabulum for all cases, including five requiring ulterior fixation obtained through the use of two screws. The femoral components were categorized using the Mont group classification: four stems were categorized as type 1, a design called single-wedge stem, characterized by flat anterior and posterior surfaces and a widened mediolateral surface with a narrower shape in the distal part [11]. Five stems were instead categorized as type 3b, therefore presenting a conical design with splines along the longitudinal axis to aid in fixation into the compact bone of the femur, and one as type 6, presenting a posterior arch to attain optimal contact when inserted into the proximal femur [11]. The mean follow-up period for evaluation of patients was 5 years, during which the Harris Hip Score was used to estimate the operational outcomes of the procedures – which improved from a preoperative mean of 34 to an 86 postoperatively – alongside a meticulous examination of the results to determine the incidence of joint infections following implantation of the prosthesis, fractures of the femur, and loosening or dislocation of the prosthesis, none of which were ultimately reported [7].
Analysis of the results indicates that the choice of the cup does not constitute a crucial issue, as the structure of the acetabulum is generally maintained. However, accurate placement and stable fixation are achieved when using press-fit cups with a hemispheric design that allows for the insertion of screws. With regard to the femoral components, type 1 and 3b designs are used for femurs presenting exostosis around the circumference of the neck, valgus neck-shaft angle, and wider neck diameter, mainly because of the straight prosthetic structure that allows for optimal meta-diaphyseal fixation. Instead, type 6 designs are more used for cases of pedicled exostosis, in which distortions are not as severe and the head and neck of the femur are not altered [7].
4 Lumbar Spinal Disorders
Osteoarthritis (OA) of the hip and pain in the spinal region frequently coexist. The alterations to which the lumbar region of the spinal cord is subjected frequently lead to severe chronic pain, which could potentially spread to the lower limbs. Therefore, when OA and lumbar spinal disorders (LSDs) occur concomitantly, it becomes more complex to establish the main source of pain in the patients [13]. However, THA has shown positive outcomes in terms of improvement of the pain in the lumbar region in patients already affected by hip osteoarthritis.
Prior to the procedure, the incidence of lower back pain (LBP) ranges from 21.2% to 60.4% [14,15,16], improving in about 60% of the cases in the postoperative period [15,16,17,18]. Nonetheless, relatively worse results have been indicated when THA was performed on patients with coexisting OA of the hip and LSD – compared to the ones not presenting any spinal disorders [13, 19] – and in patients that did not experience any improvements in the perceived pain in their lumbar region [17, 18].
4.1 Low Back Pain Improvement Using Preoperative Techniques After Performing THA: Research in Japan
The goal of the study conducted in [12] was to identify the percentage of patients experiencing improvements in their LBP after undergoing THA and to determine the preoperative spinal factors leading to such improvements.
A total of 318 primary procedures were evaluated, and the LBP was determined preoperatively via the visual analogue scale (VAS), with a score ranging from 0, indicating no pain, to 10, indicating maximum pain. In addition, the patients were asked to complete the Harris Hip Score (HHS), Oxford Hip Score (OHS), and University of California, Los Angeles (UCLA) activity scores within 1 month prior and 1 year following the surgery.
The study under analysis only included patients who received a score of 2 or higher in the preoperative VAS – ultimately involving 151 patients – which indicated the minimal clinically important difference (MCID) for lower back pain and allowed for the subsequent division of the included patients into two groups. The LBP-improved cohort was characterized by patients presenting an improvement higher than 2 points in the VAS score collected 1 year after the surgical procedure or improving from a preoperative score of 2 to a score of 0. The LBP-continued group was instead composed of patients characterized by an improvement in the VAS score of 2 or lower.
Radiographs of the spine were also analyzed with the patients standing in a relaxed position and looking in the forward direction. The parameters regarding the spine were evaluated prior to the surgical procedure. Additionally, the coronal parameters were also examined, including the Cobb angle, obliquity of the pelvis – hence the angle formed between the line joining the superior bilateral portion of the ilium and the horizontal line – and the distance separating the C7 plumb line, and the vertical line located in the central sacral area. Sagittal parameters were analyzed, including the anterior pelvic plane (APP) angle – defined as the angle between the vertical line and the plane passing through the bilateral anterior superior iliac spines and the pubic symphysis, which yielded a positive value in case the APP was rotated more forward than the vertical line – the pelvic incidence (PI), the pelvic tilt (PT), the sacral slope (SS), thoracic kyphosis, sagittal vertical axis (SVA), and lumbar lordosis (LL), alongside leg length discrepancy (LLD) [12].
The surgeries were performed via the transgluteal approach, with or without the mini-trochanteric osteotomy of the anterior section of the insertion of the gluteus medius muscle. This technique provided comprehensive visibility of the acetabulum, thus allowing for more precise positioning and orientation of the prosthetic implant, as well as increased stability for the prevention of dislocation events; however, it has been associated with increased incidence of temporary gait disablement because of the degradation of the abductor mechanism of the hip joint [20].
A total of 119 hybrid, 1 cemented, 26 cementless, 1 reverse hybrid, and 4 augmented plate and cemented implants were used throughout the procedures. Instead, the bearing surfaces employed were metal femoral head on cross-linked polyethylene in 101 instances, and ceramic head on cross-linked polyethylene in 50 cases.
The analysis of the data gathered postoperatively indicated the 62.9% of patients’ categorization in the LBP-improved cohort later on had a significantly lower mean value of 4.4 for the Cobb angle when compared to the LBP-continued cohort that had a mean value of 7.2. Additionally, the LBP-continued cohort demonstrated significant sagittal spinal imbalances postoperatively, especially regarding the APP angle, which corresponded to −6.0 ± 10.3, compared to the lower one indicated for the LBP-improved group, −1.8 ± 8.1, thus indicating an increased anterior rotation of the pelvis in the latter [12].
The results obtained for the VAS administered postoperatively, as well as the HHS, OHS, and UCLA scores, showed significantly worse outcomes for the LBP-continued group. In fact, the average score indicated for the VAS was 5.5, compared to the 0 obtained in the LBP-improved cohort. The average result from the HHS was 7.7 points higher in the LBP-improved group, which also displayed a higher average – by 5 points – in the OHS. The UCLA activity scores yielded similar outcomes, ranging from 5 to 6 in the LBP-improved group and from 3 to 6 in the LBP-continued one [12].
The factors that could have led to an improvement in the lower back pain experienced by the patients 1 year after the THA procedure were a low Cobb angle, as well as a high APP angle obtained preoperatively. Instead, factors such as a higher Cobb angle and sagittal spinal imbalances were correlated to constant LBP [12].
5 Developmental Hip Dysplasia
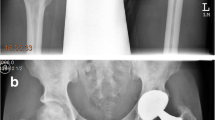
Reconstructive surgeons face many challenges when presented with the demanding procedure of hip joint reconstruction in patients affected with developmental hip dysplasia (DDH) [23]. This developmental condition is caused by mutations occurring at the WISP3 gene [21] and comprises a spectrum of progressive modifications to the femur and acetabulum, which consist in the complete distortion of the bone morphology compared to the normal rapport between femoral head and acetabulum and results in fractures, dislocation, neurovascular injuries, loosening of implants, infections, and impaired functional outcomes. THA surgeries in these patients’ results are extremely challenging and characterized by high complication rates compared to cases relative to primary osteoarthrosis, primarily because of the young age, degree of activity performed, and lack of pronounced degenerative alterations of the hips of the patients [23]. The pattern of abnormalities in dysplastic hips is characterized by a shallow acetabulum on the pelvic side, and by a small femoral head with an excessively anteverted neck on the femoral side, which lead to a reduced region of contact between the two articulating bones and therefore resulting in the transmission of a significant stress onto a reduced surface area, ultimately causing articular modifications [23]. Figure 3 depicts various radiographs that illustrate the detrimental effect of DDH on the hip of the individuals affected by this condition. Figure 3a shows the hip of a 13-year-old patient when the disease was first diagnosed. Figure 3b depicts the conditions of severe osteoarthritis of the hip of the same patient at 32 years old, which necessitated surgical intervention (THA) 2 years later, as shown in Fig. 3c. Figure 3d depicts signs of aseptic loosening of the acetabular cup after the primary THA procedure, thus requiring revision surgery. Finally, Fig. 3e illustrates the conditions of the newly implanted prosthesis after revision THA [64].

(a) Initial diagnosis of DDH, (b) advancement to a severe state of osteoarthritis, (c) THA surgery, (d) evidence of aseptic loosening of the cup after primary THA, (e) implant conditions after revision surgery
5.1 Developmental Hip Dysplasia Requiring Total Hip Replacement
The data gathered in [22] shows that the most suitable acetabular components for this complicated THA surgery are uncemented – either with or without augmentation of the surface area of the bone – which are now extensively used in moderately dysplastic hips as they present significantly low revision rates in both mid- and long-term follow-ups. Instead, cemented acetabular components seem to have a greater percentage of revision rates due to socket loosening or graft collapse, alongside decreased survival rates [24, 25]. In contrast, the use of cemented stems generated better results on the femoral side, whereas the use of proximally fit uncemented component appears to be particularly complicated in DDH patients due to deformities, which often require the addition of modular elements or the execution of osteotomy in an attempt to achieve the ideal fit [30].
Good results were also observed in DDH patients when the hip joint center was restored successfully – via radiographs performed before the procedure and intraoperative image intensifier – even through the use of a small cup characterized by a slender polyethylene liner [26]. However, problems with this specific approach have been encountered in severe cases of dislocation during the restoration of the center of rotation in THA, as the positioning of the anatomical socket might increase the difficulty of hip reduction and further increase the risk of nerve-related injuries [27,28,29,30].
Moreover, the greater flexibility in the rectification of rotational deformities and the possibility to preserve the abductor mechanism in femoral shortening via proximal osteotomy and greater trochanter distal advancement is juxtaposed with substantial complications.
In summary, THA in DDH can be adequately addressed with a uniquely designed implant, appropriate osteotomy procedures, and bone grafts, alongside precise placement of cup that allows for reconstruction of the abductor muscles’ lever arm and normal hip center, producing better results in terms of biomechanics. Despite the poorer outcomes reported for THA in DDH patients compared to the same procedures in patients not displaying any previous conditions, current evidence indicates a tendency of improving outcomes for pain relief, return to daily activities, functional improvement, and reduction of complication rates [22].
6 Renal Transplant and Hemodialysis
Renal transplant is by far the most widespread solid transplant procedure for patients with end-stage renal failure (ESRF) [36], and its positive outcomes rely on the usage of corticosteroids and immunosuppressors to avoid rejection of the newly implanted organ. However, as a consequence of the low number of donors, the number of patients receiving hemodialysis is progressively growing, and the consequences arising from this procedure, including amyloid deposition around the joint – whose major constituent was determined to be β2-microglobulin fibrils – or renal osteodystrophy, also affect the hip joint in the long run [34, 35], causing complications such as avascular necrosis, especially concerning the head of the femur [32, 33], ultimately addressed with THA.
Avascular necrosis (AVN) is generally correlated to unusually high lipid levels, which lead to the formation of microemboli and structural alterations within the cells of the endothelial layer of the integument causing the loss of proper vein function of the legs, alongside a more elevated intraosseous strain and osteonecrosis. The administration of high dosages of immunosuppressants seems to constitute one of the primary agents in the development of AVN, and it is therefore suggested to maintain the daily dosage to below 20 mg, as results indicate a risk of avascular necrosis amounting to less than 3% [36].
6.1 Total Hip Arthroplasty Outcomes on Patients with Hemodialysis and Previous Renal Transplant
THA procedures on patients with previous renal transplants or hemodialysis have been analyzed, reporting the data gathered throughout the research [32]. Results show that the comprehensive revision rate for patients previously subjected to kidney transplant corresponds to 16% at 8 years following the procedure, whereas it is slightly lower for hemodialysis patients, with a percentage of 15.7% at a mean of 7 years after primary THA [31], data that could be correlated to the migration of β2-microglobulin into the interface between bone and implant, thus contributing to early loosening of the latter [32].
Moreover, the use of uncemented implants was reported to have a substantially lower rate of revision surgeries due to dislocation or aseptic loosening for both the renal transplant (RT) group and the hemodialysis (HD) group, but the rate of deep infection calculated for end-stage renal failure patients subjected to hemodialysis was significantly higher – 10.8% – than the one obtained for the RT group, 2.1% [31]. Instead, the risk of aseptic loosening in cemented implants was reported to be significantly higher (33.3%) [31] due to the interface between bone and cement, which suppressed the formation of the bone and resulted in resorption [36] – formally described as the destruction of the bone matrix following the release of proteolytic enzymes and hydrochloric acid by osteoclasts.
Overall, THA performed through a cementless technique is considered to be the most effective alternative for patients who had been subjected to hemodialysis for an extended period of time, as data indicate a less severe stage of bone atrophy and the lack of development of stress shielding due to ingrown fixation compared to cemented THA [32].
7 Osteoarthritis
Osteoarthritis (OA) is the most widespread type of arthritis [37], and it was considered the 11th agent contributing to disability in 2015 [39]. This condition provokes severe pain during or after movements, joint stiffness, decreased flexibility and range of motion, as well as swelling [37], and it mainly affects the joints subjected to significant mechanical stress – such as the hip and the knee – causing structural changes in the hyaline articular cartilage, capsule, ultimately leading to destruction and failure of synovial joint [40]. Some of the risk factors correlated to this condition include age, female sex, deformities of the bones, and particular metabolic disorders. Additionally, another factor that increases the likelihood of developing OA is obesity [37] that is covered in the following paragraph. Figure 4a shows the radiograph of a hip in the initial stage of osteoarthritis, whereas Fig. 4b depicts the rapid progression of the disease and the detrimental effects on the hip of the patient [65].

(a) Initial stage of osteoarthritis, (b) progressive disruption of the hip joint
7.1 Impact of Weight Loss in Osteoarthritic Patients upon Total Hip and Knee Replacement
In patients affected by OA, the structural composition of cartilage is subjected to several alterations, which cause an ongoing depletion of its integrity and consequently increasing its vulnerability to external stresses [38]. In the early stages of osteoarthritis, only the surface of the articular cartilage is subjected to erosion; however, this phenomenon rapidly reaches deeper areas of the bone, which then leads to an increase in the surface of the calcified cartilage zone. Moreover, in an attempt of contrasting this inevitable erosion process, the chondrocytes present within the cartilage increase their synthetic endeavor, ultimately creating products leading to the degradation of the matrix, alongside proinflammatory mediators [40]. At this point in time, there are no authorized pharmacotherapies that have been proven to successfully prevent or cease the advancement of OA; however, several factors have been correlated to increase risks of developing the disease. Obesity is one of the main factors that provoke the development of OA [41], as results have indicated an increase of 4.6% in the probability of developing such condition compared to people with a healthy weight [42].
Based on these findings, weight loss constitutes one of the main recommendations for OA management [43,44,45,46,47]. This conclusion is backed up by studies indicating that patients experiencing a weight loss of over 7.5% compared to their initial weight displayed inferior risks of TKR. On the other hand, no significant differences were found in terms of increased risk of THR for OA patients experiencing weight loss of >7.5%; however, the risks significantly increased when patients experienced a weight gain of more than 5% [38]. These differences might be attributable to the nature of the joints under analysis. The knee is, in fact, a hinge joint, and changes in mechanical stress on a misaligned knee joint are significantly amplified due to the reduced surface area they act upon [48]. Instead, the hip joint is a ball-and-socket joint, and the greater surface area of the latter would explain the lesser sensitivity to changes in physical force as compared to the knee [38].
8 Human Immunodeficiency Virus
Human immunodeficiency virus (HIV) is a virus that targets the immune system, and, if not treated, it could culminate in acquired immunodeficiency syndrome (AIDS) [49]. The cure for this disease is yet to be discovered; however, because of the development of techniques aimed at its prevention, detection, and management, HIV is now considered more of a chronic disorder, thus allowing the affected population to carry on with their lives without major complications.
As the disorder targets and impairs the immune system of the affected individuals, the latter progressively become immunodeficient, therefore increasing their vulnerability against a wide variety of infections, as well as some kinds of cancer that healthy people are able to fight against [49].
The incidence of hip diseases associated with HIV infection is particularly common, therefore constituting a major issue particularly in South African countries, where HIV is exceptionally widespread. HIV-positive patients are more prone to the development of avascular necrosis of the hip and head of the femur, caused by the reduced mineral density of their bone connective tissue, which ultimately decreases the median age of the affected individuals requiring THA. Despite the success attributed to THA for the treatment of hip diseases, the procedure could potentially lead to severe complications in patients affected by HIV, including possible infection of the joint following the implantation of the prosthesis [51,52,53].
8.1 HIV Infection and Periprosthetic Joint Infection Correlation in Young Adults upon THA
The main goal of the study conducted in [50] was to gather the outcomes following THA in HIV-positive and HIV-negative patients, to perform a comparison of the incidence of periprosthetic joint infection (PJI) in both groups, alongside the possible correlation between HIV infection and venous thromboembolic events (VTE), revision surgery, and reintervention.
In total, 290 cases in 213 patients were comprised in the conducted analysis, with a mean age of 43 years – ranging from 26 to 54 years. The main factors leading to the performance of THA were avascular necrosis of the hip and femoral head in 78% of the cases, and osteoarthritis in the remaining 22%. The number of HIV-positive patients included in the study amounted to 180, characterized by a mean CD4 count – a value that calculates the functionality of the patient’s immune system – of 520 cells/mm3 [50].
Before the procedure, all patients were subjected to medical assessments – regardless of their HIV status – which included standard AP, lateral X-rays, blood examination, and collection of urine. For the HIV-positive group, the CD4 count was additionally attained.
The surgical procedure was later performed in all the patients, including the six presenting a CD4 count inferior to 350 cells/mm3, mainly because of the grave symptoms displayed, which resulted in serious incapacitation. The prosthesis chosen for the surgeries was an uncemented Corail®/Pinnacle System, and, following its installation, the patients were administered intravenously with three doses of prophylactic antibiotics. Subsequently, the therapy aimed at the prevention of thrombosis was commenced 12 h after the procedure, and consisted of 40 mg of enoxaparin supplied daily, which was then substituted with 10 mg of rivaroxaban – administered daily – 2 days after the procedure, sustained until 14 days postoperatively.
The obtained results showed a total of six cases of superficial wound infection after the surgery – only one of which was recorded in an HIV-positive patient – and three instances of infection of the joint postoperatively, two of which were observed in HIV-positive patients. One of the patients pertaining to the HIV-positive cohort perished due to pulmonary embolism; nonetheless, no significant difference regarding the incidence of venous thromboembolic events was observed between the two analyzed groups, which corresponded to 4% for the HIV-positive group and 6% for the HIV-negative group. The radiological assessments performed during the follow-up procedure displayed no evidence of subsidence or loosening of the implant, and no dislocations were observed during the follow-up period. Additionally, the outcomes reported by the patients, obtained via the Merle d’Aubigné Hip Score 6 months following the surgery, were analogous for both groups (p = 0.154) [50].
In conclusion, no differences were observed regarding the incidence of PJI, VTE, aseptic loosening of the implant, and patient-reported outcomes – obtained at 6 months postoperatively – as well as reintervention, mortality, or revision rates between the two groups at a mean 4-year follow-up [50].
8.2 HIV-Positive Patients’ THA Yielding Positive Functional Outcomes and Low Infection Rates
The incidence of prosthetic joint infections (PJI) has been constantly increasing despite the innovations and the improvements made to the techniques used for surgery, thus consequently leading to an increase in the requirement for revision surgeries for the treatment of such infections [55]. The HIV status of the patient is considered a substantial risk factor for PJI, alongside other factors including the body mass index and diabetic control [56]. The development of highly active antiretroviral therapy (HAART) has allowed for a more cautious management of HIV, which has now become a chronic condition rather than a fatal diagnosis. However, HIV patients treated with HAART are at increased risk of developing avascular necrosis (AVN) of the head of the femur, as the reported incidence is greater by a factor of 45–100 compared to the rest of the population [57, 58], subsequently augmenting the demand for THA.
The study performed in [54] aimed at evaluating the short- and medium-term results of non-hemophiliac HIV-positive patients subjected to THA in a sub-Saharan hospital, alongside examining patient-reported outcomes and determining the factors leading to poor outcomes and infections. The review included 87 patients that had been subjected to THA between 2010 and 2018, with a minimum follow-up period of 24 months. An examination of the CD4+ count and viral load (VL) was performed to ascertain the status of their immune system, and the surgery was initiated in patients presenting a preoperative CD4+ value over 250 cells/mm3 and, if that threshold was not reached, the procedure was postponed by 6 months. The Harris Hip Score (HHS) and Oxford Hip Score (OHS) were employed to assess the preoperative status of the patient and postoperative outcomes related to the surgery, and the condition affecting the hip was evaluated via standard radiographic techniques, and later subdivided into HIV related – if determined to be generated by HIV or a detrimental consequence of the HAART – and non-HIV related, in the case of osteoarthritis, protrusion of the acetabulum, and inflammatory arthritis.
The THA surgeries were performed via an altered anterolateral approach, and prophylactic antibiotics – consisting of cefazolin or clindamycin in case of allergies to penicillin – were administered 30 min prior and 24 h after the procedure [54]. Moreover, intravenous tranexamic acid was administered 30–60 minutes prior to the incision.
After the procedure, symptomatic patients received transfusion if the hemoglobin levels were below 8g/dL or 10g/dL, and, after discharge, low-molecular-weight heparin was prescribed for a total of 4 weeks to prevent the formation of blood clots [54].
The complications occurring after the surgery were categorized as early, if occurring before the fourth week, and late, if occurring after the fourth week, and were classified using the Clavien-Dindo-Sink Classification, which uses a grading scale of 5 points depending on the type of treatment needed for a complication [59,60,61]. The patients were then subjected to systematic follow-ups at 6 weeks, 6 months, 1 year, and then annually, which included the performance of a radiographic examination. Additionally, CD4+ count and HIV viral load were assessed at 6 weeks and then annually.
Out of the 87 patients included in the study, 15 were subjected to bilateral staged THA. The average age was 58.34 years, the average body mass index was 31.56 kg/m2, the mean value indicated for CD4+ count was 569 cells/mm3 (ranging from 51 to 1481), and the average VL was <40 copies/mL. Before the procedure, 82 patients were subjected to HAART for an average of 4.7 years, whereas the remaining 5 were not subjected to such treatment before or after the surgery and presented a mean CD4+ value of 658 cells/mm3 and of <40 copies/mL for the VL.
Avascular necrosis of the femoral head was one of the main factors leading to the THA procedure, observed in 71 patients (69.6%), followed by primary osteoarthritis, detected in 16 (15.7%). Other conditions were instead less frequent and included fractures of the femoral neck (7.8%), inflammatory conditions (2.9%), tuberculosis of the hip (0.98%), hip ankylosis (0.98%), chondrolysis (0.98%), and protrusion of the acetabulum (0.98%) [54].
Fifty-seven patients were subjected to the implantation of ceramic-on-ceramic bearing coupling, 26 to metal-on-metal polyethylene, and 19 to ceramic on polyethylene, and both uncemented and hybrid THAs were executed with DePuy Synthes CORAIL Pinnacle prosthetic implants [54].
The average length of stay was 6.4 days, and the mean size of the femur observed postoperatively was 9. The mean follow-up period was 81.24 months, during which two deaths, unrelated to the procedure, were recorded; moreover, six more patients failed to attend the periodic follow-ups. The mean CD4+ count and VL evaluated during the last follow-up were 621 cells/mm3 and <40 copies/mL, respectively [54].
In terms of functional outcomes, all patients showed significant improvement in their HHS and OHS, going from a preoperative mean value of 32 for the HHS and 23.62 for the OHS to an 81.51 and 43.43 recorded after the procedure. Additionally, the patients also reported a substantial decrease in their pain, based on the mean improvement of 8.6 on the VAS, and the overall satisfaction rate amounted to 91.4% [54].
After the procedure, the incidence of complications corresponded to 10.78%, with a total of three medical complications and eight related to the surgery. Out of these 11 complications, 4 were categorized as early, whereas 7 were classified as late, and the readmission rates were 3.92% within the first month, and 6.86% from 60 to 90 days postoperatively, whereas no readmissions were recorded in the period ranging from 30 to 60 days. Six PJIs (5.88%) – including three recently diagnosed patients that had not begun HAART – were identified and later verified by needle aspiration, one of which occurred at the site of surgery, whereas five were deep infections. Additionally, the mean VL for the patients experiencing PJIs was lower-than-detectable, and the mean CD4+ count was 523 cells/mm3 [54].
The THA was required for HIV-related causes in 78.4% of the cases, whereas it was non-HIV related in the remaining 21.6%; moreover, the incidence of complications was 7.5% for patients undergoing THA due to HIV-related causes, and 22.72% when the procedure was required for non-HIV-related motives. No correlation was found between the preoperative value indicated for CD4+ count and VL and the complications or results of the surgical procedure, as 8 out of the 11 patients who experienced complications had a CD4+ count equal or greater than 350 cells/mm3, and 5 out of the 6 patients that experienced septic complications had a CD4+ count of ≥350 cells/mm3 [54].
In summary, a substantial risk factor for the development of PJIs is the noncompliance or delayed commencement of HAART, whereas factors such as CD4+ count and VL are not correlated with worse clinical results or greater incidence of complications. Additionally, a substantial increase in functional outcomes can be achieved after THA, which can be safely executed in patients presenting HIV and undergoing HAART [54].
References
Al-Otaibi ML, et al. Total hip replacement in sickle cell disease patients with avascular necrosis of head of femur: a retrospective observational study. Ind J Orthopaedic. 2021; https://doi.org/10.1007/s43465-021-00394-6.
Houwing M, de Pagter P, van Beers E, Biemond B, Retten-bacher E, Rijneveld A, Schols EM, Philipsen JNJ, Tam-minga RYJ, van Draat KF, Nur E, Cnossen MH, SCORE Consortium. Sickle cell disease: clinical presentation and management of a global health challenge. Blood Rev. 2019;37:100580.
Al-Mousawi F, Malki A, Al-Aradi A, Al-Bagali M, Al-Sadadi A, Booz M. Total hip replacement in sickle cell disease. Int Orthop. 2002;26:157–61. Feb 14, 2019
Hernigou P, Zilber S, Filippini P, Mathieu G, Poignard A, Galacteros F. Total THA in adult osteonecrosis related to sickle cell disease. Clin Orthop Relat Res. 2008;2008(466):300–8.
Ilyas I, Alrumaih HA, Rabbani S. Noncemented total hip arthroplasty in sickle-cell disease: long-term results. J Arthroplasty. 2018;33:477–81.
D’Arienzo, Antonio, et al. Hereditary multiple exostoses: current insights. Orthopedic research and reviews, U.S. National Library of Medicine, 13 Dec. 2019., https://pubmed.ncbi.nlm.nih.gov/31853203/
Ostetto F, et al. Total hip arthroplasty in hereditary multiple exostosis patients: literature review and evaluation of 10 cases. Hip Int. 2021:112070002110250. https://doi.org/10.1177/11207000211025051.
Solomon L. Hereditary multiple exostosis. Am J Hum Genet. 1964;16:351–63.
Yoong P, Mansour R, Teh JL. Multiple hereditary exostoses and ischiofemoral impingement: a case-control study. Skeletal Radiol. 2014;43:1225–30.
Scarborough MT, Moreau G. Benign cartilage tumors. Orthop Clin North Am. 1996;27:583–9.
Kim, Jung Taek, and Jeong Joon Yoo. Implant design in cementless hip arthroplasty. Hip & pelvis, Korean Hip Society, June 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4972888/
Okuzu Y, et al. Preoperative factors associated with low back pain improvement after total hip arthroplasty in a japanese population. J Arthroplasty. 2021; https://doi.org/10.1016/j.arth.2021.08.025.
Ellenrieder M, Bader R, Bergschmidt P, Fröhlich S, Mittelmeier W. Coexistent lumbar spine disorders have a crucial impact on the clinical outcome after total hip replacement. J Orthop Sci. 2015;20:1046–52. https://doi.org/10.1007/s00776-015-0764-y.
Hsieh PH, Chang Y, Chen DW, Lee MS, Shih HN, Ueng SW. Pain distribution and response to total hip arthroplasty: a prospective observational study in 113 patients with end-stage hip disease. J Orthop Sci. 2012;17:213–8. https://doi.org/10.1007/s00776-012-0204-1.
Parvizi J, Pour AE, Hillibrand A, Goldberg G, Sharkey PF, Rothman RH. Back pain and total hip arthroplasty: a prospective natural history study. Clin Orthop Relat Res. 2010;468:1325–30. https://doi.org/10.1007/s11999-010-1236-5.
Staibano P, Winemaker M, Petruccelli D, de Beer J. Total joint arthroplasty and preoperative low back pain. J Arthroplasty. 2014;29:867–71. https://doi.org/10.1016/j.arth.2013.10.001.
Chimenti PC, Drinkwater CJ, Li W, Lemay CA, Franklin PD, O’Keefe RJ. Factors associated with early improvement in low back pain after total hip arthroplasty: a multi-center prospective cohort analyses. J Arthroplasty. 2016;31:176–9. https://doi.org/10.1016/j.arth.2015.07.028.
Weng W, Wu H, Wu M, Zhu Y, Qiu Y, Wang W. The effect of total hip arthroplasty on sagittal spinal-pelvic-leg alignment and low back pain in patients with severe hip osteoarthritis. Eur Spine J. 2016;25:3608–14. https://doi.org/10.1007/s00586-016-4444-1.
Prather H, Van Dillen LR, Kymes SM, Armbrecht MA, Stwalley D, Clohisy JC. Impact of coexistent lumbar spine disorders on clinical outcomes and physician charges associated with total hip arthroplasty. Spine J. 2012;12:363–9. https://doi.org/10.1016/j.spinee.2011.11.002.
Kuroda Y, Akiyama H, Nankaku M, So K, Matsuda S. Modified Mostardi approach with ultra- high-molecular-weight polyethylene tape for total hip arthroplasty provides a good rate of union of osteotomized fragments. J Orthop Sci. 2015;20(4):633–41. https://doi.org/10.1007/s00776-015-072-9.
Hashmi JA, Basit S, Khoshhal KI. Genetics of developmental dysplasia of the hip: Recent progress and future perspectives. J Musculoskelet Surg Res. 2019;3:245–53.
Papachristou GC, et al. Total hip replacement in developmental hip dysplasia: a narrative review. Cureus. 2021; https://doi.org/10.7759/cureus.14763.
Sanchez-Sotelo J, Trousdale RT, Berry DJ, Cabanela ME. Surgical treatment of developmental dysplasia of the hip in adults: I. Non arthroplasty options. J Am Acad Orthop Surg. 2002;10:321–33. https://doi.org/10.5435/00124635-200209000-00004.
Clavé A, Tristan L, Desseaux A, Gaucher F, Lefèvre C, Stindel E. Influence of experience on intra- and inter- observer reproducibility of the Crowe, Hartofilakidis and modified Cochin classifications. Orthop Traumatol Surg Res. 2016;102:155–9. https://doi.org/10.1016/j.otsr.2015.12.009.
Hartofilakidis G, Babis GC, Lampropoulou-Adamidou K, Vlamis J. Results of total hip arthroplasty differ in subtypes of high dislocation. Clin Orthop Relat Res. 2013;471:2972–9. https://doi.org/10.1007/s11999-013-2983-x.
Perka C, Fischer U, Taylor WR, Matziolis G. Developmental hip dysplasia treated with total hip arthroplasty with a straight stem and a threaded cup. J Bone Joint Surg Am. 2004;86:312–9. https://doi.org/10.2106/00004623-200402000-00014.
Rasi AM, Kazemian G, Khak M, Zarei R. Shortening subtrochanteric osteotomy and cup placement at true acetabulum in total hip arthroplasty of Crowe III-IV developmental dysplasia: results of midterm follow-up. Eur J Orthop Surg Traumatol. 2018;28:923–30. https://doi.org/10.1007/s00590-017-2076-8.
Kim M, Kadowaki T. High long-term survival of bulk femoral head autograft for acetabular reconstruction in cementless THA for developmental hip dysplasia. Clin Orthop Relat Res. 2010;468:1611–20. https://doi.org/10.1007/s11999-010-1288-6.
Hitz OF, Flecher X, Parratte S, Ollivier M, Argenson JN. Minimum 10-year outcome of one-stage total hip arthroplasty without subtrochanteric osteotomy using a cementless custom stem for Crowe III and IV hip dislocation. J Arthroplasty. 2018;33:2197–202. https://doi.org/10.1016/j.arth.2018.02.055.
Zhen P, Liu J, Lu H, Chen H, Li X, Zhou S. Developmental hip dysplasia treated by total hip arthroplasty using a cementless Wagner cone stem in young adult patients with a small physique. BMC Musculoskelet Disord. 2017;18:192. https://doi.org/10.1186/s12891-017-1554-9.
Popat R, et al. Outcomes of total hip arthroplasty in haemodialysis and renal transplant patients: systematic review. Hip Int. 2019;31(2):207–14. https://doi.org/10.1177/1120700019877835.
Nagoya S, Nagao M, Takada J, et al. Efficacy of cementless total hip arthroplasty in patients on long-term hemodialysis. J Arthroplasty. 2005;20:66–71.
Abbott KC, Bucci JR, Agodoa LY. Total hip arthroplasty in chronic dialysis patients in the United States. J Nephrol. 2003;16:34–9.
Jadoul M, Drüeke TB. β2 microglobulin amyloidosis: an update 30 years later. Nephrol. Dial. Transplant. 2016;31:507–9.
Fukunishi S, Yoh K, Kamae S, et al. Beta 2-microglobulin amyloid deposit in HLA-B27 transgenic rats. Mod. Rheumatol. 2007;17:380–4.
Nowicki P, Chaudhary H. Total hip replacement in renal transplant patients. J Bone Joint Surg Br. 2007;89:1561–6.
“Osteoarthritis.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 16 June 2021., https://www.mayoclinic.org/diseases-conditions/osteoarthritis/symptoms-causes/syc-20351925
Jin X, et al. Does weight loss reduce the incidence of total knee and hip replacement for osteoarthritis? – a prospective cohort study among middle-aged and older adults with overweight or obesity. Int J Obes (Lond). 2021, 1696–1704;45(8) https://doi.org/10.1038/s41366-021-00832-3.
Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1545–602.
Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393:1745–59.
Salih S, Sutton P. Obesity, knee osteoarthritis, and knee arthroplasty: a review. BMC Sports Sci Med Rehabil. 2013;5:25.
Zheng H, Chen C. Body mass index and risk of knee osteoarthritis: systematic review and meta-analysis of prospective studies. BMJ Open. 2015;5:e007568.
McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Beren-baum F, Bierma-Zeinstra SM, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr Cartil. 2014;22:363–88.
Fernandes L, Hagen KB, Bijlsma JWJ, Andreassen O, Christensen P, Conaghan PG, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis. 2013;72:1125–35.
Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012;64:465–74.
American Academy of Orthopaedic Surgeons. Treatment of osteoarthritis of the knee. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013.
RACGP. Guidelines for the management of knee and hip osteoarthritis. East Melbourne, VIC: Royal Australian College of General Practitioners; 2018.
Reijman M, HaP P, Bergink AP, Hazes JMW, Belo JN, Lievense AM, et al. Body mass index associated with onset and progression of osteoarthritis of the knee but not of the hip: the Rotterdam Study. Ann Rheum Dis. 2007;66:158–62.
“HIV/AIDS.” World Health Organization, World Health Organization, https://www.who.int/news-room/fact-sheets/detail/hiv-aids
Ngwazi M, et al. The association between HIV infection and periprosthetic joint infection following total hip replacement in young adults. SA Ortho J. 2021;20(2) https://doi.org/10.17159/2309-8309/2021/v20n2a2.
Pietrzak JRT, Maharaj Z, Mokete L, Sikhauli N. Human immunodeficiency virus in total hip arthroplasty. EFORT Open Rev. 2020;5:161–71.
Parvizi J, Sullivan TA, Pagnano MW, Trousdale RT, Bolander ME. Total joint arthroplasty in human immunodeficiency virus-positive patients: An alarming rate of early failure. J Arthroplasty. 2003;18(3):259–64.
Lehman CR, Ries MD, Paiement GD, Davidson AB. Infection after total joint arthroplasty in patient with human immunodeficiency virus or intravenous drug use. J Arthroplasty. 2001;16(3):330–5.
Rajcoomar S, et al. Good functional outcomes and low infection rates in total hip arthroplasty in HIV-positive patients, provided there is strict compliance with highly active antiretroviral therapy. J Arthroplasty. 2021;36(2):593–9. https://doi.org/10.1016/j.arth.2020.08.021.
Natsuhara KM, Shelton TJ, Meehan JP, Lum ZC. Mortality during total hip periprosthetic joint infection. J Arthroplasty. 2019;34:S337e42. https://doi.org/10.1016/j.arth.2018.12.024.
Edwards PK, Mears SC, Stambough JB, Foster SE, Barnes CL. Choices, compromises, and controversies in total knee and total hip arthroplasty modifiable risk factors: what you need to know. J Arthroplasty. 2018;33:3101e6. https://doi.org/10.1016/j.arth.2018.02.066.
Mehta P, Nelson M, Brand A, Boag F. Avascular necrosis in HIV. Rheumatol Int. 2013;33:235e8. https://doi.org/10.1007/s00296-011-2114-5.
Morse CG, Mican JM, Jones EC, Joe GO, Rick ME, Formentini E, et al. The incidence and natural history of osteonecrosis in HIV-infected Adults. Clin Infect Dis. 2007;44:739e48. https://doi.org/10.1086/511683.
Clavien PA, Sanabria JR, Strasberg SM. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery. 1992;111:518e26.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205e13. https://doi.org/10.1097/01.sla.0000133083.54934.ae.
Sink EL, Leunig M, Zaltz I, Gilbert JC, Clohisy J. Reliability of a complication classification system for orthopaedic surgery hip. Clin Orthop Relat Res. 2012;470:2220e6. https://doi.org/10.1007/s11999-012-2343-2.
Alzubaidi L, Al-Shamma O, Fadhel MA, Farhan L, Zhang J. Classification of red blood cells in sickle cell anemia using deep convolutional neural network. In: Abraham A, Cherukuri A, Melin P, Gandhi N, editors. Intelligent systems design and applications. ISDA 2018 2018. Advances in intelligent systems and computing, vol. 940. Cham: Springer; 2020. https://doi.org/10.1007/978-3-030-16657-1_51.
Ikeuchi K, Hasegawa Y, Sakano S, et al. Eccentric rotational acetabular osteotomy for osteoarthritis of the hip due to hereditary multiple exostosis: report of two cases. J Orthop Sci. 2014;19:847–50. https://doi.org/10.1007/s00776-013-0374-5.
Rahm S, Hoch A, Tondelli T, et al. Revision rate of THA in patients younger than 40 years depends on primary diagnosis – a retrospective analysis with a minimum follow-up of 10 years. Eur J Orthop Surg Traumatol. 2021;31:1335–44. https://doi.org/10.1007/s00590-021-02881-w.
Flemming DJ, Gustas-French CN. Rapidly Progressive Osteoarthritis: a Review of the Clinical and Radiologic Presentation. Curr Rheumatol Rep. 2017;19:42. https://doi.org/10.1007/s11926-017-0665-5.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Tokgöz, E. (2023). Preexisting Conditions Leading to Total Hip Arthroplasty. In: Total Hip Arthroplasty. Springer, Cham. https://doi.org/10.1007/978-3-031-08927-5_2
Download citation
DOI: https://doi.org/10.1007/978-3-031-08927-5_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-08926-8
Online ISBN: 978-3-031-08927-5
eBook Packages: EngineeringEngineering (R0)