
Abstract
Sleep, wakefulness and delirium are all associated with distinct patterns of brain activity that are detectable by scalp electroencephalography (EEG). During varying stages of sleep, common patterns visible on EEG include slow waves, delta waves, theta activity, spindles and K-complexes. These patterns reflect sleep-related homeostatic activities such as metabolic waste removal and memory consolidation. Sleep deprivation is associated with disruption of these patterns and changes in functional connectivity; the latter particularly in areas of the brain that mediate executive functions including attention, volitional behavior and emotional regulation. Based on these observations, we explore the neurophysiologic changes that may underlie the bidirectional link between sleep deprivation and delirium. We discuss implications for sleep monitoring in the ICU, current gaps in knowledge and opportunities for future research in this area.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Sleep deprivation
- Sleep disruption
- Electroencephalography
- ICU delirium
- Long-term cognitive impairment
- Dementia
- Memory consolidation
- Spindles
- Delta waves
- Functional connectivity
1 Introduction
The cognitive benefits of sleep are most evident when normal sleep is disrupted. The neurophysiologic processes underlying these benefits have been the subject of investigation for nearly a century. An important tool in this line of investigation is electroencephalography (EEG), the recording and interpretation of patterns of electrical signals from the brain. Unique patterns have been identified in EEG signals that indicate specific stages of sleep and signify particular interactions among neuronal populations within the brain. Sleep disruption is associated with altered EEG dynamics both during wakefulness and in subsequent sleep. Significant sleep disruption can precipitate delirium, a syndrome of brain dysfunction characterized by altered mental status, fluctuating levels of arousal, inattention and disordered thinking. Given that delirium is also characterized by altered physiologic patterns on EEG, this modality may provide clues to the mechanistic processes underlying the relationship between sleep disruption and delirium. In the present chapter we explore this relationship through the lens of EEG. The clinical relationship between sleep disruption and delirium is covered in chapter “Sleep Disruption and Its Relationship with Delirium: Clinical Perspectives”.
2 The Restorative Neurophysiology of Sleep
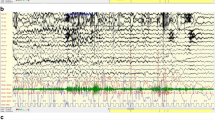
Building on the chapter “Characteristics of Sleep in Critically Ill Patients. Part I: Sleep Fragmentation and Sleep Stage Disruption”, electroencephalography (EEG) consists of the recording and interpretation of time-varying patterns of electrical signals from the brain. Identification of these patterns in the brain’s electrical activity allows one to distinguish sleep states from wakefulness and other states of consciousness (e.g. coma or delirium). Neurophysiologists examine, either by visual inspection or by quantitative analysis, the relative contributions to the EEG signal of oscillations in specific frequency ranges. The ranges most commonly identifiable on scalp EEG in adults are slow oscillations (less than 1 Hz), delta (1–4 Hz), theta (4–7 Hz), alpha (7–13 Hz), and beta (13–35 Hz) frequencies. In healthy individuals the EEG typically demonstrates alpha activity during wakefulness, theta activity during drowsiness, slow oscillations and delta activity during non-rapid eye movement (NREM) sleep and beta activity during rapid eye movement (REM) sleep (Fig. 1). Sleep spindles are a defining feature of stage II sleep. These sporadic 12–15 Hz oscillations have an outline that resembles an old-fashioned sewing spindle (broad in the middle and tapered at either end). They frequently occur in association with K-complexes - brief, high amplitude deflections of about 1 s in duration. K-complexes can often be elicited by sudden acoustic stimuli during sleep (K stands for “knock”) and likely reflect the integrity of the brain’s ability to ‘filter’ sensory stimuli [1, 2].

Selected EEG patterns related to sleep and brain structures involved in their generation. Sleep spindles and K complexes [green] indicate stage II sleep and are generated through bidirectional interactions between the thalamus and the cortex. Delta (1–4 Hz) waves [blue] predominate in slow-wave sleep and are largely driven by thalamocortical cells, though local cortical regions can generate their own intrinsic delta activity. Hippocampal theta (4–7 Hz) activity [purple] is characteristically present during REM sleep but may also appear during stages I and II
The oscillatory patterns recorded during sleep EEG are associated with specific neurophysiologic activities that support healthy cerebral function. Theta oscillations in sleep are associated with replaying memories acquired during wakefulness. Delta waves drive clearance of the brain’s waste products and may facilitate synaptic homeostasis, a mechanism by which the brain is theorized to “reorganize” itself to allow for more efficient processing. Sleep spindles are associated with memory consolidation and thus likely facilitate learning and cognitive processing. These patterns are postulated to result from interactions between the brain cortex and the thalamus, an egg-shaped structure near the center of the brain that largely serves as a relay between the brainstem and the cortex. Coordinated oscillations across disparate brain regions (also known as “functional connectivity”) allow for these regions to communicate in support of processes such as memory replay. In the remainder of this section we discuss recent work to elucidate the functions supported by these patterns of electrical activity during sleep. Though much of our knowledge to date is informed by animal studies, we focus primarily on oscillatory activity that can be measured by scalp EEG in vivo in humans.
2.1 Slow Oscillations and Delta Waves
Slow oscillations reflect neuronal firing patterns that typically fluctuate at less than 1 Hz and occur synchronously throughout the brain. They are generated by bidirectional interactions between neurons in the thalamus and the brain cortex during NREM sleep. Slow oscillations are characterized by alternating UP states (periods of increased activity of neurons in the thalamus and primary sensorimotor areas of the cortex) and DOWN states (periods of relative quiescence). These rhythms are postulated to modulate the brain’s delta wave activity during sleep [3]. They are important for sleep-dependent learning and memory processing [4], especially that of declarative (fact-based or explicit) and recognition memories [5, 6]. Delta waves, also characteristically present in NREM sleep, fluctuate between 1 Hz and 4 Hz in regional populations of neurons. Delta waves appear to be generated by intrinsic activity in the cortex that is augmented by input from the thalamus [7, 8]. Kim et al. [4] used optogenetic silencing of neurons to disrupt delta waves and observed an increase in performance gains on a skill learned prior to sleep. These observations suggest that delta waves are important for homeostatic forgetting of memories acquired prior to sleep, a function that may support effective memory consolidation [9]. Since encoding of information in the brain occurs by sequential replay of neuronal firing patterns [10, 11], memory formation requires strengthening synaptic connections among neurons (which require a considerable amount of energy to maintain). According to the synaptic homeostasis hypothesis, an important role of sleep is to “prune” these connections to allow efficient energy expenditure while integrating newly acquired information into the lived experience of the individual [9].
In addition to supporting memory consolidation, delta waves drive pulsations of cerebrospinal fluid (CSF) in and out of the skull cavity through the fourth ventricle during sleep (Fig. 2) [12]. In anesthetized animals, delta activity correlates with an influx of CSF alongside perivascular spaces through the glymphatic system [13], a paravascular pathway that facilitates clearance of interstitial solutes in the brain [14]. Delta waves thus play a role in the homeostatic evacuation of the brain’s waste products. This may explain why delta activity reduces buildup of tau protein [15] and why suppression of slow-wave activity results in buildup of amyloid beta protein [16], both markers of age-related dementia. It also may explain why suppression of delta waves is associated with age-related memory impairment [17].

EEG slow-delta waves are coupled to CSF oscillations. (a) Mean amplitude envelope of slow-delta EEG, (b) mean derivative of BOLD signals, and (c) mean CSF signal, all locked to the peaks of CSF waves during sleep in 13 humans undergoing simultaneous EEG and fMRI during NREM sleep. The shaded region represents the standard error across peak-locked trials (n = 123 peaks). (d) Calculated impulse response of the CSF signal to the EEG envelope shows a time course similar to that of previously established hemodynamic models. Shading indicates standard deviation across model folds. (e) Diagram of model linking the time course of neural activity to CSF flow. Variables include CBF and cerebral blood volume (CBV). With permission from The American Association for the Advancement of Science © 2019
The improved efficiencies in memory resulting from slow oscillations and delta waves may facilitate cognitive performance after sleep. A computational model of sleep spindles and slow oscillations with delta waves showed that the latter allow competition between memories such that memories with more reinforcement take precedence over weaker memories in the memory replay and consolidation process [18]. A separate model of sleep-like slow oscillations generated by interactions between the thalamus and the cortex showed that these oscillations are beneficial to cognitive task performance [19].
2.2 Sleep Spindles and K Complexes
Sleep spindles and K complexes result from a complex interplay among the thalamus, the hippocampus and the brain’s cortex [20, 21]. Maingret and colleagues [22] examined this phenomenon using intracranial electrodes implanted in a series of male Long-Evans rats. The authors used timed electrical stimulation to modulate the electrical patterns underlying spindles and the associated delta waves that together form K complexes during sleep. Using a spatial memory task before and after sleep, they observed that tighter coupling between cortical spindles and hippocampal fast ripples was associated with improvements in memory consolidation. Van Schalkwijk and colleagues [23] recorded sleep before and after a procedural memory task in humans and found improved task performance (fewer errors) the following day in those whose sleep spindle activity increased after learning the task. The authors concluded that spindle activity was important for memory consolidation in this sample. On the other hand, deficits in sleep spindles correlate with impaired memory consolidation among patients with schizophrenia [24]. These findings support the theory that sleep spindles are a key mechanism by which sleep supports memory consolidation.
2.3 Theta Waves
The hippocampi are a pair of horn-shaped structures in the medial regions of the brain bilaterally. The hippocampi are important for memory encoding and retrieval, and are postulated to be the primary source of theta (4–7 Hz) activity during NREM and REM sleep [25,26,27]. The hippocampus uses theta oscillations to encode memories of specific sequences of locations, such as the path an animal might take to find food [28] and reactivate when planning to repeat the same sequence [29]. REM theta oscillations are also proposed to mediate processing of emotional memories by way of coordinated activity between the hippocampus and the cortex [30]. Coordinated theta activity between the hippocampus and the ventral striatum, a brain structure important to salience, facilitates replay of memories during sleep [27, 31]. This ‘memory replay’ phenomenon has been observed in humans and rodents, and is postulated to be the first step in the process of sleep-dependent memory consolidation [32].
2.4 Functional Connectivity Patterns in Normal Sleep
Functional connectivity refers to the degree of covariance between two physiologic signals recorded from distinct regions of the brain. Commonly recorded signals include electrical fluctuations, as recorded using EEG, and hemodynamic fluctuations, as measured using blood oxygen level dependent (BOLD) fMRI. An observed correlation between two signals suggests some form of communication between the neuronal populations that generate them, either by causal influence of one population over the other, or by virtue of a third party generator that exerts a synchronizing influence over both populations simultaneously [33]. The synchronizing population may or may not represent part of a “rich club”—a group of highly interconnected brain regions that play a key role in global integration of information across the entire brain [34]. Measures of instantaneous connectivity across the cerebral cortex are lower in slow-wave sleep compared to wakefulness [35, 36]. This phenomenon may reflect the corresponding decrease in sensory integration that occurs with diminished conscious awareness during sleep [37].
The functional utility of altered connectivity patterns during sleep has been under much speculation. During slow wave sleep, sequences of neuronal firing patterns observed during wakefulness are spontaneously replayed at an accelerated timescale [38]. Berkers et al. trained volunteers on 50 visual stimuli paired with 50 auditory stimuli during wakefulness and monitored the same individuals using EEG and fMRI during sleep. When the participants reached slow-wave sleep, the investigators prompted reactivation of memories by replaying the auditory stimuli at low volume. They then tested the participants’ memory of the audio-visual pairings after awakening. They found that greater connectivity between stimulus-relevant areas of the cortex and the hippocampus during memory reactivation correlated with better performance on the post-sleep memory task [39]. This finding suggests dynamic changes in brain connectivity patterns during sleep may support memory replay, a key step in sleep-related memory consolidation [5]. Computational models suggest the observed changes in connectivity may in turn be driven by theta oscillations [40], and this is supported by a study of post-sleep recall of vocabulary learned prior to sleep [27].
Functional connectivity may also play a role in determining when sleep may be disrupted by external sensory stimuli. Bastuji and colleagues [41] used lasers to deliver stimuli during slow-wave sleep to 14 individuals undergoing intracranial EEG monitoring for epilepsy. They observed a significant increase in the probability of awakening when there was enhanced connectivity among areas of the brain responsible for sensory processing. This association was maintained independent of sleep stage and may explain, in part, the observation that ICU patients exhibit very little slow-wave sleep. If the brain’s intrinsic response to sepsis or sedation, for example, results in greater connectivity among sensory regions, this may result in higher sensitivity to the variety of stimuli in the ICU environment.
3 Neural Dynamics in Sleep Disruption
During and after sleep disruption, there are observable changes in EEG activity patterns. Sleep deprivation disrupts functional connectivity, primarily in the prefrontal cortex and related regions. Sleep deprivation was associated with decreased connectivity between left central and right frontocentral regions during wakefulness in a series of 18 healthy, right-handed young men [42]. Vermeij and colleagues [43] compared high-density resting state EEGs in a series of eight healthy participants during a day following normal sleep versus a day following sleep disruption. Using a graph theoretical analysis approach, the authors found sleep deprivation to affect the EEG in a manner that was topographically specific: a significant decrease in prefrontal interconnectedness in the alpha frequency band (typically associated with normal wakefulness), and a significant increase in global functional connectivity in the theta frequency range. The fact that the prefrontal region was the most strongly affected, may explain why functions mediated by this region may be most impacted by sleep deprivation [43]. Such functions include the process of initiating or sustaining any non-reflex response (energization), developing and implementing a plan (task setting), periodically checking that one remains on task (monitoring), behavioral/emotional regulation, understanding of one’s own thoughts (metacognition), vigilant attention, working memory, and learning that is dependent on the hippocampus [44, 45]. Deficits in functional connectivity of the prefrontal cortex due to sleep deprivation may be expected to result in deficits in any or all of these executive functions which are some of the defining clinical features of delirium (see chapter “Sleep Disruption and Its Relationship with Delirium: Clinical Perspectives”).
Aberrant functional connectivity may also be the mechanism by which sleep deprivation leads to neuropsychological dysfunction and impairment of fine motor control. Decreased connectivity between the prefrontal cortex and the amygdala, an almond-shaped region important for processing of fear and other emotions, results in impaired emotional regulation in sleep-deprived individuals. In a study of 30 healthy adult males undergoing 36 h of complete sleep deprivation, alterations in connectivity among regions involved in motor regulatory control were associated with impaired somatic fine motor function [46]. The same study revealed aberrant communication of sensory information in areas responsible for sensory processing. Altogether these findings suggest that changes in functional connectivity among specific brain networks underlie cognitive and motor deficits after sleep deprivation [46].
EEG activity patterns can be quantified to measure the brain’s response to sleep deprivation. Skorucak and colleagues [47] conducted a cross-over study to investigate the response to 7 days of sleep restriction (6 h in bed) versus sleep extension (10 h in bed) followed by 40 h of sleep deprivation and 12 h of recovery sleep in healthy participants. The investigators used polysomnographic recordings during the sleep sessions to examine sleep architecture and slow-wave activity. Sleep deprivation resulted in less REM sleep during sleep restriction and greater frontal and central slow wave activity during recovery sleep [47, 48].
The recovery period that follows sleep deprivation is more intense than normal sleep. Characteristics of this increased intensity include decreased responsiveness to the environment, altered EEG properties (specifically increased delta power and decreased sleep spindle activity), and increased sleep time. In a study by Mander and colleagues [49], 9 healthy adults underwent functional magnetic resonance imaging (fMRI) on two occasions: once after 9 h of normal sleep following 38 h of being awake, and once after 10 h of recovery sleep, also following 38 hours of being awake. It was found that recovery sleep was an average of 111 min longer than normal sleep. Recovery sleep also altered markers of prefrontal activation the following day. The increase in delta power during recovery sleep was most prominent in the frontal cortex, and task performance increased with recovery sleep. These findings reinforce the claim that slow-wave sleep is important for the recovery of prefrontal functions (including task performance) that may be lost or diminished during sleep deprivation.
4 Neural Dynamics in Delirium
The electrophysiologic characteristics of delirium were first described by Engel and Romano in the 1940s [50]. They placed electrodes at the frontal, central and posterior areas of the scalp in 53 patients and grouped recordings into five stages of delirium based on their observations of the patients’ degree of disturbance in awareness. Delirium severity progressively worsened from stage I to stage V. In stages I and II (mild to moderate delirium) the authors observed normal waking EEG patterns with increased theta (5–7 Hz) activity. In stages II and III there was a predominance of low voltage fast (beta) activity. Stages III and IV were characterized by prominent delta and theta activity (2–7 Hz oscillations) with very little of the alpha (8–13 Hz) activity typically seen in normal wakefulness. In stage IV there were periods of regular (monomorphic), high amplitude delta (0.5–3 Hz) waves, at times with superimposed low voltage fast beta activity. In the most severe stage of delirium (stage V), the EEG was almost entirely composed of fairly regular, moderately high amplitude delta activity (3–7 Hz). Little to no normal alpha or beta activity was apparent at this stage.
In the decades since this original investigation, the patterns of activity described by Romano and Engel have been observed in groups of patients with specific etiologies of delirium. Increased irregular theta and delta activity is typically present in delirium due to endocrine or metabolic disorders [51]. Repetitive, frontally predominant delta waves with a characteristic triphasic morphology are historically associated with hepatic encephalopathy but have also been observed in renal failure, respiratory failure, severe sepsis and medication toxicity [52,53,54]. Intoxication with benzodiazepines or other substances that activate gamma aminobutyric acid (GABA) receptors in the brain is associated with increased beta activity, particularly in frontal regions [55]. Monomorphic delta waves with overriding beta activity can be observed in patients with autoimmune encephalitis [56]. Yet for the most part, attempts to obtain diagnostic specificity in regard to delirium etiology have been disappointing using conventional analysis techniques [53].
Some investigators have attempted to characterize electroencephalographic patterns in delirium using more computational techniques. Numan and colleagues [57] recorded EEGs in 18 patients with postoperative hypoactive delirium and 40 age- and sex-matched controls (20 recovering from anesthesia and 20 non-delirious control patients). In general, EEGs in the delirious patients were similar to those in the sedated patients, demonstrating increased delta activity and decreased global functional connectivity in the alpha range compared to non-delirious controls. Compared to patients recovering from anesthesia, the EEG in delirious patients exhibited less activity in the alpha (8–13 Hz) frequency range. Betweenness centrality, a measure of global integration, was also decreased in the alpha range in delirium compared with controls and with sedated patients [57].
Importantly, EEG recordings change dynamically. The features we have described thus far may fluctuate over time in terms of their relative contributions to the overall EEG signal. These fluctuations can reasonably be expected to be even more prominent in the case of delirium, which is commonly characterized by changes in level of arousal and alertness, and transient phenomena such as hallucinations. Van der Kooi and Slooter [58] captured these fluctuations elegantly by measuring the coefficient of variation (CV) of the canonical frequency ranges among 26 delirious and 28 non-delirious patients after cardiac surgery. Delirium was associated with increased CV in the alpha (8–13 Hz) range globally, and increased CV in the beta (13–20 Hz) range in the frontal region. Contrary to other frequency ranges, CV in the delta (0.5–4 Hz) range was decreased in the delirium group. The mechanisms for this difference are incompletely understood but may relate to post-anesthetic sleep intrusions among non-delirious participants that are suppressed in delirium. Importantly, alterations in the variability of delta activity not only may occur in acute delirium but may give hints to patterns of cognitive impairment long after critical illness [59]. Further exploration of these phenomena may provide clues to the distinction between the pathological delta activity associated with delirium and ‘normal’ delta oscillations contributing to healthy brain activity during sleep.
The EEG patterns classically associated with mild to moderate stages of delirium have also been described in mechanically ventilated patients, who commonly experience severe sleep disruption [60, 61]. Clinical evidence of delirium (as determined by Glasgow Coma Scale [62] score less than 15 or a Richmond Agitation-Sedation Scale [63] score less than −1 and positive Confusion Assessment Method for the ICU) was an exclusion criterion for this study. Yet 16 (28%) of 57 patients demonstrated periods of high amplitude irregular (polymorphic) delta activity without sleep spindles or K complexes, which the authors termed “atypical sleep”. During wakefulness, these patients exhibited excessive theta (6 Hz and below) activity, which the authors described as “pathologic wakefulness”. The striking similarity between these patterns and those classically described by Romano and Engel [50], along with the observation that sleep deprived patients are at higher risk of delirium [64], raises the possibility that delirium and atypical sleep/pathologic wakefulness may reflect two sides of the same coin. Chapter “Atypical Sleep and Pathologic Wakefulness” describes these findings in greater detail.
5 Sleep Deprivation: Toward a Hypothesis of Deliriogenesis
The electrophysiologic changes observed in sleep deprivation give a window into possible mechanisms by which sleep disruption may precipitate delirium in compromised individuals (Table 1). When wakefulness persists and normal NREM sleep is not permitted to take place, a lack of slow oscillations and delta waves lead to disrupted CSF flow dynamics [12]. This may result in a buildup of the brain’s waste products, a consequence that may have effects akin to hepatic or renal compromise, wherein systemic toxins are allowed to build up in the bloodstream. In such cases patients often experience fluctuations in level of arousal and impaired judgment. Decreased waste clearance might be expected to have more pronounced acute effects in the context of neurodegenerative diseases, such that this may preferentially affect people already vulnerable because of an underlying condition such as dementia [65]. Indeed, accumulation of toxic protein aggregates is a pathological hallmark of Alzheimer’s Disease (AD) [66], and patients with AD experience worse cognitive decline after an episode of delirium [67].
A lack of coordinated theta waves, delta waves and spindles due to sleep disruption likely impairs the brain’s ability to process and consolidate memories [3]. Absent or diminished memory consolidation hinders retention of past information and, according to prevailing theory of memory consolidation mechanisms, may result in a progressively disorganized cortical network. This disorganization is characterized by worsening metabolic inefficiencies, i.e. higher energy requirements resulting from un-pruned synapses coupled with inefficient acquisition and storage of new information [9, 68]. Deficits in processing of recently acquired information and impaired ability to integrate new information may combine to produce an acute state of confusion. Thus, although the diagnostic criteria of delirium pivot primarily on inattention, when we focus on the genesis of delirium from sleep disruption, what we find is a problem that is precipitated by impairments in memory processing [69, 70].
As described above, sleep disruption is also associated with diminished connectivity within the prefrontal region and between prefrontal and emotion processing centers. These physiologic changes can further exacerbate symptoms of inattention and result in impaired emotional control [71] and perceptual distortions [72], effects that may underlie the behavioral dysregulation observed in patients with hyperactive delirium.
Disruptions in the brain’s metabolic waste processing, impaired memory processing and acquisition, perceptual distortions and executive disinhibition may combine to create a syndrome akin to delirium in sleep-deprived individuals (Fig. 3). Yet delirium itself may also worsen sleep disruption and exacerbate impairments in the associated cognitive processes. In a convenience sample of 12 postoperative patients recovering from orthopedic surgery, delirium severity (as measured by the revised Delirium Rating Scale [73]) was associated with shorter total sleep time on night 1 and increased waking delta power on postoperative day 1, but decreased delta power on night 2 after surgery [74]. While delirium is classically associated with increased theta and delta activity during wakefulness, there is a lack of the organized sleep architecture defining various sleep stages. This may be due to absence of coordinated slow oscillations modulating cerebral function as observed by Dash and Colleagues [3]. Whether the delta and theta waves thus observed is the brain’s attempt to ‘catch up’ on homeostatic sleep functions versus an entirely disparate pattern (i.e. driven by unique generators unrelated to sleep homeostasis and decoupled from CSF pulse flow dynamics) remains to be elucidated. Nonetheless, the bidirectional effect of sleep disruption and delirium may result in a self-propelling cycle, with escalating impairments in memory, cognition and metabolic waste clearance that become difficult for the brain to regulate without external interventions (Fig. 3). Such interventions may include reorientation to familiar faces and voices, modulation of sensory stimuli and promotion of regular sleep-wake cycles. These effects underscore the importance of preserving quality sleep, particularly among individuals at higher risk of delirium, and motivate adherence to systematic protocols that include optimizing sleep quality to minimize risk of delirium in inpatient settings [75, 76].

Deliriogenic Potential of Sleep Disruption (A Neurophysiologic Perspective): Lack of the normal physiologic activity characterizing sleep leads to 1) disruptions in CSF flow dynamics and impaired clearance of the brain’s metabolic waste products, 2) reductions in the normal memory consolidation processes that allow for efficient memory processing and efficient acquisition of new information, and 3) disorganized connectivity among brain regions responsible for memory processing, perception, emotional control and other cognitive functions. These deficits cause a cascade of symptoms that are characterized by pathological neuronal firing patterns (manifest on EEG recordings as pathological delta and theta waves) and ultimately, due to increasing sleep pressure, lead to characteristic signs of delirium. Atypical sleep and pathological wakefulness, though present in non-delirious patients, may represent subsyndromal delirium or EEG harbingers of impending delirium onset
6 Clinical Implications: Sleep in the ICU and Beyond
The propensity for sleep disruption to precipitate or contribute to delirium in at-risk patients raises the question of how best to ensure optimal sleep quality in the ICU. Though polysomnography (PSG) is the gold standard for monitoring and assessing sleep quality, PSG is often impractical in the ICU environment and traditional scoring criteria do not translate well to this setting [61]. Sleep questionnaires are limited by subjectivity and are not suitable for patients with impaired communication. Accelerometry devices may be hindered by restrictions in spontaneous movement due to indwelling catheters or physical injuries. A role can be envisioned for limited-montage EEG as a standardized measurement of sleep in the ICU. Attempts have been made to use bispectral index to stage sleep in critically ill patients [77], and emerging wearable EEG devices may find utility in this setting [78, 79]. Importantly, these will require careful study for optimal implementation given the ICU-specific conditions (e.g. sedation, hepatic or renal failure, mechanical ventilation) that frequently influence EEG signals [80, 81]. Chapter “Methods for Routine Sleep Assessment and Monitoring” reviews sleep assessment in more detail.
While delirium in the ICU confers a dose-dependent increase in the risk of long-term cognitive impairment [82] and sleep deprivation is associated with worse cognitive trajectory among the general population [83], little is known about sleep disruption and cognitive impairment in the post-ICU period. Between 10 and 61% of ICU survivors experience persistent sleep disturbances up to 6 months after critical illness [84]. Wilcox et al. followed 102 ICU survivors to estimate sleep using actigraphy and assess cognition using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). They found an association between sleep fragmentation and cognitive impairment at 7 days after ICU discharge but not at 6- or 12-month follow-up [85]. Though EEG features of sleep and wakefulness improve simultaneously with improvements in cognitive function during critical illness, the timing and trajectory of these changes in the post-ICU period is yet to be elucidated [86].
7 Summary and Conclusions
Normal sleep is characterized by a series of neurophysiologic processes that are identifiable in EEG activity patterns. Slow oscillations, delta and theta waves, and sleep spindles indicate particular types of activity within and between specialized structures in the brain. The hippocampus, thalamus, and cerebral cortex play integral parts in the processes of waste clearance, memory consolidation and cortical reorganization during sleep. These functions are important for maintenance of cerebral function and their disruption leads to symptoms and signs consistent with delirium, particularly among at-risk individuals. These patterns give insight to possible neurophysiologic mechanisms underlying the relationship between sleep disruption and delirium. We propose that sleep disruption may be characterized by specific alterations in EEG activity patterns that result in inefficient clearance of cerebral metabolic waste, impaired memory consolidation and disrupted brain connectivity, leading to memory loss, inattention, and difficulty processing new information. The physiologic processes underlying delirium may further exacerbate sleep disruption, fueling a self-propelling cycle and motivating interventions to maintain appropriate sleep hygiene in at-risk populations.
Yet several gaps exist in our understanding of this relationship. Are the delta waves of delirium and those of slow-wave sleep borne of the same neural generators? What of the theta activity that is typically observed in earlier stages of delirium? Does the modulatory effect of slow oscillations remain intact in delirium? And fundamentally: does impaired memory consolidation increase risk of delirium independent of other functions of sleep? Both sleep disruption and delirium are associated with long-term cognitive decline and increased risk of dementia [82, 87]. Are the neurophysiologic processes linking these conditions also responsible for cognitive aging? Investigations to elucidate these questions will inform development of therapeutic interventions and motivate approaches to optimizing the restorative functions of sleep.
References
Loomis AL, Harvey EN, Hobart G. Potential rhythms of the cerebral cortex during sleep. Science 1935;81(0036-8075 (Print)):597–8.
Caporro M, Zulfi H, Yeh HJ, Lenartowicz A, Buttinelli C, Parvizi J, et al. Functional MRI of sleep spindles and K-complexes. Clin Neurophysiol. 2012;123(2):303–9. https://doi.org/10.1016/j.clinph.2011.06.018.
Dash MB. Infraslow coordination of slow wave activity through altered neuronal synchrony. Sleep. 2019;42(12):1–13. https://doi.org/10.1093/sleep/zsz170.
Kim J, Gulati T, Ganguly K. Competing roles of slow oscillations and Delta waves in memory consolidation versus forgetting. Cell. 2019;179(2):514–26.e13. https://doi.org/10.1016/j.cell.2019.08.040.
Diekelmann S, Born J. The memory function of sleep. Nat Rev Neurosci. 2010;11(2):114–26. https://doi.org/10.1038/nrn2762.
Daurat A, Terrier P, Foret J, Tiberge M. Slow wave sleep and recollection in recognition memory. Conscious Cogn. 2007;16(2):445–55. https://doi.org/10.1016/j.concog.2006.06.011.
Gent TC, Bandarabadi M, Herrera CG, Adamantidis AR. Thalamic dual control of sleep and wakefulness. Nat Neurosci. 2018;21(7):974–84. https://doi.org/10.1038/s41593-018-0164-7.
Steriade M, Nunez A, Amzica F. Intracellular analysis of relations between the slow (<I Hz) neocortical oscillation and other sleep rhythms of the electroencephalogram. J Neurosci. 1993;13(8):3266–83. https://doi.org/10.1016/S0040-4039(97)01107-6.
Tononi G, Cirelli C. Sleep and the price of plasticity: from synaptic and cellular homeostasis to memory consolidation and integration. Neuron. 2014;81(1):12–34. https://doi.org/10.1016/j.neuron.2013.12.025.
Peters AJ, Chen SX, Komiyama T. Emergence of reproducible spatiotemporal activity during motor learning. Nature. 2014;510(7504):263–7. https://doi.org/10.1038/nature13235.
Okubo TS, Mackevicius EL, Payne HL, Lynch GF, Fee MS. Growth and splitting of neural sequences in songbird vocal development. Nature. 2015;528(7582):352–7. https://doi.org/10.1038/nature15741.
Fultz NE, Bonmassar G, Setsompop K, Stickgold RA, Rosen BR, Polimeni JR, et al. Coupled electrophysiological, hemodynamic, and cerebrospinal fluid oscillations in human sleep. Science. 2019;366(6465):628–31. https://doi.org/10.1126/science.aax5440.
Hablitz LM, Vinitsky HS, Sun Q, Staeger FF, Sigurdsson B, Mortensen KN, et al. Increased glymphatic influx is correlated with high EEG delta power and low heart rate in mice under anesthesia. Sci Adv. 2019;5(2):eaav5447. https://doi.org/10.1126/sciadv.aav5447.
Iliff JJ, Wang M, Liao Y, Plogg BA, Peng W, Gundersen GA, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid beta. Sci Transl Med. 2012;4(147):147ra11. https://doi.org/10.1126/scitranslmed.3003748.
Iaccarino HF, Singer AC, Martorell AJ, Rudenko A, Gao F, Gillingham TZ, et al. Gamma frequency entrainment attenuates amyloid load and modifies microglia. Nature. 2016;540(7632):230–5. https://doi.org/10.1038/nature20587.
Ju YS, Ooms SJ, Sutphen C, Macauley SL, Zangrilli MA, Jerome G, et al. Slow wave sleep disruption increases cerebrospinal fluid amyloid-beta levels. Brain. 2017;140(8):2104–11. https://doi.org/10.1093/brain/awx148.
Mander BA, Rao V, Lu B, Saletin JM, Lindquist JR, Ancoli-Israel S, et al. Prefrontal atrophy, disrupted NREM slow waves and impaired hippocampal-dependent memory in aging. Nat Neurosci. 2013;16(3):357–64. https://doi.org/10.1038/nn.3324.
Wei Y, Krishnan GP, Komarov M, Bazhenov M. Differential roles of sleep spindles and sleep slow oscillations in memory consolidation. 2018.
Capone C, Pastorelli E, Golosio B, Paolucci PS. Sleep-like slow oscillations improve visual classification through synaptic homeostasis and memory association in a thalamo-cortical model. Sci Rep. 2019;9(1):1–11. https://doi.org/10.1038/s41598-019-45525-0.
Schabus M, Dang-Vu TT, Albouy G, Balteau E, Boly M, Carrier J, et al. Hemodynamic cerebral correlates of sleep spindles during human non-rapid eye movement sleep. Proc Natl Acad Sci U S A. 2007;104(32):13164–9. https://doi.org/10.1073/pnas.0703084104.
Andrillon T, Nir Y, Staba RJ, Ferrarelli F, Cirelli C, Tononi G, et al. Sleep spindles in humans: insights from intracranial EEG and unit recordings. J Neurosci. 2011;31(49):17821. https://doi.org/10.1523/JNEUROSCI.2604-11.2011.
Maingret N, Girardeau G, Todorova R, Goutierre M, Zugaro M. Hippocampo-cortical coupling mediates memory consolidation during sleep. Nat Neurosci. 2016;19(7):959–64. https://doi.org/10.1038/nn.4304.
van Schalkwijk FJ, Hauser T, Hoedlmoser K, Ameen MS, Wilhelm FH, Sauter C, et al. Procedural memory consolidation is associated with heart rate variability and sleep spindles. J Sleep Res. 2020;29(3):1–8. https://doi.org/10.1111/jsr.12910.
Manoach DS, Stickgold R. Abnormal sleep spindles, memory consolidation, and schizophrenia. Annu Rev Clin Psychol. 2017;2019(15):451–79. https://doi.org/10.1146/annurev-clinpsy-050718-095754.
Sirota A, Montgomery S, Fujisawa S, Isomura Y, Zugaro M, Buzsáki G. Entrainment of neocortical neurons and gamma oscillations by the hippocampal theta rhythm. Neuron. 2008;60(4):683–97. https://doi.org/10.1016/j.neuron.2008.09.014.
Goutagny R, Jackson J, Williams S. Self-generated theta oscillations in the hippocampus. Nat Neurosci. 2009;12(12):1491–3. https://doi.org/10.1038/nn.2440.
Schreiner T, Doeller CF, Jensen O, Rasch B, Staudigl T. Theta phase-coordinated memory reactivation reoccurs in a slow-oscillatory rhythm during NREM sleep. Cell Rep. 2018;25(2):296–301. https://doi.org/10.1016/j.celrep.2018.09.037.
Dragoi G, Buzsáki G. Temporal encoding of place sequences by hippocampal cell assemblies. Neuron. 2006;50(1):145–57. https://doi.org/10.1016/j.neuron.2006.02.023.
Wikenheiser AM, Redish AD. Hippocampal theta sequences reflect current goals. Nat Neurosci. 2015;18(2):289–94. https://doi.org/10.1038/nn.3909.
Hutchison IC, Rathore S. The role of REM sleep theta activity in emotional memory. Front Psychol. 2015;6:1439.
Lansink CS, Goltstein PM, Lankelma JV, McNaughton BL, Pennartz CMA. Hippocampus leads ventral striatum in replay of place-reward information. PLoS Biol. 2009;7(8) https://doi.org/10.1371/journal.pbio.1000173.
Klinzing JG, Niethard N, Born J. Mechanisms of systems memory consolidation during sleep. Nat Neurosci. 2019;22(October) https://doi.org/10.1038/s41593-019-0467-3.
Buzsaki G, Draguhn A. Neuronal oscillations in cortical networks. Science. 2004;304(5679):1926–9. https://doi.org/10.1126/science.1099745.
van den Heuvel MP, Sporns O. Rich-club organization of the human connectome. J Neurosci. 2011;31(44):15775–86. https://doi.org/10.1523/JNEUROSCI.3539-11.2011.
Imperatori LS, Betta M, Cecchetti L, Canales-Johnson A, Ricciardi E, Siclari F, et al. EEG functional connectivity metrics wPLI and wSMI account for distinct types of brain functional interactions. Sci Rep. 2019;9(1):1–15. https://doi.org/10.1038/s41598-019-45289-7.
Massimini M, Ferrarelli F, Huber R, Esser SK, Singh H, Tononi G. Breakdown of cortical effective connectivity during sleep. Science. 2005;309(5744):2228–32. https://doi.org/10.1126/science.1117256.
Tononi G. Consciousness as integrated information: a provisional manifesto. Biol Bull. 2008;215(3):216–42. https://doi.org/10.2307/25470707.
Lee AK, Wilson MA. Memory of sequential experience in the hippocampus during slow wave sleep. Neuron. 2002;36(6):1183–94. https://doi.org/10.1016/s0896-6273(02)01096-6.
Berkers RMWJ, Ekman M, van Dongen EV, Takashima A, Barth M, Paller KA, et al. Cued reactivation during slow-wave sleep induces brain connectivity changes related to memory stabilization. Sci Rep. 2018;8(1):1–12. https://doi.org/10.1038/s41598-018-35287-6.
Theodoni P, Rovira B, Wang Y, Roxin A. Theta-modulation drives the emergence of connectivity patterns underlying replay in a network model of place cells. elife. 2018;7:1–33. https://doi.org/10.7554/eLife.37388.
Bastuji H, Cadic-Melchior A, Magnin M, Garcia-Larrea L. Intracortical functional connectivity predicts arousal to noxious stimuli during sleep in humans. J Neurosci. 2021;41(23):5115–23. https://doi.org/10.1523/JNEUROSCI.2935-20.2021.
Na SH, Jin SH, Kim SY. The effects of total sleep deprivation on brain functional organization: mutual information analysis of waking human EEG. Int J Psychophysiol. 2006;62(2):238–42. https://doi.org/10.1016/j.ijpsycho.2006.03.006.
Verweij IM, Romeijn N, Smit DJA, Piantoni G, Van Someren EJW, van der Werf YD. Sleep deprivation leads to a loss of functional connectivity in frontal brain regions. BMC Neurosci. 2014;15:1–10. https://doi.org/10.1186/1471-2202-15-88.
Henri-Bhargava A, Stuss DT, Freedman M. Clinical assessment of prefrontal lobe functions. CONTINUUM lifelong learning in Neurology. 2018;24(3, BEHAVIORAL NEUROLOGY AND PSYCHIATRY):704–26. https://doi.org/10.1212/CON.0000000000000609.
Qi J, Li BZ, Zhang Y, Pan B, Gao YH, Zhan H, et al. Disrupted small-world networks are associated with decreased vigilant attention after total sleep deprivation. Neuroscience. 2021;471:51–60. https://doi.org/10.1016/j.neuroscience.2021.07.010.
Wang H, Yu K, Yang T, Zeng L, Li J, Dai C, et al. Altered functional connectivity in the resting state neostriatum after complete sleep deprivation: impairment of motor control and regulatory network. Front Neurosci. 2021;15(August):1–11. https://doi.org/10.3389/fnins.2021.665687.
Skorucak J, Arbon EL, Dijk DJ, Achermann P. Response to chronic sleep restriction, extension, and subsequent total sleep deprivation in humans: adaptation or preserved sleep homeostasis? Sleep. 2018;41(7):1–17. https://doi.org/10.1093/sleep/zsy078.
Vyazovskiy VV, Delogu A. NREM and REM sleep: complementary roles in recovery after wakefulness. Neuroscientist. 2014;20(3):203–19. https://doi.org/10.1177/1073858413518152.
Mander BA, Reid KJ, Baron KG, Tjoa T, Parrish TB, Paller KA, et al. EEG measures index neural and cognitive recovery from sleep deprivation. J Neurosci. 2010;30(7):2686–93. https://doi.org/10.1523/JNEUROSCI.4010-09.2010.
Romano J, Engel GL. Delirium: Electroencephalographic data. Arch Neurol Psychiatr. 1944;51:356–77.
Faigle R, Sutter R, Kaplan PW. Electroencephalography of encephalopathy in patients with endocrine and metabolic disorders. J Clin Neurophysiol. 2013;30(5):505–16. https://doi.org/10.1097/WNP.0b013e3182a73db9.
Kaplan PW. The EEG in metabolic encephalopathy and coma. J Clin Neurophysiol. 2004;21(5):307–18.
Sutter R, Kaplan PW. Clinical and electroencephalographic correlates of acute encephalopathy. J Clin Neurophysiol. 2013;30(5):443–53. https://doi.org/10.1097/WNP.0b013e3182a73bc2.
Payne LE, Gagnon DJ, Riker RR, Seder DB, Glisic EK, Morris JG, et al. Cefepime-induced neurotoxicity: a systematic review. Crit Care. 2017;21(1):276. https://doi.org/10.1186/s13054-017-1856-1.
Akeju O, Pavone KJ, Westover MB, Vazquez R, Prerau MJ, Harrell PG, et al. A comparison of propofol- and dexmedetomidine-induced electroencephalogram dynamics using spectral and coherence analysis. Anesthesiology. 2014;121(5):978–89. https://doi.org/10.1097/ALN.0000000000000419.
Schmitt SE, Pargeon K, Frechette ES, Hirsch LJ, Dalmau J, Friedman D. Extreme delta brush. Neurology. 2012;79(11):1094. https://doi.org/10.1212/WNL.0b013e3182698cd8.
Numan T, Slooter AJC, van der Kooi AW, Hoekman AML, Suyker WJL, Stam CJ, et al. Functional connectivity and network analysis during hypoactive delirium and recovery from anesthesia. Clin Neurophysiol. 2017;128(6):914–24. https://doi.org/10.1016/j.clinph.2017.02.022.
van der Kooi AW, Slooter AJ, van Het Klooster MA, Leijten FS. EEG in delirium: increased spectral variability and decreased complexity. Clin Neurophysiol. 2014;125(10):2137–9. https://doi.org/10.1016/j.clinph.2014.02.010.
Williams Roberson S, Azeez N, Taneja R, Pun BT, Pandharipande P, Jackson JC, et al. The relationship between EEG characteristics during critical illness and long-term cognitive impairment. Neurology. 2020;94(15 Supp)
Drouot X, Roche-Campo F, Thille AW, Cabello B, Galia F, Margarit L, et al. A new classification for sleep analysis in critically ill patients. Sleep Med. 2012;13(1):7–14. https://doi.org/10.1016/j.sleep.2011.07.012.
Watson PL, Pandharipande P, Gehlbach BK, Thompson JL, Shintani AK, Dittus BS, et al. Atypical sleep in ventilated patients: empirical electroencephalography findings and the path toward revised ICU sleep scoring criteria. Crit Care Med. 2013;41(8):1958–67. https://doi.org/10.1097/CCM.0b013e31828a3f75.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2(7872):81–4. https://doi.org/10.1016/s0140-6736(74)91639-0.
Sessler CN, Gosnell MS, Grap MJ, Brophy GM, O'Neal PV, Keane KA, et al. The Richmond agitation-sedation scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166(10):1338–44. https://doi.org/10.1164/rccm.2107138.
Weinhouse GL, Schwab RJ, Watson PL, Patil N, Vaccaro B, Pandharipande P, et al. Bench-to-bedside review: delirium in ICU patients – importance of sleep deprivation. Crit Care. 2009;13(6) https://doi.org/10.1186/cc8131.
Da Mesquita S, Papadopoulos Z, Dykstra T, Brase L, Farias FG, Wall M, et al. Meningeal lymphatics affect microglia responses and anti-Aβ immunotherapy. Nature. 2021;593(7858):255–60. https://doi.org/10.1038/s41586-021-03489-0.
Tarasoff-Conway JM, Carare RO, Osorio RS, Glodzik L, Butler T, Fieremans E, et al. Clearance systems in the brain-implications for Alzheimer disease. Nat Rev Neurol. 2015;11(8):457–70. https://doi.org/10.1038/nrneurol.2015.119.
Fong TG, Jones RN, Marcantonio ER, Tommet D, Gross AL, Habtemariam D, et al. Adverse outcomes after hospitalization and delirium in persons with Alzheimer disease. Ann Intern Med. 2012;156(12):848–56, W296. https://doi.org/10.7326/0003-4819-156-12-201206190-00005
Vyazovskiy VV, Olcese U, Lazimy YM, Faraguna U, Esser SK, Williams JC, et al. Cortical firing and sleep homeostasis. Neuron. 2009;63(6):865–78. https://doi.org/10.1016/j.neuron.2009.08.024.
Sanders RD. Hypothesis for the pathophysiology of delirium: role of baseline brain network connectivity and changes in inhibitory tone. Med Hypotheses. 2011;77(1):140–3. https://doi.org/10.1016/j.mehy.2011.03.048.
Maldonado JR. Delirium pathophysiology: an updated hypothesis of the etiology of acute brain failure. Int J Geriatr Psychiatry. 2018;33(11):1428–57. https://doi.org/10.1002/gps.4823.
Simon EB, Oren N, Sharon H, Kirschner A, Goldway N, Okon-Singer H, et al. Losing neutrality: the neural basis of impaired emotional control without sleep. J Neurosci. 2015;35(38):13194–205. https://doi.org/10.1523/JNEUROSCI.1314-15.2015.
Petrovsky N, Ettinger U, Hill A, Frenzel L, Meyhöfer I, Wagner M, et al. Sleep deprivation disrupts prepulse inhibition and induces psychosis-like symptoms in healthy humans. J Neurosci. 2014;34(27):9134. https://doi.org/10.1523/JNEUROSCI.0904-14.2014.
Trzepacz PT, Mittal D, Torres R, Kanary K, Norton J, Jimerson N. Validation of the delirium rating scale-revised-98: comparison with the delirium rating scale and the cognitive test for delirium. J Neuropsychiatry Clin Neurosci. 2001;13(2):229–42. https://doi.org/10.1176/jnp.13.2.229.
Evans JL, Nadler JW, Preud'homme XA, Fang E, Daughtry RL, Chapman JB, et al. Pilot prospective study of post-surgery sleep and EEG predictors of post-operative delirium. Clin Neurophysiol. 2017;128(8):1421–5. https://doi.org/10.1016/j.clinph.2017.05.004.
Pun BT, Balas MC, Barnes-Daly MA, Thompson JL, Aldrich JM, Barr J, et al. Caring for critically ill patients with the ABCDEF bundle: results of the ICU liberation collaborative in over 15,000 adults. Crit Care Med. 2019;47(1):3–14. https://doi.org/10.1097/CCM.0000000000003482.
Devlin JW, Skrobik Y, Gelinas C, Needham DM, Slooter AJC, Pandharipande PP, et al. Clinical practice guidelines for the prevention and Management of Pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825–e73. https://doi.org/10.1097/CCM.0000000000003299.
Nicholson T, Patel J, Sleigh JW. Sleep patterns in intensive care unit patients: a study using the bispectral index. Crit Care Resusc. 2001;3(2):86–91.
Arnal PJ, Thorey V, Debellemaniere E, Ballard ME, Bou Hernandez A, Guillot A, et al. The Dreem headband compared to polysomnography for electroencephalographic signal acquisition and sleep staging. Sleep. 2020;43(11) https://doi.org/10.1093/sleep/zsaa097.
Mikkelsen KB, Tabar YR, Kappel SL, Christensen CB, Toft HO, Hemmsen MC, et al. Accurate whole-night sleep monitoring with dry-contact ear-EEG. Sci Rep. 2019;9(1):16824. https://doi.org/10.1038/s41598-019-53115-3.
Watson PL. Measuring sleep in critically ill patients: beware the pitfalls. Crit Care. 2007;11(4):159. https://doi.org/10.1186/cc6094.
Pisani MA, Friese RS, Gehlbach BK, Schwab RJ, Weinhouse GL, Jones SF. Sleep in the intensive care unit. Am J Respir Crit Care Med. 2015;191(7):731–8. https://doi.org/10.1164/rccm.201411-2099CI.
Pandharipande PP, Girard TD, Jackson JC, Morandi A, Thompson JL, Pun BT, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306–16. https://doi.org/10.1056/NEJMoa1301372.
Ma Y, Liang L, Zheng F, Shi L, Zhong B, Xie W. Association between sleep duration and cognitive decline. JAMA Netw Open. 2020;3(9):e2013573. https://doi.org/10.1001/jamanetworkopen.2020.13573.
Altman MT, Knauert MP, Pisani MA. Sleep disturbance after hospitalization and critical illness: a systematic review. Ann Am Thorac Soc. 2017;14(9):1457–68. https://doi.org/10.1513/AnnalsATS.201702-148SR.
Wilcox ME, McAndrews MP, Van J, Jackson JC, Pinto R, Black SE, et al. Sleep fragmentation and cognitive trajectories after critical illness. Chest. 2021;159(1):366–81. https://doi.org/10.1016/j.chest.2020.07.036.
Wilcox ME, Lim AS, McAndrews MP, Wennberg RA, Pinto RL, Black SE, et al. A study protocol for an observational cohort investigating COGnitive outcomes and WELLness in survivors of critical illness: the COGWELL study. BMJ Open. 2017;7(7):e015600. https://doi.org/10.1136/bmjopen-2016-015600.
Waser M, Lauritzen MJ, Fagerlund B, Osler M, Mortensen EL, Sørensen HBD, et al. Sleep efficiency and neurophysiological patterns in middle-aged men are associated with cognitive change over their adult life course. J Sleep Res. 2019;28(4):e12793. https://doi.org/10.1111/jsr.12793.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Okinedo, I., Andrews, P.S., Ely, E.W., Williams Roberson, S. (2022). Sleep Disruption and Its Relationship with Delirium: Electroencephalographic Perspectives. In: Weinhouse, G.L., Devlin, J.W. (eds) Sleep in Critical Illness. Springer, Cham. https://doi.org/10.1007/978-3-031-06447-0_8
Download citation
DOI: https://doi.org/10.1007/978-3-031-06447-0_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-06446-3
Online ISBN: 978-3-031-06447-0
eBook Packages: MedicineMedicine (R0)